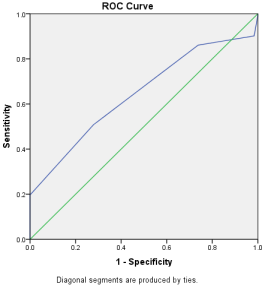
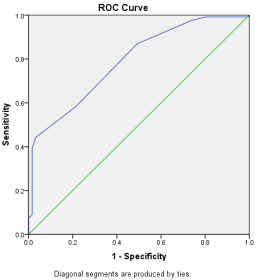
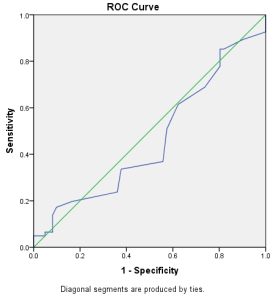
Introduction: Endometrial carcinoma is the sixth most common cancer for females in the world and the seventh most common gynecological cancer in developing countries. The values of platelet indices (MPV, PDW) and red cell distribution width (RDW) are associated with different stages of endometrial and cervical carcinoma. Thus, this study aimed to determine the relation of MPV, PDW, and RDW with endometrial carcinoma. Methods: This cross-sectional study was conducted in the Department of Gynecological Oncology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh from July 2022 to July 2023. This study included 61 women with histopathologically confirmed endometrial carcinoma (FIGO stage I to IV) as cases and 122 women with histopathologically confirmed benign endometrial disease as the control group. Result: This study found that the case group had a higher mean age (55.62 years vs. 43.75 years). Blood parameter findings showed higher mean MPV (10.46 vs. 9.96) and RDW (46.64 vs. 43.05) in cases. PDW mean was lower in cases (11.33 vs. 14.39). MPV correlated positively with the FIGO stage and histological type, while PDW had a negative correlation. ROC analysis of MPV yielded an AUC of 0.645, with a cut-off of 10.50 showing sensitivity 58%, specificity 72%, and accuracy 57%. ROC analysis of PDW yielded an AUC of 0.789, with a cut-off of 13.50 showing sensitivity 44%, specificity 97%, and accuracy 61%. Multivariant regression revealed MPV to be the strongest factor of endometrial carcinoma (OR-6.20, p=0.039). Conclusion: This study showed that the mean platelet volume (MPV) and red cell distribution width (RDW) are potential markers for detecting endometrial carcinoma.
| Published in | Journal of Cancer Treatment and Research (Volume 13, Issue 1) |
| DOI | 10.11648/j.jctr.20251301.11 |
| Page(s) | 1-9 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Platelet Indices, Red Cell Distribution Width (RDW), Endometrial Carcinoma, Uterine Bleeding
Variables | Cases (61) | Control (122) | P value |
|---|---|---|---|
Age | |||
24-43 | 7 (11.5%) | 59 (48.4%) | b0.001s |
44-63 | 40 (65.6%) | 63 (51.6%) | |
≥64 | 15 (23%) | 0 | |
MeanSD | 55.6210.24 | 43.756.63 | c0.001s |
MeanSD | 47.709.76 | ||
Median (min-max) | 46 (24-72) | ||
Educational Qualification | |||
Illiterate | 13 (21.3%) | 4 (3.3%) | b0.001s |
Primary pass | 19 (31.1%) | 21 (17.2%) | |
Secondary pass | 10 (16.4%) | 38 (31.1%) | |
Higher Secondary | 18 (29.5%) | 45 (36.9%) | |
Graduate | 1 (1.6%) | 14 (11.5%) | |
Marital status | |||
Married | 40 (26.1%) | 113 (73.9%) | a0.001s |
Widow/widower | 21 (70%) | 9 (30%) | |
Associated disease | |||
HTN | 30 (93.8%) | 2 (6.2%) | b0.001s |
DM | 31 (88.6%) | 4 (11.4%) | |
No comorbidity | 0 | 116 (100%) | |
BMI kg/m2 | |||
Normal (18.5-24.9) | 1 (1.6%) | 105 (86.1%) | b0.001s |
Overweight (25-29.9) | 23 (37.7%) | 12 (9.8%) | |
Obesity (>30) | 37 (60.7%) | 38 (4.1%) | |
Variables | Cases (61) | Control (122) | P value |
|---|---|---|---|
Menstrual history | |||
Menorrhagia | 3 (3.1%) | 94 (96.9%) | b0.001s |
Menorrhagia+ dysmenorrhea | 0 | 14 (100%) | |
Intermenstrual bleeding | 12 (85.7%) | 2 (14.3%) | |
Post-menopausal bleeding | 30 (100%) | 0 | |
Menorrhagia+ Intermenstrual bleeding | 16 (57.1%) | 12 (42.9%) | |
Parity | |||
Nullipara | 6 (9.8%) | 19 (15.6%) | b0.001s |
Para (1-2) | 22 (36.1%) | 14 (11.5%) | |
Miltipara | 33 (54.1%) | 89 (73%) | |
Contraceptive use | |||
OCP | 27 (27.8%) | 70 (72.2%) | b0.001s |
OCP+IUCD | 0 | 1 (100%) | |
OCP+Implanon | 0 | 4 (100%) | |
IUCD | 0 | 1 (100%) | |
Implanon | 0 | 15 (100%) | |
Tubal ligation | 2 (15.3%) | 11 (84.61%) | |
Nothing | 27 (51.9%) | 25 (48.70%) | |
History of HRT | |||
Yes | 2 (100%) | 0 | |
No | 0 | 0 | |
Variables | Cases (61) | Control (122) | P value |
|---|---|---|---|
Family member suffering from endometrial cancer | |||
Yes | 4 (100%) | 0 | a0.004s |
No | 57 (31.8%) | 122 (68.2%) | |
Duration of symptoms (months) | |||
meanSD | 6.312.16 | 23.258.02 | c0.001s |
meanSD | 17.6110.41 | ||
Median (min-max) | 18 (2-48) | ||
Variables | Cases (61) | Control (122) | P value |
|---|---|---|---|
MPV | |||
MeanSD | 10.461.26 | 9.961.25 | c0.012s |
MeanSD | 10.161.27 | ||
Median (min-max) | 10 (5-16) | ||
PDW | |||
MeanSD | 11.331.78 | 14.394.62 | c0.001s |
MeanSD | 13.374.16 | ||
Median (min-max) | 12 (2-53) | ||
RDW | |||
MeanSD | 46.646.18 | 43.057.03 | c0.001s |
MeanSD | 44.266.95 | ||
Median (min-max) | 44 (2-62) | ||
Variables | MPV | P value |
|---|---|---|
Correlation coefficient | ||
FIGO stage | 0.334 | d0.009s |
Histological grade | 0.166 | d0.204ns |
PDW | ||
Age | -0.357 | d0.001s |
FIGO stage | -0.202 | d0.122ns |
Histological grade | -0.284 | d0.028s |
RDW | ||
FIGO stage | 0.031 | d0.815ns |
Variables | Univariate regression (OR) | P value | Multivariate logistic regression (OR) | P value |
|---|---|---|---|---|
PDW | 1.68 (1.37-2.07) | e0.001s | ||
MPV | 4.27 (1.72-10.58) | e0.002s | 6.20 (1.09-35.1) | f0.039s |
Histological grade | 1.0 | e0.001s | ||
Age | 1.5 (1.15-2.08) | e0.004s |
Cutoff value | Sensitivity | Specificity | PPV | NPV | Accuracy | Youden index (j=sen+spe-1) | |
|---|---|---|---|---|---|---|---|
MPV | 10.50 | 0.580 | 0.721 | 0.42 | 0.78 | 0.57 | 0.230 |
PDW | 13.50 | 0.443 | 0.967 | 0.46 | 0.96 | 0.61 | 0.410 |
RDW | 49.50 | 0.172 | 0.902 | 0.389 | 0.725 | 0.233 | 0.074 |
BSMMU | Bangabandhu Sheikh Mujib Medical University |
| [1] | Amant F, Moerman P, Neven P, Timmerman D, Limbergen V, Vergote E. Endometrial cancer. Lancet. 2005; 366: 491-505. |
| [2] | Burke WM, Orr J, Leitao M, et al. Endometrial cancer: a review and current management strategies: part II. Gynecol Oncol. 2014; 134: 393-402. |
| [3] | Cakal B, Akoz AG, Ustundag Y, Yalinkilic M, Ulker A, Ankarali H. Red cell distribution width for assessment of activity of inflammatory bowel disease. Dig Dis Sci. 2009; 54: 842-7. |
| [4] | Clarke K, Sagunarthy R, Kansal S. RDW as an additional marker in inflammatory bowel disease/undifferentiated colitis. Dig Dis Sci. 2008; 53: 2521-3. |
| [5] | Candido J, Hagemann T. Cancer related inflammation. J Clin Immunol. 2013; 33: 79-84. |
| [6] | De Gonzalo-Calvo D, De Luxan-Delgado B, Rodriguez-Gonzalez S, Garcia-Macia M, Suarez FM, Solano JJ, et al. Interleukin 6, soluble tumor necrosis factor receptor I and red blood cell distribution width as biological markers of functional dependence in an elderly population: a translational approach. Cytokine. 2012; 58: 193-8. |
| [7] | Duffy TP, Kelley WN, Dupont HL, Glick JH, Harris ED, Hathaway DR, et al. Approach to the patient with anemia. In: Kelley’s textbook of internal medicine. Philadelphia, PA: Lippincott Williams and Wilkins; 1997. p. 1295-9. |
| [8] | Forhecz Z, Gombos T, Borgulya G, Pozsonyi Z, Prohaszka Z, Janoskuti L. Red cell distribution width in heart failure: prediction of clinical events and relationship with markers of ineffective erythropoiesis, inflammation, renal function, and nutritional state. Am Heart J. 2009; 158: 659-66. |
| [9] | Günay E, Sarınç Ulaşlı S, Akar O, Ahsen A, Günay S, Koyuncu T. Neutrophil-to-lymphocyte ratio in chronic obstructive pulmonary disease: a retrospective study. Inflammation. 2014; 37: 374-80. |
| [10] | Gao J, Yang G, Wen W, et al. Impact of known risk factors on endometrial cancer burden in Chinese women. Eur J Cancer Prev. 2016; 25: 329-34. |
| [11] | Heng DY, Xie W, Regan MM, Warren MA, Golshayan AR, Sahi C, et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: results from a large multicenter study. J Clin Oncol. 2009; 27: 5794-9. |
| [12] | Iwasaki A, Hamanaka W, Harnada T, Maekawa S, Enatsu S, Shirakusa T. Significance of platelet counts in patients who underwent surgical treatment for lung metastasis. Int Surg. 2007; 92: 103-9. |
| [13] | Kim DK, Oh SY, Kwon HC, Lee S, Kwon KA, Kim BG, et al. Clinical significances of preoperative serum interleukin-6 and C-reactive protein level in operable gastric cancer. BMC Cancer. 2009; 9: 155. |
| [14] | Kemal Y, Demirag G, Bas B, et al. The value of red blood cell distribution width in endometrial cancer. Clin Chem Lab Med. 2015; 53: 823-7. |
| [15] | Lippi G, Plebani M. Red blood cell distribution width (RDW) and human pathology: one size fits all. Clin Chem Lab Med. 2014; 52: 1247-9. |
| [16] | Urick ME, Bell DW. Clinical actionability of molecular targets in endometrial cancer. Nat Rev Cancer. 2019; 19(9): 510-21. |
| [17] | McMillan DC. Systemic inflammation, nutritional status, and survival in patients with cancer. Curr Opin Clin Nutr Metab Care. 2009; 12: 223-6. |
| [18] | Sica A, Allavena P, Mantovani A. Cancer related inflammation: the macrophage connection. Cancer Lett. 2008; 267: 204-15. |
| [19] | Nadar S, Blann A, Lip G. Platelet morphology and plasma indices of platelet activation in essential hypertension: effects of amlodipine-based antihypertensive therapy. Ann Med. 2004; 36: 552-7. |
| [20] | Rhodes CJ, Howard LS, Busbridge M, Ashby D, Kondili E, Gibbs JS, et al. Iron deficiency and raised hepcidin in idiopathic pulmonary arterial hypertension: clinical prevalence, outcomes, and mechanistic insights. J Am Coll Cardiol. 2011; 58: 300-9. |
| [21] | Suzuki K, Aiura K, Kitagou M, Hoshimoto S, Takahashi S, Ueda M, et al. Platelet counts closely correlate with the disease-free survival interval of pancreatic cancer patients. Hepatogastroenterology. 2004; 51: 847-53. |
| [22] | Yayla Abide C, Bostanci Ergen E, Cogendez E, Kilicci C, Uzun F, Ozkaya E, et al. Evaluation of complete blood count parameters to predict endometrial cancer. J Clin Lab Anal. 2018; 32(6): e22438. |
| [23] | Song C, Cao J, Zhang F, Wang C, Guo Z, Lin Y, et al. Nutritional risk assessment by scored patient-generated subjective global assessment associated with demographic characteristics in 23,904 common malignant tumors patients. Nutr Cancer. 2019; 71(1): 50-60. |
| [24] | Oge T, Yalcin O, Ozalp SS, Isikci T. Platelet volume as a parameter for platelet activation in patients with endometrial cancer. J Obstet Gynaecol. 2013; 33(3): 301-4. |
| [25] | Gao L, Nie X, Zhang W, Gou R, Hu Y, Qi Y, et al. Identification of long noncoding RNA RP11-89K21.1 and RP11-357H14.17 as prognostic signatures of endometrial carcinoma via integrated bioinformatics analysis. Cancer Cell Int. 2020; 20: 1-8. |
| [26] | Kurtoglu E, Kokcu A, Celik H, Sari S, Tosun M. Platelet indices may be useful in discrimination of benign and malignant endometrial lesions and early and advanced stage endometrial cancer. Asian Pac J Cancer Prev. 2015; 16(13): 5397-400. |
| [27] | Zhang L, Yu CH, Guo KP, Huang CZ, Mo LY. Prognostic role of red blood cell distribution width in patients with sepsis: a systematic review and meta-analysis. BMC Immunol. 2020; 21: 1-8. |
| [28] | Karateke A, Kaplanoglu M, Baloglu A. Relations of platelet indices with endometrial hyperplasia and endometrial cancer. Asian Pac J Cancer Prev. 2015; 16(12): 4905-8. |
| [29] | Shen WJ, Fu S, Li N, Li LL, Cao ZG, Li C, et al. Decreased mean platelet volume is associated with cervical cancer development. Asian Pac J Cancer Prev. 2017; 18(7): 1769-72. |
| [30] | Chen H, Wu Q, Zhang Y, Li Q, Ma J, Kong F, et al. Nomograms based on the novel platelet index score predict postoperative prognosis in endometrial cancer. Gynecol Oncol. 2020; 158(3): 689-97. |
| [31] | Petric AN, Živadinović R, Mitić D, Stanojević M, Živadinović A, Kostić I. Hematological and biochemical markers in determining the diagnosis and stage prediction of endometrial cancer. Ginekol Pol. 2023; 94(4): 283-90. |
| [32] | Ji M, Lu Y, Guo L, Feng F, Wan X, Xiang Y. Endometrial carcinoma with yolk sac tumor-like differentiation and elevated serum β-hCG: a case report and literature review. Onco Targets Ther. 2013; 1515-22. |
APA Style
Islam, J., Begum, S. A., Amatullah, M., Mahmud, T., Akter, L., et al. (2025). Pretreatment Platelet Indices and Red Cell Distribution Width as a Predictor of Endometrial Carcinoma Among Patients with Abnormal Uterine Bleeding. Journal of Cancer Treatment and Research, 13(1), 1-9. https://doi.org/10.11648/j.jctr.20251301.11
ACS Style
Islam, J.; Begum, S. A.; Amatullah, M.; Mahmud, T.; Akter, L., et al. Pretreatment Platelet Indices and Red Cell Distribution Width as a Predictor of Endometrial Carcinoma Among Patients with Abnormal Uterine Bleeding. J. Cancer Treat. Res. 2025, 13(1), 1-9. doi: 10.11648/j.jctr.20251301.11
AMA Style
Islam J, Begum SA, Amatullah M, Mahmud T, Akter L, et al. Pretreatment Platelet Indices and Red Cell Distribution Width as a Predictor of Endometrial Carcinoma Among Patients with Abnormal Uterine Bleeding. J Cancer Treat Res. 2025;13(1):1-9. doi: 10.11648/j.jctr.20251301.11
@article{10.11648/j.jctr.20251301.11,
author = {Jannatul Islam and Shirin Akter Begum and Mehriban Amatullah and Tasfia Mahmud and Latifa Akter and Afroza Khanom and Naznin Akter Zahan and Nasrin Akter},
title = {Pretreatment Platelet Indices and Red Cell Distribution Width as a Predictor of Endometrial Carcinoma Among Patients with Abnormal Uterine Bleeding
},
journal = {Journal of Cancer Treatment and Research},
volume = {13},
number = {1},
pages = {1-9},
doi = {10.11648/j.jctr.20251301.11},
url = {https://doi.org/10.11648/j.jctr.20251301.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jctr.20251301.11},
abstract = {Introduction: Endometrial carcinoma is the sixth most common cancer for females in the world and the seventh most common gynecological cancer in developing countries. The values of platelet indices (MPV, PDW) and red cell distribution width (RDW) are associated with different stages of endometrial and cervical carcinoma. Thus, this study aimed to determine the relation of MPV, PDW, and RDW with endometrial carcinoma. Methods: This cross-sectional study was conducted in the Department of Gynecological Oncology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh from July 2022 to July 2023. This study included 61 women with histopathologically confirmed endometrial carcinoma (FIGO stage I to IV) as cases and 122 women with histopathologically confirmed benign endometrial disease as the control group. Result: This study found that the case group had a higher mean age (55.62 years vs. 43.75 years). Blood parameter findings showed higher mean MPV (10.46 vs. 9.96) and RDW (46.64 vs. 43.05) in cases. PDW mean was lower in cases (11.33 vs. 14.39). MPV correlated positively with the FIGO stage and histological type, while PDW had a negative correlation. ROC analysis of MPV yielded an AUC of 0.645, with a cut-off of 10.50 showing sensitivity 58%, specificity 72%, and accuracy 57%. ROC analysis of PDW yielded an AUC of 0.789, with a cut-off of 13.50 showing sensitivity 44%, specificity 97%, and accuracy 61%. Multivariant regression revealed MPV to be the strongest factor of endometrial carcinoma (OR-6.20, p=0.039). Conclusion: This study showed that the mean platelet volume (MPV) and red cell distribution width (RDW) are potential markers for detecting endometrial carcinoma.
},
year = {2025}
}
TY - JOUR T1 - Pretreatment Platelet Indices and Red Cell Distribution Width as a Predictor of Endometrial Carcinoma Among Patients with Abnormal Uterine Bleeding AU - Jannatul Islam AU - Shirin Akter Begum AU - Mehriban Amatullah AU - Tasfia Mahmud AU - Latifa Akter AU - Afroza Khanom AU - Naznin Akter Zahan AU - Nasrin Akter Y1 - 2025/01/21 PY - 2025 N1 - https://doi.org/10.11648/j.jctr.20251301.11 DO - 10.11648/j.jctr.20251301.11 T2 - Journal of Cancer Treatment and Research JF - Journal of Cancer Treatment and Research JO - Journal of Cancer Treatment and Research SP - 1 EP - 9 PB - Science Publishing Group SN - 2376-7790 UR - https://doi.org/10.11648/j.jctr.20251301.11 AB - Introduction: Endometrial carcinoma is the sixth most common cancer for females in the world and the seventh most common gynecological cancer in developing countries. The values of platelet indices (MPV, PDW) and red cell distribution width (RDW) are associated with different stages of endometrial and cervical carcinoma. Thus, this study aimed to determine the relation of MPV, PDW, and RDW with endometrial carcinoma. Methods: This cross-sectional study was conducted in the Department of Gynecological Oncology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh from July 2022 to July 2023. This study included 61 women with histopathologically confirmed endometrial carcinoma (FIGO stage I to IV) as cases and 122 women with histopathologically confirmed benign endometrial disease as the control group. Result: This study found that the case group had a higher mean age (55.62 years vs. 43.75 years). Blood parameter findings showed higher mean MPV (10.46 vs. 9.96) and RDW (46.64 vs. 43.05) in cases. PDW mean was lower in cases (11.33 vs. 14.39). MPV correlated positively with the FIGO stage and histological type, while PDW had a negative correlation. ROC analysis of MPV yielded an AUC of 0.645, with a cut-off of 10.50 showing sensitivity 58%, specificity 72%, and accuracy 57%. ROC analysis of PDW yielded an AUC of 0.789, with a cut-off of 13.50 showing sensitivity 44%, specificity 97%, and accuracy 61%. Multivariant regression revealed MPV to be the strongest factor of endometrial carcinoma (OR-6.20, p=0.039). Conclusion: This study showed that the mean platelet volume (MPV) and red cell distribution width (RDW) are potential markers for detecting endometrial carcinoma. VL - 13 IS - 1 ER -
Department of Obstetrics and Gynecology, Upazila Health Complex, Daudcandi, Cumilla, Bangladesh
Department of Gynecological Oncology, Bangabandhu Sheikh Mujib Medical University, Shahbag, Dhaka, Bangladesh
Department of Obstetrics and Gynecology, Bangabandhu Sheikh Mujib Medical University, Shahbag, Dhaka, Bangladesh
Department of Pharmacology, Dr. Sirajul Islam Medical College, Dhaka, Bangladesh
Department of Gynecological Oncology, Bangabandhu Sheikh Mujib Medical University, Shahbag, Dhaka, Bangladesh
Department of Gynecological Oncology, National Institute of Cancer Research & Hospital, Dhaka, Bangladesh
OSD, Directorate General of Health Services, Dhaka, Bangladesh
OSD, Directorate General of Health Services, Dhaka, Bangladesh
Information