Objective: Despite the widespread use of propofol for painless abortion, it is frequently associated with cardiopulmonary adverse events. Ciprofol, a novel intravenous anesthetic agent, demonstrates a more favorable respiratory and hemodynamic stability profile. The aims of this study were to evaluate the efficacy and safety of ciprofol-nalbuphine combination in mitigating cardiopulmonary complications and enhancing recovery following painless abortion procedures. Methods: A total of 120 patients scheduled for elective painless abortion, aged 18-39 years, ASA physical status I or II, were selected. They were randomly divided into a Propofol-Nalbuphine group (PN group, n = 60) and a Ciprofol-Nalbuphine group (CN group, n = 60) using a random number table. Anesthesia was induced by intravenous injection of nalbuphine 0.1 mg/kg, followed 3 minutes later by intravenous injection of propofol (2 mg/kg, PN group) or ciprofol (0.4 mg/kg, CN group). Anesthesia was maintained by continuous intravenous infusion of propofol or ciprofol. The incidence of cardiopulmonary adverse reactions (respiratory depression, hypotension, bradycardia), changes in heart rate (HR), mean arterial pressure (MAP), and pulse oxygen saturation (SpO2) at different time points were observed. Additionally, drug dosage, induction time, operative time, recovery time, injection pain, postoperative uterine contraction pain, and surgeon satisfaction were compared between the two groups. Results: Compared with PN, CN demonstrated a lower incidence of cardiopulmonary adverse reactions (15% vs. 40%, P < 0.05) and shorter recovery time (2.8 ± 1.8 vs. 1.9 ± 0.8 min, P < 0.05). The CN group also had reduced injection pain (3.3% vs. 16.6%) and intraoperative body movement (10% vs. 20%) (both P < 0.05). Surgeons reported higher satisfaction scores with CN (8.9 ± 1.0 vs. 8.0 ± 1.0, P < 0.001). MAP decreased after induction in both groups, with no intergroup difference (P > 0.05). Anesthesia induction time, operative time, and postoperative uterine contraction pain did not differ significantly between groups (P > 0.05). Conclusion: Intravenous anesthesia using ciprofol 0.4 mg/kg combined with nalbuphine 0.1 mg/kg is safe and effective for painless abortion. It offers advantages such as fewer cardiopulmonary adverse events, faster recovery, and less injection pain, making it worthy of clinical application and promotion.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Surgical abortion is a widely utilized medical intervention for terminating pregnancies in their early stages. Due to the pain and emotional distress typically involved, many patients choose to undergo the procedure with pain management options
[1]
Rajkumar RP. The Relationship Between Access to Abortion and Mental Health in Women of Childbearing Age: Analyses of Data From the Global Burden of Disease Studies. Cureus. 2022; 14(11): e31433.
. As a result, there is a strong demand for anesthetic agents that must offer rapid onset, adequate sedation, superior analgesia, brief recovery, and few side effects. Propofol is commonly used for anesthesia in painless abortion procedures due to its advantages of rapid onset, quick metabolism, and high clearance rate
[2]
Gu J, Liu Y, Lin X, et al. Comparison of Remimazolam-Flumazenil and Propofol on Psychomotor Function and Emergence Following General Anesthesia in Surgical Abortion: A Randomized Controlled Trial. Drug Des Devel Ther. 2024; 18: 6447-6457.
. However, its adverse effects such as respiratory depression, hypotension, and injection pain have attracted widespread clinical attention
[3]
Zhang H, Zhang M, Hao L, et al. Comparison of the Effects of Ciprofol and Propofol on Postoperative Nausea and Vomiting in Patients Undergoing Outpatient Hysteroscopy. Drug Des Devel Ther. 2024; 18: 5701-5707.
. Ciprofol (HSK3486) is a novel 2, 6-disubstituted phenolic derivative. Based on the structural framework of propofol, the addition of a cyclopropyl group enhances its binding affinity to the γ-aminobutyric acid type A (GABA-A) receptor
[4]
Bian Y, Zhang H, Ma S, et al. Mass balance, pharmacokinetics and pharmacodynamics of intravenous HSK3486, a novel anaesthetic, administered to healthy subjects. Br J Clin Pharmacol. 2021; 87(1): 93-105.
Liao J, Li M, Huang C, et al. Pharmacodynamics and Pharmacokinetics of HSK3486, a Novel 2, 6-Disubstituted Phenol Derivative as a General Anesthetic. Front Pharmacol. 2022; 13: 830791.
, thereby inducing sedative and anesthetic effects in the central nervous system
[6]
Akhtar SMM, Fareed A, Ali M, et al. Efficacy and safety of Ciprofol compared with Propofol during general anesthesia induction: A systematic review and meta-analysis of randomized controlled trials (RCT). J Clin Anesth. 2024; 94: 111425.
. Although the pharmacokinetic characteristics of ciprofol are comparable to those of propofol, studies have shown that the incidence of adverse events such as respiratory depression, hypotension, and injection pain is significantly lower with ciprofol than with propofol
[7]
Li J, Wang X, Liu J, et al. Comparison of ciprofol (HSK3486) versus propofol for the induction of deep sedation during gastroscopy and colonoscopy procedures: A multi-centre, non-inferiority, randomized, controlled phase 3 clinical trial. Basic Clin Pharmacol Toxicol. 2022; 131(2): 138-148.
. Nalbuphine, as a μ-receptor antagonist and κ-receptor agonist, offers advantages such as effective visceral pain suppression and a lower incidence of postoperative nausea and vomiting (PONV) compared to other opioids
[8]
Deng C, Wang X, Zhu Q, et al. Comparison of nalbuphine and sufentanil for colonoscopy: A randomized controlled trial. PLoS One. 2017; 12(12): e0188901.
Based on its unique pharmacological properties, the synthetic opioid nalbuphine represents a promising analgesic choice for painless abortion procedures
[9]
Fang P, Qian J, Ding J, Pan X, Su H, Liu X. Comparison of Analgesic Effects between Nalbuphine and Sufentanil in First-Trimester Surgical Abortion: A Randomized, Double-Blind, Controlled Trial. Pain Ther. 2022; 11(1): 121-132.
. While clinical trials and meta-analyses have indicated that ciprofol is associated with lower rates of respiratory depression, hypotension, and injection pain compared to propofol in the context of painless gastrointestinal endoscopy
[3]
Zhang H, Zhang M, Hao L, et al. Comparison of the Effects of Ciprofol and Propofol on Postoperative Nausea and Vomiting in Patients Undergoing Outpatient Hysteroscopy. Drug Des Devel Ther. 2024; 18: 5701-5707.
Akhtar SMM, Fareed A, Ali M, et al. Efficacy and safety of Ciprofol compared with Propofol during general anesthesia induction: A systematic review and meta-analysis of randomized controlled trials (RCT). J Clin Anesth. 2024; 94: 111425.
, it remains uncertain whether combining nalbuphine with ciprofol confers a clear benefit over its combination with propofol for painless abortion, due to the absence of relevant comparative studies. Therefore, we conducted a trial to compare the effects of nalbuphine combined with either propofol or ciprofol for anesthesia in painless abortion, aiming to inform clinical anesthetic selection. We postulated that the combination of ciprofol and nalbuphine could potentially improve procedural safety and expedite recovery after abortion. Although the safety of ciprofol as a single agent in gastroscopy and colonoscopy has been documented
[10]
Guan X, Jiao Z, Gong X, et al. Efficacy of Pre-Treatment with Remimazolam on Prevention of Propofol-Induced Injection Pain in Patients Undergoing Abortion or Curettage: A Prospective, Double-Blinded, Randomized and Placebo-Controlled Clinical Trial. Drug Des Devel Ther. 2021; 15: 4551-4558.
, there is a scarcity of high-quality clinical data on the efficacy and safety of the ciprofol-nalbuphine combination for sedation in abortion. To investigate this, we performed a head-to-head comparison between ciprofol and propofol for moderate sedation during abortion, with a focus on cardiopulmonary complications and recovery parameters.
2. Material and Methods
Design and patients
This single-center, randomized, controlled clinical trial was conducted at the Wuxi Huishan District People’s Hospital, Jiangsu Province, China. This study was approved by the Ethics Committee of Huishan District People's Hospital in Wuxi (Approval No: HYLL (YJ)-2025003). The study was performed in full compliance with the ethical standards set forth by the Declaration of Helsinki (1975 revision). Written informed consent was a mandatory requirement for all participants before the commencement of any study-related procedures.
The study enrolled 120 patients who were scheduled for elective painless abortion, aged 18-39 years. Using a random number table, participants were allocated to either the PN group (n = 60) or the CN group (n = 60). Eligibility requirements consisted of: American Society of Anesthesiologists (ASA) physical status class I-II, respiratory rate 12-18 breaths/min, heart rate 50-100 beats/min, systolic blood pressure (SBP) 90-180 mmHg, diastolic blood pressure (DBP) 60-100 mmHg, and room-air SpO₂ above 95%. Exclusion criteria were: known hypersensitivity to propofol, ciprofol, or nalbuphine; anticipated difficult airway; significant psychiatric illness or emotional instability; compromised cardiopulmonary function (e.g., severe hypertension, myocardial ischemia, heart failure, second-degree atrioventricular block, or severe chronic obstructive pulmonary disease); hepatic or renal impairment; and any other condition considered clinically unsuitable for inclusion by the investigators.
Anesthesia Management
The randomization was performed in a 1:1 ratio using a computer-generated sequence, assigning patients to either the ciprofol or propofol group, with no stratification applied. Allocation concealment was ensured through sequentially numbered, sealed opaque envelopes. Upon opening the envelope, the assigned anesthetic agent was administered by the attending anesthesiologist according to a predetermined sedation protocol designed to maintain patient safety. In the operating room, patients were placed in the lithotomy position. Standard monitoring was established, including non-invasive blood pressure, electrocardiogram, and SpO₂. Prior to the procedure, all patients received supplemental oxygen at 3 L/min via nasal cannula, which continued until full recovery of consciousness following the procedure.
Prior to study drug administration, all patients received a bolus of 0.1 mg/kg nalbuphine (Nalbuphine Hydrochloride Injection, 10 mg/2 ml; Yangtze River Pharmaceutical Industry Co., Ltd., China) intravenously over 15 seconds. Following this, patients were randomized to receive an initial induction dose of either 0.4 mg/kg ciprofol or 2.0 mg/kg propofol (both from HaiSiKe, Liaoning, China). The anesthesiologist administered the induction agent intravenously over 30 seconds. Sedation depth was monitored with the Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) scale
[11]
Gao SH, Tang QQ, Wang CM, et al. The efficacy and safety of ciprofol and propofol in patients undergoing colonoscopy: A double-blind, randomized, controlled trial. J Clin Anesth. 2024; 95: 111474.
. Abortion commenced once adequate sedation was attained, defined as an MOAA/S score of ≤ 3. Throughout the procedure, MOAA/S scores were recorded at two-minute intervals. If body movements were observed, maintenance sedation was provided as bolus supplements: 0.1 mg/kg ciprofol in the ciprofol group or 0.5 mg/kg propofol in the propofol group. A desaturation event was defined as a decrease in SpO₂ below 90% lasting more than 10 seconds, prompting immediate airway interventions such as jaw thrust or bag-mask ventilation. If hypoxemia persisted or oxygen saturation failed to improve, manual ventilation was instituted. Pharmacological support with atropine, ephedrine, and/or inotropes was administered in response to hypotension (SBP < 90 mmHg) or bradycardia (HR < 50 beats per minute). Hemodynamic deviations were defined as follows: hypotension and hypertension were respectively defined as a decrease or increase of ≥ 20% in either MAP or SBP relative to baseline values. Bradycardia was defined as a HR ≤50 beats per minute. Hypoxemia was characterized by a SpO₂ below 90% lasting for more than 10 seconds. Following the painless abortion procedure, patients were monitored continuously in the post-anesthesia care unit (PACU). The Aldrete score
[12]
Roelandt P, Haesaerts R, Demedts I, Bisschops R. Implementation of the Aldrete score reduces recovery time after non-anesthesiologist-administered procedural sedation in gastrointestinal endoscopy. Endosc Int Open. 2022; 10(12): E1544-E1547.
was recorded at two-minute intervals, and transfer from the PACU to the observation area was permitted after three consecutive readings of ≥ 9 were obtained. Eligibility for final discharge was determined using the Modified Post-Anesthesia Discharge Scoring System (MPADSS), with a score of 10 required across five domains: vital signs, ambulation, nausea/vomiting, pain, and intraoperative bleeding
[13]
Edokpolo LU, Mastriano DJ, Serafin J, et al. Discharge Readiness after Propofol with or without Dexmedetomidine for Colonoscopy: A Randomized Controlled Trial. Anesthesiology. 2019; 131(2): 279-286.
The primary endpoint was the incidence of cardiopulmonary adverse events, which included hypotension, bradycardia, and hypoxemia. The secondary endpoints included the time of induction, surgical duration, time to awakening; total dosage of ciprofol, propofol, and nalbuphine; incidence of injection pain, dreaming, uterine pain; and operator satisfaction.
Calculation of sample size
PASS 15.0.5 (NCSS, LLC, Kaysville, USA) was utilized for sample size calculation.
In gynecological surgery, the incidences of anesthesia-related adverse events during general anesthesia induction with propofol and ciprofol were reported as 48.3% and 20.0%, respectively
[14]
Chen BZ, Yin XY, Jiang LH, et al. The efficacy and safety of ciprofol use for the induction of general anesthesia in patients undergoing gynecological surgery: a prospective randomized controlled study. BMC Anesthesiology, 2022, 22(1): 245.
. Using a 1:1 allocation ratio, with a two-sided significance level (α) of 0.05 and a power (1-β) of 0.9, and accounting for an estimated dropout rate of 10%, the calculated sample size required was 120 patients, with 60 participants assigned to each group.
Statistical analysis
Statistical analysis was performed using SPSS version 22.0 (IBM, Armonk, NY, USA). The normality of continuous variables was evaluated with the Shapiro-Wilk test. Normally distributed variables are presented as mean ± standard deviation (SD) and were compared using the independent two-sample t-test. Non-normally distributed variables are summarized as median (range) and were analyzed using the Mann-Whitney U test. Categorical variables are expressed as frequencies and percentages, and were compared using the chi-square (χ²) test or Fisher’s exact test, as appropriate. A two-sided P-value of less than 0.05 was defined as statistically significant.
3. Results
3.1. Trial Population and Baseline Characteristics
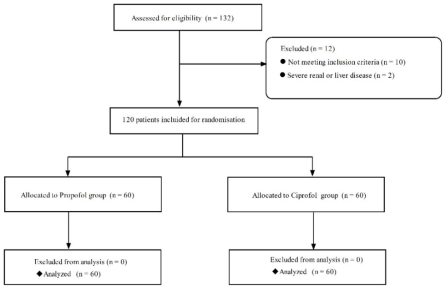
Between March 2025 and October 2025, a total of 120 patients scheduled for painless abortion at Huishan District People’s Hospital, Xinglin College of Nantong University, were assessed for eligibility. After applying the predefined exclusion criteria, eligible participants were enrolled and randomly assigned to receive sedation with either ciprofol or propofol (Figure 1). No statistically significant differences were observed between the two groups in baseline demographic, clinical, or procedural characteristics. (P > 0.05) (Table 1).
Table 1. Patient demographics and baseline values.
Variable
Group PN (n = 60)
Group CN (n = 60)
2/ t
P-value
Age (years old)
31.8±5.5
31.7±4.8
0.035
0.972
Height (cm)
160.9± 5.3
160.8±5.8
0.909
0.909
Weight (kg)
57.6±9.2
59.4±8.0
1.169
0.245
BMI (kg/m2)
22.1±3.1
22.9±2.9
1.413
0.160
ASA physical status
0.229
0.632
I grade
55
56
II grade
5
4
Note: Data were presented as mean (SD) or n (%), as appropriate; SD = standard deviation.
3.2. Anesthetic Use and Sedation-related Time
Table 2. Consumption of anesthetics and sedation-related time.
Variable
Group PN (n = 60)
Group CN (n = 60)
2/ t
P-value
Nalbuphine dose (mg)
5.5±0.9
5.7±0.8
0.895
0.372
Sedative-agent dose (mg)
Induction dose (mg)
108.3±15.3
28.6±4.4
Total dose (mg)
121.6±25.7
31.6±5.7
Time
Induction (Second)
47.8±5.1
49.1±5.4
1.394
0.166
Operation (min)
6.5±1.9
6.9±2.1
1.276
0.205
Recover (min)
2.8±1.8
1.9±0.8
3.503
0.001
There were no statistically significant differences between the two groups in terms of anesthesia induction time, surgical duration, or nalbuphine dosage (P > 0.05). However, the recovery time was significantly shorter in the CN group compared to the PN group (P < 0.05) (Table 2).
3.3. Primary and Secondary Outcomes
Compared to the PN group, the CN group demonstrated a significant reduction in the incidence of intraoperative cardiopulmonary adverse events and injection pain (P < 0.05). Operator satisfaction scores were markedly higher in the CN group than in the PN group (P < 0.001). No statistically significant differences were observed between the two groups regarding other perioperative adverse events (P > 0.05) (Table 3).
Table 3. Adverse events.
Outcomes
Group PN (n = 60)
Group CN (n = 60)
2/t
P-value
Primary outcome
Hypotension
13 (21.6%)
3 (5.0%)
5.841
0.016
Bradycardia
9 (15.0%)
5 (8.3%)
1.294
0.255
hypoxemia
2 (3.3%)
1 (1.6%)
0.000
1.000
Total incidence rate
24 (40.0%)
9 (15.0%)
9.404
0.002
Secondary outcome
Injection pain
10 (16.6%)
2 (3.3%)
4.537
0.033
Body movement
20 (33.3%)
10 (16.6%)
4.444
0.035
Dreaming
22 (36.6%)
18 (30%)
0.600
0.439
Uterine pain
19 (31.6%)
20 (33.3%)
0.038
0.845
Fatigue
2 (3.3%)
3 (5.0%)
0.000
1.000
Gynecologist satisfaction
8.0±1.0
8.9±1.0
4.497
<0.001
3.4. Hemodynamics
No statistically significant differences were observed between the two groups in MAP, HR, or SpO2 (Table 4).
Table 4. Hemodynamics between the two groups.
Variable
Group PN (n=60)
Group CN (n=60)
t
P-value
MAP (mmHg)
T1
90.4±12.2
90.2±13.1
0.086
0.931
T2
71.5±11.0
74.8±11.3
1.588
0.115
T3
82.7±15.7
87.2±16.0
1.561
0.121
T4
87.5±14.9
91.6±16.2
1.446
0.151
T5
86.6±13.9
90.5±14.45
1.534
0.128
HR (beats/min)
T1
79.9±9.3
83.5±13.3
1.721
0.088
T2
72.0±8.1
72.6±10.2
0.336
0.738
T3
69.2±8.2
70.1±9.1
0.568
0.571
T4
68.6±8.3
69.9±8.7
0.836
0.405
T5
71.7±8.1
73.9±8.3
1.503
0.136
SpO2 (%)
T1
99.4±0.5
99.4±0.5
0.172
0.864
T2
98.9±0.7
98.8±1.3
0.680
0.498
T3
98.9±0.9
98.9±0.7
0.492
0.668
T4
98.9±0.4
98.8±0.7
0.303
0.762
T5
99.0±0.5
99.1±0.5
0.885
0.378
Note: T1: Before anesthesia induction, T2: After anesthesia induction, T3: During cervical dilation, T4: End of surgery, T5: Upon leaving the recovery room.
4. Discussion
Our study focused on the combination of ciprofol and nalbuphine for painless abortion sedation for the first time. The findings substantiated the protocol's promise, verifying its capacity to reliably produce target sedation, decrease the incidence of respiratory complications, and foster improved hemodynamic stability.
This study confirmed that both ciprofol (0.4 mg/kg) and propofol (2 mg/kg), when used for induction in combination with nalbuphine (0.1 mg/kg) and titrated for maintenance based on MOAA/S scores, were effective in completing the abortion procedure. However, the ciprofol-nalbuphine regimen demonstrated advantages including fewer cardiopulmonary adverse effects, shorter recovery time, and a lower incidence of injection pain. In this study, the incidence of hypotension was 21.6% in the NP group, compared to only 5.0% in the NC group, indicating that ciprofol exhibits better efficacy in reducing cardiopulmonary adverse effects, which is consistent with previous studies
[11]
Gao SH, Tang QQ, Wang CM, et al. The efficacy and safety of ciprofol and propofol in patients undergoing colonoscopy: A double-blind, randomized, controlled trial. J Clin Anesth. 2024; 95: 111474.
Liu J, Hong A, Zeng J, et al. The efficacy of ciprofol versus propofol on anesthesia in patients undergoing endoscopy: a systematic review and meta-analysis of randomized controlled trials. BMC Anesthesiol. 2024; 24(1): 359.
. It demonstrated that propofol-nalbuphine sedation for Endoscopic retrograde cholangiopancreatography significantly reduced respiratory depression and procedural interruption compared with propofol-fentanyl, likely attributable to the unique pharmacodynamics of nalbuphine
[16]
Wang P, Chen Y, Guo Y, et al. Comparison of propofol-nalbuphine and propofol-fentanyl sedation for patients undergoing endoscopic retrograde cholangiopancreatography: a double-blind, randomized controlled trial. BMC Anesthesiol. 2022; 22(1): 47.
. In a randomized, double-blind colonoscopy trial, a ciprofol dose of 0.4-0.5 mg/kg provided comparable sedative efficacy to 2.0 mg/kg of propofol, with no statistically significant differences in safety outcomes between the two groups
[17]
Teng Y, Ou M, Wang X, et al. Efficacy and safety of ciprofol for the sedation/anesthesia in patients undergoing colonoscopy: Phase IIa and IIb multi-center clinical trials. Eur J Pharm Sci. 2021; 164: 105904.
. Compared to ciprofol, propofol was associated with a higher incidence of hypotension during induction due to its sympatholytic effects
[18]
Zhang J, Liu R, Bi R, et al. Comparison of ciprofol-alfentanil and propofol-alfentanil sedation during bidirectional endoscopy: A prospective, double-blind, randomised, controlled trial. Dig Liver Dis. 2024; 56(4): 663-671.
. The findings of this study also indicated a higher intraoperative hypotension rate in the NP group than in the NC group, although the difference was not statistically significant. A possible explanation for this observation is that intravenous administration of nalbuphine prior to general anesthesia induction reduced the required induction dose of propofol. The occurrence of anesthesia-related hypotension and sinus bradycardia may be linked to the GABA-ergic modulatory mechanism of propofol within the autonomic nuclei of the brainstem, which exerts inhibitory effects on both chronotropic regulation and vasomotor tone maintenance
[19]
Wang X, Wang X, Liu J, et al. Effects of ciprofol for the induction of general anesthesia in patients scheduled for elective surgery compared to propofol: a phase 3, multicenter, randomized, double-blind, comparative study. Eur Rev Med Pharmacol Sci. 2022; 26(5): 1607-1617.
It has been reported in the literature that propofol was associated with a relatively high incidence of injection pain, reaching up to 52.4%
[7]
Li J, Wang X, Liu J, et al. Comparison of ciprofol (HSK3486) versus propofol for the induction of deep sedation during gastroscopy and colonoscopy procedures: A multi-centre, non-inferiority, randomized, controlled phase 3 clinical trial. Basic Clin Pharmacol Toxicol. 2022; 131(2): 138-148.
. In the present study, however, the incidence was only 16.6%, which may be attributed to the analgesic effect provided by the preemptive intravenous administration of nalbuphine. Meanwhile, the lower concentration (1%) of the lipid emulsion in ciprofol contributes to its increased hydrophobicity, which is another factor explaining its reduced incidence of injection pain
[20]
Teng Y, Ou MC, Wang X, et al. Pharmacokinetic and pharmacodynamic properties of ciprofol emulsion in Chinese subjects: a single center, open-label, single-arm dose-escalation phase 1 study. Am J Transl Res. 2021; 13(12): 13791-13802.
[20]
. Lower incidence of injection pain with ciprofol administration was theorized to correlate with heightened patient satisfaction scores. Previous studies have shown that in anesthesia for painless gastrointestinal endoscopy using nalbuphine combined with propofol, the ED50 and ED95 of nalbuphine are 0.078 mg/kg and 0.162 mg/kg, respectively
[21]
Li S, Wang Y, Chen X, Huang T, et al. Effective Doses of Nalbuphine Combined With Propofol for Painless Gastroscopy in Adults: A Randomized Controlled Trial. Front Pharmacol. 2021; 12: 673550.
. Given that the duration and surgical stimulation during painless abortion were typically shorter and less intense than those during painless gastrointestinal endoscopy, the dosage of nalbuphine was set at 0.1 mg/kg in this study. This study found an induction time of approximately 50 seconds with 0.4 mg/kg ciprofol, which is notably shorter than the 63.4-second onset time reported by Gao et al
[11]
Gao SH, Tang QQ, Wang CM, et al. The efficacy and safety of ciprofol and propofol in patients undergoing colonoscopy: A double-blind, randomized, controlled trial. J Clin Anesth. 2024; 95: 111474.
. This difference may be related to the preemptive administration of nalbuphine. The satisfaction of surgeon primarily depends on the patient's intraoperative cooperation (absence of involuntary movements) and an efficient workflow (short recovery time and expedited turnover). In this study, the incidence of intraoperative body movement reactions in the PN group was twice that in the CN group, which explains why the satisfaction level among obstetricians and gynecologists was lower in the PN group compared to the CN group. The results of this investigation found that the incidence of dreaming was 36.6% in the PN group and 30% in the CN group, a difference that was not statistically significant and consistent with the findings of Zhou et al
[22]
Zhou R, Fu L, Liu S, et al. Influences of Propofol, Ciprofol and Remimazolam on Dreaming During Anesthesia for Gastrointestinal Endoscopy: A Randomized Double-Blind Parallel-Design Trial. Drug Des Devel Ther. 2024; 18: 1907-1915.
. Consequently, it cannot be inferred that dreaming leads to higher patient satisfaction, as intraoperative dreams are influenced by multiple factors including the type of anesthetic agent, depth of anesthesia, age, gender, and preoperative psychological state
[23]
Yoshida A, Fujii K, Yoshikawa T, Kawamata T. Factors associated with quality of dreams during general anesthesia: a prospective observational study. J Anesth. 2021; 35(4): 576-580.
The limitations of this study include: (1) The exclusion of obese individuals, combined with a relatively young cohort, likely contributed to a lower observed incidence of upper airway obstruction; (2) Routine blood glucose monitoring was not performed before the abortion procedure, as hypoglycemia can also lead to hypotension; (3) Conducted at a single center, this study had inherent limitations regarding the external validity of its conclusions; (4) The adverse effects of sedative medications after discharge were not systematically evaluated.
Abbreviations
ASA
American Society of Anesthesiologists
BMI
Body Mass Index
DBP
Diastolic Blood Pressure
HR
Heart Rate
MAP
Mean Arterial Pressure
MOAA/S
Modified Observer’s Assessment of Alertness/Sedation
PACU
Post-Anesthesia Care Unit
PONV
Postoperative Nausea and Vomiting
SpO2
Pulse Oxygen Saturation
SBP
Systolic Blood Pressure
Acknowledgments
We extend our sincere gratitude to our families for their unwavering support and continuous encouragement throughout the duration of this study.
Data Availability Statement
All original data will be available when contact the correspondence author by email.
Conflicts of Interest
The authors declare that they have no competing interests.
References
[1]
Rajkumar RP. The Relationship Between Access to Abortion and Mental Health in Women of Childbearing Age: Analyses of Data From the Global Burden of Disease Studies. Cureus. 2022; 14(11): e31433.
Gu J, Liu Y, Lin X, et al. Comparison of Remimazolam-Flumazenil and Propofol on Psychomotor Function and Emergence Following General Anesthesia in Surgical Abortion: A Randomized Controlled Trial. Drug Des Devel Ther. 2024; 18: 6447-6457.
Zhang H, Zhang M, Hao L, et al. Comparison of the Effects of Ciprofol and Propofol on Postoperative Nausea and Vomiting in Patients Undergoing Outpatient Hysteroscopy. Drug Des Devel Ther. 2024; 18: 5701-5707.
Bian Y, Zhang H, Ma S, et al. Mass balance, pharmacokinetics and pharmacodynamics of intravenous HSK3486, a novel anaesthetic, administered to healthy subjects. Br J Clin Pharmacol. 2021; 87(1): 93-105.
Liao J, Li M, Huang C, et al. Pharmacodynamics and Pharmacokinetics of HSK3486, a Novel 2, 6-Disubstituted Phenol Derivative as a General Anesthetic. Front Pharmacol. 2022; 13: 830791.
Akhtar SMM, Fareed A, Ali M, et al. Efficacy and safety of Ciprofol compared with Propofol during general anesthesia induction: A systematic review and meta-analysis of randomized controlled trials (RCT). J Clin Anesth. 2024; 94: 111425.
Li J, Wang X, Liu J, et al. Comparison of ciprofol (HSK3486) versus propofol for the induction of deep sedation during gastroscopy and colonoscopy procedures: A multi-centre, non-inferiority, randomized, controlled phase 3 clinical trial. Basic Clin Pharmacol Toxicol. 2022; 131(2): 138-148.
Deng C, Wang X, Zhu Q, et al. Comparison of nalbuphine and sufentanil for colonoscopy: A randomized controlled trial. PLoS One. 2017; 12(12): e0188901.
Fang P, Qian J, Ding J, Pan X, Su H, Liu X. Comparison of Analgesic Effects between Nalbuphine and Sufentanil in First-Trimester Surgical Abortion: A Randomized, Double-Blind, Controlled Trial. Pain Ther. 2022; 11(1): 121-132.
Guan X, Jiao Z, Gong X, et al. Efficacy of Pre-Treatment with Remimazolam on Prevention of Propofol-Induced Injection Pain in Patients Undergoing Abortion or Curettage: A Prospective, Double-Blinded, Randomized and Placebo-Controlled Clinical Trial. Drug Des Devel Ther. 2021; 15: 4551-4558.
Gao SH, Tang QQ, Wang CM, et al. The efficacy and safety of ciprofol and propofol in patients undergoing colonoscopy: A double-blind, randomized, controlled trial. J Clin Anesth. 2024; 95: 111474.
Roelandt P, Haesaerts R, Demedts I, Bisschops R. Implementation of the Aldrete score reduces recovery time after non-anesthesiologist-administered procedural sedation in gastrointestinal endoscopy. Endosc Int Open. 2022; 10(12): E1544-E1547.
Edokpolo LU, Mastriano DJ, Serafin J, et al. Discharge Readiness after Propofol with or without Dexmedetomidine for Colonoscopy: A Randomized Controlled Trial. Anesthesiology. 2019; 131(2): 279-286.
Chen BZ, Yin XY, Jiang LH, et al. The efficacy and safety of ciprofol use for the induction of general anesthesia in patients undergoing gynecological surgery: a prospective randomized controlled study. BMC Anesthesiology, 2022, 22(1): 245.
Liu J, Hong A, Zeng J, et al. The efficacy of ciprofol versus propofol on anesthesia in patients undergoing endoscopy: a systematic review and meta-analysis of randomized controlled trials. BMC Anesthesiol. 2024; 24(1): 359.
Wang P, Chen Y, Guo Y, et al. Comparison of propofol-nalbuphine and propofol-fentanyl sedation for patients undergoing endoscopic retrograde cholangiopancreatography: a double-blind, randomized controlled trial. BMC Anesthesiol. 2022; 22(1): 47.
Teng Y, Ou M, Wang X, et al. Efficacy and safety of ciprofol for the sedation/anesthesia in patients undergoing colonoscopy: Phase IIa and IIb multi-center clinical trials. Eur J Pharm Sci. 2021; 164: 105904.
Zhang J, Liu R, Bi R, et al. Comparison of ciprofol-alfentanil and propofol-alfentanil sedation during bidirectional endoscopy: A prospective, double-blind, randomised, controlled trial. Dig Liver Dis. 2024; 56(4): 663-671.
Wang X, Wang X, Liu J, et al. Effects of ciprofol for the induction of general anesthesia in patients scheduled for elective surgery compared to propofol: a phase 3, multicenter, randomized, double-blind, comparative study. Eur Rev Med Pharmacol Sci. 2022; 26(5): 1607-1617.
Teng Y, Ou MC, Wang X, et al. Pharmacokinetic and pharmacodynamic properties of ciprofol emulsion in Chinese subjects: a single center, open-label, single-arm dose-escalation phase 1 study. Am J Transl Res. 2021; 13(12): 13791-13802.
[21]
Li S, Wang Y, Chen X, Huang T, et al. Effective Doses of Nalbuphine Combined With Propofol for Painless Gastroscopy in Adults: A Randomized Controlled Trial. Front Pharmacol. 2021; 12: 673550.
Zhou R, Fu L, Liu S, et al. Influences of Propofol, Ciprofol and Remimazolam on Dreaming During Anesthesia for Gastrointestinal Endoscopy: A Randomized Double-Blind Parallel-Design Trial. Drug Des Devel Ther. 2024; 18: 1907-1915.
Yoshida A, Fujii K, Yoshikawa T, Kawamata T. Factors associated with quality of dreams during general anesthesia: a prospective observational study. J Anesth. 2021; 35(4): 576-580.
Huang, Z., Gong, W., Feng, T., Zhang, Z., Yu, Z. (2026). Comparison of Ciprofol-nalbuphine and
Propofol-nalbuphine Sedation During Painless Abortion:
A Randomized Controlled Trial. Journal of Gynecology and Obstetrics, 14(1), 37-44. https://doi.org/10.11648/j.jgo.20261401.14
Huang, Z.; Gong, W.; Feng, T.; Zhang, Z.; Yu, Z. Comparison of Ciprofol-nalbuphine and
Propofol-nalbuphine Sedation During Painless Abortion:
A Randomized Controlled Trial. J. Gynecol. Obstet.2026, 14(1), 37-44. doi: 10.11648/j.jgo.20261401.14
Huang Z, Gong W, Feng T, Zhang Z, Yu Z. Comparison of Ciprofol-nalbuphine and
Propofol-nalbuphine Sedation During Painless Abortion:
A Randomized Controlled Trial. J Gynecol Obstet. 2026;14(1):37-44. doi: 10.11648/j.jgo.20261401.14
@article{10.11648/j.jgo.20261401.14,
author = {Zu-chao Huang and Wan-wan Gong and Tian-kui Feng and Zhong Zhang and Zhi-yang Yu},
title = {Comparison of Ciprofol-nalbuphine and
Propofol-nalbuphine Sedation During Painless Abortion:
A Randomized Controlled Trial},
journal = {Journal of Gynecology and Obstetrics},
volume = {14},
number = {1},
pages = {37-44},
doi = {10.11648/j.jgo.20261401.14},
url = {https://doi.org/10.11648/j.jgo.20261401.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jgo.20261401.14},
abstract = {Objective: Despite the widespread use of propofol for painless abortion, it is frequently associated with cardiopulmonary adverse events. Ciprofol, a novel intravenous anesthetic agent, demonstrates a more favorable respiratory and hemodynamic stability profile. The aims of this study were to evaluate the efficacy and safety of ciprofol-nalbuphine combination in mitigating cardiopulmonary complications and enhancing recovery following painless abortion procedures. Methods: A total of 120 patients scheduled for elective painless abortion, aged 18-39 years, ASA physical status I or II, were selected. They were randomly divided into a Propofol-Nalbuphine group (PN group, n = 60) and a Ciprofol-Nalbuphine group (CN group, n = 60) using a random number table. Anesthesia was induced by intravenous injection of nalbuphine 0.1 mg/kg, followed 3 minutes later by intravenous injection of propofol (2 mg/kg, PN group) or ciprofol (0.4 mg/kg, CN group). Anesthesia was maintained by continuous intravenous infusion of propofol or ciprofol. The incidence of cardiopulmonary adverse reactions (respiratory depression, hypotension, bradycardia), changes in heart rate (HR), mean arterial pressure (MAP), and pulse oxygen saturation (SpO2) at different time points were observed. Additionally, drug dosage, induction time, operative time, recovery time, injection pain, postoperative uterine contraction pain, and surgeon satisfaction were compared between the two groups. Results: Compared with PN, CN demonstrated a lower incidence of cardiopulmonary adverse reactions (15% vs. 40%, P P P P P > 0.05). Anesthesia induction time, operative time, and postoperative uterine contraction pain did not differ significantly between groups (P > 0.05). Conclusion: Intravenous anesthesia using ciprofol 0.4 mg/kg combined with nalbuphine 0.1 mg/kg is safe and effective for painless abortion. It offers advantages such as fewer cardiopulmonary adverse events, faster recovery, and less injection pain, making it worthy of clinical application and promotion.},
year = {2026}
}
TY - JOUR
T1 - Comparison of Ciprofol-nalbuphine and
Propofol-nalbuphine Sedation During Painless Abortion:
A Randomized Controlled Trial
AU - Zu-chao Huang
AU - Wan-wan Gong
AU - Tian-kui Feng
AU - Zhong Zhang
AU - Zhi-yang Yu
Y1 - 2026/02/06
PY - 2026
N1 - https://doi.org/10.11648/j.jgo.20261401.14
DO - 10.11648/j.jgo.20261401.14
T2 - Journal of Gynecology and Obstetrics
JF - Journal of Gynecology and Obstetrics
JO - Journal of Gynecology and Obstetrics
SP - 37
EP - 44
PB - Science Publishing Group
SN - 2376-7820
UR - https://doi.org/10.11648/j.jgo.20261401.14
AB - Objective: Despite the widespread use of propofol for painless abortion, it is frequently associated with cardiopulmonary adverse events. Ciprofol, a novel intravenous anesthetic agent, demonstrates a more favorable respiratory and hemodynamic stability profile. The aims of this study were to evaluate the efficacy and safety of ciprofol-nalbuphine combination in mitigating cardiopulmonary complications and enhancing recovery following painless abortion procedures. Methods: A total of 120 patients scheduled for elective painless abortion, aged 18-39 years, ASA physical status I or II, were selected. They were randomly divided into a Propofol-Nalbuphine group (PN group, n = 60) and a Ciprofol-Nalbuphine group (CN group, n = 60) using a random number table. Anesthesia was induced by intravenous injection of nalbuphine 0.1 mg/kg, followed 3 minutes later by intravenous injection of propofol (2 mg/kg, PN group) or ciprofol (0.4 mg/kg, CN group). Anesthesia was maintained by continuous intravenous infusion of propofol or ciprofol. The incidence of cardiopulmonary adverse reactions (respiratory depression, hypotension, bradycardia), changes in heart rate (HR), mean arterial pressure (MAP), and pulse oxygen saturation (SpO2) at different time points were observed. Additionally, drug dosage, induction time, operative time, recovery time, injection pain, postoperative uterine contraction pain, and surgeon satisfaction were compared between the two groups. Results: Compared with PN, CN demonstrated a lower incidence of cardiopulmonary adverse reactions (15% vs. 40%, P P P P P > 0.05). Anesthesia induction time, operative time, and postoperative uterine contraction pain did not differ significantly between groups (P > 0.05). Conclusion: Intravenous anesthesia using ciprofol 0.4 mg/kg combined with nalbuphine 0.1 mg/kg is safe and effective for painless abortion. It offers advantages such as fewer cardiopulmonary adverse events, faster recovery, and less injection pain, making it worthy of clinical application and promotion.
VL - 14
IS - 1
ER -
Huang, Z., Gong, W., Feng, T., Zhang, Z., Yu, Z. (2026). Comparison of Ciprofol-nalbuphine and
Propofol-nalbuphine Sedation During Painless Abortion:
A Randomized Controlled Trial. Journal of Gynecology and Obstetrics, 14(1), 37-44. https://doi.org/10.11648/j.jgo.20261401.14
Huang, Z.; Gong, W.; Feng, T.; Zhang, Z.; Yu, Z. Comparison of Ciprofol-nalbuphine and
Propofol-nalbuphine Sedation During Painless Abortion:
A Randomized Controlled Trial. J. Gynecol. Obstet.2026, 14(1), 37-44. doi: 10.11648/j.jgo.20261401.14
Huang Z, Gong W, Feng T, Zhang Z, Yu Z. Comparison of Ciprofol-nalbuphine and
Propofol-nalbuphine Sedation During Painless Abortion:
A Randomized Controlled Trial. J Gynecol Obstet. 2026;14(1):37-44. doi: 10.11648/j.jgo.20261401.14
@article{10.11648/j.jgo.20261401.14,
author = {Zu-chao Huang and Wan-wan Gong and Tian-kui Feng and Zhong Zhang and Zhi-yang Yu},
title = {Comparison of Ciprofol-nalbuphine and
Propofol-nalbuphine Sedation During Painless Abortion:
A Randomized Controlled Trial},
journal = {Journal of Gynecology and Obstetrics},
volume = {14},
number = {1},
pages = {37-44},
doi = {10.11648/j.jgo.20261401.14},
url = {https://doi.org/10.11648/j.jgo.20261401.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jgo.20261401.14},
abstract = {Objective: Despite the widespread use of propofol for painless abortion, it is frequently associated with cardiopulmonary adverse events. Ciprofol, a novel intravenous anesthetic agent, demonstrates a more favorable respiratory and hemodynamic stability profile. The aims of this study were to evaluate the efficacy and safety of ciprofol-nalbuphine combination in mitigating cardiopulmonary complications and enhancing recovery following painless abortion procedures. Methods: A total of 120 patients scheduled for elective painless abortion, aged 18-39 years, ASA physical status I or II, were selected. They were randomly divided into a Propofol-Nalbuphine group (PN group, n = 60) and a Ciprofol-Nalbuphine group (CN group, n = 60) using a random number table. Anesthesia was induced by intravenous injection of nalbuphine 0.1 mg/kg, followed 3 minutes later by intravenous injection of propofol (2 mg/kg, PN group) or ciprofol (0.4 mg/kg, CN group). Anesthesia was maintained by continuous intravenous infusion of propofol or ciprofol. The incidence of cardiopulmonary adverse reactions (respiratory depression, hypotension, bradycardia), changes in heart rate (HR), mean arterial pressure (MAP), and pulse oxygen saturation (SpO2) at different time points were observed. Additionally, drug dosage, induction time, operative time, recovery time, injection pain, postoperative uterine contraction pain, and surgeon satisfaction were compared between the two groups. Results: Compared with PN, CN demonstrated a lower incidence of cardiopulmonary adverse reactions (15% vs. 40%, P P P P P > 0.05). Anesthesia induction time, operative time, and postoperative uterine contraction pain did not differ significantly between groups (P > 0.05). Conclusion: Intravenous anesthesia using ciprofol 0.4 mg/kg combined with nalbuphine 0.1 mg/kg is safe and effective for painless abortion. It offers advantages such as fewer cardiopulmonary adverse events, faster recovery, and less injection pain, making it worthy of clinical application and promotion.},
year = {2026}
}
TY - JOUR
T1 - Comparison of Ciprofol-nalbuphine and
Propofol-nalbuphine Sedation During Painless Abortion:
A Randomized Controlled Trial
AU - Zu-chao Huang
AU - Wan-wan Gong
AU - Tian-kui Feng
AU - Zhong Zhang
AU - Zhi-yang Yu
Y1 - 2026/02/06
PY - 2026
N1 - https://doi.org/10.11648/j.jgo.20261401.14
DO - 10.11648/j.jgo.20261401.14
T2 - Journal of Gynecology and Obstetrics
JF - Journal of Gynecology and Obstetrics
JO - Journal of Gynecology and Obstetrics
SP - 37
EP - 44
PB - Science Publishing Group
SN - 2376-7820
UR - https://doi.org/10.11648/j.jgo.20261401.14
AB - Objective: Despite the widespread use of propofol for painless abortion, it is frequently associated with cardiopulmonary adverse events. Ciprofol, a novel intravenous anesthetic agent, demonstrates a more favorable respiratory and hemodynamic stability profile. The aims of this study were to evaluate the efficacy and safety of ciprofol-nalbuphine combination in mitigating cardiopulmonary complications and enhancing recovery following painless abortion procedures. Methods: A total of 120 patients scheduled for elective painless abortion, aged 18-39 years, ASA physical status I or II, were selected. They were randomly divided into a Propofol-Nalbuphine group (PN group, n = 60) and a Ciprofol-Nalbuphine group (CN group, n = 60) using a random number table. Anesthesia was induced by intravenous injection of nalbuphine 0.1 mg/kg, followed 3 minutes later by intravenous injection of propofol (2 mg/kg, PN group) or ciprofol (0.4 mg/kg, CN group). Anesthesia was maintained by continuous intravenous infusion of propofol or ciprofol. The incidence of cardiopulmonary adverse reactions (respiratory depression, hypotension, bradycardia), changes in heart rate (HR), mean arterial pressure (MAP), and pulse oxygen saturation (SpO2) at different time points were observed. Additionally, drug dosage, induction time, operative time, recovery time, injection pain, postoperative uterine contraction pain, and surgeon satisfaction were compared between the two groups. Results: Compared with PN, CN demonstrated a lower incidence of cardiopulmonary adverse reactions (15% vs. 40%, P P P P P > 0.05). Anesthesia induction time, operative time, and postoperative uterine contraction pain did not differ significantly between groups (P > 0.05). Conclusion: Intravenous anesthesia using ciprofol 0.4 mg/kg combined with nalbuphine 0.1 mg/kg is safe and effective for painless abortion. It offers advantages such as fewer cardiopulmonary adverse events, faster recovery, and less injection pain, making it worthy of clinical application and promotion.
VL - 14
IS - 1
ER -