Despite being associated with tropical regions of the world, parasitic infestations of the central nervous system have rapidly evolved over the years to involve previously non-endemic countries. This has been aided by transmigration of populations and ecological drifts, thereby creating health problems of immense socioeconomic implications. Pathophysiologic processes that accompany these infections involve the elaboration of leucocytes, macrophages and inflammatory cytokines leading to the denudation of the blood brain barrier with consequent vasogenic edema with increased intracranial pressure, These infestations manifest with various symptoms of neurologic importance which may include headaches, altered sensorium, and progressive neurologic deficits attributable to the mass effect of tissue necrosis caused by neuroinflammatory reaction to the presence of the parasites. This article attempts to survey the predisposing factors, clinical outcomes and complications of these infestations, while exploring the complex interplay between the clinical presentation, diagnostic modalities and interactions between humans and their environment which aid the proliferation of these parasites. It is imperative to highlight the importance of optimal clinical scrutiny and judgment in diagnosing these conditions while advocating for public health intervention strategies and collaborative research efforts to ameliorate the potential complications of these infestations which exert an extreme impact in the prognosis of affected patients with attendant neurologic sequelae.
| Published in | International Journal of Neurosurgery (Volume 9, Issue 1) |
| DOI | 10.11648/j.ijn.20250901.15 |
| Page(s) | 30-49 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Parasitic Infestation, Neuroinflammation, Clinical Presentation
TNF | Tumor Necrosis Factor |
CNS | Central Nervous System |
FLAIR | Fluid-Attenuated Inversion Recovery |
ELISA | Enzyme Linked Immunosorbent Assay |
AIDS | Acquired Immune Deficiency Syndrome |
HTLV-1 | Human T-Lymphotropic Virus Type 1 |
MRI | Magnetic Resonance Image |
| [1] |
Abdel Razek AA, Watcharakorn A, Castillo M. Parasitic diseases of the central nervous system. Neuroimaging Clin N Am. 2011 Nov; 21(4): 815-41, viii.
https://doi.org/10.1016/j.nic.2011.07.005 Epub 2011 Sep 3. |
| [2] | Idro R, Ogwang R, Barragan A, Raimondo JV, Masocha W. Neuroimmunology of Common Parasitic Infections in Africa. Front Immunol. 2022 Feb 10; 13: 791488. |
| [3] | Winkler AS. Neurocysticercosis in sub-Saharan Africa: a review of prevalence, clinical characteristics, diagnosis, and management. Pathog Glob Health. 2012 Sep; 106(5): 261-74. |
| [4] | Ndimubanzi PC, Carabin H, Budke CM, et al. A systematic review of the frequency of neurocyticercosis with a focus on people with epilepsy. PLoS Negl Trop Dis 2010; 4(11): e870. |
| [5] | Center for Disease Control. DPDx Laboratory Identifiation of Parasites of Public Health Concern. Taeniasis: |
| [6] | Coyle CM. Neurocysticercosis: an update. Curr Infect Dis Rep. 2014 Nov; 16(11): 437. |
| [7] | Montano SM, Villaran MV, Ylquimiche L, et al. Neurocysticercosis: association between seizures, serology, and brain CT in rural Peru. Neurol. 2005; 65: 229-33. |
| [8] | Fleury A, Carrillo-Mezo R, Flisser A, Sciutto E, Corona T. Subarachnoid basal neurocysticercosis: a focus on the most severe form of the disease. Expert Rev Anti-Infect Ther. 2011; 9: 123-33. |
| [9] | Cuetter AC, Andrews RJ. Intraventricular neurocysticercosis: 18 consecutive patients and review of the literature. Neurosurg Focus. 2002; 12: e5. |
| [10] | Alsina GA, Johnson JP, McBride DQ, Rhoten PR, Mehringer CM, Stokes JK. Spinal neurocysticercosis. Neurosurg Focus. 2002; 12: e8. |
| [11] | Del Brutto OH. Neurocysticercosis. Handb Clin Neurol. 2014; 121: 1445-59. |
| [12] | Del Brutto OH. Human Neurocysticercosis: An Overview. Pathogens. 2022 Oct 20; 11(10): 1212. |
| [13] | Siyadatpanah A, Brunetti E, Emami Zeydi A, Moghadam YD, Agudelo Higuita NI. Cerebral Cystic Echinococcosis. Case Rep Infect Dis. 2020 Feb 29; 2020: 1754231. |
| [14] | El Saqui A, Aggouri M, Benzagmout M, Chakour K, El Faiz Chaoui M. Cerebral hydatid cysts in children: about 15 cases. Pan Afr Med J. 2017 Apr 13; 26: 205. French. |
| [15] | Karshima, S. N., Ahmed, M. I., Adamu, N. B. et al. Africa-wide meta-analysis on the prevalence and distribution of human cystic echinococcosis and canine Echinococcus granulosus infections. Parasites Vectors 15, 357 (2022). |
| [16] | Center for Disease Control. DPDx Laboratory Identifiation of Parasites of Public Health Concern. Echinococcosis : |
| [17] |
Demir MK, Yapıcıer Ö, Jameel MA, Bozbuğa M. Cerebral hydatid disease with serpent sign, calcifications, and peripheral enhancement. Acta Neurol Belg. 2020 Oct; 120(5): 1173-1175.
https://doi.org/10.1007/s13760-019-01104-8 Epub 2019 Feb 28. |
| [18] | Carod Artal, F. J. Cerebral and spinal schistosomiasis. Curr. Neurol. Neurosci. Rep. 2012, 12, 666-674. |
| [19] | John, C. C.; Carabin, H.; Montano, S. M.; Bangirana, P.; Zunt, J. R.; Peterson, P. K. Global research priorities for infections that affect the nervous system. Nature 2015, 527, S178-S186. |
| [20] | Center for Disease Control. DPDx Laboratory Identifiation of Parasites of Public Health Concern. Schistosomiasis. |
| [21] | Tunali V, Korkmaz M. Emerging and Re-Emerging Parasitic Infections of the Central Nervous System (CNS) in Europe. Infect Dis Rep. 2023 Oct 25; 15(6): 679-699. |
| [22] | Liu H, Lim CC, Feng X, Yao Z, Chen Y, Sun H, Chen X. MRI in cerebral schistosomiasis: characteristic nodular enhancement in 33 patients. AJR Am J Roentgenol. 2008 Aug; 191(2): 582-8. |
| [23] | Ma, G.; Holland, C. V.; Wang, T.; Hofmann, A.; Fan, C. K.; Maizels, R. M.; Hotez, P. J.; Gasser, R. B. Human toxocariasis. Lancet Infect. Dis. 2018, 18, e14-e24. |
| [24] | Ajayi OO, Duhlinska DD, Agwale SM, Njoku M. Frequency of human toxocariasis in Jos, Plateau State, Nigeria. Mem Inst Oswaldo Cruz. 2000 Mar-Apr; 95(2): 147-9. |
| [25] | Center for Disease Control. DPDx Laboratory Identifiation of Parasites of Public Health Concern. Toxocariasis. |
| [26] | Xinou E, Lefkopoulos A, Gelagoti M, Drevelegas A, Diakou A, Milonas I, Dimitriadis AS. CT and MR imaging findings in cerebral toxocaral disease. AJNR Am J Neuroradiol. 2003 Apr; 24(4): 714-8. |
| [27] | Duprez TP, Bigaignon G, Delgrange E, Desfontaines P, Hermans M, Vervoort T, Sindic CJ, Buysschaert M. MRI of cervical cord lesions and their resolution in Toxocara canis myelopathy. Neuroradiology. 1996 Nov; 38(8): 792-5. |
| [28] |
Dietrich CF, Cretu C, Dong Y. Imaging of toxocariasis. Adv Parasitol. 2020; 109: 165-187.
https://doi.org/10.1016/bs.apar.2020.03.001 Epub 2020 Apr 25. |
| [29] | Centers for Disease Control and Prevention, 2014. Parasites—Strongyloides. Available at: |
| [30] | Lynn MK, Morrissey JA, Conserve DF. Soil-Transmitted Helminths in the USA: a Review of Five Common Parasites and Future Directions for Avenues of Enhanced Epidemiologic Inquiry. Curr Trop Med Rep. 2021; 8(1): 32-42. |
| [31] | Eslahi AV, Badri M, Nahavandi KH, Houshmand E, Dalvand S, Riahi SM, Johkool MG, Asadi N, Hoseini Ahangari SA, Taghipour A, Zibaei M, Khademvatan S. Prevalence of strongyloidiasis in the general population of the world: a systematic review and meta-analysi. |
| [32] | Woll F, Gotuzzo E, Montes M. Strongyloides stercoralis infection complicating the central nervous system. Handb Clin Neurol. 2013; 114: 229-34. |
| [33] | Montes M, Sanchez C, Verdonck K, Lake JE, Gonzalez E, Lopez G, Terashima A, Nolan T, Lewis DE, Gotuzzo E, White AC Jr. Regulatory T cell expansion in HTLV-1 and strongyloidiasis co-infection is associated with reduced IL-5 responses to Strongyloides sterc. |
| [34] | Center for Disease Control. DPDx Laboratory Identifiation of Parasites of Public Health Concern. Strongyloides strcolaris. |
| [35] | Jain AK, Agarwal SK, el-Sadr W. Streptococcus bovis bacteremia and meningitis associated with Strongyloides stercoralis colitis in a patient infected with human immunodeficiency virus. Clin Infect Dis. 1994 Feb; 18(2): 253-4. |
| [36] | Oktar N, Ozer HM, Demirtas E. Central Nervous System Strongyloides Stercoralis. A Case Report. Turk Neurosurg. 2020; 30(5): 776-779. |
| [37] | Keiser PB, Nutman TB. Strongyloides stercoralis in the Immunocompromised Population. Clin Microbiol Rev. 2004 Jan; 17(1): 208-17. |
| [38] | Datry A, Hilmarsdottir I, Mayorga-Sagastume R, Lyagoubi M, Gaxotte P, Biligui S, Chodakewitz J, Neu D, Danis M, Gentilini M. Treatment of Strongyloides stercoralis infection with ivermectin compared with albendazole: results of an open study of 60 cases. |
| [39] | Center for Disease Control. DPDx Laboratory Identifiation of Parasites of Public Health Concern. Trichinellosis. |
| [40] | Bruschi F, Brunetti E, Pozio E. Neurotrichinellosis. Handb Clin Neurol. 2013; 114: 243-9. |
| [41] | Rosca EC, Tudor R, Cornea A, Simu M. Central Nervous System Involvement in Trichinellosis: A Systematic Review. Diagnostics (Basel). 2021 May 25; 11(6): 945. |
| [42] |
Neghina R, Iacobiciu I, Neghina AM, Marincu I. Trichinellosis, another helminthiasis affecting the central nervous system. Parasitol Int. 2011 Jun; 60(2): 230.
https://doi.org/10.1016/j.parint.2011.01.007 Epub 2011 Feb 1. |
| [43] | Dupouy-Camet, Jean & Bruschi, Fabrizio. Management and diagnosis of human trichinellosis. FAO/WHO/OIE Guidelines for the Surveillance, Management, Prevention and Control of Trichinellosis. 2017 : 37-68. |
| [44] |
Shrivastava A, Arora P, Khare A, Goel G, Kapoor N. Central nervous system filariasis masquerading as a glioma: case report. J Neurosurg. 2017 Sep; 127(3): 691-693.
https://doi.org/10.3171/2016.9.JNS161092 Epub 2016 Dec 23. |
| [45] | Nyagang SM, Cumber SN, Cho JF, Keka EI, Nkfusai CN, Wepngong E, Tsoka-Gwegweni JM, Fokam EB. Prevalence of onchocerciasis, attitudes and practices and the treatment coverage after 15 years of mass drug administration with ivermectin in the Tombel Health D. |
| [46] | Center for Disease Control. DPDx Laboratory Identifiation of Parasites of Public Health Concern. Filariasis. |
| [47] | Pittella JE. Pathology of CNS parasitic infections. Handb Clin Neurol. 2013; 114: 65-88. |
| [48] | Arndts K, Kegele J, Massarani AS, Ritter M, Wagner T, Pfarr K, Lämmer C, Dörmann P, Peisker H, Menche D, Al-Bahra M, Prazeres da Costa C, Schmutzhard E, Matuja W, Hoerauf A, Layland-Heni LE, Winkler AS. Epilepsy and nodding syndrome in association with an. |
| [49] |
Finsterer J, Auer H. Parasitoses of the human central nervous system. J Helminthol. 2013 Sep; 87(3): 257-70.
https://doi.org/10.1017/S0022149X12000600 Epub 2012 Oct 10. |
| [50] | Klaren VN, Kijlstra A. Toxoplasmosis, an overview with emphasis on ocular involvement. Ocul Immunol Inflamm. 2002; 10: 1-26. |
| [51] | Kamani J, Mani AU, Egwu GO, Kumshe HA. Seroprevalence of human infection with Toxoplasma gondii and the associated risk factors, in Maiduguri, Borno state, Nigeria. Ann Trop Med Parasitol. 2009; 103: 317-21. |
| [52] | Swai ES, Schoonman L. Seroprevalence of Toxoplasma gondii infection amongst residents of Tanga district in north-east Tanzania. Tanzan J Health Res. 2009; 11: 205-9. |
| [53] | Xiao Y, Yin J, Jiang N, Xiang M, Hao L, Lu H, et al. Seroepidemiology of human Toxoplasma gondii infection in China. BMC Infect Dis. 2010; 10: 4. |
| [54] | Ohiolei JA, Isaac C. Toxoplasmosis in Nigeria: the story so far (1950-2016): a review. Folia Parasitol (Praha). 2016 Aug 22; 63: 2016.030. |
| [55] | Center for Disease Control. DPDx Laboratory Identifiation of Parasites of Public Health Concern.Toxoplasmosis. |
| [56] | Furtado JM, Smith JR, Belfort R Jr, Gattey D, Winthrop KL. Toxoplasmosis: a global threat. J Glob Infect Dis. 2011 Jul; 3(3): 281-4. |
| [57] | Batra A, Tripathi RP, Gorthi SP. Magnetic resonance evaluation of cerebral toxoplasmosis in patients with the acquired immunodeficiency syndrome. Acta Radiol. 2004 Apr; 45(2): 212-21. |
| [58] | Thurnher MM, Donovan Post MJ. Neuroimaging in the brain in HIV-1-infected patients. Neuroimaging Clin N Am. 2008 Feb; 18(1): 93-117; viii. |
| [59] | Chang L, Cornford ME, Chiang FL, Ernst TM, Sun NC, Miller BL. Radiologic-pathologic correlation. Cerebral toxoplasmosis and lymphoma in AIDS. AJNR Am J Neuroradiol. 1995 Sep; 16(8): 1653-63. |
| [60] | Montoya JG. Laboratory diagnosis of Toxoplasma gondii infection and toxoplasmosis. J Infect Dis. 2002; 185: S73-82. |
| [61] | Lopez A, Dietz VJ, Wilson M, Navin TR, Jones JL. Preventing congenital toxoplasmosis. MMWR Recomm Rep. 2000; 49: 59-68. |
| [62] | Luft BJ, Chua A. Central nervous system toxoplasmosis in HIV pathogenesis, diagnosis, and therapy. Curr Infect Dis Re. 2000; 2: 358-62. |
| [63] | Oyerinde JP, Alonge AA, Adegbite-Hollist AF, Ogunbi O. The epidemiology of Entamoeba histolytica in a Nigerian urban population. Int J Epidemiol. 1979 Mar; 8(1): 55-9. |
| [64] | Umeche N. The incidence of amoebiasis among secondary school students in Calabar, Nigeria. Folia Parasitol (Praha). 1983; 30(3): 277-80. |
| [65] | Singh P, Kochhar R, Vashishta RK, Khandelwal N, Prabhakar S, Mohindra S, Singhi P. Amebic meningoencephalitis: spectrum of imaging findings. AJNR Am J Neuroradiol. 2006 Jun-Jul; 27(6): 1217-21. |
| [66] | Center for Disease Control. DPDx Laboratory Identifiation of Parasites of Public Health Concern.Amebiasis. |
| [67] | Orbison JA, Reeves N, Leedham CL, Blumberg JM. Amebic brain abscess; review of the literature and report of five additional cases. Medicine (Baltimore). 1951 Sep; 30(3): 247-82. |
| [68] | Morán P, Serrano-Vázquez A, Rojas-Velázquez L, González E, Pérez-Juárez H, Hernández EG, Padilla MLA, Zaragoza ME, Portillo-Bobadilla T, Ramiro M, Ximénez C. Amoebiasis: Advances in Diagnosis, Treatment, Immunology Features and the Interaction with the In. |
| [69] | Haque R, Huston CD, Hughes M, Houpt E, Petri WA Jr. Amebiasis. N Engl J Med. 2003 Apr 17; 348(16): 1565-73. |
| [70] | Schiess N, Villabona-Rueda A, Cottier KE, Huether K, Chipeta J, Stins MF. Pathophysiology and neurologic sequelae of cerebral malaria. Malar J. 2020 Jul 23; 19(1): 266. |
| [71] |
Orimadegun AE, Fawole O, Okereke JO, Akinbami FO, Sodeinde O. Increasing burden of childhood severe malaria in a Nigerian tertiary hospital: implication for control. J Trop Pediatr. 2007 Jun; 53(3): 185-9.
https://doi.org/10.1093/tropej/fmm002 Epub 2007 Feb 7 |
| [72] | Elesha SO, Adepoju FB, Banjo AA. Rising incidence of cerebral malaria in Lagos, Nigeria: a postmoterm study. East Afr Med J. 1993 May; 70(5): 302-6. |
| [73] | Hunt NH, Grau GE. Cytokines: accelerators and brakes in the pathogenesis of cerebral malaria. Trends Immunol. 2003 Sep; 24(9): 491-9. |
| [74] | Dondorp AM, Ince C, Charunwatthana P, Hanson J, van Kuijen A, Faiz MA, Rahman MR, Hasan M, Bin Yunus E, Ghose A, Ruangveerayut R, Limmathurotsakul D, Mathura K, White NJ, Day NP. Direct in vivo assessment of microcirculatory dysfunction in severe falcipar. |
| [75] | Center for Disease Control. DPDx Laboratory Identifiation of Parasites of Public Health Concern.Plasmodiasis. |
| [76] |
Nickerson JP, Tong KA, Raghavan R. Imaging cerebral malaria with a susceptibility-weighted MR sequence. AJNR Am J Neuroradiol. 2009 Jun; 30(6): e85-6.
https://doi.org/10.3174/ajnr.A1568 Epub 2009 Mar 25. |
| [77] | Nguyen TH, Day NP, Ly VC, Waller D, Mai NT, Bethell DB, Tran TH, White NJ. Post-malaria neurological syndrome. Lancet. 1996 Oct 5; 348(9032): 917-21. |
| [78] | Tamzali Y, Demeret S, Haddad E, Guillot H, Caumes E, Jauréguiberry S. Post-malaria neurological syndrome: four cases, review of the literature and clarification of the nosological framework. Malar J. 2018 Oct 26; 17(1): 387. |
| [79] |
World Health Organisation Newsroom fact sheets. Trypanosomiasis.
https://www.who.int/news-room/fact-sheets/detail/chagas-disease-(american-trypanosomiasis) |
| [80] | Center for Disease Control. DPDx Laboratory Identifiation of Parasites of Public Health Concern. African trypanosomiasis. |
| [81] | Lucas S, Bell J, Chimelli L (2008). Parasitic and fungal infections. In: S Love, DN Louis, DW Ellison (Eds.), Greenfield’s Neuropathology. Hodder Arnold, London, pp. 1447-1487. |
| [82] |
Pittella JE. Central nervous system involvement in Chagas disease: a hundred-year-old history. Trans R Soc Trop Med Hyg. 2009 Oct; 103(10): 973-8.
https://doi.org/10.1016/j.trstmh.2009.04.012 Epub 2009 May 19. |
| [83] | Carod-Artal FJ, Gascon J. Chagas disease and stroke. Lancet Neurol. 2010 May; 9(5): 533-42. |
| [84] | Braakman HM, van de Molengraft FJ, Hubert WW, Boerman DH. Lethal African trypanosomiasis in a traveler: MRI and neuropathology. Neurology. 2006 Apr 11; 66(7): 1094-6. |
| [85] | Gill D, Chatha D, Carpio-O’Donovan R. MR imaging findings in African trypansomiasis. AJNR Am J Neuroradiol 2003; 24: 1 383-5. |
| [86] | Chacko G. Parasitic diseases of the central nervous system. Semin Diagn Pathol. 2010 Aug; 27(3): 167-85. |
| [87] |
Kenfak A, Eperon G, Schibler M, Lamoth F, Vargas MI, Stahl JP. Diagnostic approach to encephalitis and meningoencephalitis in adult returning travellers. Clin Microbiol Infect. 2019 Apr; 25(4): 415-421.
https://doi.org/10.1016/j.cmi.2019.01.008 Epub 2019 Jan 29. |
| [88] |
Carpio A, Romo ML, Parkhouse RM, Short B, Dua T. Parasitic diseases of the central nervous system: lessons for clinicians and policy makers. Expert Rev Neurother. 2016; 16(4): 401-14.
https://doi.org/10.1586/14737175.2016.1155454 Epub 2016 Mar 4. |
| [89] |
Semenza JC, Paz S. Climate change and infectious disease in Europe: Impact, projection and adaptation. Lancet Reg Health Eur. 2021 Oct; 9: 100230.
https://doi.org/10.1016/j.lanepe.2021.100230 Epub 2021 Oct 7. |
APA Style
Azode, K. M., Ewoye, E. E., Okongwu, C. C. (2025). Parasitic Infestations of the Central Nervous System - A Review Article. International Journal of Neurosurgery, 9(1), 30-49. https://doi.org/10.11648/j.ijn.20250901.15
ACS Style
Azode, K. M.; Ewoye, E. E.; Okongwu, C. C. Parasitic Infestations of the Central Nervous System - A Review Article. Int. J. Neurosurg. 2025, 9(1), 30-49. doi: 10.11648/j.ijn.20250901.15
@article{10.11648/j.ijn.20250901.15,
author = {Kelechi Michael Azode and Ese Enaorho Ewoye and Chigozie Chidozie Okongwu},
title = {Parasitic Infestations of the Central Nervous System - A Review Article
},
journal = {International Journal of Neurosurgery},
volume = {9},
number = {1},
pages = {30-49},
doi = {10.11648/j.ijn.20250901.15},
url = {https://doi.org/10.11648/j.ijn.20250901.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijn.20250901.15},
abstract = {Despite being associated with tropical regions of the world, parasitic infestations of the central nervous system have rapidly evolved over the years to involve previously non-endemic countries. This has been aided by transmigration of populations and ecological drifts, thereby creating health problems of immense socioeconomic implications. Pathophysiologic processes that accompany these infections involve the elaboration of leucocytes, macrophages and inflammatory cytokines leading to the denudation of the blood brain barrier with consequent vasogenic edema with increased intracranial pressure, These infestations manifest with various symptoms of neurologic importance which may include headaches, altered sensorium, and progressive neurologic deficits attributable to the mass effect of tissue necrosis caused by neuroinflammatory reaction to the presence of the parasites. This article attempts to survey the predisposing factors, clinical outcomes and complications of these infestations, while exploring the complex interplay between the clinical presentation, diagnostic modalities and interactions between humans and their environment which aid the proliferation of these parasites. It is imperative to highlight the importance of optimal clinical scrutiny and judgment in diagnosing these conditions while advocating for public health intervention strategies and collaborative research efforts to ameliorate the potential complications of these infestations which exert an extreme impact in the prognosis of affected patients with attendant neurologic sequelae.
},
year = {2025}
}
TY - JOUR T1 - Parasitic Infestations of the Central Nervous System - A Review Article AU - Kelechi Michael Azode AU - Ese Enaorho Ewoye AU - Chigozie Chidozie Okongwu Y1 - 2025/04/19 PY - 2025 N1 - https://doi.org/10.11648/j.ijn.20250901.15 DO - 10.11648/j.ijn.20250901.15 T2 - International Journal of Neurosurgery JF - International Journal of Neurosurgery JO - International Journal of Neurosurgery SP - 30 EP - 49 PB - Science Publishing Group SN - 2640-1959 UR - https://doi.org/10.11648/j.ijn.20250901.15 AB - Despite being associated with tropical regions of the world, parasitic infestations of the central nervous system have rapidly evolved over the years to involve previously non-endemic countries. This has been aided by transmigration of populations and ecological drifts, thereby creating health problems of immense socioeconomic implications. Pathophysiologic processes that accompany these infections involve the elaboration of leucocytes, macrophages and inflammatory cytokines leading to the denudation of the blood brain barrier with consequent vasogenic edema with increased intracranial pressure, These infestations manifest with various symptoms of neurologic importance which may include headaches, altered sensorium, and progressive neurologic deficits attributable to the mass effect of tissue necrosis caused by neuroinflammatory reaction to the presence of the parasites. This article attempts to survey the predisposing factors, clinical outcomes and complications of these infestations, while exploring the complex interplay between the clinical presentation, diagnostic modalities and interactions between humans and their environment which aid the proliferation of these parasites. It is imperative to highlight the importance of optimal clinical scrutiny and judgment in diagnosing these conditions while advocating for public health intervention strategies and collaborative research efforts to ameliorate the potential complications of these infestations which exert an extreme impact in the prognosis of affected patients with attendant neurologic sequelae. VL - 9 IS - 1 ER -
Neurosurgery Unit, Department of Surgery, Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria
Department of Morbid Anatomy and Forensic Medicine, Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria
Department of Morbid Anatomy and Forensic Medicine, Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria
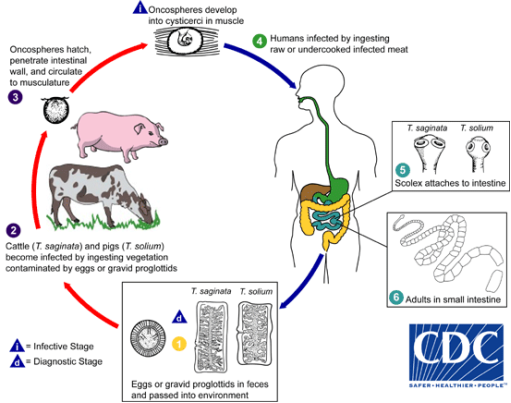
Figure 1. Life Cycle of Taeniasis showing Pigs as intermediate host who consume eggs of the parasite in contaminated vegetation. Humans as the definitive hosts of the parasite get infected from consuming poorly prepared pork meat [5].
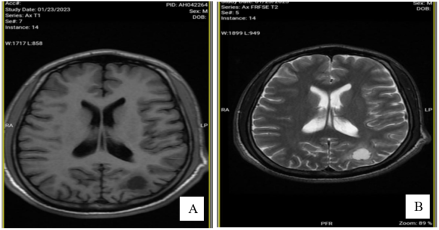
Figure 2. Axial magnetic resonance images of a 23 year old male managed for neurocysticercosis (A) T1 Image showing isointensity of the lesion. (B) T2 image showing hyperintensity.
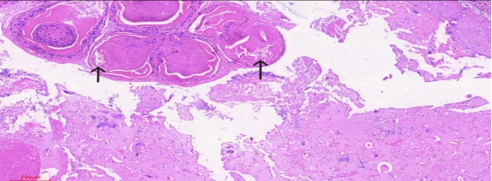
Figure 3. Histology slides of a patient with neurocysticercosis showing cyst walls encircling the parasite and surrounded by foamy macrophages and giant cells.
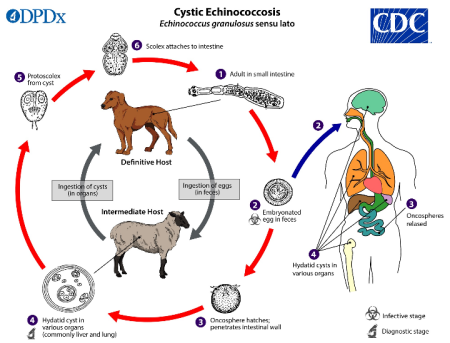
Figure 4. Life Cycle of Echinococcosis showing that humans get infected by ingesting food or water containing eggs of the parasite passed on by infected dogs or sheep [16].
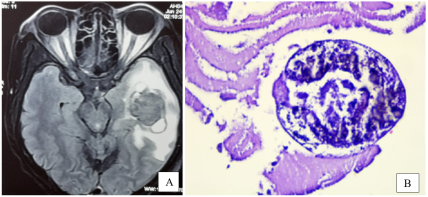
Figure 5. (A) Axial T2 FLAIR image showing multiple sac like echinococci daughter cysts in the left temporal lobe surrounding a central necrotic core with perilesional edema (B) Histology slide of a cerebral hydatid cyst showing a calcified scolex of Echinococcus granulosus [17].
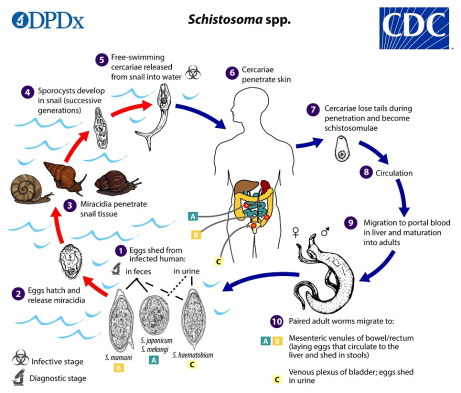
Figure 6. Life cycle of Schistosoma spp showing the bulinus snail as the intermediate host which releases cercariae that infects man, the definitive host of the parasite [20].
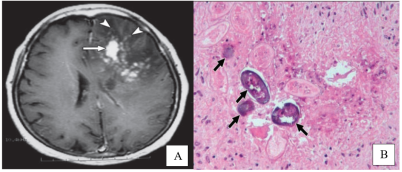
Figure 7. (A) Axial TI image with contrast showing an aggregate of nodular lesions which are contrast enhancing in the left frontal lobe with marked perilesional edema and effacement of the left lateral ventricle. (B) Histopathologic slide with arrows showing multiple ova of Schistosoma japonicum and granuloma formation around them [22].
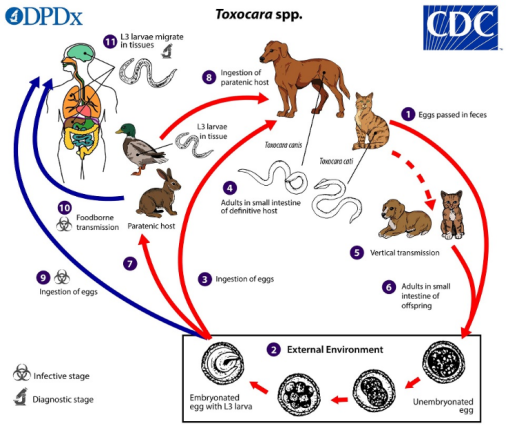
Figure 8. Life cycle of toxocariasis showing a complex interplay between multiple intermediate hosts and humans as the definitive host who get infected from consumption of poorly prepared animal food [25].
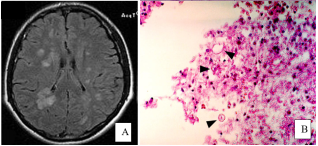
Figure 9. (A) Brain CT scan image of a patient with toxocariasis showing multiple bilateral hyperdense lesions in the periventricular and subcortical regions with biventricular effacement [28]. (B) Histology slide with arrows showing larva of Toxocara spp in the brain with surrounding layer of inflammatory cells [21].
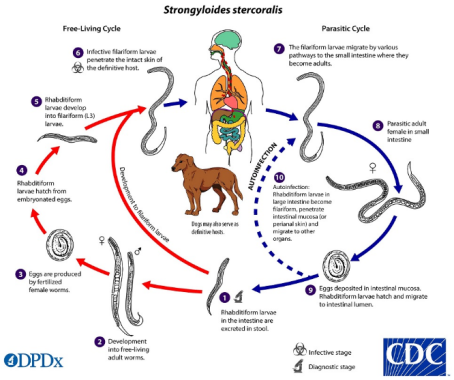
Figure 10. Life cycle of Strongyloides stercolaris showing an interconnection between the parasitic and free living forms of the parasite [34].
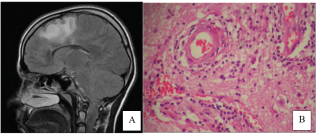
Figure 11. (A) MRI FLAIR image of a 13 year old female patient showing a hyperintense lesion in the frontal lobe anterior to the Rolandic sulcus with an irregular hyperintense rim of perilesional edema (B) Histopathology slide of a resected specimen from the lesion showing vasculitis with surrounding eosinophilic cells and macrophages [36].
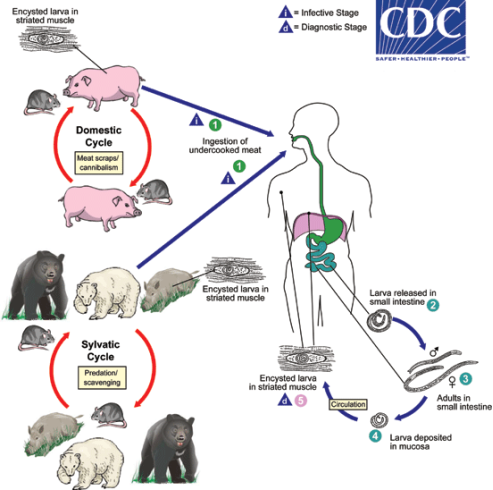
Figure 12. Life cycle of Trichinella spp. Humans contract the disease by consumption of undercooked animals [39].
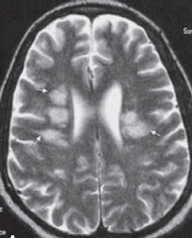
Figure 13. Axial T2 weighted image of a patient with neurotrihinellosis showing multiple bilateral subcortical hyperintense lesions with minimal rim of perilesional edema [43].
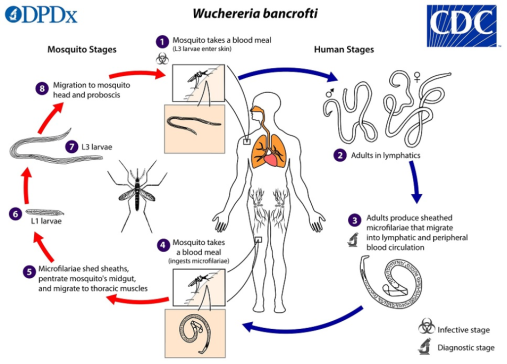
Figure 14. Life Cycle of the filarial infestation, Wuchereria bancrofti [46].
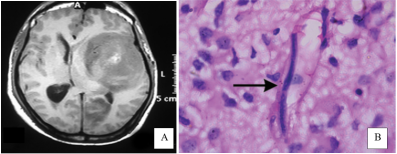
Figure 15. (A) Axial T1 MRI of a 27 year old male with neurofilariasis showing a concentric shaped mixed intensity lesion in the left cerebral hemisphere abuting on the basal ganglia, obliterating the left ventricle with periventricular hyperintense lesions (B) Histopathology slide with arrow showing microfilariae within a cerebral cappilary in a background of reactive gemistocyte and inflammatory cells with widening of the Virchow Robin spaces [44].
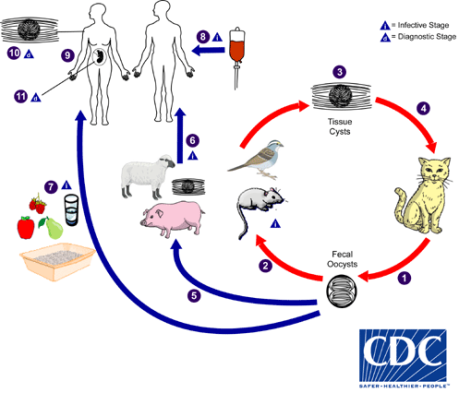
Figure 16. Life Cycle of Toxoplasma gondii. [55].

Figure 17. (A) Axial contrast MRI of a patient with Cerebral toxoplasmosis showing bi-thalamic concentric shaped lesions abutting on the wall of the 3rd ventricle. The left lesion is contrast enhancing. (B) Histopathology slides of cerebral toxoplasmosis showing the classic triad of interfollicular and perifollicular epithelioid histocytes with patches of B-lymphocytes in a background of reactive germinal regions.
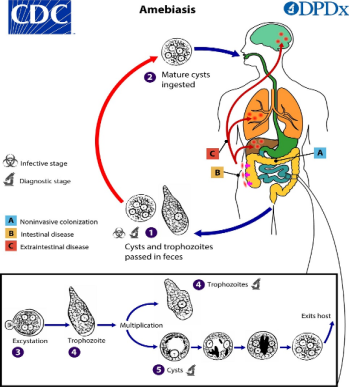
Figure 18. Life cycle of amebiasis depicting human transmission occurs from ingestion of mature cyst through various media including contaminated water and food [66].
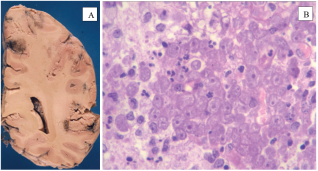
Figure 19. (A) Gross specimen showing the left half of the coronal section of a brain with granulomatous amebic encephalitis showing multiple petechial hemorrhagic nodules with adjacnt areas of tissue necrosis in the subcortical white matter and cerebral cortex (B) Histopathologic slide showing grnulomatous amebic encephalitis caused by Balamuthia mandrillaris. There is marked eosinophilia around the trophozoites of the parasite with a prominent large lymphocyte in the background. [47].

Figure 20. Contrast enhanced coronal and axial CT scan images of a patient with right temporal lobe amebic brain abscess showing an irregular shaped hypointense lesion with mild perilesional edema and encephalomalacia of surrounding brain tissue.
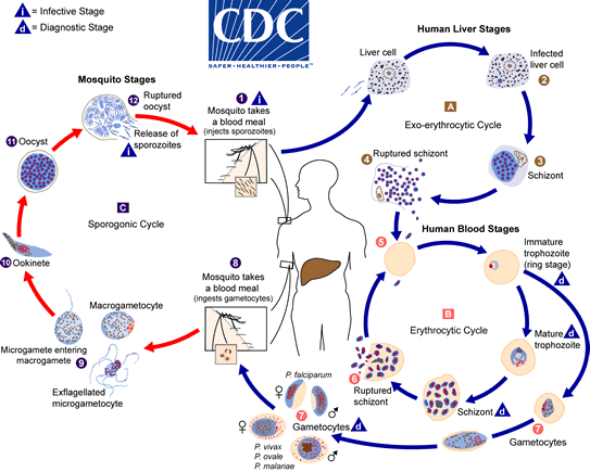
Figure 21. Life cycle of Plasmodiasis [75].
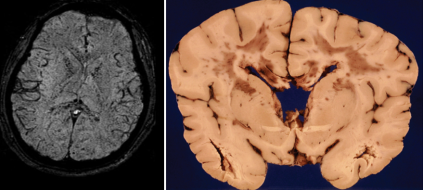
Figure 22. Cerebral malaria (A) Axial view of susceptibility weighted MRI sequence showing multiple areas of petechial hemorrhages noted at the corpus callosum, internal capsule and grey white matter junction. 76 (B) Coronal view of gross brain specimen with cerebral malaria showing areas of multiple petechial hemorrhages involving the cerebral white matter, internal capsule and corpus callosum with flattening of the gyri [47].
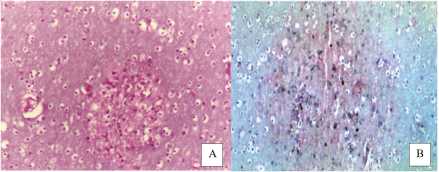
Figure 23. Histopathology slides in cerebral malaria. (A) Durck granuloma which is a collection of brain microglial cells around a capillary containing parasitized red blood cells. (B) Hemozoin pigment, a crystalline brownish discoloration due to iron-porphyrin complex derived from anerobic metabolism of glucose and hemoglobin breakdown by plasmodium parasites in the red blood cells. [47].
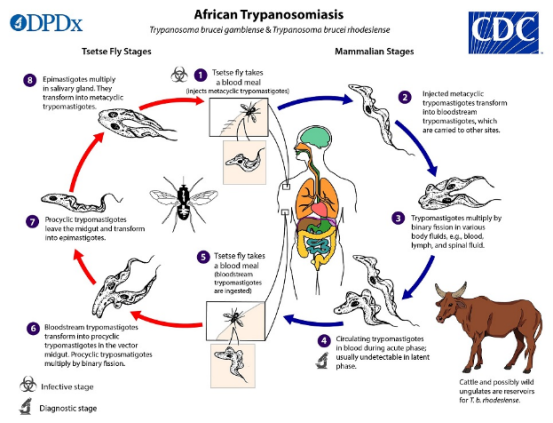
Figure 24. Life cycle of African trypanosomiasis [80].
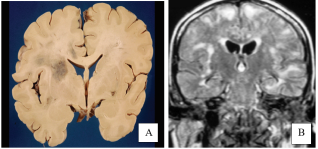
Figure 25. (A) Coronal section of a gross brain specimen of a patient who had Chagas disease showing necrotic hemorrgic area involving the right cerebral white cortical matter and the basal ganglia with anterior limb and genu of the right internal capsule [47]. (B) Coronal section of T2 FLAIR image of a 52 year old female patient with cerebral Chagas disease showing multiple areas of hyprintensee lesions along the sylvian fisssures, parafalcine regions and cerebral convexities. [84].
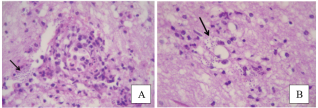
Figure 26. Hematoxylin-eosin staining of a resected brain specimen of a patient with Chagas encephalitis in low power (A) and high power (B) magnification with an arrow showing amastigote nest in a background of perivascular aggregate of eosinophils and lymphocytes. [47].
Information

