A unicornuate uterus is a rare congenital Müllerian anomaly resulting from incomplete development of one Müllerian duct and accounts for approximately 2-13% of all uterine malformations. This anomaly is associated with a wide range of adverse reproductive outcomes, including recurrent pregnancy loss, ectopic pregnancy, preterm birth, malpresentation, fetal growth restriction, and increased rates of operative delivery. Consequently, pregnancies in women with a unicornuate uterus are categorized as high risk and require careful antenatal surveillance and individualized obstetric management. We report the case of a 29-year-old woman with a term breech pregnancy at 40 weeks and 1 day of gestation who presented in active labor and underwent emergency lower segment cesarean section. Intraoperatively, a right-sided unicornuate uterus with a non-communicating rudimentary horn was incidentally identified. The ipsilateral fallopian tube and ovary were normal, while the contralateral adnexa were attached to the rudimentary horn. A healthy female neonate weighing 3.0 kg was delivered with an immediate cry. The postoperative period was uneventful, and both maternal and neonatal outcomes were favorable. This case demonstrates that successful term pregnancy is achievable in women with a unicornuate uterus despite inherent obstetric risks. It underscores the importance of maintaining a high index of suspicion for uterine anomalies in women presenting with recurrent malpresentation or adverse obstetric history and highlights the role of vigilant antenatal monitoring and tailored obstetric care in optimizing outcomes.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Congenital uterine anomalies arise due to abnormal formation, fusion, or resorption of the Müllerian ducts during embryogenesis, typically between the sixth and twelfth weeks of gestation. These anomalies represent an important cause of reproductive morbidity. While many affected women remain asymptomatic, such anomalies are frequently detected during evaluation for infertility, recurrent pregnancy loss, or adverse obstetric outcomes. The reported prevalence ranges from 1-10% in the general population and is significantly higher among women with infertility or recurrent miscarriage
[1]
Chan YY, Jayaprakasan K, Tan A, Thornton JG, Coomarasamy A, Raine-Fenning NJ. Reproductive outcomes in women with congenital uterine anomalies: a systematic review. Ultrasound Obstet Gynecol. 2011; 38: 371-82.
[2]
Chan YY, Jayaprakasan K, Zamora J, Thornton JG, Raine-Fenning NJ, Coomarasamy A. The prevalence of congenital uterine anomalies in unselected and high-risk populations. Hum Reprod Update. 2011; 17: 761-71.
[1, 2]
.
A unicornuate uterus is an uncommon Müllerian duct anomaly resulting from partial or complete failure of development of one Müllerian duct. It accounts for approximately 2.3-13.2% of all uterine malformations
[3]
Reichman D, Laufer MR, Robinson BK. Pregnancy outcomes in unicornuate uteri: a review. Fertil Steril. 2009; 91: 1886-94.
[4]
Hua M, Odibo AO, Longman RE, Macones GA, Roehl KA, Cahill AG. Congenital uterine anomalies and adverse pregnancy outcomes. Am J Obstet Gynecol. 2011; 205: 558. e1-5.
[5]
Fedele L, Zamberletti D, Vercellini P, Dorta M, Candiani GB. Reproductive performance of women with unicornuate uterus. Fertil Steril. 1987; 47: 416-9.
[6]
Grimbizis GF, et al. Clinical implications of congenital uterine anomalies. Reprod Biomed Online. 2014; 29: 665-83.
[3-6]
. Depending on the extent of development of the contralateral duct, a rudimentary horn may be present, which may be communicating, non-communicating, or absent. The presence and type of rudimentary horn have important clinical implications and significantly influence obstetric risk.
The reduced uterine cavity, abnormal myometrial architecture, and compromised uteroplacental circulation associated with a unicornuate uterus predispose affected women to miscarriage, ectopic pregnancy, preterm labor, malpresentation, fetal growth restriction, and increased rates of cesarean delivery
[3]
Reichman D, Laufer MR, Robinson BK. Pregnancy outcomes in unicornuate uteri: a review. Fertil Steril. 2009; 91: 1886-94.
[4]
Hua M, Odibo AO, Longman RE, Macones GA, Roehl KA, Cahill AG. Congenital uterine anomalies and adverse pregnancy outcomes. Am J Obstet Gynecol. 2011; 205: 558. e1-5.
[5]
Fedele L, Zamberletti D, Vercellini P, Dorta M, Candiani GB. Reproductive performance of women with unicornuate uterus. Fertil Steril. 1987; 47: 416-9.
[6]
Grimbizis GF, et al. Clinical implications of congenital uterine anomalies. Reprod Biomed Online. 2014; 29: 665-83.
[7]
Raga F, et al. Reproductive impact of congenital Müllerian anomalies. Fertil Steril. 1997; 68: 689-96.
[3-7]
. Pregnancy occurring within a non-communicating rudimentary horn carries an extremely high risk of uterine rupture, often occurring in the second trimester and leading to catastrophic hemorrhage.
Despite these risks, successful pregnancies, including term deliveries, have been reported, particularly when gestation occurs within the well-developed uterine horn. Due to the rarity of this condition and heterogeneity in clinical outcomes, individual case reports remain valuable for expanding understanding of clinical behavior and refining obstetric management strategies.
These anatomical limitations explain the high incidence of early pregnancy loss, fetal growth restriction, and preterm delivery reported in the literature
[3]
Reichman D, Laufer MR, Robinson BK. Pregnancy outcomes in unicornuate uteri: a review. Fertil Steril. 2009; 91: 1886-94.
[6]
Grimbizis GF, et al. Clinical implications of congenital uterine anomalies. Reprod Biomed Online. 2014; 29: 665-83.
[15]
Jayaprakasan K, et al. Uterine anomalies and early pregnancy outcome. Ultrasound Obstet Gynecol. 2011; 37: 727-32.
[16]
Venetis CA, et al. Clinical implications of congenital uterine anomalies. Reprod Biomed Online. 2014; 29: 665-83.
[3, 6, 15, 16]
.
2. Case Report
2.1. Patient Information
A 29-year-old unbooked woman, gravida 4 para 1 living 1 abortion 2 (G4P1L1A2), at 30 weeks and 1 day of gestation, presented to the outpatient department for routine antenatal evaluation. She had a history of one previous lower segment cesarean section.
2.2. Obstetric History
Her first pregnancy, ten years earlier, resulted in an emergency cesarean section for breech presentation at a government hospital in Uttar Pradesh, leading to the delivery of a healthy female infant. Operative records were unavailable, and it was unclear whether a uterine anomaly had been noted during that procedure.
She subsequently experienced two spontaneous first-trimester abortions occurring nine and eight years earlier, respectively. Both resolved without surgical intervention.
2.3. Antenatal Course and Investigations
The patient was registered for antenatal care at our institution. Ultrasonography performed at 31 weeks and 5 days of gestation demonstrated a singleton fetus in persistent breech presentation with no gross congenital anomalies. Amniotic fluid volume was adequate. In view of breech presentation in a previously scarred uterus, an elective repeat cesarean section was planned.
However, the patient was lost to follow-up and presented later at 40 weeks and 1 day of gestation in active labor. On admission, she was afebrile and hemodynamically stable. Abdominal examination revealed a longitudinal lie with breech presentation and rightward deviation of the uterus. Cardiotocography showed a reactive non-stress test. Routine laboratory investigations were within normal limits.
2.3.1. Risk Stratification and Antenatal Considerations
Pregnancies occurring in women with congenital uterine anomalies should be classified as high risk due to increased maternal and fetal morbidity. Risk stratification should include assessment of obstetric history, uterine morphology, placental location, and fetal growth patterns. Serial ultrasonographic surveillance is recommended to monitor fetal growth and amniotic fluid volume, as uteroplacental insufficiency is frequently reported in unicornuate uterus
[12]
American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 12. Obstet Gynecol. 2000; 95 (Suppl): 1-12.
[16]
Venetis CA, et al. Clinical implications of congenital uterine anomalies. Reprod Biomed Online. 2014; 29: 665-83.
[12, 16]
. Cervical length assessment may be considered in selected cases because of an increased risk of preterm birth, although evidence regarding prophylactic cerclage remains inconclusive.
2.3.2. Labor Assessment and Decision-making
At presentation in active labor at 40 weeks and 1 day of gestation, the patient was assessed comprehensively with special consideration to her previous cesarean section and persistent breech presentation. Clinical examination revealed a rightward deviation of the gravid uterus, which retrospectively may indicate an underlying uterine anomaly. Given the presence of a previously scarred uterus, breech presentation, and advanced labor, vaginal birth after cesarean section was considered inappropriate. Hence, the decision for emergency lower segment cesarean section was made to ensure optimal maternal and fetal safety.
2.4. Therapeutic Intervention and Intraoperative Findings
An emergency lower segment cesarean section was performed under spinal anesthesia. Intraoperatively, a right-sided unicornuate uterus was identified with a left non-communicating rudimentary horn. The ipsilateral fallopian tube and ovary were normal, while the contralateral adnexa were attached to the rudimentary horn and displaced inferiorly.
A live female neonate weighing 3.0 kg was delivered with an immediate cry. The uterus was closed in two layers without difficulty, and no postpartum hemorrhage occurred. The patient declined sterilization after counseling.
2.5. Postoperative Course
Postoperative recovery was uneventful. Breastfeeding was initiated successfully. Both mother and neonate were discharged on postoperative day four in stable condition.
Differential Diagnosis
The differential diagnosis included other congenital Müllerian duct anomalies, particularly bicornuate uterus and uterus didelphys. A bicornuate uterus is characterized by a deep central fundal cleft and two symmetric uterine horns, while uterus didelphys involves complete duplication of uterine cavities and cervices.
In the present case, intraoperative findings demonstrated a single asymmetric uterine cavity with one fully developed horn and a contralateral rudimentary horn without cervical duplication, confirming the diagnosis of unicornuate uterus. Other conditions such as hydrosalpinx or adnexal masses were excluded.
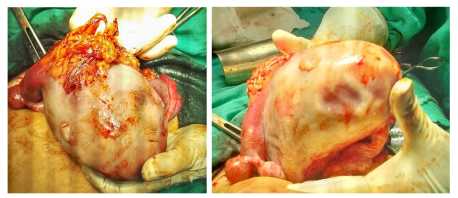
Figure 1. Intraoperative photograph showing a right-sided Unicornuate uterus (U) with a left non-communicating rudimentary horn (RH). The ipsilateral adnexa appear normal, while the contralateral adnexa are attached to the rudimentary horn.
3. Outcome and Follow-up
Both maternal and neonatal outcomes were favorable. The patient was counseled regarding the implications of the uterine anomaly for future pregnancies and advised early antenatal registration, close surveillance, and planned delivery in a tertiary care center.
4. Discussion
Unicornuate uterus is associated with significantly impaired reproductive outcomes, although rare cases of successful singleton and even twin pregnancies have been reported in the literature
[3]
Reichman D, Laufer MR, Robinson BK. Pregnancy outcomes in unicornuate uteri: a review. Fertil Steril. 2009; 91: 1886-94.
[6]
Grimbizis GF, et al. Clinical implications of congenital uterine anomalies. Reprod Biomed Online. 2014; 29: 665-83.
[9]
Nanda S, et al. Successful twin pregnancy in a unicornuate uterus. Arch Gynecol Obstet. 2009; 280: 993-5.
[3, 6, 9]
.
Clinical presentation varies widely. Some women present in adolescence with dysmenorrhea or chronic pelvic pain, particularly if a functional rudimentary horn is present, whereas others remain asymptomatic until pregnancy. Diagnosis often requires advanced imaging modalities such as three-dimensional ultrasonography or magnetic resonance imaging, which provide superior anatomical delineation
[8]
Khati NJ, et al. Unicornuate uterus and its variants. J Ultrasound Med. 2012; 31: 319-31.
[14]
Grimbizis GF, Campo R. Congenital malformations of the female genital tract. Hum Reprod. 2010; 25: 546-53.
[17]
Woelfer B, et al. Reproductive outcomes with uterine anomalies. Obstet Gynecol. 2001; 98: 1099-1103.
[8, 14, 17]
.
Pregnancy in a non-communicating rudimentary horn is associated with rupture rates ranging from 50-90%, typically occurring during the second trimester, and carries substantial maternal morbidity
[10]
Amritha B, et al. Ruptured rudimentary horn pregnancy. J Med Case Rep. 2012; 6: 102.
. Early diagnosis and surgical excision of a functional rudimentary horn are therefore recommended when identified antenatally.
In contrast, management of an asymptomatic rudimentary horn identified incidentally during cesarean section remains controversial. There are no standardized guidelines advocating routine excision, and conservative management may be considered in carefully selected women desiring future fertility
[13]
Bodur S, et al. Unicornuate uterus diagnosed at third cesarean section. Pak J Med Sci. 2017; 33: 779-81.
. Meta-analyses confirm poorer reproductive outcomes in women with unicornuate uterus compared with those having normal uterine anatomy
[16]
Venetis CA, et al. Clinical implications of congenital uterine anomalies. Reprod Biomed Online. 2014; 29: 665-83.
[18]
Rackow BW, Arici A. Reproductive performance in Müllerian anomalies. Curr Opin Obstet Gynecol. 2007; 19: 229-37.
[20]
Reichman D, Laufer MR. Congenital uterine anomalies affecting reproduction. Best Pract Res Clin Obstet Gynaecol. 2010; 24: 193-208.
[16, 18, 20]
.
The presence of a rudimentary horn plays a critical role in determining clinical outcomes. Functional non-communicating rudimentary horns pose a significant risk of hematometra, endometriosis, and ectopic pregnancy, while pregnancies within such horns are associated with extremely high rupture rates and maternal mortality if not diagnosed early
[10]
Amritha B, et al. Ruptured rudimentary horn pregnancy. J Med Case Rep. 2012; 6: 102.
. As a result, prophylactic excision of a functional rudimentary horn is generally recommended when identified outside pregnancy; however, management decisions must be individualized when diagnosis occurs incidentally during cesarean section.
Long-term reproductive outcomes in women with unicornuate uterus remain suboptimal even after successful term delivery. Studies indicate increased recurrence of malpresentation, repeat cesarean delivery, and preterm birth in subsequent pregnancies
[16]
Venetis CA, et al. Clinical implications of congenital uterine anomalies. Reprod Biomed Online. 2014; 29: 665-83.
[18]
Rackow BW, Arici A. Reproductive performance in Müllerian anomalies. Curr Opin Obstet Gynecol. 2007; 19: 229-37.
[20]
Reichman D, Laufer MR. Congenital uterine anomalies affecting reproduction. Best Pract Res Clin Obstet Gynaecol. 2010; 24: 193-208.
[16, 18, 20]
. Therefore, patients should be counseled that successful pregnancy does not eliminate future obstetric risk. Multidisciplinary care involving obstetricians, radiologists, and neonatologists is essential to optimize outcomes in future gestations.
5. Recommendations
Women diagnosed with a unicornuate uterus should receive preconception counseling regarding potential obstetric risks. Early antenatal registration is essential. Detailed imaging using three-dimensional ultrasonography or magnetic resonance imaging should be considered to delineate uterine anatomy. Serial ultrasound surveillance for fetal growth and placental assessment is recommended throughout pregnancy. Delivery should be planned in a tertiary care center with facilities for emergency obstetric intervention. Postpartum counseling regarding future pregnancies and interpregnancy spacing is strongly advised.
6. Strengths and Limitations
The major strength of this case report is the documentation of a successful term pregnancy in a woman with unicornuate uterus and non-communicating rudimentary horn, a condition typically associated with poor obstetric outcomes. The incidental intraoperative diagnosis highlights the diagnostic challenges encountered in routine clinical practice, particularly in resource-limited settings.
Limitations include the absence of preoperative imaging confirming the uterine anomaly and lack of operative records from the previous cesarean section. Nevertheless, the clinical findings and favorable outcome contribute meaningful insight to existing literature and reinforce the importance of individualized obstetric management.
Abbreviations
BMI
Body Mass Index
CTG
Cardiotocography
ESIC
Employees’ State Insurance Corporation
G4P1L1A2
Gravida 4 Para 1 Living 1 Abortion 2
LSCS
Lower Segment Cesarean Section
MRI
Magnetic Resonance Imaging
NST
Non-Stress Test
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Chan YY, Jayaprakasan K, Tan A, Thornton JG, Coomarasamy A, Raine-Fenning NJ. Reproductive outcomes in women with congenital uterine anomalies: a systematic review. Ultrasound Obstet Gynecol. 2011; 38: 371-82.
[2]
Chan YY, Jayaprakasan K, Zamora J, Thornton JG, Raine-Fenning NJ, Coomarasamy A. The prevalence of congenital uterine anomalies in unselected and high-risk populations. Hum Reprod Update. 2011; 17: 761-71.
[3]
Reichman D, Laufer MR, Robinson BK. Pregnancy outcomes in unicornuate uteri: a review. Fertil Steril. 2009; 91: 1886-94.
[4]
Hua M, Odibo AO, Longman RE, Macones GA, Roehl KA, Cahill AG. Congenital uterine anomalies and adverse pregnancy outcomes. Am J Obstet Gynecol. 2011; 205: 558. e1-5.
[5]
Fedele L, Zamberletti D, Vercellini P, Dorta M, Candiani GB. Reproductive performance of women with unicornuate uterus. Fertil Steril. 1987; 47: 416-9.
[6]
Grimbizis GF, et al. Clinical implications of congenital uterine anomalies. Reprod Biomed Online. 2014; 29: 665-83.
[7]
Raga F, et al. Reproductive impact of congenital Müllerian anomalies. Fertil Steril. 1997; 68: 689-96.
[8]
Khati NJ, et al. Unicornuate uterus and its variants. J Ultrasound Med. 2012; 31: 319-31.
[9]
Nanda S, et al. Successful twin pregnancy in a unicornuate uterus. Arch Gynecol Obstet. 2009; 280: 993-5.
[10]
Amritha B, et al. Ruptured rudimentary horn pregnancy. J Med Case Rep. 2012; 6: 102.
Burman, K., Kaur, S. M., Verma, T. (2026). Pregnancy in a Unicornuate Uterus with Rudimentary Horn: A Case Report. Journal of Gynecology and Obstetrics, 14(1), 45-49. https://doi.org/10.11648/j.jgo.20261401.15
Burman, K.; Kaur, S. M.; Verma, T. Pregnancy in a Unicornuate Uterus with Rudimentary Horn: A Case Report. J. Gynecol. Obstet.2026, 14(1), 45-49. doi: 10.11648/j.jgo.20261401.15
Burman K, Kaur SM, Verma T. Pregnancy in a Unicornuate Uterus with Rudimentary Horn: A Case Report. J Gynecol Obstet. 2026;14(1):45-49. doi: 10.11648/j.jgo.20261401.15
@article{10.11648/j.jgo.20261401.15,
author = {Kanika Burman and Seema Manmeet Kaur and Trishika Verma},
title = {Pregnancy in a Unicornuate Uterus with Rudimentary Horn: A Case Report},
journal = {Journal of Gynecology and Obstetrics},
volume = {14},
number = {1},
pages = {45-49},
doi = {10.11648/j.jgo.20261401.15},
url = {https://doi.org/10.11648/j.jgo.20261401.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jgo.20261401.15},
abstract = {A unicornuate uterus is a rare congenital Müllerian anomaly resulting from incomplete development of one Müllerian duct and accounts for approximately 2-13% of all uterine malformations. This anomaly is associated with a wide range of adverse reproductive outcomes, including recurrent pregnancy loss, ectopic pregnancy, preterm birth, malpresentation, fetal growth restriction, and increased rates of operative delivery. Consequently, pregnancies in women with a unicornuate uterus are categorized as high risk and require careful antenatal surveillance and individualized obstetric management. We report the case of a 29-year-old woman with a term breech pregnancy at 40 weeks and 1 day of gestation who presented in active labor and underwent emergency lower segment cesarean section. Intraoperatively, a right-sided unicornuate uterus with a non-communicating rudimentary horn was incidentally identified. The ipsilateral fallopian tube and ovary were normal, while the contralateral adnexa were attached to the rudimentary horn. A healthy female neonate weighing 3.0 kg was delivered with an immediate cry. The postoperative period was uneventful, and both maternal and neonatal outcomes were favorable. This case demonstrates that successful term pregnancy is achievable in women with a unicornuate uterus despite inherent obstetric risks. It underscores the importance of maintaining a high index of suspicion for uterine anomalies in women presenting with recurrent malpresentation or adverse obstetric history and highlights the role of vigilant antenatal monitoring and tailored obstetric care in optimizing outcomes.},
year = {2026}
}
TY - JOUR
T1 - Pregnancy in a Unicornuate Uterus with Rudimentary Horn: A Case Report
AU - Kanika Burman
AU - Seema Manmeet Kaur
AU - Trishika Verma
Y1 - 2026/02/24
PY - 2026
N1 - https://doi.org/10.11648/j.jgo.20261401.15
DO - 10.11648/j.jgo.20261401.15
T2 - Journal of Gynecology and Obstetrics
JF - Journal of Gynecology and Obstetrics
JO - Journal of Gynecology and Obstetrics
SP - 45
EP - 49
PB - Science Publishing Group
SN - 2376-7820
UR - https://doi.org/10.11648/j.jgo.20261401.15
AB - A unicornuate uterus is a rare congenital Müllerian anomaly resulting from incomplete development of one Müllerian duct and accounts for approximately 2-13% of all uterine malformations. This anomaly is associated with a wide range of adverse reproductive outcomes, including recurrent pregnancy loss, ectopic pregnancy, preterm birth, malpresentation, fetal growth restriction, and increased rates of operative delivery. Consequently, pregnancies in women with a unicornuate uterus are categorized as high risk and require careful antenatal surveillance and individualized obstetric management. We report the case of a 29-year-old woman with a term breech pregnancy at 40 weeks and 1 day of gestation who presented in active labor and underwent emergency lower segment cesarean section. Intraoperatively, a right-sided unicornuate uterus with a non-communicating rudimentary horn was incidentally identified. The ipsilateral fallopian tube and ovary were normal, while the contralateral adnexa were attached to the rudimentary horn. A healthy female neonate weighing 3.0 kg was delivered with an immediate cry. The postoperative period was uneventful, and both maternal and neonatal outcomes were favorable. This case demonstrates that successful term pregnancy is achievable in women with a unicornuate uterus despite inherent obstetric risks. It underscores the importance of maintaining a high index of suspicion for uterine anomalies in women presenting with recurrent malpresentation or adverse obstetric history and highlights the role of vigilant antenatal monitoring and tailored obstetric care in optimizing outcomes.
VL - 14
IS - 1
ER -
Burman, K., Kaur, S. M., Verma, T. (2026). Pregnancy in a Unicornuate Uterus with Rudimentary Horn: A Case Report. Journal of Gynecology and Obstetrics, 14(1), 45-49. https://doi.org/10.11648/j.jgo.20261401.15
Burman, K.; Kaur, S. M.; Verma, T. Pregnancy in a Unicornuate Uterus with Rudimentary Horn: A Case Report. J. Gynecol. Obstet.2026, 14(1), 45-49. doi: 10.11648/j.jgo.20261401.15
Burman K, Kaur SM, Verma T. Pregnancy in a Unicornuate Uterus with Rudimentary Horn: A Case Report. J Gynecol Obstet. 2026;14(1):45-49. doi: 10.11648/j.jgo.20261401.15
@article{10.11648/j.jgo.20261401.15,
author = {Kanika Burman and Seema Manmeet Kaur and Trishika Verma},
title = {Pregnancy in a Unicornuate Uterus with Rudimentary Horn: A Case Report},
journal = {Journal of Gynecology and Obstetrics},
volume = {14},
number = {1},
pages = {45-49},
doi = {10.11648/j.jgo.20261401.15},
url = {https://doi.org/10.11648/j.jgo.20261401.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jgo.20261401.15},
abstract = {A unicornuate uterus is a rare congenital Müllerian anomaly resulting from incomplete development of one Müllerian duct and accounts for approximately 2-13% of all uterine malformations. This anomaly is associated with a wide range of adverse reproductive outcomes, including recurrent pregnancy loss, ectopic pregnancy, preterm birth, malpresentation, fetal growth restriction, and increased rates of operative delivery. Consequently, pregnancies in women with a unicornuate uterus are categorized as high risk and require careful antenatal surveillance and individualized obstetric management. We report the case of a 29-year-old woman with a term breech pregnancy at 40 weeks and 1 day of gestation who presented in active labor and underwent emergency lower segment cesarean section. Intraoperatively, a right-sided unicornuate uterus with a non-communicating rudimentary horn was incidentally identified. The ipsilateral fallopian tube and ovary were normal, while the contralateral adnexa were attached to the rudimentary horn. A healthy female neonate weighing 3.0 kg was delivered with an immediate cry. The postoperative period was uneventful, and both maternal and neonatal outcomes were favorable. This case demonstrates that successful term pregnancy is achievable in women with a unicornuate uterus despite inherent obstetric risks. It underscores the importance of maintaining a high index of suspicion for uterine anomalies in women presenting with recurrent malpresentation or adverse obstetric history and highlights the role of vigilant antenatal monitoring and tailored obstetric care in optimizing outcomes.},
year = {2026}
}
TY - JOUR
T1 - Pregnancy in a Unicornuate Uterus with Rudimentary Horn: A Case Report
AU - Kanika Burman
AU - Seema Manmeet Kaur
AU - Trishika Verma
Y1 - 2026/02/24
PY - 2026
N1 - https://doi.org/10.11648/j.jgo.20261401.15
DO - 10.11648/j.jgo.20261401.15
T2 - Journal of Gynecology and Obstetrics
JF - Journal of Gynecology and Obstetrics
JO - Journal of Gynecology and Obstetrics
SP - 45
EP - 49
PB - Science Publishing Group
SN - 2376-7820
UR - https://doi.org/10.11648/j.jgo.20261401.15
AB - A unicornuate uterus is a rare congenital Müllerian anomaly resulting from incomplete development of one Müllerian duct and accounts for approximately 2-13% of all uterine malformations. This anomaly is associated with a wide range of adverse reproductive outcomes, including recurrent pregnancy loss, ectopic pregnancy, preterm birth, malpresentation, fetal growth restriction, and increased rates of operative delivery. Consequently, pregnancies in women with a unicornuate uterus are categorized as high risk and require careful antenatal surveillance and individualized obstetric management. We report the case of a 29-year-old woman with a term breech pregnancy at 40 weeks and 1 day of gestation who presented in active labor and underwent emergency lower segment cesarean section. Intraoperatively, a right-sided unicornuate uterus with a non-communicating rudimentary horn was incidentally identified. The ipsilateral fallopian tube and ovary were normal, while the contralateral adnexa were attached to the rudimentary horn. A healthy female neonate weighing 3.0 kg was delivered with an immediate cry. The postoperative period was uneventful, and both maternal and neonatal outcomes were favorable. This case demonstrates that successful term pregnancy is achievable in women with a unicornuate uterus despite inherent obstetric risks. It underscores the importance of maintaining a high index of suspicion for uterine anomalies in women presenting with recurrent malpresentation or adverse obstetric history and highlights the role of vigilant antenatal monitoring and tailored obstetric care in optimizing outcomes.
VL - 14
IS - 1
ER -