Abstract
Introduction: Ensuring accurate patient setup is crucial in radiotherapy for head and neck cancer (HNC) due to the intricate anatomy and the closeness to vital organs. This study aimed to assess and compare the effectiveness of two different daily pre-treatment auto image registration techniques utilizing Radixact TomoTherapy-based megavoltage computed tomography (MVCT) to enhance setup accuracy and treatment consistency. Materials and Methods: A prospective analysis was performed on a cohort of twenty HNC patients undergoing treatment with Radixact TomoTherapy. Two image verification techniques were assessed: one focused on aligning bony anatomy (Method A) and the other on adjusting the cross-wire at the center of the planning target volume (PTV) for automatic registration (Method B). Daily MVCT images were taken and analyzed to determine translational setup corrections, which were documented for further analysis. Results: Method B exhibited slightly lower mean systematic errors in both the longitudinal and lateral directions, although the differences were not statistically significant. Method A demonstrated significantly lower errors in the vertical (Z-axis) direction (p = 0.013). Overall displacement vectors favored Method A, yet multivariate analysis indicated no significant difference between the two methods. Therefore, both methods were found to perform similarly, with Method A showing superior vertical alignment. Conclusions: Both auto image registration techniques provide accuracy and dependability, bolstered by reproducible anatomy and clinician supervision. For optimal precision, Method A is suggested for initial gross alignment, followed by Method B for fine-tuning around the target volume, thereby improving dose precision and safety in high-accuracy radiotherapy treatments. Key Messages: Combining initial alignment with Method A and refinement with Method B enhances precision and safety in head and neck radiotherapy, optimizing setup accuracy using Radixact TomoTherapy MVCT imaging.
Keywords
Image Registration, Crosswire, MVCT, Radixact Tomotherapy, Setup Error
1. Introduction
Precision radiotherapy is essential in the curative treatment of various cancers
| [1] | Beaton L, Bandula S, Gaze MN, Sharma RA. How rapid advances in imaging are defining the future of precision radiation oncology. Br J Cancer. 2019; 120(8): 779-90.
https://doi.org/10.1038/s41416-019-0412-y |
[1]
. It can be administered as a standalone therapy or in conjunction with other treatment options, achieving a cure rate of approximately 40% for cancer patients
. Recent technological advancements have enabled the customization of radiotherapy to better align with the unique needs of each patient and their specific diagnosis. Online Image guided radiotherapy (IGRT) allows the correction of both systematic (treatment preparation) and random (treatment delivery) errors so that targeting can be more accurate. Providing greater security of target coverage and reducing the dose to surrounding normal tissues
. The combination of Image guided intensity modulated radiotherapy (IG-IMRT) allows treatments previously considered impossible
. Mega voltage computed tomography (MVCT) on the tomotherapy system allowed daily volumetric evaluation of pre-treatment position of patients
| [7] | Kupelian PA, Ramsey C, Meeks SL, Willoughby TR, Forbes A, Wagner TH, et al. Serial megavoltage CT imaging during external beam radiotherapy for non-small-cell lung cancer: Observations on tumor regression during treatment. Int J Radiat Oncol Biol Phys. 2005; 63(4): 1024-8.
https://doi.org/10.1016/j.ijrobp.2005.03.055 |
[7]
.
MVCT was found to be an important imaging tool for precise radiation delivery because it provides considerably more anatomical detail than conventional radiation therapy port films used for patient setup verification. There is a growing number of publications comparing treatment plans of different radiotherapy techniques to helical tomotherapy (HT) delivery
| [8] | Yartsev S, Kron T, Cozzi L, Fogliata A, Bauman G. Tomotherapy planning of small brain tumours. Radiother Oncol. 2005; 74(1): 49-52.
https://doi.org/10.1016/j.radonc.2004.12.003 |
| [9] | Langen KM, Meeks SL, Poole DO, Wagner TH, Willoughby TR, Kupelian PA, et al. The use of megavoltage CT (MVCT) images for dose recomputations. Phys Med Biol. 2005; 50(18): 4259-76. https://doi.org/10.1088/0031-9155/50/18/001 |
[8, 9]
. During MVCT scanning, the nominal energy of the incident electron beam is reduced from 6 to 3.5 MV, and the radiation field is collimated in the longitudinal direction to 4 mm. All multileaf collimator (MLC) leaves are open during the MVCT acquisition
| [10] | Jeraj R, Mackie TR, Balog J, Olivera G, Pearson D, Kapatoes J, et al. Radiation characteristics of helical tomotherapy. Med Phys. 2004; 31(2): 396-404. https://doi.org/10.1118/1.1639992 |
[10]
. MVCT images enable radiation therapists (RTT) to assess the precise dose administered during each treatment fraction. The dose for subsequent treatments will be adjusted according to the evaluation findings and the treatment plan, facilitating dose-adaptive and precision radiotherapy
| [11] | Jin S, Xu X, Su Z, Tang L, Zheng M, Liang P, Zhang H. MVCT image enhancement using reference-based encoder-decoder convolutional neural network. Expert Syst Appl. 2023; 241: 122576. https://doi.org/10.1016/j.eswa.2023.122576 |
[11]
. IGRT focuses on obtaining patient anatomical data within the treatment environment to inform decision-making, enhancing treatment quality. With new technical advancements, the development of automated tools for image registration and the quantification of setup errors has become feasible and has significantly advanced the practice of IGRT
.
Several elements, including auto registration algorithms and matching techniques employed in an image registration software, play a crucial role in maintaining the geometric precision of patient positioning errors throughout the treatment delivery process
| [14] | Jarrett D, Stride E, Vallis K, Gooding MJ. Applications and limitations of machine learning in radiation oncology. Br J Radiol. 2019; 92(1100): 20190001.
https://doi.org/10.1259/bjr.20190001 |
| [15] | Guo Y, Hao Z, Zhao S, Gong J, Yang F. Artificial intelligence in health care: Bibliometric analysis. J Med Internet Res. 2020; 22(7): e18228. https://doi.org/10.2196/18228 |
[14, 15]
. At present, we are unaware of any specific data that contrasts the various matching methods employed in the radixact tomotherapy treatment delivery console. Therefore, this study aims to assess the impact of different auto registration techniques on patient setup inaccuracies in individuals receiving head and neck helical tomotherapy treatment.
This study fills a gap in current research by directly comparing two automatic image registration methods, bone-based and target-centered on the Radixact Tomotherapy system. Previous studies mostly looked at older Tomotherapy or CBCT systems, but very little data exist for the newer Radixact platform. Our work adds new information about how these two techniques perform in daily use and how they can improve setup accuracy for head and neck cancer treatments.
2. Materials and Methods
In this prospective study, twenty patients with head and neck cancer received a total dose of 60 Gy in 30 fractions using a 6 MV FFF photon beam delivered via the Tomo Helical technique on the Radixact X9 system (
Table 1,
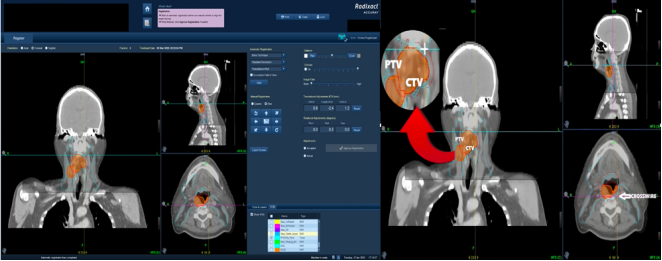
Figure 1). Daily image verification was performed using MVCT according to the institutional image guidance protocol, resulting in 40 MVCT scans for setup verification. Two different auto-registration methods were evaluated for image alignment accuracy. Each MVCT image verification incorporated a crosswire to facilitate precise alignment across the sagittal, coronal, and axial views. To assess the effectiveness of crosswire-based auto-registration, daily offset data were collected for both registration methods. In Method A, the acquired volumetric image was auto-matched using the Bone T algorithm to determine translational offset corrections (
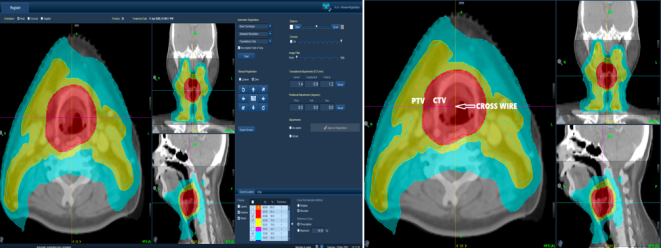
Figure 2). In Method B, a crosswire was positioned at the center of the planning target volume (PTV) before performing auto-matching (
Figure 3). The resulting offset data from both techniques were analyzed to identify the optimal image registration approach.
The treatment delivery console allows radiation therapists (RTTs) to manage all aspects of the treatment process, including initiating, pausing, and monitoring treatment delivery, as well as handling patient imaging and positioning. It serves as a central component of the TomoTherapy system, integrating treatment planning, CT-based image guidance, and delivery. The console enables registration of patient imaging data to ensure congruence between the treatment plan and patient anatomy. Both automatic and manual registration options are available to align daily scans with planning images, with updates reflected in all three anatomical views. The Bone T algorithm relies exclusively on high-density bone data points for accurate alignment during auto-registration.
Table 1. Patient demographics and clinical details for 20 head and neck cancer cases treated with 60 Gy/30 fractions using 6 MV FFF Tomo Helical on Radixact X9 with daily MVCT verification.
Characteristic | Category / Unit | Number of Patients (n) | Percentage (%) |
Age (years) | Mean ± SD = 58.4 ± 8.6 (Range: 42-73) | - | - |
Gender | Male | 10 | 50 |
| Female | 10 | 50 |
Primary Tumor Site | Oropharynx | 7 | 35 |
| Larynx | 5 | 25 |
| Hypopharynx | 4 | 20 |
| Nasopharynx | 2 | 10 |
| Oral cavity | 2 | 10 |
Laterality of Lesion | Right | 9 | 45 |
| Left | 8 | 40 |
| Midline | 3 | 15 |
Prescribed Dose | 60 Gy in 30 fractions | 20 | 100 |
Beam Energy | 6 MV FFF photon beam | 20 | 100 |
Treatment Technique | Tomo Helical (Radixact X9 system) | 20 | 100 |
Image Guidance Modality | MVCT (Daily pre-treatment) | 20 | 100 |
Immobilization Device | 4 Clamp H&N Mould | 20 | 100 |
Treatment Duration (days) | Mean ± SD = 42.3 ± 3.1 | - | - |
Figure 1. The figure illustrates the Radixact X9 tomotherapy system.
Figure 2. Showing Bone T auto-registration interface on the TomoTherapy console (Method A).
Figure 3. Interphase of Bone T auto-registration (Method B) after cross-wire alignment at PTV center on the TomoTherapy.
2.1. Patient Selection
A total of twenty patients diagnosed with HNC participated in this study. These individuals underwent intensity-modulated (IM) helical tomotherapy at our facility from July 2024 to December 2024. The age range of the patients was between 42 and 73 years, encompassing all genders, and they received a dosage of 60 Gy over 30 fractions during their initial radiotherapy sessions. Patients who required a replan were excluded from the study due to significant anatomical alterations, as neither registration technique was able to fulfil the clinical treatment criteria.
2.2. Image Acquisition
The primary objective of obtaining MVCT images before the commencement of treatment is to confirm and adjust the patient's positioning for the procedure. This procedure requires the alignment of daily images with the planning images. A variety of image registration tools are available at the tomotherapy treatment delivery console, including blending tools, contrast adjustments, image enlargement tools, and crosswire alignments. RTT’s are responsible for selecting the superior-inferior extent of the MVCT scan, which offers two parameters for selection. First, the scan range must be established, which is adaptable and typically includes the PTV treatment area. A wider scan range will inherently require more time to complete. The second parameter relates to the image pitch, which affects the nominal slice thickness. There are three available options: fine, normal, and coarse, corresponding to nominal slice thicknesses of 2 mm, 4 mm, and 6 mm, respectively. Since the gantry operates at a constant speed during all imaging procedures, scanning the same volume will take longer in fine mode than in normal mode.
2.3. Image Registration
Bone (T) matching (Translational) (BM): Automates the alignment of reference and onboard CT images by allowing the crosswire to be positioned randomly within the image dataset. This technique utilizes chamfer matching algorithms to ascertain the required translation and rotation, relying on densities that are indicative of bone densities. (Method A)
Bone (T) with the Crosswire placing at the Center of the PTV (Translational): This method aligns reference and onboard CT images by ensuring that the crosswire is positioned centrally within the PTV volume of the image dataset. Calculation of Setup errors denotes the difference between the planned and actual positioning of a patient during treatment. (Method B)
These errors are typically evaluated by comparing an onboard treatment image with its corresponding reference image, with a focus on the patient's setup error within the treatment field. Setup errors are classified into two primary categories: (1) Systematic error and (2) Random error. Systematic patient error (∑) is calculated by averaging the measured setup errors for each imaged fraction across all directions, using three different matching methods. Conversely, random error (σ) is determined by the root mean square of the standard deviations of errors recorded for each patient, also utilizing three matching methods. The mean setup error (M) indicates the average setup error across all directions, while the maximum error (E) is defined as the largest deviation observed in each direction, again employing three matching methods.
Following the guidelines set forth by ICRU 50, 62, and 83, Radiation oncologists and RTTs were identified the gross tumor volume (GTV), clinical target volume (CTV), and organ at risk volume (OAR). To mitigate uncertainties in patient setup during treatment, the planned target volume (PTV) was established around the CTV. RTTs conducted a comparison between the onboard MVCT images and the registered CT images to determine the final setup error, which received approval from the radiation oncologist. Adjustments were made through couch offset corrections at the treatment delivery console.
2.4. Significance of Setup Errors
Setup errors in MVCT-based image matching during radiotherapy can significantly compromise treatment accuracy, potentially resulting in insufficient tumor dose coverage or excessive radiation exposure to healthy tissues. Accurate alignment is vital for effective therapy, as it reduces the risk of complications. Implementing regular corrections and adaptive planning strategies can help alleviate these errors, thereby ensuring optimal radiation delivery and enhancing patient outcomes. In the context of MVCT-based image matching for radiotherapy, such errors can severely impact the precision of treatment. Therefore, maintaining precise alignment is crucial for effective dose administration, as it minimizes exposure to healthy tissues while maximizing the targeting of the tumor. Even slight misalignments can jeopardize treatment effectiveness, highlighting the need for stringent quality assurance measures and corrective interventions to uphold therapeutic precision.
Random error, which reflects unpredictable day-to-day variations in patient setup, was intentionally excluded from this study to maintain a focused evaluation of systematic errors, those consistent deviations that can be corrected with proper alignment protocols. Systematic error has a more direct impact on long-term dose delivery accuracy and treatment planning, as it affects every fraction in a similar way. Since our objective was to compare the precision of two auto-registration techniques in establishing consistent patient positioning across fractions, focusing solely on systematic error provided a clearer and more clinically relevant assessment of setup accuracy. Additionally, the limited sample size and uniform imaging protocol reduced the variability typically needed to analyze random error reliably.
2.5. Ethics Statement
This study was conducted in accordance with the ethical principles and adhered to all applicable national and institutional guidelines for human research. All patients included in this study provided written informed consent before participation, allowing the use of their anonymized imaging and treatment data for research and publication purposes. No additional procedures or interventions beyond routine clinical care were performed. The confidentiality and privacy of all patient information were strictly maintained throughout the study.
3. Results
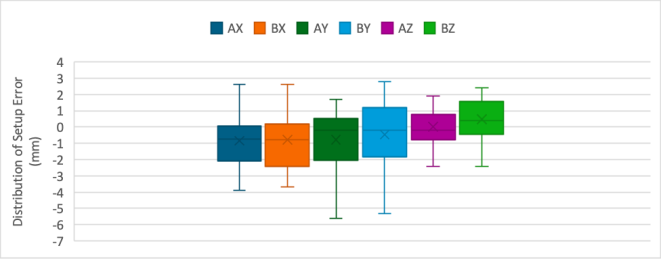
Box and Whiskers Plot illustrating the distribution of setup error between Method A and Method B across longitudinal (X), lateral (Y), and vertical (Z) axes. Shown in
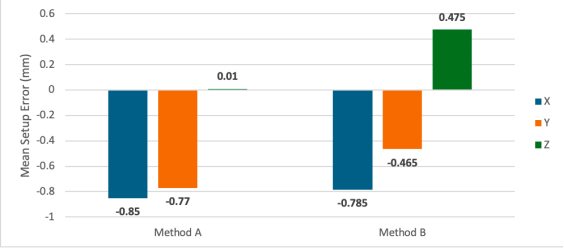
Figure 4. The analysis of the effects of two distinct auto-matching techniques on patient setup errors revealed both commonalities and divergences, with the findings illustrated through tables and graphs. (
Table 2) presents the mean systematic errors (Σ) in patient setup across three axes: Method A recorded a longitudinal direction (X) of -0.85 mm, a lateral direction (Y) of -0.77 mm, and a vertical direction (Z) of 0.01 mm, while Method B showed a longitudinal direction (X) of -0.785 mm, a lateral direction (Y) of -0.465 mm, and a vertical direction (Z) of 0.475 mm, as depicted in
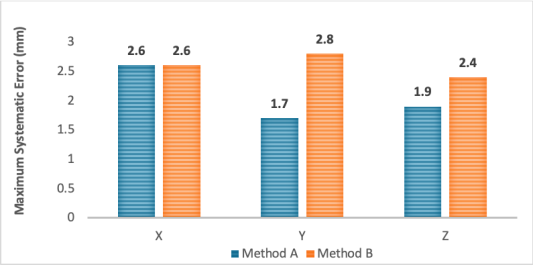
Figure 5. Method B exhibited a marginally lower mean systematic error compared to Method A in both the longitudinal (X) and lateral (Y) directions; however, this difference was not statistically significant (P > 0.05). In contrast, a statistically significant difference was identified in the mean systematic error between Method A (Σ = 0.01) and Method B (Σ = 0.475) in the vertical (Z) direction (P = 0.013*), indicating that Method A had a lower mean systematic error than Method B. The maximum errors were slightly lower in Method A than in Method B shown in
Figure 6.
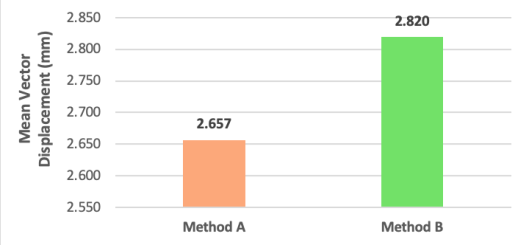
The average displacement vector outcomes were lower in Method A compared to Method B. Statistically, no significant difference was identified between the two methods (P > 0.05). (
Table 2) presents the results of paired samples t-tests conducted to evaluate the individual error components (X, Y, Z) for both Method A and Method B shown in
Figure 7. The analysis indicated no significant difference in the X-component errors between the two methods, t(19) = -0.831, p = 0.416. Likewise, the differences in Y-component errors did not reach significance, although a trend was observed, t(19) = -1.756, p = 0.095. Conversely, a statistically significant difference was noted in the Z-component errors, t(19) = -2.758, p = 0.013*, with Method A exhibiting lower error rates. (
Table 3) demonstrates the interdependence between Method A and Method B.
Furthermore, a multivariate analysis (Hotelling’s T
2 test) was performed to assess the overall impact of the error vector (X, Y, Z) between Method A and Method B across 20 patients. The findings indicated a test statistic of 2.3884, with 3 numerator degrees of freedom and 36 denominator degrees of freedom. The associated p-value was 0.5271, suggesting no significant difference in the overall effect of error components between the two methods (p > 0.05). Paired t-test was performed for the comparison between two auto matching methods A and B, to evaluate the P value for measured results using JAMOVI (version 2.3.28) software. A comprehensive summary of the results is presented in
Table 4.
Table 2. Comparison of systematic error (Σ) between two auto matching methods for head and neck cancer.
Setup Error | Mean (Method A) | Mean (Method B) | Mean Difference (A-B) | Std. Error | Sig. |
X (Lateral) | -0.85 | -0.785 | -0.065 | 0.0782 | 0.416NS |
Y (Longitudinal) | -0.77 | -0.465 | -0.305 | 0.1737 | 0.095NS (TREND) |
Z (Vertical) | 0.01 | 0.475 | -0.465 | 0.1686 | 0.013* |
X - Lateral, Y - Longitudinal, Z - Vertical, Σ - Systematic Error, * The mean difference is significant at the 0.05 level, NS - Non Significant, NS (TREND) - Non Significant, but shows a trend towards significance.
Table 3. Illustrating the dependency relationship between Method A and Method B.
Aspect | Method A | Method B | Dependency |
Initial Setup | Refines this initial setup using image registration | Used to position the patient close to treatment isocenter | Bone T&R depends on accurate initial crosswire setup to minimize correction magnitude |
Error Correction | Corrects for internal (bony) positional errors | Cannot detect internal misalignments | Bone T&R corrects the shortcomings of crosswire-only alignment |
Workflow Efficiency | Requires MVCT imaging and processing | Faster, requires no imaging | Crosswire helps reduce scan length and registration time by starting close to the target |
Use in Adaptive Therapy | Crucial | Not used | Adaptive workflows require precise registration; bone T&R is foundational |
Table 4. A detailed overview of the results.
Parameter | Axis / Component | Method A | Method B | Statistical Test / Value | p-value | Interpretation |
Mean Systematic Error (Σ) | Longitudinal (X) | −0.85 mm | −0.785 mm | Paired t-test | >0.05 | No significant difference |
| Lateral (Y) | −0.77 mm | −0.465 mm | Paired t-test | >0.05 | Comparable accuracy |
| Vertical (Z) | 0.01 mm | 0.475 mm | Paired t-test | 0.013* | Method A more accurate |
Average Displacement Vector | — | Lower in Method A | Higher in Method B | Paired t-test | >0.05 | No significant difference |
Maximum Error Magnitude | — | Slightly lower | Slightly higher | Descriptive comparison | — | Method A marginally better |
Paired Sample t-Test Results | X-component | — | — | t(19) = −0.831 | 0.416 | Not significant |
| Y-component | — | — | t(19) = −1.756 | 0.095 | Trend, not significant |
| Z-component | — | — | t(19) = −2.758 | 0.013* | Significant difference |
Multivariate Analysis (Hotelling’s T2) | Combined (X, Y, Z) | — | — | T2 = 2.3884 (df = 3,36) | 0.5271 | No significant overall difference |
Software Used | — | — | — | JAMOVI v2.3.28 | — | Statistical analysis platform |
Summary Interpretation | — | — | — | — | — | Method A showed lower mean and vertical errors; only Z-axis difference was statistically significant. |
Figure 4. Box and Whisker Plot showing setup error distribution for Method A and Method B across X (lateral), Y (longitudinal), and Z (vertical) axes.
** AX- The lateral direction offset shifts in Group A, AY- The longitudinal direction offset shifts in Group A, AZ- The vertical direction offset shifts in Group A, BX- The lateral direction offset shifts in Group B, BY- The longitudinal direction offset shifts in Group B, BZ- The vertical direction offset shifts in Group B.
Figure 5. Graphical depiction of the mean setup error in the lateral (X), longitudinal (Y), and vertical (Z) directions for both methods.
Figure 6. Represents a graphical depiction of the maximum systematic errors along the X, Y, and Z axes for both auto-registration techniques.
Figure 7. The figure illustrates the mean vector displacement for both Method A and Method B.
4. Discussion
Precise positioning of patients is crucial in image-guided radiotherapy (IGRT), particularly in anatomically intricate areas such as the head and neck. Method A exhibited a significantly reduced error in the vertical (Z) axis, Method B, which employs MVCT-based auto-matching, consistently showed lower errors in both the longitudinal (X) and lateral (Y) axes. These axes are especially important for head and neck cancers due to the closeness of dose-limiting organs like the spinal cord and parotid glands. Although the differences observed in the X and Y axes were not statistically significant, the persistent trend indicates enhanced spatial reliability with Method B.
The difference seen in the vertical (Z-axis) direction is important because it could affect radiation dose to nearby organs such as the spinal cord or brainstem. Even small vertical shifts can change how much dose these organs receive. The better vertical accuracy found with the bone-based method may therefore help reduce unwanted radiation to these sensitive areas. A multivariate analysis (Hotelling’s T2) revealed no significant overall difference between the two methods; however, from a clinical standpoint, the volumetric guidance and reproducibility offered by Method B render it more favorable. Consequently, Method B presents both practical and clinical benefits, advocating for its adoption as a standard method in head and neck IGRT.
Accurate image registration is critical for the safe and effective delivery of radiotherapy, particularly in image-guided treatments where Mega voltage Computed Tomography (MVCT) is used to align patients prior to radiation delivery. Among the various registration techniques, Cross Wire Matching (CWM), Bone Matching (BM), and Grey Scale Matching (GSM) have emerged as widely implemented methods. Each has unique benefits and limitations, but a growing body of evidence and clinical rationale supports the assertion that cross-wire matching (CWM) offers superior reliability, safety, and clinical utility, especially in high-precision treatment contexts. Method B is fundamentally a landmark-based registration technique, often utilizing visible anatomical structures such as vertebral bodies, dental restorations, or implanted fiducial markers. This method allows clinicians to manually align well-defined, reproducible reference points, which leads to high inter-fractional consistency. Unlike GSM, which is highly sensitive to image quality and susceptible to contrast variation, or BM, which performs well only in regions with clearly visible skeletal structures, Method B is less influenced by imaging artifacts or soft tissue deformations.
For example, in prostate radiotherapy, Hashido (2018) reported that manual registration using anatomical landmarks provided more reliable alignment compared to automatic registration, especially in the presence of anatomical variability such as rectal filling. This highlights the robustness of CWM under variable imaging conditions. One of the most compelling arguments for CWM is its alignment with the principle of “clinician oversight.” Unlike fully automated methods, CWM enables RTT’s to visually confirm and adjust alignment in real time. This reduces the risk of false-positive registrations
| [16] | Hashido T, Nakasone S, Fukao M, Ota S, Inoue S. Comparison between manual and automatic image registration in image-guided radiation therapy using megavoltage cone-beam computed tomography with an imaging beam line for prostate cancer. Radiol Phys Technol. 2018; 11(4): 392-405.
https://doi.org/10.1007/s12194-018-0476-z |
[16]
. Cao et al. (2019) noted that while grayscale methods could register soft tissues well, manual corrections based on anatomical landmarks were frequently required in thoracic tumors affected by respiratory motion. CWM, therefore, becomes the de facto safety net, allowing for trusted visual confirmation
| [17] | Cao X, Liu M, Zhai F, Li N, Bao C, Liu Y, et al. Comparison of different registration methods and landmarks for image-guided radiation therapy of pulmonary tumors. BMC Med Imaging. 2019; 19(1): 46. https://doi.org/10.1186/s12880-019-0343-3 |
[17]
. In high-precision treatments such as stereotactic body radiotherapy (SBRT) or stereotactic radiosurgery (SRS), sub-millimeter accuracy is non-negotiable. Here, even the most sophisticated automatic algorithms may falter under the demands of tight margins and dose escalation.
Mi et al. (2024) conducted a direct comparison between bone and tumor matching in carbon ion therapy for non-small cell lung cancer, concluding that tumor-based registration (analogous to GSM) was less stable in the presence of anatomical shifts, supporting the use of bone-based (and by extension, landmark-based) methods in critical alignments
| [18] | Mi J, Jia S, Chen L, Li Y, Sun J, Zhang L, et al. Bone matching versus tumor matching in image-guided carbon ion radiotherapy for locally advanced non-small cell lung cancer. Radiat Oncol. 2024; 19(1): 178.
https://doi.org/10.1186/s13014-024-02564-w |
[18]
. The AAPM Report by Brock et al. (2017) outlines the importance of matching the registration method to the clinical context and emphasizes that landmark-based methods remain essential for ensuring alignment integrity, particularly in high-risk or high-precision treatments
| [19] | Brock KK, Mutic S, McNutt TR, Li H, Kessler ML. Use of image registration and fusion algorithms and techniques in radiotherapy: Report of the AAPM Radiation Therapy Committee Task Group No. 132. Med Phys. 2017; 44(7): e43-e76. https://doi.org/10.1002/mp.12256 |
[19]
. Recent advances in artificial intelligence (AI) have further transformed registration strategies in image-guided radiotherapy. Deep-learning frameworks have been reported to significantly enhance registration accuracy, reduce inter-observer variability, and accelerate processing time without compromising clinical reliability
. AI-based CBCT-MVCT fusion models have demonstrated promising results in automated setup verification and dose recalculation workflows
| [21] | Neylon J, Luximon DC, Ritter T, Lamb JM. Proof-of-concept study of artificial intelligence-assisted review of CBCT image guidance. J Appl Clin Med Phys. 2023; 24(9): e14016.
https://doi.org/10.1002/acm2.14016 |
[21]
. Furthermore, the 2024 ESTRO-AAPM consensus underscores the importance of validation, interpretability, and clinician oversight in AI-driven registration systems to ensure safe integration into routine radiotherapy
| [22] | Hurkmans C, Bibault J-E, Brock KK, van Elmpt W, Feng M, Fuller CD, et al. A joint ESTRO and AAPM guideline for development, clinical validation and reporting of artificial intelligence models in radiation therapy. Radiotherapy Oncol. 2024; 197: 110345.
https://doi.org/10.1016/j.radonc.2024.110345 |
[22]
. Both auto registration techniques leads to improved treatment accuracy, reduced setup errors, and enhanced patient safety. By enabling precise alignment using stable anatomical landmarks or fiducial markers, Method B is especially crucial in stereotactic radiosurgery (SRS) and other high-precision modalities, where even sub-millimeter deviations can compromise dose delivery or increase toxicity. visual verification capability of this technique makes it indispensable in such critical treatments. Integrating both methods may offer an optimal balance between accuracy and efficiency. While Method A ensures superior vertical precision, Method B provides consistent lateral and longitudinal stability. A combined or hybrid registration strategy using automated MVCT-based alignment followed by manual verification with anatomical landmarks can enhance confidence in setup accuracy. This approach unites the speed of automation with clinician-guided precision, ultimately improving reproducibility, minimizing setup errors, and ensuring safer dose delivery in high-precision head and neck radiotherapy.
5. Conclusions
Both auto image registration techniques offers a unique blend of precision, resilience, and clinician control. Its reliance on reproducible anatomical features or implanted markers makes it highly reliable across treatment fractions, and its integration with human verification enhances clinical confidence and patient safety. Particularly in stereotactic and high-accuracy radiotherapy. Our recommendation is to initially employ Method A for gross anatomical image registration, which aims to reduce significant errors or offsets. This should be followed by Method B to obtain an estimate of precise alignment of the desired PTV area, thereby ensuring accurate dose delivery to the target region.
6. Limitations of the Study
This research has a number of limitations that need to be recognized. Firstly, the sample size was quite small (n = 20), which could restrict the statistical power and the applicability of the results. It is essential to conduct larger multi-institutional studies to confirm these findings across various patient demographics and treatment environments. Secondly, the study focused solely on cases of head and neck cancer, where bony landmarks and anatomical consistency are relatively well established. As a result, the findings may not be directly applicable to other anatomical areas, such as the thoracic or pelvic regions, where the movement of internal organs and variability in soft tissue are more significant.
Abbreviations
AAPM | American Association of Physicists in Medicine |
BM | Bone Matching |
CTV | Clinical Target Volume |
CWM | Cross Wire Matching |
CT | Computed Tomography |
DICOM | Digital Imaging and Communications in Medicine |
DOF | Degree of Freedom |
FFF | Flattening Filter Free |
GTV | Gross Tumor Volume |
GSM | Grey Scale Matching |
HNC | Head and Neck Cancer |
HT | Helical TomoTherapy |
IGRT | Image-Guided Radiotherapy |
IG-IMRT | Image-Guided Intensity Modulated Radiotherapy |
ICRU | International Commission on Radiation Units and Measurements |
IMRT | Intensity Modulated Radiotherapy |
MLC | Multileaf Collimator |
MVCT | Megavoltage Computed Tomography |
OAR | Organ at Risk |
PTV | Planning Target Volume |
QA | Quality Assurance |
RTT | Radiation Therapist |
SBRT | Stereotactic Body Radiotherapy |
SRS | Stereotactic Radiosurgery |
Σ (Sigma) | Systematic Error |
σ (Sigma) | Random Error |
X, Y, Z | Translational Axes (Longitudinal, Lateral, and Vertical Directions) |
Author Contributions
Subrata Roy: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing
Rajiv Kumar Singh: Formal Analysis, Software, Supervision, Validation, Writing – original draft, Writing – review & editing
Afnan Paikarathodi: Investigation, Methodology, Validation, Writing – review & editing
Sunil Maurya: Investigation, Methodology, Software, Validation
Anurag Luharia: Software, Supervision, Validation
Prashik Dube: Software, Writing – original draft, Writing – review & editing
Acknowledgments
The authors extend their sincere gratitude to the Department of Radiation Oncology and the Radiation Therapy team at our institution for their invaluable technical support and collaboration throughout the course of this study. We deeply appreciate the cooperation of all participating patients and the dedicated efforts of the Radiation Therapists who ensured the accuracy and consistency of data collection during treatment delivery. The authors also thank the medical physicists and oncologists whose expertise in image verification and data interpretation significantly enhanced the quality and integrity of this research.
Funding
This research did not obtain any specific grants from funding agencies in the public, commercial, or non-profit sectors.
Data Availability Statement
The data utilized to support the findings of this study can be requested from the corresponding author.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
| [1] |
Beaton L, Bandula S, Gaze MN, Sharma RA. How rapid advances in imaging are defining the future of precision radiation oncology. Br J Cancer. 2019; 120(8): 779-90.
https://doi.org/10.1038/s41416-019-0412-y
|
| [2] |
Department of Health and Social Care. Radiotherapy Services in England 2012. London: DHSC; 2012. Available from:
https://www.gov.uk/government/publications/radiotherapy-services-in-england-2012
|
| [3] |
Hanna TP, Shafiq J, Delaney GP, Vinod SK, Thompson SR, Barton MB. The population benefit of evidence-based radiotherapy: 5-year local control and overall survival benefits. Radiotherapy Oncol. 2018; 126(2): 191-7.
https://doi.org/10.1016/j.radonc.2017.11.004
|
| [4] |
British Institute of Radiology. Geometric Uncertainties in Daily Online IGRT: Updated Report. London: BIR; [cited 2025 Nov 1]. Available from:
https://www.bir.org.uk/publications/geometric-uncertainties.aspx
|
| [5] |
The Royal College of Radiologists, Institute of Physics and Engineering in Medicine, Society and College of Radiographers. On Target: Ensuring Geometric Accuracy in Radiotherapy. London: RCR; [cited 2025 Nov 1]. Available from:
https://www.rcr.ac.uk/publication/target-ensuring-geometric-accuracy-radiotherapy
|
| [6] |
Dawson LA, Jaffray DA. Advances in image-guided radiation therapy. J Clin Oncol. 2007; 25(8): 938-46.
https://doi.org/10.1200/JCO.2006.09.9515
|
| [7] |
Kupelian PA, Ramsey C, Meeks SL, Willoughby TR, Forbes A, Wagner TH, et al. Serial megavoltage CT imaging during external beam radiotherapy for non-small-cell lung cancer: Observations on tumor regression during treatment. Int J Radiat Oncol Biol Phys. 2005; 63(4): 1024-8.
https://doi.org/10.1016/j.ijrobp.2005.03.055
|
| [8] |
Yartsev S, Kron T, Cozzi L, Fogliata A, Bauman G. Tomotherapy planning of small brain tumours. Radiother Oncol. 2005; 74(1): 49-52.
https://doi.org/10.1016/j.radonc.2004.12.003
|
| [9] |
Langen KM, Meeks SL, Poole DO, Wagner TH, Willoughby TR, Kupelian PA, et al. The use of megavoltage CT (MVCT) images for dose recomputations. Phys Med Biol. 2005; 50(18): 4259-76.
https://doi.org/10.1088/0031-9155/50/18/001
|
| [10] |
Jeraj R, Mackie TR, Balog J, Olivera G, Pearson D, Kapatoes J, et al. Radiation characteristics of helical tomotherapy. Med Phys. 2004; 31(2): 396-404.
https://doi.org/10.1118/1.1639992
|
| [11] |
Jin S, Xu X, Su Z, Tang L, Zheng M, Liang P, Zhang H. MVCT image enhancement using reference-based encoder-decoder convolutional neural network. Expert Syst Appl. 2023; 241: 122576.
https://doi.org/10.1016/j.eswa.2023.122576
|
| [12] |
Van Herk M. Different styles of image-guided radiotherapy. Semin Radiat Oncol. 2007; 17(4): 258-67.
https://doi.org/10.1016/j.semradonc.2007.07.003
|
| [13] |
Verellen D, De Ridder M, Linthout N, Tournel K, Soete G, Storme G. Innovations in image-guided radiotherapy. Nat Rev Cancer. 2007; 7(12): 949-60.
https://doi.org/10.1038/nrc2288
|
| [14] |
Jarrett D, Stride E, Vallis K, Gooding MJ. Applications and limitations of machine learning in radiation oncology. Br J Radiol. 2019; 92(1100): 20190001.
https://doi.org/10.1259/bjr.20190001
|
| [15] |
Guo Y, Hao Z, Zhao S, Gong J, Yang F. Artificial intelligence in health care: Bibliometric analysis. J Med Internet Res. 2020; 22(7): e18228.
https://doi.org/10.2196/18228
|
| [16] |
Hashido T, Nakasone S, Fukao M, Ota S, Inoue S. Comparison between manual and automatic image registration in image-guided radiation therapy using megavoltage cone-beam computed tomography with an imaging beam line for prostate cancer. Radiol Phys Technol. 2018; 11(4): 392-405.
https://doi.org/10.1007/s12194-018-0476-z
|
| [17] |
Cao X, Liu M, Zhai F, Li N, Bao C, Liu Y, et al. Comparison of different registration methods and landmarks for image-guided radiation therapy of pulmonary tumors. BMC Med Imaging. 2019; 19(1): 46.
https://doi.org/10.1186/s12880-019-0343-3
|
| [18] |
Mi J, Jia S, Chen L, Li Y, Sun J, Zhang L, et al. Bone matching versus tumor matching in image-guided carbon ion radiotherapy for locally advanced non-small cell lung cancer. Radiat Oncol. 2024; 19(1): 178.
https://doi.org/10.1186/s13014-024-02564-w
|
| [19] |
Brock KK, Mutic S, McNutt TR, Li H, Kessler ML. Use of image registration and fusion algorithms and techniques in radiotherapy: Report of the AAPM Radiation Therapy Committee Task Group No. 132. Med Phys. 2017; 44(7): e43-e76.
https://doi.org/10.1002/mp.12256
|
| [20] |
Teuwen J, Gouw ZAR, Sonke JJ. Artificial intelligence for image registration in radiation oncology. Semin Radiat Oncol. 2022; 32(4): 330-342.
https://doi.org/10.1016/j.semradonc.2022.06.003
|
| [21] |
Neylon J, Luximon DC, Ritter T, Lamb JM. Proof-of-concept study of artificial intelligence-assisted review of CBCT image guidance. J Appl Clin Med Phys. 2023; 24(9): e14016.
https://doi.org/10.1002/acm2.14016
|
| [22] |
Hurkmans C, Bibault J-E, Brock KK, van Elmpt W, Feng M, Fuller CD, et al. A joint ESTRO and AAPM guideline for development, clinical validation and reporting of artificial intelligence models in radiation therapy. Radiotherapy Oncol. 2024; 197: 110345.
https://doi.org/10.1016/j.radonc.2024.110345
|
Cite This Article
-
APA Style
Roy, S., Singh, R. K., Paikarathodi, A., Maurya, S., Luharia, A., et al. (2025). An Analytical Comparison of Two Daily Pre-Treatment Image Verification Approaches Utilizing Radixact™ Tomotherapy-Based Megavoltage Computed Tomography for Head and Neck Cancer Patients. Journal of Cancer Treatment and Research, 13(4), 153-163. https://doi.org/10.11648/j.jctr.20251304.17
 Copy
|
Copy
|
 Download
Download
ACS Style
Roy, S.; Singh, R. K.; Paikarathodi, A.; Maurya, S.; Luharia, A., et al. An Analytical Comparison of Two Daily Pre-Treatment Image Verification Approaches Utilizing Radixact™ Tomotherapy-Based Megavoltage Computed Tomography for Head and Neck Cancer Patients. J. Cancer Treat. Res. 2025, 13(4), 153-163. doi: 10.11648/j.jctr.20251304.17
Copy
|
Download
AMA Style
Roy S, Singh RK, Paikarathodi A, Maurya S, Luharia A, et al. An Analytical Comparison of Two Daily Pre-Treatment Image Verification Approaches Utilizing Radixact™ Tomotherapy-Based Megavoltage Computed Tomography for Head and Neck Cancer Patients. J Cancer Treat Res. 2025;13(4):153-163. doi: 10.11648/j.jctr.20251304.17
Copy
|
Download
-
@article{10.11648/j.jctr.20251304.17,
author = {Subrata Roy and Rajiv Kumar Singh and Afnan Paikarathodi and Sunil Maurya and Anurag Luharia and Prashik Dube},
title = {An Analytical Comparison of Two Daily Pre-Treatment Image Verification Approaches Utilizing Radixact™ Tomotherapy-Based Megavoltage Computed Tomography for Head and Neck Cancer Patients},
journal = {Journal of Cancer Treatment and Research},
volume = {13},
number = {4},
pages = {153-163},
doi = {10.11648/j.jctr.20251304.17},
url = {https://doi.org/10.11648/j.jctr.20251304.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jctr.20251304.17},
abstract = {Introduction: Ensuring accurate patient setup is crucial in radiotherapy for head and neck cancer (HNC) due to the intricate anatomy and the closeness to vital organs. This study aimed to assess and compare the effectiveness of two different daily pre-treatment auto image registration techniques utilizing Radixact TomoTherapy-based megavoltage computed tomography (MVCT) to enhance setup accuracy and treatment consistency. Materials and Methods: A prospective analysis was performed on a cohort of twenty HNC patients undergoing treatment with Radixact TomoTherapy. Two image verification techniques were assessed: one focused on aligning bony anatomy (Method A) and the other on adjusting the cross-wire at the center of the planning target volume (PTV) for automatic registration (Method B). Daily MVCT images were taken and analyzed to determine translational setup corrections, which were documented for further analysis. Results: Method B exhibited slightly lower mean systematic errors in both the longitudinal and lateral directions, although the differences were not statistically significant. Method A demonstrated significantly lower errors in the vertical (Z-axis) direction (p = 0.013). Overall displacement vectors favored Method A, yet multivariate analysis indicated no significant difference between the two methods. Therefore, both methods were found to perform similarly, with Method A showing superior vertical alignment. Conclusions: Both auto image registration techniques provide accuracy and dependability, bolstered by reproducible anatomy and clinician supervision. For optimal precision, Method A is suggested for initial gross alignment, followed by Method B for fine-tuning around the target volume, thereby improving dose precision and safety in high-accuracy radiotherapy treatments. Key Messages: Combining initial alignment with Method A and refinement with Method B enhances precision and safety in head and neck radiotherapy, optimizing setup accuracy using Radixact TomoTherapy MVCT imaging.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - An Analytical Comparison of Two Daily Pre-Treatment Image Verification Approaches Utilizing Radixact™ Tomotherapy-Based Megavoltage Computed Tomography for Head and Neck Cancer Patients
AU - Subrata Roy
AU - Rajiv Kumar Singh
AU - Afnan Paikarathodi
AU - Sunil Maurya
AU - Anurag Luharia
AU - Prashik Dube
Y1 - 2025/12/19
PY - 2025
N1 - https://doi.org/10.11648/j.jctr.20251304.17
DO - 10.11648/j.jctr.20251304.17
T2 - Journal of Cancer Treatment and Research
JF - Journal of Cancer Treatment and Research
JO - Journal of Cancer Treatment and Research
SP - 153
EP - 163
PB - Science Publishing Group
SN - 2376-7790
UR - https://doi.org/10.11648/j.jctr.20251304.17
AB - Introduction: Ensuring accurate patient setup is crucial in radiotherapy for head and neck cancer (HNC) due to the intricate anatomy and the closeness to vital organs. This study aimed to assess and compare the effectiveness of two different daily pre-treatment auto image registration techniques utilizing Radixact TomoTherapy-based megavoltage computed tomography (MVCT) to enhance setup accuracy and treatment consistency. Materials and Methods: A prospective analysis was performed on a cohort of twenty HNC patients undergoing treatment with Radixact TomoTherapy. Two image verification techniques were assessed: one focused on aligning bony anatomy (Method A) and the other on adjusting the cross-wire at the center of the planning target volume (PTV) for automatic registration (Method B). Daily MVCT images were taken and analyzed to determine translational setup corrections, which were documented for further analysis. Results: Method B exhibited slightly lower mean systematic errors in both the longitudinal and lateral directions, although the differences were not statistically significant. Method A demonstrated significantly lower errors in the vertical (Z-axis) direction (p = 0.013). Overall displacement vectors favored Method A, yet multivariate analysis indicated no significant difference between the two methods. Therefore, both methods were found to perform similarly, with Method A showing superior vertical alignment. Conclusions: Both auto image registration techniques provide accuracy and dependability, bolstered by reproducible anatomy and clinician supervision. For optimal precision, Method A is suggested for initial gross alignment, followed by Method B for fine-tuning around the target volume, thereby improving dose precision and safety in high-accuracy radiotherapy treatments. Key Messages: Combining initial alignment with Method A and refinement with Method B enhances precision and safety in head and neck radiotherapy, optimizing setup accuracy using Radixact TomoTherapy MVCT imaging.
VL - 13
IS - 4
ER -
Copy
|
Download