Neurocysticercosis is a parasitic infestation of the central nervous system caused by larva of the helminth Taenia solium. It is a relatively uncommon aetiology for seizures with varying presentations which are dependent on the stage of the cyst, its location and the immune response of the host. Incidence is rising in developing countries due to renewed interest in piggery. Associated risk factors include poor sanitary condition, rearing pigs or consumption of pork meat and overcrowded living conditions. Diagnostic yield has improved in recent years following relative improved health care seeking attitude, availability of neuroimaging modalities such as cranial magnetic resonance imaging and pathologic analysis of resected tissue specimen. Though prevalence has been domiciled in rural and suburban communities, an increase in global transmigration of individuals has led to some incidence in developed counties. The advent of cysticidal therapy which is complementary to surgical resection of symptomatic lesions has helped improve the prognosis and attenuate disease progression in these patients while improving clinical outcomes of treatment. We present a 23-year-old male patient with adult onset seizures who had neuroimaging and brain biopsy with histopathologic diagnosis of neurocysticercosis. The disease should be entertained in a patient with adult onset seizure residing in a potentially endemic area. We also encourage multidisciplinary management for optimal outcome.
| Published in | Journal of Surgery (Volume 13, Issue 1) |
| DOI | 10.11648/j.js.20251301.15 |
| Page(s) | 32-36 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Neurocysticercosis, Adult Onset Seizures, Poor Sanitary Conditions
MRI | Magnetic Resonance Imaging |
FLAIR | Fluid Attenuated Inversion Recovery |
| [1] | Ojo O. A, Onyia C. U, Lawal B. O, Awolowo N. A. Neurocysticercosis in a Nigerian woman -missed diagnosis of a neglected disease and surgical management. World Neurosurgery: X, Volume 23, 2024, 100380, |
| [2] | Garcia HH. Parasitic Infections of the Nervous System. Continuum (Minneap Minn). 2021 Aug 1; 27(4): 943-962. |
| [3] | Del Brutto OH, Santibáñez R, Idrovo L, Rodrìguez S, Díaz-Calderón E, Navas C, Gilman RH, Cuesta F, Mosquera A, Gonzalez AE, Tsang VC, García HH. Epilepsy and neurocysticercosis in Atahualpa: a door-to-door survey in rural coastal Ecuador. Epilepsia. 2005 Apr; 46(4): 583-7. |
| [4] | Owolabi LF, Owolabi SD, Adamu B, Jibo AM, Alhaji ID. Epilepsy treatment gap in Sub-Saharan Africa: Meta-analysis of community-based studies. Acta Neurol Scand. 2020 Jul; 142(1): 3-13. |
| [5] | Ndimubanzi PC, Carabin H, Budke CM, Nguyen H, Qian YJ, Rainwater E, Dickey M, Reynolds S, Stoner JA. A systematic review of the frequency of neurocyticercosis with a focus on people with epilepsy. PLoS Negl Trop Dis. 2010 Nov 2; 4(11): e870. |
| [6] |
WHO: taeniasis/cysticercosis (2020). Accessed: November 25, 2021:
https://www.who.int/en/news-room/factsheets/detail/taeniasis-cysticercosis |
| [7] | Nash T. Edema surrounding calcified intracranial cysticerci: clinical manifestations, natural history, and treatment. Pathog Glob Health. 2012 Sep; 106(5): 275-9. |
| [8] | García HH, Gonzalez AE, Evans CA, Gilman RH; Cysticercosis Working Group in Peru. Taenia solium cysticercosis. Lancet. 2003 Aug 16; 362(9383): 547-56. |
| [9] | Medina, M. T. and Christopher M DeGiorgio. “Introduction to neurocysticercosis: a worldwide epidemic.” Neurosurgical Focus 12 (2002): 1-1. |
| [10] | Sharma BS, Banerjee AK, Kak VK. Intramedullary spinal cysticercosis. Case report and review of literature. Clin Neurol Neurosurg. 1987; 89(2): 111-6. |
| [11] | Joubert J. Cysticercal meningitis--a pernicious form of neurocysticercosis which responds poorly to praziquantel. S Afr Med J. 1990 May 19; 77(10): 528-30. |
| [12] | Apuzzo, Michael L. J., William R. Dobkin, Chi-Shing Zee, Jyc Chan, Steven Giannotta and Martin H. Weiss. “Surgical considerations in treatment of intraventricular cysticercosis. An analysis of 45 cases.” Journal of neurosurgery 60 2(1984): 400-7. |
| [13] | Melki J, Koffi E, Boka M, Touré A, Soumahoro MK, Jambou R. Taenia solium cysticercosis in West Africa: status update. Parasite. 2018; 25: 49. |
| [14] | Sinha S, Sharma BS. Neurocysticercosis: a review of current status and management. J Clin Neurosci. 2009; 16(7): 867-76. |
| [15] | Tsang VC, Brand JA, Boyer AE. An enzyme-linked immunoelectrotransfer blot assay and glycoprotein antigens for diagnosing human cysticercosis (Taenia solium). J Infect Dis. 1989 Jan; 159(1): 50-9. |
| [16] | White AC Jr, Coyle CM, Rajshekhar V, Singh G, Hauser WA, Mohanty A, Garcia HH, Nash TE. Diagnosis and Treatment of Neurocysticercosis: 2017 Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA) and the American Society of Tropical Medicine and Hygiene (ASTMH). Clin Infect Dis. 2018 Apr 3; 66(8): e49-e75. |
| [17] | Del Brutto OH, Nash TE, White AC Jr, Rajshekhar V, Wilkins PP, Singh G, Vasquez CM, Salgado P, Gilman RH, Garcia HH. Revised diagnostic criteria for neurocysticercosis. J Neurol Sci. 2017 Jan 15; 372: 202-210. |
| [18] | Carpio A. Neurocysticercosis: an update. Lancet Infect Dis. 2002 Dec; 2(12): 751-62. |
| [19] | Sharma M, Singh T, Mathew A. Antiepileptic drugs for seizure control in people with neurocysticercosis. Cochrane Database Syst Rev. 2015 Oct 12; (10): CD009027. |
| [20] | Singhi PD, Dinakaran J, Khandelwal N, Singhi SC. One vs. two years of anti-epileptic therapy in children with single small enhancing CT lesions. J Trop Pediatr. 2003 Oct; 49(5): 274-8. |
APA Style
Azode, K. M., Olasode, B. J., Komolafe, E. O. (2025). Neurocysticercosis: A Case of an Unusual Cause of Seizures. Journal of Surgery, 13(1), 32-36. https://doi.org/10.11648/j.js.20251301.15
ACS Style
Azode, K. M.; Olasode, B. J.; Komolafe, E. O. Neurocysticercosis: A Case of an Unusual Cause of Seizures. J. Surg. 2025, 13(1), 32-36. doi: 10.11648/j.js.20251301.15
AMA Style
Azode KM, Olasode BJ, Komolafe EO. Neurocysticercosis: A Case of an Unusual Cause of Seizures. J Surg. 2025;13(1):32-36. doi: 10.11648/j.js.20251301.15
@article{10.11648/j.js.20251301.15,
author = {Kelechi Michael Azode and Babatunde Josiah Olasode and Edward Oluwole Komolafe},
title = {Neurocysticercosis: A Case of an Unusual Cause of Seizures
},
journal = {Journal of Surgery},
volume = {13},
number = {1},
pages = {32-36},
doi = {10.11648/j.js.20251301.15},
url = {https://doi.org/10.11648/j.js.20251301.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.js.20251301.15},
abstract = {Neurocysticercosis is a parasitic infestation of the central nervous system caused by larva of the helminth Taenia solium. It is a relatively uncommon aetiology for seizures with varying presentations which are dependent on the stage of the cyst, its location and the immune response of the host. Incidence is rising in developing countries due to renewed interest in piggery. Associated risk factors include poor sanitary condition, rearing pigs or consumption of pork meat and overcrowded living conditions. Diagnostic yield has improved in recent years following relative improved health care seeking attitude, availability of neuroimaging modalities such as cranial magnetic resonance imaging and pathologic analysis of resected tissue specimen. Though prevalence has been domiciled in rural and suburban communities, an increase in global transmigration of individuals has led to some incidence in developed counties. The advent of cysticidal therapy which is complementary to surgical resection of symptomatic lesions has helped improve the prognosis and attenuate disease progression in these patients while improving clinical outcomes of treatment. We present a 23-year-old male patient with adult onset seizures who had neuroimaging and brain biopsy with histopathologic diagnosis of neurocysticercosis. The disease should be entertained in a patient with adult onset seizure residing in a potentially endemic area. We also encourage multidisciplinary management for optimal outcome.
},
year = {2025}
}
TY - JOUR T1 - Neurocysticercosis: A Case of an Unusual Cause of Seizures AU - Kelechi Michael Azode AU - Babatunde Josiah Olasode AU - Edward Oluwole Komolafe Y1 - 2025/02/20 PY - 2025 N1 - https://doi.org/10.11648/j.js.20251301.15 DO - 10.11648/j.js.20251301.15 T2 - Journal of Surgery JF - Journal of Surgery JO - Journal of Surgery SP - 32 EP - 36 PB - Science Publishing Group SN - 2330-0930 UR - https://doi.org/10.11648/j.js.20251301.15 AB - Neurocysticercosis is a parasitic infestation of the central nervous system caused by larva of the helminth Taenia solium. It is a relatively uncommon aetiology for seizures with varying presentations which are dependent on the stage of the cyst, its location and the immune response of the host. Incidence is rising in developing countries due to renewed interest in piggery. Associated risk factors include poor sanitary condition, rearing pigs or consumption of pork meat and overcrowded living conditions. Diagnostic yield has improved in recent years following relative improved health care seeking attitude, availability of neuroimaging modalities such as cranial magnetic resonance imaging and pathologic analysis of resected tissue specimen. Though prevalence has been domiciled in rural and suburban communities, an increase in global transmigration of individuals has led to some incidence in developed counties. The advent of cysticidal therapy which is complementary to surgical resection of symptomatic lesions has helped improve the prognosis and attenuate disease progression in these patients while improving clinical outcomes of treatment. We present a 23-year-old male patient with adult onset seizures who had neuroimaging and brain biopsy with histopathologic diagnosis of neurocysticercosis. The disease should be entertained in a patient with adult onset seizure residing in a potentially endemic area. We also encourage multidisciplinary management for optimal outcome. VL - 13 IS - 1 ER -
Neurosurgery Unit, Department of Surgery, Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria
Department of Morbid Anatomy and Forensic Medicine, Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria
Neurosurgery Unit, Department of Surgery, Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria
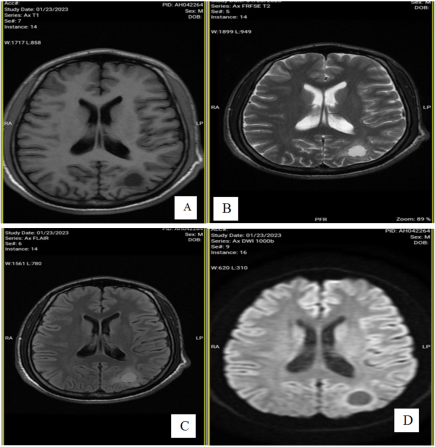
Figure 1. Axial MRI images of the patient with showing a well circumscribed oval shaped lesion in the left occipital lobe. (A) T1 Image showing isointensity of the lesion. (B) T2 image showing hyperintensity. (C) T2 FLAIR image showing increased signal intensity. (D) Diffusion weighted image showing an area of restricted diffusion occupied by the lesion.
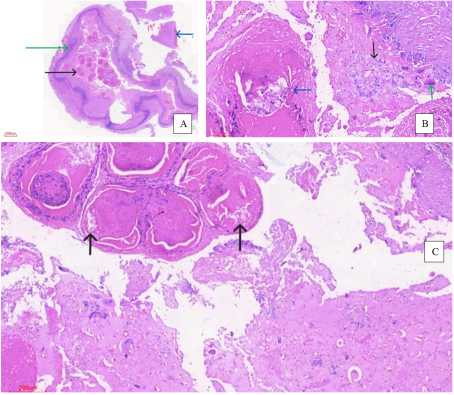
Figure 2. Histology slides of the resected brain specimen. (A) Green arrow shows cyst wall, black arrow shows parasite, blue arrow shows brain tissue. (B) Black arrow shows foamy macrophages, green arrow shows giant cells, blue arrow shows parasite. (C) Black arrows show parasite structures reminiscent of hooklets.
Information

