Abstract
Despite the benefits of laparoscopic cholecystectomy, the incidence of bile duct disruption has increased significantly over the years, from a range of 0.1 to 0.2% during the open cholecystectomy (CA) era to a range of 0.4 to 0.6% in the laparoscopic cholecystectomy (LC) era. and 0.72% per year in single-port cholecystectomy. Most prevention or safety interventions alone have not achieved adequate implementation and outcomes in terms of bile duct injury have remained largely unchanged. Nothing could be further from the truth than trying to establish infallible formulas for the prevention of surgical injuries of the bile duct. Bile duct injury secondary to cholecystectomy is one of the most catastrophic complications for both the patient and the surgeon due to its repercussions. The main factor in addressing this problem is prevention, performing gentle and careful surgical technique, recognizing when the situation is beyond the surgeon's ability, and being vigilant to ask for experienced help. It must be recognized that the latter and the decision to convert are not signs of incapacity, but of good judgment. Perhaps one of the most important principles is to keep in mind that any surgeon can present them. Only from this premise can the recommendations of the 10 high safety requirements and the 7 transoperative maneuvers for a safe cholecystectomy be useful, which together with a structured and competency-based teaching-learning process can further reduce the rate of surgical disruption of the bile duct.
|
Published in
|
Journal of Cancer Treatment and Research (Volume 13, Issue 3)
|
|
DOI
|
10.11648/j.jctr.20251303.22
|
|
Page(s)
|
41-51 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Bile Duct Disruption, Cholecystectomy, Bile Duct Injury, Bile Duct, Safety Vision
1. Introduction
The gold standard for the treatment of gallstone disease is laparoscopic cholecystectomy (LC); more than 90% of cholecystectomies are performed annually with this approach. In more than 99% of cases, the procedure is performed without complications. The correct identification of the structures of the biliary bladder hilum (cystic duct and artery) recommended by Strasberg, and the 360° verification (Doublet), are the most effective safety maneuvers in the prevention of surgical disruption of the bile duct (BVD). However, they continue to occur, so we consider that these criteria are not sufficient for their prevention. Multiple criteria (SAGES, Delphi) have been mentioned, but most of these criteria have not achieved adequate implementation and the results in terms of bile duct injury have remained almost unchanged, with no decrease in the risk of injury
| [1] | Giger U, Ouaissi M. Bile duct injury and use of cholangiography during laparoscopic cholecystectomy. Br J Surg. 2011 Mar; 98(3): 391-6 https://doi.org/10.1002/bjs.7335 |
| [2] | Strasberg S, Hertl M, Soper N. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995 Jan; 180(1): 101 -25. |
[1, 2]
. The development of technology has allowed the implementation of alternative methods such as single port or robotic-assisted surgery.
| [3] | De U. Evolution of cholecystectomy: A tribute to Cari August Langenbuch. Indian J Surg. 2004 Mar- Apr; 66(2): 97-100. |
[3]
.
The surgeon should also be mentioned as a risk factor for BVD, both in his knowledge and in his know-how. The competencies, skills and abilities that must be obtained over time to perform surgeries. This lack in the educational field can be significantly reduced with an adequate competency-based curriculum that includes simulators, to later and always in a tutorial form, initiate surgery in living patients, in this way the line of learning is shortened and therefore the DQVB is reduced. With this teaching-learning process and the review of multiple publications, reinforcing knowledge and know-how allows us to suggest 10 safety criteria and 7 transoperative safety maneuvers in cholecystectomy.
2. Surgical Bile Duct Disruption
Benign bile duct lesions are those solutions of continuity or obstructions of the bile ducts caused by surgery, the most common is laparoscopic cholecystectomy in 95%, vascular lesions of the biliary tree are also included and can be of the hepatic arteries, common, right or left, as well as the portal vein.
.
Considering that cholecystectomy is one of the most common procedures, and that more than 750,000 cholecystectomies are performed per year in the United States alone, the number of patients with BVDC could be higher than 3,000 cases per year.
| [5] | Vera Rodríguez F and Magaña Sánchez. Catastrophic bile duct injuries. In: Mexican Association of General Surgery, A. C.; Noyola Villalobos HF, Magaña Sánchez, coordinators. PROACI Surgery Update Program; Cycle 1. Mexico City: Artmed Panamericana; 2017, p. 109-32 (Distance Continuing Education System, v. 4). |
[5].
Despite the benefits of laparoscopic cholecystectomy, the incidence of bile duct injury has increased significantly over the years, from a range of 0.1 to 0.2% during the open cholecystectomy (AC) era to a range of 0.4 to 0.6% in the laparoscopic cholecystectomy (LC) era. and 0.72% per year in single-port cholecystectomy, which has repercussions in the clinical, labor, economic and legal fields. In studies carried out in our country by Mercado and Pérez-Morales, an incidence of BVDC of 0.4% and 0.6% respectively is described, which is within international ranges.
| [6] | Velasco-Espinoza MF et al. Comparative analysis of bile duct lesions: prevalence in patients with laparoscopic cholecystectomy and open cholecystectomy at the General Hospital 450 in Durango, Mexico. General Surgeon 2018; 40(3): 159-163. |
[6]
.
The general surgeon must be prepared to face surgical scenarios in which it is not possible to perform a critical safety view (VCS), this can be found in less than 1% due to severe inflammation of the gallbladder; the deformity of the conventional anatomy caused by such inflammation, the presence of aberrant bile ducts and arterial vessels, and the learning curve of the general surgeon in laparoscopic or open surgery, leading to disruption of the bile ducts or complex biliovascular lesions that can end in serious complications and even death.
Complications that arise after BVDD are biliary stenosis, hepatic atrophy, cholangitis, and intrahepatic lithiasis. Later, secondary fibrosis or cirrhosis and portal hypertension, developed by prolonged biliary obstruction associated with recurrent cholangitis, may develop.
| [7] | Limaylla-Vega H, Vega-Gonzales E. Iatrogenic lesions of the bile ducts. Rev Gastroenterol Peru. 2017; 37(4): 350-6. |
[7]
In this context, the economic and legal impact must also be considered. Bile duct injury is the leading cause of post-CL lawsuits and results in compensation payments of more than $500,000, and the annual cost of litigation exceeds $1 billion in the United States alone.
| [8] | Kumar M, Agrawal CS. Three port versus standars four-port laparoscopic cholecysrectomy: a Randomomized controlled clinical trial in a community-based teaching hospital in easterm Nepal. JSLS. 2007 Jul-Sep; 11(3): 358-62 PMID: 17931519 PMCID: PMC3015828. |
[8]
.
3. Aetiology
The most frequent cause is the incorrect identification of the structures of Calot's triangle, due to severe tissue inflammation with deformity of the conventional anatomy of the gallbladder and billiard pathway that leads the surgeon to confuse the main bile duct with the cystic duct.
| [5] | Vera Rodríguez F and Magaña Sánchez. Catastrophic bile duct injuries. In: Mexican Association of General Surgery, A. C.; Noyola Villalobos HF, Magaña Sánchez, coordinators. PROACI Surgery Update Program; Cycle 1. Mexico City: Artmed Panamericana; 2017, p. 109-32 (Distance Continuing Education System, v. 4). |
[5]
The surgeon's experience strongly influences the incidence of BVD. It is estimated that 90% of these occur during the first 30 cases of the newly graduated surgeon (who had to carry out a structured and competency-based teaching-learning process). For a long time, the responsibility for this iatrogenic increase has been attributed to the learning curve of this approach. Laparoscopic vision involves a new two-dimensional vision, a different angle of vision (tangential), the use of new instruments and the absence of touch. It requires visuospatial learning and prior training at different levels to gain experience.
4. Risk Factors for Bile Duct Injury
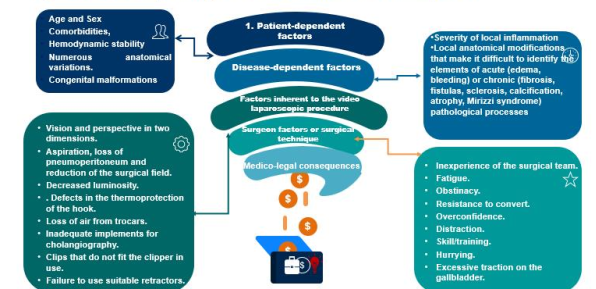
The predisposing factors for BVDD can be grouped into the following categories in
Figure 1.
5. Teaching-learning Process
It should be determined whether safe cholecystectomy is a teaching method applicable to emergency and elective procedures.
| [9] | Gutiérrez Samperio. Technology and simulation as an educational strategy in the acquisition of surgical skills and abilities. Surgeon January-March 2016 Vol. 38, no. 1 / p. 5-6. |
[9]
Some of the risk factors for DQVB are the surgeon both in his knowledge and in his know-how. This deficiency comes from the educational field, which can be significantly reduced with an adequate competency-based curriculum that includes knowledge of surgical anatomy, surgical techniques and surgical criteria; in addition to the know-how with skills and abilities that can be advanced in simulators with specific rubrics and staggered with basic and advanced exercises, to later and always in a tutorial form start surgery in living patients, in this way we shorten the line of learning and therefore reduce the DQVB.
Simulation is a training methodology for the acquisition of surgical skills and abilities that reproduces reality in a controlled and safe environment. Its main objective is to acquire and/or improve psychomotor skills, although it also supports the consolidation of communication, coordination, professionalism and leadership skills.
| [10] | Master JM, Palazuelos AC. Clinical simulation as a tool to facilitate culture change in health organizations: practical application of advanced learning theory. Rev colomb anesthesioly. 2014; 42(2): 124-128 https://doi.org/10.5554/issn.2256-2087 |
[10]
.
In recent years, simulation has been booming since in order to complete the adequate training of a scientific surgeon we must not only impact knowledge (transmitting current knowledge based on evidence), but above all on know-how (achieving surgical autonomy), and promoting the being, through responsible, committed and supportive training, in short, ethics (it is not the time it takes, but how the patient evolves).
Simulation, following the experiences of Fitts and Posner, indicate that it requires advancing in a progressive and complex way over three stages:
1) Cognitive stage. Where the student is taught what the skill consists of, how it should be performed and what type of equipment or technological development it requires.
2) Integrative stage. Where the student practices in different simulators until the skill is obtained; and where he could have had errors that were corrected without any damage and repeated the procedure so many times it was necessary until it was standardized.
3) Autonomous stage. Where the student already performs the manual skill acquired in a routine and safe way, so that at the surgical moment he no longer distracts his attention from how the procedure is performed (atraumatic tissue management, bimanual dexterity, depth perception, surgical knots, handling of staplers, etc.). Therefore, he devotes all his attention to the specific surgical technique and the general conditions of his patient.
| [11] | Fernández Vázquez JM: Code of Medical Ethics. Soc Méd Orto, Méx, 2011: 225-41 PMC3399321 Identificador de producto principal: 22826677. |
[11]
.
Simulation for the acquisition of surgical skills and abilities represents an ethical necessity since, as Ziv mentions, through this procedure patients are protected and are not the object of learning.
| [12] | ZIV A. Simulation-Based Medical Education-From Vision to Reality. Educación Médica 2007; 10(3): 147-148. |
[12]
Simulation favors the acquisition of skills and abilities as it is the only object of interest when performing the exercise, taking away from the mind the clinical conditions and the specific surgical technique that our patient presents and requires. And conversely, in the real surgical moment, the main thing is to make clinical and technical decisions that the patient requires, and not to have detractors of how to perform some surgical skill that should already be performed automatically. Definitely, the acquisition of surgical skills and abilities is faster with simulation, since we can repeat the exercise as many times as necessary (like airline pilots), simulating any surgical scenario, without waiting for a real clinical case to allow it.
| [13] | Chuang Kl, Corley D, Postlethwaite DA, Merchant M, Harris HW. Does ¡n-creased experience with laparoscopic cholecystectomy yield more complex bile duct injuries? Am J Surg. 2012 Apr; 203(4): 480-7. ID de producto: PMC7364374 ID de producto: 32704435. |
| [14] | Magaña Sánchez IJ. Acute cholecystitis. In: Mexican Association of General Surgery, A. C.; Noyola Villalobos HF, Magaña Sánchez IJ, coordinators, PROACI Surgery Update Program: Cycle 1. Mexico City: Artmed Panamericana; 2017. p. 85-108 (Distance Continuing Education System, v. 4). |
[13, 14]
.
6. Safety Culture
Multiple efforts have been made to improve safety in LC in the preoperative, transoperative, and postoperative periods, including:
1) The appropriate time for the surgical procedure;
2) The appropriate selection of cases;
3) Evaluation of surgeons' training;
4) Photo documentation of critical steps of surgery.
The performance of a transoperative cholangiography.
Most of these interventions have failed to achieve adequate implementation and the results in terms of bile duct injury have remained almost unchanged,
| [1] | Giger U, Ouaissi M. Bile duct injury and use of cholangiography during laparoscopic cholecystectomy. Br J Surg. 2011 Mar; 98(3): 391-6 https://doi.org/10.1002/bjs.7335 |
| [2] | Strasberg S, Hertl M, Soper N. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995 Jan; 180(1): 101 -25. |
[1, 2]
There are currently two international initiatives aimed at adopting a culture of safety in the performance of laparoscopic cholecystectomy, the objective of which is its widespread adoption aimed at increasing patient safety and improving surgical outcomes. These initiatives are the prevention and treatment of bile duct injuries: the 2012 European Association for Laparoscopic Surgery and SAGES guidelines, the Delphi expert consensus, Critical View of Safety during Laparoscopic Cholecystectomy,
| [2] | Strasberg S, Hertl M, Soper N. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995 Jan; 180(1): 101 -25. |
[2]
Where 15 critical factors were identified to improve outcomes and reduce the incidence of bile duct injuries.
| [15] | Pucher PH, Brunt LM, Fanelli RD, Asbun HJ, Aggarwal R. SAGES expert Delphi consensus; critical factors for safe surgical practice in laparoscopic cholecystectomy. Surg Endose. 2015 Nov; 29(11): 3074-85. https://doi.org/10.1007/s00464-015-4079-z |
[15]
.
In Mexico, there are the Clinical Practice Guidelines for Cholecystitis and Bile Duct Injury prepared by the Mexican Association of General Surgery, as well as the Clinical Practice Guide for the Diagnosis and Treatment of Cholecystitis and Cholelithiasis of the National Center for Technological Excellence in Health (CENETEC), which must be known and implemented in the medical environment.
.
Since the primary cause of BVDQ is misidentification of the main BV or an aberrant duct as a cystic duct (CC), the surgeon should use an artery and CC identification method. Among the methods used, the following have been highlighted:
1) Tristructure method: we must identify during LC: CC, common hepatic duct and common bile duct.
2) Fischer's method: consists of separating the gallbladder completely from the gallbladder bed from the bottom towards the infundibulum as in open surgery, until it hangs from the artery and the CC. This is especially difficult in the case of intrahepatic or severely inflamed vesicles. The separation of the gallbladder from the liver bed also tends to bleed more, as it has not previously ligated to the cystic artery.
3) Infundibulum technique: consists of identifying the CHD by joining the vesicular infundibulum. It is the most widely used technique in most centres today. It has the disadvantage of not preventing BVDD in patients with occult cystic duct syndrome. For this reason, different groups systematically recommend the use of intraoperative cholangiography (IOC) with this type of technique.
4) Strasberg's Critical Sight Technique: consists of the dissection and release of Calot's triangle until the artery and cystic duct (CC) are exposed and the base of the liver is exposed. Once this view is reached, these structures can only correspond to the duct and the cystic artery. To perform a correct VCS, three maneuvers are required:
a) Dissect Calot's triangle completely, skeletonizing the cystic duct and artery and removing all existing fat and fibrosis.
b) Separate the lower part of the gallbladder from the hepatic bed by exposing the non-peritonized side of the gallbladder.
c) Observe in a 360° view that only two structures enter the gallbladder.
Doublet score: The Doublet score is the sum of VSC in two anterior and posterior planes of the already dissected cholecystoduodenal ligament, giving us three points for each view, with a maximum score of 6 points. Doublet's photo documentation should provide the dynamic advantages that laparoscopic surgery allows, although it is possible to apply it in CA. It is qualified by two photographs, since it is the permanent, accessible and economical method that is available for easy reproduction. The highest rating of each criterion between the two perspectives should be taken, in order to sufficiently distinguish the dissection. If the sufficient rating is achieved, 5 points or more, then it means that the structures are already well distinguished, and the VCS is satisfactorily identified.
Other security methods:
Cholangiography: (CIO) IOC can help prevent BVCD in at least three ways: It shows the diversity of the biliary tree and its abnormalities, helps the surgeon identify patients at risk for BVCD due to abnormal anatomies, and if BVDC has occurred, allows for identification and repair.
IOC has been shown to be cost-effective, especially when used by less experienced surgeons and if there are risk factors. Other studies do not accept that IOC prevents the incidence of BVCD and highlight the increase in total surgery time.
Intraoperative laparoscopic ultrasound: in a recent multicenter study, its advantages for the prevention of BVCD are highlighted, although it is another very expensive method and sometimes not available in all hospitals, which does not completely replace IOC but opens up a hopeful future.
| [17] | Ruiz Gómez. et al. Iatrogenic lesions of the bile duct. CIR ESP. 2010; 88(4): 211-221 https://doi.org/10.1016/j.ciresp.2010.03.045 |
| [18] | Rodríguez Fernández. Current knowledge about iatrogenic bile duct lesions. "Saturnino Lora" Clinical Surgical Teaching Hospital, Santiago de Cuba. Vol. 56, No. 3 (2017). |
[17, 18].
Finally, the most innovative trend in 2017 to face anatomical variants and avoid biliary lesions during cholecystectomy is Precision Multimodal Navigation, which combines virtual reality, intraoperative augmented reality, infrared cholangiography with indocyanine green and software for manipulating images previously obtained by magnetic resonance imaging.
| [19] | Loera-Torres MA, Fuentes M, Alvarado O, Noyola H. Tips and tricks against anatomical variants of the bile duct. International echoes in general surgery. Module X. Cholecystectomy and bile duct 2018. |
[19]
Another method not available in all hospitals.
7. Predictors of Difficult Cholecystectomy
1) There is currently no objective measure to establish the difficulty in a cholecystectomy. The identification of these variables becomes a challenge, the most important factors identified in the studies were: documented acute cholecystitis (clinical, biochemical and imaging) 100%, history of acute cholecystitis 100%, male gender 85%, history of upper hemiabdomen surgery 85%, obesity 75%, age over 55 years 70%, leukocytosis 100%, wall thickening by USG 100%. Other factors, although less significant for the need for conversion, were: multiple pictures (from greater than 2 to greater than 10), palpable gallbladder, ASA classification 3 or 4 and the surgeon's experience 75%, hydrocholecyst, atrophic sclerotic gallbladder, impacted litho.
| [20] | Pinto Angulo Víctor Manuel. The surgeon's opportunity for a nightmarish gallbladder. In: International echoes in general surgery. Module X. Cholecystectomy and bile duct. Mexico. Mexican Association of General Surgery. 2018. 15-25. |
| [21] | Buitrago-Jaramillo 2019 Buitrago-jaramillo. Iatrogenic lesions of the bile duct. Hepatopancreatobiliary surgery management guidelines. August 2019. |
[20, 21]
See
Figure 1 of risk factors.
Figure 1. Adapted by the author. Taken from Ruiz, 2010- Loera-Torres 2018.
2) Tokyo: The Tokyo 2018 Guidelines (TG18) expand the indications for CL in difficult conditions for each level of severity. As a result of expanding the indications for LC to treat acute cholecystitis (AC), it is absolutely necessary to avoid any increase in bile duct injury, particularly vasculo-biliary injury.
| [22] | Jiménez Chavarría Enrique. Competency-Based Strategy for Safe Cholecystectomy. International echoes in general surgery. Module X. Cholecystectomy and bile duct 2018. |
[22]
.
3) Parkland Visual Assessment: The
Parkland Grading Scale (PGS) for cholecystitis was developed to stratify the severity of gallbladder disease. That easy-to-implement, five-level rating system, based on anatomy and inflammatory changes, was shown to be highly reproducible.
This classification can predict a difficult cholecystectomy and propose a cholecystostomy or a subtotal cholecystectomy from the beginning.
The above techniques help to achieve lower LQVB; however, it is necessary to recognize that they have limitations. Not too much ego-emotional effort should be made for the conversion to an open procedure to take place. If the laparoscopic procedure is complex, it should be converted. If after conversion the difficulty in resolving it continues, cholecystostomy should be considered, or subtotal cholecystectomy in each of its variants (fenestrated or reconstructed) represents the surgical technique of choice.
| [24] | Strasberg SM, Pucci MJ, Brunt LM, Deziel DJ. Subtotal Cholecystectomy-”Fenestrating" vs “Reconstituting” Subtypes and the Prevention of Bile Duct Injury: Definition of the Optimal Procedure in Difficult Operative Conditions. J Am Coll Surg. 2016 Jan; 222(1): 89-96. https://doi.org/10.1016/j.jamcollsurg.2015.09.019 |
[24]
These consist of: 1. Reconstructed subtotal cholecystectomy. Resection of the fundic part of the gallbladder leaving a gallbladder remnant which is sutured. In fenestrated fistula, the gallbladder is not occluded, but the cystic can be sutured internally, and although it has a higher incidence of postoperative biliary fistula, it is not associated with recurrent cholecystolithiasis. And 2. Fenestrated subtotal cholecystectomy. In this subtotal cholecystectomy, the gallbladder is not sutured, but the cystic duct is sutured internally.
It is better to inform the patient that he or she requires a second operation to resolve the problem and not a second operation to repair serious damage. As Strasberg points out, "
It is important to remember that gallbladder disease is a benign entity and does not warrant a thoughtless attempt to proceed with an operation of considerable technical difficulty."
| [25] | Mercado et al. What should be done in case of suspicion or injury to the bile duct? Review article. Mexican Association of Endoscopic Surgery, A. C. Vol. 11 No. 2 Apr.-Jun. 2010. |
[25]
.
Most of these interventions alone have failed to achieve adequate implementation and the results in terms of bile duct injury have remained largely unchanged.
| [1] | Giger U, Ouaissi M. Bile duct injury and use of cholangiography during laparoscopic cholecystectomy. Br J Surg. 2011 Mar; 98(3): 391-6 https://doi.org/10.1002/bjs.7335 |
| [2] | Strasberg S, Hertl M, Soper N. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995 Jan; 180(1): 101 -25. |
[1, 2]
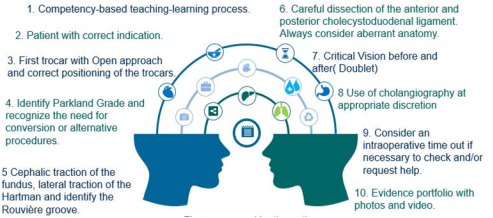
To date, there are no widely disseminated validated scoring systems that are used to intraoperatively stratify the severity of inflammation of a gallbladder. Perhaps one of the most important and real principles is to keep in mind that any surgeon can present them. Only from this premise can the following 10 recommendations be useful, which should be taken as an airplane pilot does before taking off he must check that everything is in proper function, likewise we must check that we have all the elements and tools for a safe intervention. (
Figure 2). And by the way, this should be the case for any surgery. From these 10 recommendations, 7 transoperative maneuvers are necessary to avoid a bile duct disruption. Just as knowledge allows us to distinguish a difficult cholecystectomy and proceed, as already mentioned, to a subtotal shunt or cholecystectomy. Know-how allows us to perform these maneuvers safely. (see Surgical technique and images 1-7) The knowledge of the being allows us to distinguish when it is necessary to change our behavior.
Figure 2. Prepared by the Author.
It is worth mentioning that we must leave the division of laparoscopic or open cholecystectomy, the safety measures are the same for both, they are for the patient and for the surgery team, which is why they must be complied with in the two access routes.
The surgeon must establish in his or her interview with the patient, a good informed consent that includes: the indication for cholecystectomy, risks of the type of intervention (laparoscopic) and the conversion to an open procedure and the reasons for this must be adequately explained, the frequency with which a lesion occurs (0.3 to 0.6%) and that its causes are multiple and what are its possible solutions. from endoscopic management with sphincterotomy and prosthesis for lateral lesions to that of a biliodigestive diversion, emphasizing that these complications are uncommon
| [25] | Mercado et al. What should be done in case of suspicion or injury to the bile duct? Review article. Mexican Association of Endoscopic Surgery, A. C. Vol. 11 No. 2 Apr.-Jun. 2010. |
[25].
8. Surgical Technique
The optic trocar has a caliber of 10 mm and is in the umbilical area or in a slightly supraumbilical position, in obese patients.
| [26] | Deguines JB, Qassemyar Q, Dhahri A, Brehant O, Fuks D, Verhaeghe P, et al. Technique of open laparoscopy for supramesocolic surgery in obese patients. Surg Endosc 2010; 24: 2053-5. |
[26]
Once optics have been introduced, a global examination of the peritoneal cavity is carried out to check that there are no adhesions or other undiagnosed pathologies. The other three trocars are then introduced under visual control. Its insertion point is variable depending on the patient's anatomy. Apply the visual scale of the Parkland Classification and regulate behavior.
Good exposure of the hepatic pedicle is essential before initiating any surgical dissection. The hepatic pedicle is exposed in a plane constituted by a supero-inferior space retracting upwards the inferior aspect of segment IV and downwards the duodenopancreatic block. In open surgery, a malleable valve is used to elevate the liver and the hand of the first assistant to descend the first portion of the duodenum. In laparoscopic surgery, a hepatic separator inserted in the epigastric trocar and the patient in the anti-Trendelenburg position will have been used, respectively, or cephalic traction of the gallbladder fundus with port 4. There are often some adhesions in the gallbladder and omentum or hepatoduodenal ligament; rarely it is the right transverse colon or the duodenum. These adhesions are sectioned with scissors flush with the gallbladder wall. A release of epiploic adhesions is carried out in a descending direction starting from the liver. This allows the body of the gallbladder to be visualized.
This surgical time should be done gently so as not to injure the transverse colon or duodenum, which may be attached to the gallbladder. Usually, in acute cholecystitis, the gallbladder is stressed and its wall is inflamed. The puncture of the gallbladder with a large needle allows both the biliary contents to be evacuated and a sample to be taken for bacteriological study. This procedure allows the gallbladder to be held in place with a grasping forceps.
After analyzing step by step the surgical maneuvers to achieve better exposure and identification of the anatomical elements of the hepatocystic triangle, we have come to define those that seem most useful to us and calling them the 7 high security transoperative maneuvers for cholecystectomy. In order to gain a better understanding of these maneuvers, it is necessary to take the center of the cholecystohepatic triangle as a reference point in laparoscopic clockwise view. So, correspondingly, when we say that some structure is pulled at "12 o'clock" we mean a vertical retraction upwards on our monitor screen, or if it is at "7 o'clock", the traction will be towards the lower left quadrant of the monitor screen and so on.
First maneuver: Retraction of the fundus of the gallbladder at 10 or 12 and the Hartman at 7. The first instrument introduced into the abdominal cavity is a fenestrated grasp forceps that is inserted under visual control through the epigastric trocar. With it, the bottom of the gallbladder is firmly grasped, moving it outwards and up (at 10 o'clock), while the lower edge of the right lobe of the liver is raised. The control of it is carried out by the assistant with his right hand. A fenestrated grasping forceps is inserted into the right lateral trocar, holding the surgeon's left hand. With it, he pulls the infundibulum of the gallbladder down and out (at 7 o'clock). The surgeon, with his left hand, grasps the lateral aspect of the Hartmann pouch with a grasper and retracts it into the lower left quadrant of the laparoscopic image. This manoeuvre is intended to "open" the cholecysto-hepatic triangle and is probably the most relevant during surgery. The dissecting hook, or scissors, are inserted by the trocar operator. (
Figure 3).
Figure 3. First Maneuver. Infrahepatic exposure. The fundus of the gallbladder retracts toward the anterior aspect of the abdomen (toward the 10-12 o'clock radius) and the bursa of Hartmann retracts laterally and downward (toward the 7 o'clock radius).
This cholecystectomy time allows the gallbladder neck to be separated from the main bile duct and the cystic pedicle to be horizontalized, thus moving it away from the hepatic pedicle, opening Calot's triangle and reducing the risk of injury to the main bile duct during cystic pedicle dissection.
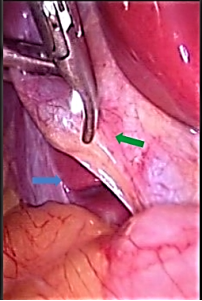
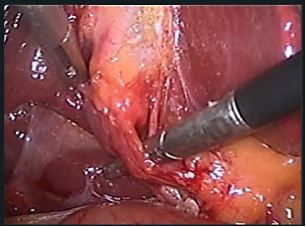
Second manoeuvre: The careful view of the Rouviere Groove and the coat of arms of Mc Elmoyle. To be able to start dissection above these structures. An alternative reference point, to guide the beginning of dissection, is the sulcus of Rouvière or incisure hepatis dextra (IHD), also known as the incisure of Gans, represents an important anatomical landmark. The shield of Mc Elmoyle, is the union of Hartman's bag with the infundibulum, it should not be dissected under these elements (
Figure 4).
Figure 4. Second maneuver. Identification of the Rouviere Groove (blue arrow) and McElmoyle's Coat of Arms (Green Arrow).
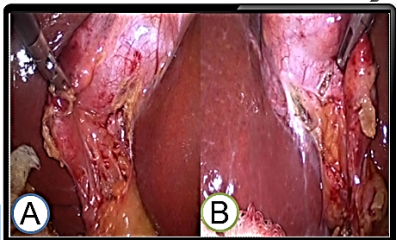
Third maneuver: Exposure of Calot's triangle and hepatocystic. To expose the posterior aspect of the triangle, the vesicular infundibulum will be tilted upwards and forwards by means of the atraumatic forceps, while the separator is pushed back into the hepatic pedicle. (
Figure 5).
Figure 5. Third maneuver. A. Cholecystoduodenal ligament (white arrow) its vertex and its anterior aspect. B. Exposure of the posterior aspect of the vesicular infundibulum. (black arrow) Continuity with the gallbladder peritoneum (Dotted line).
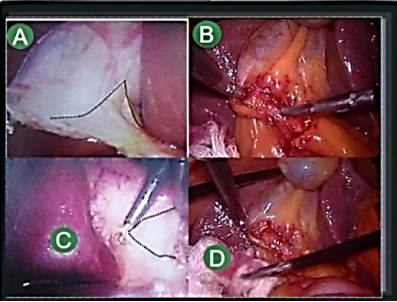
Fourth maneuver: Dissection of the hepatocystic triangle. It begins at the junction between the infundibulum and the cystic duct through the incision of the anterior peritoneal sheet, and then the posterior one a few millimeters from the gallbladder wall. Throughout the dissection, contact with the gallbladder is maintained. The infundibulocistic junction should be clearly visualized, staying away from the cysticocholedocus junction and avoiding dissecting the VBP. Always above the Rouviere furrow. (Figura 6) The instrument of choice continues to be the electrocoagulator, although, depending on the surgeon's preference and difficulties, a dissecting forceps or a mounted buffer may be used. The advantage of the hook lies in isolating each minor anatomical structure through the triangle and sectioning them after identification and electrocoagulation.
Figure 6. Fourth maneuver. Cholecystoduodenal ligament. Perform the dissection of the structures to achieve a critical vision of safety. A and B. Stroke of release of the anterosuperior sheet of the cholecystoduodenal ligament. C and D Stroke of release of the posteroinferior sheet of the cholecystoduodenal ligament. The dotted line marks the opening of the peritoneum.
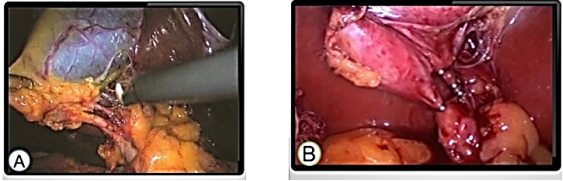
Sixth maneuver: Dissection of the elements of the triangle. We began the dissection of the elements of the cholecystohepatic triangle using a Maryland-type dissector to dissect the peritoneum at the point where the Hartmann's bursa ends and the cystic duct begins. At this site, the tendency of peritoneal dissection should be directed proximally along the lateral border of the Hartmann, toward the hepatoduodenal ligament to uncover the first tubular structure, which almost always corresponds to the cystic duct. (
Figure 8) This dissection is performed while remaining flush with the gallbladder and atraumatically. In this phase, Calot's triangle is completely released, both on its ventral and dorsal side. And the gallbladder is only attached at the bottom to the gallbladder bed; it is the technique called "flag", described by Jean Mouiel, 1991.
Figure 8. Sixth Maneuver. Dissection and exposure. Identification of what appears to be the cystic duct on the lower border of the cholecysto-hepatic triangle and identification of what appears to be the cystic artery in the center of the cholecysto-hepatic triangle.
With few exceptions, the elements of the cholecystohepatic triangle are covered by a variable amount of fat that prevents their correct identification before dissecting them. Thus, our recommendation is that, even if the anatomy is "apparently clear" before dissection, the center of the triangle should be avoided until the tubular structure that makes up its lower border has been clearly identified. In addition, it must be taken into account that anatomical variants are very frequent in this area. This is the part of the dissection that requires the most patience from the surgeon, as it is the one that has the highest risk of bleeding and injury.
Seventh maneuver: Verify that no duct returns to the liver, that only two elements go back and forth from the gallbladder. By rating Doublet three points before and three after with an identification security of 5 points or more. This maneuver is the one that provides the greatest safety in the dissection to avoid a disruption of the bile duct. In fact, no duct should be tied before this maneuver has been performed and verified. (
Figure 9).
Figure 9. Seventh Maneuver. VSC and Doublet. A. Surgical view of the complete dissection of Calot's triangle according to Strasberg's criteria (Perform Doublet). B. Control of pedicle elements.
This is the right time to give some time out, reassess or if in doubt ask for help from another surgeon. Once the high-security maneuvers for laparoscopic cholecystectomy have been completed and verified, we will be able to proceed to the corresponding ligation and division of the structures. Proceed to the cholecystectomy itself, which is performed with adequate hemostasis with subsequent removal of the gallbladder.
9. Conclusions
Bile duct injury secondary to cholecystectomy is one of the most catastrophic complications for both the patient and the surgeon due to its repercussions. The main factor in addressing this problem is prevention, performing gentle and careful surgical technique, recognizing when the situation is beyond the surgeon's capacity, and being attentive to ask for experienced help. It must be recognized that the latter and the decision to convert are not signs of incapacity but of good judgment.
Most prevention or safety interventions alone have failed to achieve adequate implementation and outcomes in terms of bile duct injury have remained largely unchanged.
| [1] | Giger U, Ouaissi M. Bile duct injury and use of cholangiography during laparoscopic cholecystectomy. Br J Surg. 2011 Mar; 98(3): 391-6 https://doi.org/10.1002/bjs.7335 |
| [2] | Strasberg S, Hertl M, Soper N. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995 Jan; 180(1): 101 -25. |
[1, 2]
Perhaps one of the most important principles is to keep in mind that any surgeon can present them. Only from this premise with a structured and competency-based teaching-learning process, can it be useful to know the 10 requirements that must be checked for high safety and to know how to do the 7 transoperative maneuvers for a safe cholecystectomy; which together with being to detect and accept when the procedure may damage and make the decision to convert in time, or perform variants of cholecystectomy can further decrease the rate of surgical disruption of the bile duct.
Abbreviations
AC | Open Cholecystectomy |
LC | Laparoscopic Cholecystectomy |
BVD | Surgical Bile Duct Disruption |
VCS | Critical Safety View |
CC | Cystic Duct |
IOC | Intraoperative Cholangiography |
Author Contributions
Juan Hernandez Orduña is the sole author. The author read and approved the final manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Giger U, Ouaissi M. Bile duct injury and use of cholangiography during laparoscopic cholecystectomy. Br J Surg. 2011 Mar; 98(3): 391-6
https://doi.org/10.1002/bjs.7335
|
| [2] |
Strasberg S, Hertl M, Soper N. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995 Jan; 180(1): 101 -25.
|
| [3] |
De U. Evolution of cholecystectomy: A tribute to Cari August Langenbuch. Indian J Surg. 2004 Mar- Apr; 66(2): 97-100.
|
| [4] |
Committee for the preparation of clinical practice guidelines. Cholecystitis clinical practice guideline. Mexico. Mexican Association of General Surgery A. C. 2014.
https://amcg.org.mx/wp-content/uploads/2020/06/colecistitis.pdf
(Accessed 26 August 2020).
|
| [5] |
Vera Rodríguez F and Magaña Sánchez. Catastrophic bile duct injuries. In: Mexican Association of General Surgery, A. C.; Noyola Villalobos HF, Magaña Sánchez, coordinators. PROACI Surgery Update Program; Cycle 1. Mexico City: Artmed Panamericana; 2017, p. 109-32 (Distance Continuing Education System, v. 4).
|
| [6] |
Velasco-Espinoza MF et al. Comparative analysis of bile duct lesions: prevalence in patients with laparoscopic cholecystectomy and open cholecystectomy at the General Hospital 450 in Durango, Mexico. General Surgeon 2018; 40(3): 159-163.
|
| [7] |
Limaylla-Vega H, Vega-Gonzales E. Iatrogenic lesions of the bile ducts. Rev Gastroenterol Peru. 2017; 37(4): 350-6.
|
| [8] |
Kumar M, Agrawal CS. Three port versus standars four-port laparoscopic cholecysrectomy: a Randomomized controlled clinical trial in a community-based teaching hospital in easterm Nepal. JSLS. 2007 Jul-Sep; 11(3): 358-62 PMID: 17931519 PMCID: PMC3015828.
|
| [9] |
Gutiérrez Samperio. Technology and simulation as an educational strategy in the acquisition of surgical skills and abilities. Surgeon January-March 2016 Vol. 38, no. 1 / p. 5-6.
|
| [10] |
Master JM, Palazuelos AC. Clinical simulation as a tool to facilitate culture change in health organizations: practical application of advanced learning theory. Rev colomb anesthesioly. 2014; 42(2): 124-128
https://doi.org/10.5554/issn.2256-2087
|
| [11] |
Fernández Vázquez JM: Code of Medical Ethics. Soc Méd Orto, Méx, 2011: 225-41 PMC3399321 Identificador de producto principal: 22826677.
|
| [12] |
ZIV A. Simulation-Based Medical Education-From Vision to Reality. Educación Médica 2007; 10(3): 147-148.
|
| [13] |
Chuang Kl, Corley D, Postlethwaite DA, Merchant M, Harris HW. Does ¡n-creased experience with laparoscopic cholecystectomy yield more complex bile duct injuries? Am J Surg. 2012 Apr; 203(4): 480-7. ID de producto: PMC7364374 ID de producto: 32704435.
|
| [14] |
Magaña Sánchez IJ. Acute cholecystitis. In: Mexican Association of General Surgery, A. C.; Noyola Villalobos HF, Magaña Sánchez IJ, coordinators, PROACI Surgery Update Program: Cycle 1. Mexico City: Artmed Panamericana; 2017. p. 85-108 (Distance Continuing Education System, v. 4).
|
| [15] |
Pucher PH, Brunt LM, Fanelli RD, Asbun HJ, Aggarwal R. SAGES expert Delphi consensus; critical factors for safe surgical practice in laparoscopic cholecystectomy. Surg Endose. 2015 Nov; 29(11): 3074-85.
https://doi.org/10.1007/s00464-015-4079-z
|
| [16] |
Group of the clinical practice guidelines for the diagnosis and treatment of cholecystitis and cholelithiasis. Clinical Practice Guideline Diagnosis and Treatment of Cholecystitis and Cholelithiasis. Mexico. CENETEC. 2009.
http://www.cenetec.salud.gob.mx/descargas/gpc/CatalogoMaestro/237_IMSS_09_Colecistitis_Colelitiasis/EyR_IMSS_237_09.pdf
(accessed August 26, 2020).
|
| [17] |
Ruiz Gómez. et al. Iatrogenic lesions of the bile duct. CIR ESP. 2010; 88(4): 211-221
https://doi.org/10.1016/j.ciresp.2010.03.045
|
| [18] |
Rodríguez Fernández. Current knowledge about iatrogenic bile duct lesions. "Saturnino Lora" Clinical Surgical Teaching Hospital, Santiago de Cuba. Vol. 56, No. 3 (2017).
|
| [19] |
Loera-Torres MA, Fuentes M, Alvarado O, Noyola H. Tips and tricks against anatomical variants of the bile duct. International echoes in general surgery. Module X. Cholecystectomy and bile duct 2018.
|
| [20] |
Pinto Angulo Víctor Manuel. The surgeon's opportunity for a nightmarish gallbladder. In: International echoes in general surgery. Module X. Cholecystectomy and bile duct. Mexico. Mexican Association of General Surgery. 2018. 15-25.
|
| [21] |
Buitrago-Jaramillo 2019 Buitrago-jaramillo. Iatrogenic lesions of the bile duct. Hepatopancreatobiliary surgery management guidelines. August 2019.
|
| [22] |
Jiménez Chavarría Enrique. Competency-Based Strategy for Safe Cholecystectomy. International echoes in general surgery. Module X. Cholecystectomy and bile duct 2018.
|
| [23] |
Madni TD, Nakonezny PA, Barrios E et al. Parkland Scale Rating for Cholecystitis Am J Surg, 2018 April, 215(4): 625-630
https://doi.org/10.1016/j.amjsurgi.2018.08.005
|
| [24] |
Strasberg SM, Pucci MJ, Brunt LM, Deziel DJ. Subtotal Cholecystectomy-”Fenestrating" vs “Reconstituting” Subtypes and the Prevention of Bile Duct Injury: Definition of the Optimal Procedure in Difficult Operative Conditions. J Am Coll Surg. 2016 Jan; 222(1): 89-96.
https://doi.org/10.1016/j.jamcollsurg.2015.09.019
|
| [25] |
Mercado et al. What should be done in case of suspicion or injury to the bile duct? Review article. Mexican Association of Endoscopic Surgery, A. C. Vol. 11 No. 2 Apr.-Jun. 2010.
|
| [26] |
Deguines JB, Qassemyar Q, Dhahri A, Brehant O, Fuks D, Verhaeghe P, et al. Technique of open laparoscopy for supramesocolic surgery in obese patients. Surg Endosc 2010; 24: 2053-5.
|
Cite This Article
-
APA Style
Orduña, J. H. (2025). Safe Cholecystectomy as a Competency-based Teaching Method to Prevent Bile Duct Disruption. Journal of Cancer Treatment and Research, 13(3), 41-51. https://doi.org/10.11648/j.jctr.20251303.22
 Copy
|
Copy
|
 Download
Download
ACS Style
Orduña, J. H. Safe Cholecystectomy as a Competency-based Teaching Method to Prevent Bile Duct Disruption. J. Cancer Treat. Res. 2025, 13(3), 41-51. doi: 10.11648/j.jctr.20251303.22
Copy
|
Download
AMA Style
Orduña JH. Safe Cholecystectomy as a Competency-based Teaching Method to Prevent Bile Duct Disruption. J Cancer Treat Res. 2025;13(3):41-51. doi: 10.11648/j.jctr.20251303.22
Copy
|
Download
-
@article{10.11648/j.jctr.20251303.22,
author = {Juan Hernandez Orduña},
title = {Safe Cholecystectomy as a Competency-based Teaching Method to Prevent Bile Duct Disruption
},
journal = {Journal of Cancer Treatment and Research},
volume = {13},
number = {3},
pages = {41-51},
doi = {10.11648/j.jctr.20251303.22},
url = {https://doi.org/10.11648/j.jctr.20251303.22},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jctr.20251303.22},
abstract = {Despite the benefits of laparoscopic cholecystectomy, the incidence of bile duct disruption has increased significantly over the years, from a range of 0.1 to 0.2% during the open cholecystectomy (CA) era to a range of 0.4 to 0.6% in the laparoscopic cholecystectomy (LC) era. and 0.72% per year in single-port cholecystectomy. Most prevention or safety interventions alone have not achieved adequate implementation and outcomes in terms of bile duct injury have remained largely unchanged. Nothing could be further from the truth than trying to establish infallible formulas for the prevention of surgical injuries of the bile duct. Bile duct injury secondary to cholecystectomy is one of the most catastrophic complications for both the patient and the surgeon due to its repercussions. The main factor in addressing this problem is prevention, performing gentle and careful surgical technique, recognizing when the situation is beyond the surgeon's ability, and being vigilant to ask for experienced help. It must be recognized that the latter and the decision to convert are not signs of incapacity, but of good judgment. Perhaps one of the most important principles is to keep in mind that any surgeon can present them. Only from this premise can the recommendations of the 10 high safety requirements and the 7 transoperative maneuvers for a safe cholecystectomy be useful, which together with a structured and competency-based teaching-learning process can further reduce the rate of surgical disruption of the bile duct.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Safe Cholecystectomy as a Competency-based Teaching Method to Prevent Bile Duct Disruption
AU - Juan Hernandez Orduña
Y1 - 2025/09/03
PY - 2025
N1 - https://doi.org/10.11648/j.jctr.20251303.22
DO - 10.11648/j.jctr.20251303.22
T2 - Journal of Cancer Treatment and Research
JF - Journal of Cancer Treatment and Research
JO - Journal of Cancer Treatment and Research
SP - 41
EP - 51
PB - Science Publishing Group
SN - 2376-7790
UR - https://doi.org/10.11648/j.jctr.20251303.22
AB - Despite the benefits of laparoscopic cholecystectomy, the incidence of bile duct disruption has increased significantly over the years, from a range of 0.1 to 0.2% during the open cholecystectomy (CA) era to a range of 0.4 to 0.6% in the laparoscopic cholecystectomy (LC) era. and 0.72% per year in single-port cholecystectomy. Most prevention or safety interventions alone have not achieved adequate implementation and outcomes in terms of bile duct injury have remained largely unchanged. Nothing could be further from the truth than trying to establish infallible formulas for the prevention of surgical injuries of the bile duct. Bile duct injury secondary to cholecystectomy is one of the most catastrophic complications for both the patient and the surgeon due to its repercussions. The main factor in addressing this problem is prevention, performing gentle and careful surgical technique, recognizing when the situation is beyond the surgeon's ability, and being vigilant to ask for experienced help. It must be recognized that the latter and the decision to convert are not signs of incapacity, but of good judgment. Perhaps one of the most important principles is to keep in mind that any surgeon can present them. Only from this premise can the recommendations of the 10 high safety requirements and the 7 transoperative maneuvers for a safe cholecystectomy be useful, which together with a structured and competency-based teaching-learning process can further reduce the rate of surgical disruption of the bile duct.
VL - 13
IS - 3
ER -
Copy
|
Download