Neuromyelitis Optica spectrum disorder is a condition in which antibodies are elaborated against aquaporin water channels in the end foot processes of astrocytes due to autoimmune dysregulation thereby initiating a cascade of neuroinflammatory events that culminates in astrocytic injury, dysfunctional axonal blebs and demyelination of the central nervous system neurons. Its cervical spine symptom may sometimes mimic a similar presentation of a cervical spine lesion, this is further underscored by its core clinical magnetic resonance image feature of longitudinally extensive transverse myelitis bearing radiologic similarities with an intramedullary spinal cord lesion thereby resonating the need to maintain a high index of suspicion when evaluating patients with either conditions. Laboratory elucidation of increased titers of aquaporin -4 immunoglobulin and seronegativity for oligoclonal bands is the diagnostic hallmark of the condition and helps differentiate it from similar conditions such as multiple sclerosis and myelin oligodendrocyte glycoprotein disorder. While the mainstay of treatment involves the use of steroids, immunosuppressive therapy and plasmapheresis, it is pertinent to highlight that surgery may have a potential benefit in patients with acute exacerbations of symptoms attributable to cervical spine compressive myelopathy due to the disease. We report a case of a 50-year-old female who had clinical features initially suspected to be a spinal cord lesion but eventually proven with laboratory parameters and histological analysis of resected tissue specimen to be in keeping with Neuromyelitis Optica spectrum disorder.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Neuromyelitis Optica spectrum disorder is a disease condition of the central nervous system in which there is an autoimmune complement and antibody-mediated cellular destruction causing injury o astrocytes with an impediment to their functions such as the perpetuation of immune responses, propagation of synaptic transmission and maintenance of the integrity of the blood-brain barrier
[1]
Lucchinetti CF, Guo Y, Popescu B, et al. The pathology of an autoimmune astrocytopathy: lessons learned from neuromyelitis optica. Brain Pathol 2014; 24(1): 83-97.
Described by Eugene Devic in 1984, the disease condition which was previously attributed to bear similarity with multiple sclerosis, has been distinguished from the former as an autoimmune astrocytopathy following the discovery of antibodies IgG that bind to the water channel aquaporin-4 located in the astrocytic end foot process. This stimulates a cascade of cell-mediated and antibody-dependent destruction of astrocytes with consequent loss of oligodendrocytes leading to demyelination
[2]
Fujihara K, Misu T, Nakashima I, et al. Neuromyelitis optica should be classified as an astrocytopathic disease rather than a demyelinating disease. Clin Exp Neuroimmunol 2012; 3: 58-73.
Given an annual worldwide prevalence range of 0.5 to 4 per 100,000, the highest incidence and prevalence rate of 0.73 per 100,000 and 10 per 100,000 persons respectively have been documented in the Afro-Caribbean regions with a 40-year mean age of onset and a male-to-female ratio of 1:9
[3]
Papp V, Magyari M, Aktas O, et al. Worldwide incidence and prevalence of neuromyelitis optica. Neurology 2021; 96(2): 59-77.
. Systematic review of Eligible studies in Africa documented 410 cases reported in 10 African countries mainly domiciled in the North Africa subregion with a median age of diagnosis of 33 years and female preponderance of 75%
[4]
Musubire AK, Derdelinckx J, Reynders T, Meya DB, Bohjanen PR, Cras P, Willekens B. Neuromyelitis Optica Spectrum Disorders in Africa: A Systematic Review. Neurol Neuroimmunol Neuroinflamm. 2021 Oct 18; 8(6): e1089.
While documented reports have shown patients with spastic quadriplegia, tonic spasms, neck pain with a positive Lhermitte sign and biochemical features of antiphospholipid syndrome
[5]
Komolafe MA, Komolafe EO, Sunmonu T, Olateju S, Asaleye M, Adesina OA, Badmus SA. New onset neuromyelitis optica in a young Nigerian woman with possible antiphospholipid syndrome: A case report. Journal of Medical Case Reports. 2008; 2(1): 348.
, the core clinical features of the disease condition include longitudinally extensive transverse myelitis, optic neuritis, area postrema syndrome and brainstem syndromes with presentation of gaze palsies, hearing loss, difficulty with breathing and swallowing which are indicative of cranial nerve involvement
[6]
Wingerchuk DM, Banwell B, Bennett JL, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology 2015; 85(2): 177-189.
Given the rarity of the disease condition, its clinical manifestation of symptoms that may be suggestive of other common prevalent conditions such as a high cervical spine lesion and the relative unavailability and high cost of diagnostic modalities in a resource-limited setting, its clinical presentation often presents a diagnostic dilemma which requires a high index of suspicion and clinical acumen to diagnose.
2. Case Presentation
A 50-year-old right-handed female presented to us with Progressive weakness involving all limbs of 2 weeks duration. The weakness started from the left shoulder, then the left upper limb and progressed in a cyclical pattern until the patient became quadriplegic over a 2-week duration. There was a history of a one-week fever and sore throat which occurred a month before presentation and resolved when she took antibiotics and antimalaria medication. There was a positive history of photophobia with no blurring of vision or diplopia. She had recurrent episodes of vomiting with no other features suggestive of raised intracranial pressure. There was difficulty with swallowing, however there was no hearing loss nor dysphagia. She had no history of similar symptoms in a first-degree family relative.
Pertinent findings on examination were essentially in the neurologic system where she had an increased tone and deep tendon reflexes (Table 1) with motor and sensory levels bilaterally at C4 myotome and C5 dermatomes respectively. Joint position and vibration sense were absent bilaterally. Per rectal examination showed an absent perianal and deep anal pressure sensation, a lax anal sphincteric tone and an absent bulbocavernosus reflex. She had features of lower cranial nerve palsies such as difficulty with deglutition and tongue protrusion.
Table 1. Musculoskeletal examination findings.
Motor examination
Right upper limb
Right lower limb
Left upper limb
Left lower limb
Bulk
Normal
Normal
Normal
Normal
Tone
Increased
Increased
Increased
Increased
Power
MRC grade 0
MRC grade 0
MRC grade 0
MRC grade 0
Reflexes
Increased
Increased
Increased
Increased
We entertained a diagnosis of a high cervical spinal cord tumour with the possibility of a foramen magnum lesion and demyelinating diseases of the central nervous system such as multiple sclerosis, neuromyelitis optica spectrum disorder and myelin oligodendrocyte associated glycoprotein disorders. She had laboratory blood investigations, the results of which are shown in Table 2.
Table 2. Laboratory investigation results.
Value
Interpretation
Packed cell volume
45%
Normal
White blood cell count
7000 cells/mm3
Normal
Platelets
213,000 cells/mm3
Normal
Creatinine
151mmol/L (50-132mmol/L)
Elevated
Urea
12.5mmol/L (2.5-5.8mmol/L)
Elevated
Potassium
3.5mmol/L (3-5mmol/L)
Normal
Sodium
135mmol/L (120-140mmol/L)
Normal
Bicarbonate
22mmol/L (20-30mmol/L)
Normal
Hepatitis B surface antigen
Positive
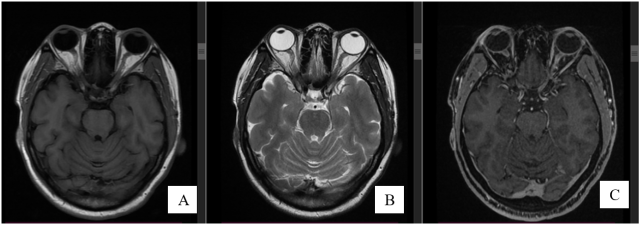
A brain magnetic resonance image showed an impingement in the course of the right optic nerve with decreased T2 signal intensity within the nerve close to the optic chiasm and decreased contrast uptake (Figure 1).
Figure 1. Brain MRI scan showing hyperintensity in the course of the right optic nerve on T1 weighted image (A), with a relatively increased signal intensity within the nerve compared to the left on T2 weighted image (B) and decreased contrast uptake in the right optic nerve (C).
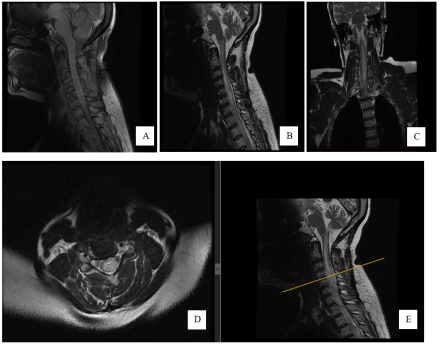
A cervical spine Magnetic Resonance Image (MRI) scan revealed a non-contrast enhancing longitudinal intramedullary spinal cord lesion extending from C3 to T2 spinal segment with bulbous expansion of the cord, increased signal on T2 and decreased CSF signal on myelogram of the involved spinal cord segments (Figure 2).
On the 3rd-day post-admission, she developed severe respiratory distress thereby necessitating admission into the intensive care unit this also informed the decision for emergency surgical exploration with the aim of resection while serum samples for Aquaporin 4 IgG antibodies and oligoclonal bands were sent to the laboratory for assay to rule out other differential diagnosis.
Figure 2. Cervical spine MRI scan with (A) Sagittal T1 image showing isointense bulbous expansion of the cord from C3-C7 spinal segments. (B) and (C) Sagittal and coronal T2 weighted images showing increased signal intensity within the bulbous spinal cord expansion extending from C3-C7 spinal segments. (D) T2 weighted image showing an Axial representation of a Sagittal slice (E) of the spinal cord at C4/C5 segment showing the lesion to be intramedullary.
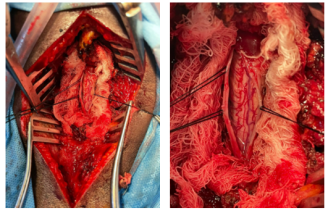
On the 4th day of admission, due to progressively worsening respiratory distress and deteriorating clinical condition, she had a C3-C6 Laminectomy with intramedullary exploration and biopsy of a C5 spinal cord segment for histologic analysis. Intra-operative findings were a normal-looking dura and normal spinal cord consistency with no obvious intramedullary tumour (Figure 3).
Figure 3. Intra-operative pictures showing a normal spinal cord appearance with no extramedullary nor intramedullary lesion visible.
On the 2nd day post-op, her laboratory results returned with elevated titers of aquaporin 4 IgG antibodies (1:32) while serum MOD IgG antibody titers were not elevated. Her D-dimer and C-reactive protein levels were elevated while her other investigation results were within the normal range of values (Table 3).
Table 3. Laboratory investigations showing elevated titres of Serum AQP4 antibody and other acute phase proteins.
Parameter
Value
Interpretation
Serum AQP4 antibody
Titre 1:32
Elevated
Serum MOG IgG antibody
Titre 1: <10
Not elevated
D-dimer
>10 (0-0.5mg/L)
Elevated
Serum lactate
0.87 (0.5 -2.2mmol/L)
Normal
C-reactive protein
255.33 (<10mmol/L)
Elevated
Postoperatively she was managed in the intensive care unit on ventilatory support through an endotracheal tube, had nasogastric tube feeding and was placed on meropenem, metronidazole, LMW heparin, azathioprine, prednisolone, rabeprazole, haematinics, tenofovir, vitamin D and warfarin. She was also commenced on cardiopulmonary and neurophysiotherapy.
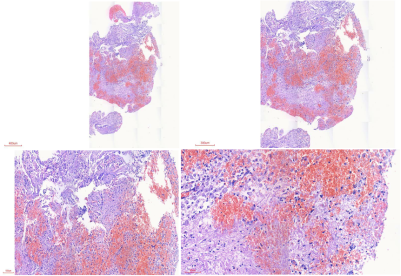
Histology report of the biopsied tissue specimen made a pathologic diagnosis of an Inflammatory lesion with no evidence of malignancy (Figure 4).
Figure 4. Microscopic section showing neural tissue with reactive glial cells showing ballooning and cytoplasmic clearing. There is edema, hemorrhage and capillary proliferation with no atypical cells seen.
She had a tracheostomy sited on POD-12 and was maintained on CPAP ventilatory mode afterwards. She developed sudden onset respiratory distress on postoperative day 27 with consequent hemodynamic instability. Efforts at cardiopulmonary resuscitation were not successful as she died some minutes later.
3. Discussion
Neuromyelitis Optica spectrum disorder is an autoimmune disease condition in which antibodies are elaborated against aquaporin 4 IgG domiciled in the astrocytic end foot process initiating a cascade of cell-mediated antibody and complement-dependent destruction of astrocytes leading to loss of oligodendrocytes and extensive demyelination in the central nervous system
[7]
Winkler A, Wrzos C, Haberl M, et al. Blood-brain barrier resealing in neuromyelitis optica occurs independently of astrocyte regeneration. J Clin Invest 2021; 131(5): e141694.
Fujihara K, Misu T, Nakashima I, et al. Neuromyelitis optica should be classified as an astrocytopathic disease rather than a demyelinating disease. Clin Exp Neuroimmunol 2012; 3: 58-73.
It is predominantly a disease with female preponderance affecting middle-aged women
[2]
Fujihara K, Misu T, Nakashima I, et al. Neuromyelitis optica should be classified as an astrocytopathic disease rather than a demyelinating disease. Clin Exp Neuroimmunol 2012; 3: 58-73.
The pathogenesis of the condition involves risk factors such as infection, oxidative stress and immune tolerance dysfunction leading to local inflammation, pathogenic antibody formation and denudation of the blood-brain barrier
[7]
Winkler A, Wrzos C, Haberl M, et al. Blood-brain barrier resealing in neuromyelitis optica occurs independently of astrocyte regeneration. J Clin Invest 2021; 131(5): e141694.
. Our patient had a poorly treated upper respiratory tract infection a month before the onset of symptoms which could have served as a predisposing risk factor. She also showed raised serum titers of acute phase proteins such as C-reactive protein and D-dimer which are markers of inflammation.
She manifested key cardinal diagnostic clinical features of the disease such as area postrema syndrome, transverse myelitis and brainstem syndrome
[6]
Wingerchuk DM, Banwell B, Bennett JL, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology 2015; 85(2): 177-189.
manifesting as difficulty with swallowing, breathing and limb weakness
[8]
Flanagan E. Neuromyelitis optica spectrum disorder and other non-multiple sclerosis central nervous system inflammatory diseases. Continuum (Minneap Minn) 2019; 25(3): 815-844.
, as well as brain and cervical MRI features in keeping with a possible right optic neuritis and longitudinally extensive transverse myelitis respectively. Other MRI diagnostic requirements which were not apparent in our patient include area postrema/dorsal medulla lesions, and peri ependymal brainstem lesions
[6]
Wingerchuk DM, Banwell B, Bennett JL, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology 2015; 85(2): 177-189.
Her histopathologic slides showed reactive glial cells with cytoplasmic clearing, edema and capillary proliferation in keeping with the neuro-inflammatory process. This is similar to findings of axonal damage, eosinophilic infiltration, microglia cell activation and perivascular immunoglobulin deposition typically seen in Devic’s disease
[9]
Gold R, Linington C. Devic’s disease: bridging the gap between laboratory and clinic. Brain. 2002 Jul; 125(Pt 7): 1425-7.
Given the relative rarity of the condition in our environment and the clinical presentation of the patient, our initial diagnosis was a possible foramen magnum lesion. The cervical MRI finding made us consider an intramedullary spinal cord lesion. The rapidly progressive nature of the course of her symptoms informed the decision for ICU admission, mechanical ventilation, and surgical decompression of the spine to relieve symptoms and obtain biopsy tissue for histologic analysis. We also entertained other possible medical differential diagnoses such as myelin oligodendrocyte disorder, neuromyelitis Optica spectrum disorder and multiple sclerosis, which motivated the need to request serum aquaporin 4 antibodies and oligoclonal bands to confirm diagnosis and rule out other differentials.
There has been documented evidence of marked postoperative neurologic improvement in 89% of 19 patients with compressive cervical myelopathy due to CNS demyelinating disease
[10]
Youssef C, Barrie U, Elguindy M, Christian Z, Caruso JP, Johnson ZD, Hall K, Aoun SG, Bagley CA, Al Tamimi M. Compressive Cervical Myelopathy in Patients With Demyelinating Disease of the Central Nervous System: Improvement After Surgery Despite a Late Di.
[10]
and symptomatic relief following surgical decompression and instrumental fusion in a patient presenting with radiologic features in keeping with ossified posterior longitudinal ligament of the cervical and thoracic spine
[11]
Kodama H, Kawamura N, Nagatani S, Ishikawa Y, Kunogi J. Neuromyelitis Optica Spectrum Disorders (NMOSDs) Diagnosed After Surgery for the Ossification of the Posterior Longitudinal Ligament of the Cervical and Thoracic Spine: A Case Report. Cureus. 2024 Ju.
[11]
thereby lending credence to the assertion that surgical treatment may confer some clinical improvement in patients with features of compressive myelopathy secondary to demyelinating spine disease
[10]
Youssef C, Barrie U, Elguindy M, Christian Z, Caruso JP, Johnson ZD, Hall K, Aoun SG, Bagley CA, Al Tamimi M. Compressive Cervical Myelopathy in Patients With Demyelinating Disease of the Central Nervous System: Improvement After Surgery Despite a Late Di.
[10]
.
Our patient had a cell-based assay of serum AQP4 in the course of her evaluation which is the recommended standard of laboratory investigative modality with a sensitivity and specificity yield of 80-100% and 86-100% respectively
[6]
Wingerchuk DM, Banwell B, Bennett JL, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology 2015; 85(2): 177-189.
Flanagan E. Neuromyelitis optica spectrum disorder and other non-multiple sclerosis central nervous system inflammatory diseases. Continuum (Minneap Minn) 2019; 25(3): 815-844.
. This has an advantage over enzyme-linked immunosorbent assay (ELISA) test with a higher yield of false positive results. However, it has been noted that the serum levels of AQP4 IgG do not reliably predict the course of the disease nor response to therapy, thus creating a need for biomarkers that could gauge the course and severity of the disease
[12]
Sato DK, Callegaro D, Lana-Peixoto MA, et al. Distinction between MOG antibody-positive and AQP4 antibody-positive NMO spectrum disorders. Neurology 2014; 82(6): 474-481.
The aim of immunosuppressive therapy includes preventing relapses, and increasing the chances of recuperation from acute disease exacerbation while attenuating the risk of disability
[2]
Fujihara K, Misu T, Nakashima I, et al. Neuromyelitis optica should be classified as an astrocytopathic disease rather than a demyelinating disease. Clin Exp Neuroimmunol 2012; 3: 58-73.
. Medications that have been used in the treatment and control of disease progression include mycophenolate mofetil, rituximab, azathioprine and prednisolone
[13]
Brod SA. Review of approved NMO therapies based on mechanism of action, efficacy and long-term effects. Mult Scler Relat Disord 2020; 46: 102538.
; she had the latter two among other medications and showed a reduction of respiratory distress following commencement of therapy.
Elucidation of the immunopathogenesis of the disease has led to the discovery of monoclonal antibodies that modify complement system activation, decrease antibody production and block IL-6 receptor; this has been reflected in the mechanism of action of novel therapies such as Eculizumab, Inebilizumab and Satralizumab respectively
[13]
Brod SA. Review of approved NMO therapies based on mechanism of action, efficacy and long-term effects. Mult Scler Relat Disord 2020; 46: 102538.
. Immune reconstitution treatments such as autologous transplant of stem cell bone marrow have demonstrated some clinical improvement in disease course, reducing progression to disability, and inducing remission of clinical symptoms and radiologic features of disease
[15]
Greco R, Bondanza A, Oliveria MC, et al. Autologous hematopoietic stem cell transplantation in neuromyelitis optica: a registry study of the EBMT Autoimmune Diseases Working Party. Mult Scler 2015; 21(2): 189-197.
Burton JM, Duggan P, Costello F, et al. A pilot trial of autologous hematopoietic stem cell transplant in neuromyelitis optic spectrum disorder. Mult Scler Relat Disord 2021; 53: 102990.
Our patient developed sudden onset respiratory distress which culminated in her demise. While this could be attributable to a possible relapse, she had some of the risk factors associated with increased propensity for relapse such as younger age, female sex and either African or European descent, having a short disease duration that could have predisposed her to more episodes of acute exacerbation
[17]
Ma X, Kermode AG, Hu X, Qui W. Risk of relapse in patients with neuromyelitis optica spectrum disorder: recognition and preventive strategy. Mult Scler Relat Disord 2020; 46: 102522.
. Relapses could be heralded by tonic spasms and area postrema syndrome with the recovery of two-thirds of cases following early administration of high-dose corticosteroids with or without plasma exchange therapy administered within two weeks of onset of symptoms
[19]
Banerjee A, Ng J, Coleman J, et al. Outcomes from acute attacks of neuromyelitis optica spectrum disorder correlate with severity of attack, age and delay to treatment. Mult Scler Relat Disord 2019; 28: 60-63.
This article highlights an incidence of Neuromyelitis Optica spectrum disorder and the need to entertain a high index of suspicion of its existence while evaluating potential patients who present with compressive features presumably attributable to cervical spine tumours. It underscores that in addition to the mainstream medical management comprising of immunosuppressive therapy, steroids and plasma exchange therapy, surgical decompression of the spine may offer the benefit of acute relief of complaints in patients who may have symptoms of compressive myelopathy attributable to the affected spine segments.
Abbreviations
AQP4
Aquaporin 4
MRC
Medical Research Council
MOG
Myelin Oligodendrocyte Glycoprotein
CPAP
Continuous Positive Airway Pressure
POD
Post-Operative Day
MRI
Magnetic Resonance Image
ELISA
Enzyme Linked Immunosorbent Assay
IgG
Immunoglobulin G
Author Contributions
Kelechi Michael Azode: Conceptualization, Data curation, Formal Analysis, Writing – original draft, Writing – review & editing
Simon Adewale Balogun: Supervision, Validation, Visualization
Edward Oluwole Komolafe: Project administration, Supervision, Validation, Visualization
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Lucchinetti CF, Guo Y, Popescu B, et al. The pathology of an autoimmune astrocytopathy: lessons learned from neuromyelitis optica. Brain Pathol 2014; 24(1): 83-97.
Fujihara K, Misu T, Nakashima I, et al. Neuromyelitis optica should be classified as an astrocytopathic disease rather than a demyelinating disease. Clin Exp Neuroimmunol 2012; 3: 58-73.
Komolafe MA, Komolafe EO, Sunmonu T, Olateju S, Asaleye M, Adesina OA, Badmus SA. New onset neuromyelitis optica in a young Nigerian woman with possible antiphospholipid syndrome: A case report. Journal of Medical Case Reports. 2008; 2(1): 348.
Winkler A, Wrzos C, Haberl M, et al. Blood-brain barrier resealing in neuromyelitis optica occurs independently of astrocyte regeneration. J Clin Invest 2021; 131(5): e141694.
Flanagan E. Neuromyelitis optica spectrum disorder and other non-multiple sclerosis central nervous system inflammatory diseases. Continuum (Minneap Minn) 2019; 25(3): 815-844.
Youssef C, Barrie U, Elguindy M, Christian Z, Caruso JP, Johnson ZD, Hall K, Aoun SG, Bagley CA, Al Tamimi M. Compressive Cervical Myelopathy in Patients With Demyelinating Disease of the Central Nervous System: Improvement After Surgery Despite a Late Di.
[11]
Kodama H, Kawamura N, Nagatani S, Ishikawa Y, Kunogi J. Neuromyelitis Optica Spectrum Disorders (NMOSDs) Diagnosed After Surgery for the Ossification of the Posterior Longitudinal Ligament of the Cervical and Thoracic Spine: A Case Report. Cureus. 2024 Ju.
[12]
Sato DK, Callegaro D, Lana-Peixoto MA, et al. Distinction between MOG antibody-positive and AQP4 antibody-positive NMO spectrum disorders. Neurology 2014; 82(6): 474-481.
Greco R, Bondanza A, Oliveria MC, et al. Autologous hematopoietic stem cell transplantation in neuromyelitis optica: a registry study of the EBMT Autoimmune Diseases Working Party. Mult Scler 2015; 21(2): 189-197.
Burton JM, Duggan P, Costello F, et al. A pilot trial of autologous hematopoietic stem cell transplant in neuromyelitis optic spectrum disorder. Mult Scler Relat Disord 2021; 53: 102990.
Ma X, Kermode AG, Hu X, Qui W. Risk of relapse in patients with neuromyelitis optica spectrum disorder: recognition and preventive strategy. Mult Scler Relat Disord 2020; 46: 102522.
Banerjee A, Ng J, Coleman J, et al. Outcomes from acute attacks of neuromyelitis optica spectrum disorder correlate with severity of attack, age and delay to treatment. Mult Scler Relat Disord 2019; 28: 60-63.
Azode, K. M., Balogun, S. A., Komolafe, M. A., Olasode, B. J., Komolafe, E. O. (2025). Diagnostic Dilemma in the Management of a Cervical Spinal Cord Lesion: A Case Report of Neuromyelitis Optica Spectrum Disorder. International Journal of Neurosurgery, 9(1), 23-29. https://doi.org/10.11648/j.ijn.20250901.14
Azode, K. M.; Balogun, S. A.; Komolafe, M. A.; Olasode, B. J.; Komolafe, E. O. Diagnostic Dilemma in the Management of a Cervical Spinal Cord Lesion: A Case Report of Neuromyelitis Optica Spectrum Disorder. Int. J. Neurosurg.2025, 9(1), 23-29. doi: 10.11648/j.ijn.20250901.14
Azode KM, Balogun SA, Komolafe MA, Olasode BJ, Komolafe EO. Diagnostic Dilemma in the Management of a Cervical Spinal Cord Lesion: A Case Report of Neuromyelitis Optica Spectrum Disorder. Int J Neurosurg. 2025;9(1):23-29. doi: 10.11648/j.ijn.20250901.14
@article{10.11648/j.ijn.20250901.14,
author = {Kelechi Michael Azode and Simon Adewale Balogun and Morenikeji Adeyoyin Komolafe and Babatunde Josiah Olasode and Edward Oluwole Komolafe},
title = {Diagnostic Dilemma in the Management of a Cervical Spinal Cord Lesion: A Case Report of Neuromyelitis Optica Spectrum Disorder
},
journal = {International Journal of Neurosurgery},
volume = {9},
number = {1},
pages = {23-29},
doi = {10.11648/j.ijn.20250901.14},
url = {https://doi.org/10.11648/j.ijn.20250901.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijn.20250901.14},
abstract = {Neuromyelitis Optica spectrum disorder is a condition in which antibodies are elaborated against aquaporin water channels in the end foot processes of astrocytes due to autoimmune dysregulation thereby initiating a cascade of neuroinflammatory events that culminates in astrocytic injury, dysfunctional axonal blebs and demyelination of the central nervous system neurons. Its cervical spine symptom may sometimes mimic a similar presentation of a cervical spine lesion, this is further underscored by its core clinical magnetic resonance image feature of longitudinally extensive transverse myelitis bearing radiologic similarities with an intramedullary spinal cord lesion thereby resonating the need to maintain a high index of suspicion when evaluating patients with either conditions. Laboratory elucidation of increased titers of aquaporin -4 immunoglobulin and seronegativity for oligoclonal bands is the diagnostic hallmark of the condition and helps differentiate it from similar conditions such as multiple sclerosis and myelin oligodendrocyte glycoprotein disorder. While the mainstay of treatment involves the use of steroids, immunosuppressive therapy and plasmapheresis, it is pertinent to highlight that surgery may have a potential benefit in patients with acute exacerbations of symptoms attributable to cervical spine compressive myelopathy due to the disease. We report a case of a 50-year-old female who had clinical features initially suspected to be a spinal cord lesion but eventually proven with laboratory parameters and histological analysis of resected tissue specimen to be in keeping with Neuromyelitis Optica spectrum disorder.
},
year = {2025}
}
TY - JOUR
T1 - Diagnostic Dilemma in the Management of a Cervical Spinal Cord Lesion: A Case Report of Neuromyelitis Optica Spectrum Disorder
AU - Kelechi Michael Azode
AU - Simon Adewale Balogun
AU - Morenikeji Adeyoyin Komolafe
AU - Babatunde Josiah Olasode
AU - Edward Oluwole Komolafe
Y1 - 2025/04/19
PY - 2025
N1 - https://doi.org/10.11648/j.ijn.20250901.14
DO - 10.11648/j.ijn.20250901.14
T2 - International Journal of Neurosurgery
JF - International Journal of Neurosurgery
JO - International Journal of Neurosurgery
SP - 23
EP - 29
PB - Science Publishing Group
SN - 2640-1959
UR - https://doi.org/10.11648/j.ijn.20250901.14
AB - Neuromyelitis Optica spectrum disorder is a condition in which antibodies are elaborated against aquaporin water channels in the end foot processes of astrocytes due to autoimmune dysregulation thereby initiating a cascade of neuroinflammatory events that culminates in astrocytic injury, dysfunctional axonal blebs and demyelination of the central nervous system neurons. Its cervical spine symptom may sometimes mimic a similar presentation of a cervical spine lesion, this is further underscored by its core clinical magnetic resonance image feature of longitudinally extensive transverse myelitis bearing radiologic similarities with an intramedullary spinal cord lesion thereby resonating the need to maintain a high index of suspicion when evaluating patients with either conditions. Laboratory elucidation of increased titers of aquaporin -4 immunoglobulin and seronegativity for oligoclonal bands is the diagnostic hallmark of the condition and helps differentiate it from similar conditions such as multiple sclerosis and myelin oligodendrocyte glycoprotein disorder. While the mainstay of treatment involves the use of steroids, immunosuppressive therapy and plasmapheresis, it is pertinent to highlight that surgery may have a potential benefit in patients with acute exacerbations of symptoms attributable to cervical spine compressive myelopathy due to the disease. We report a case of a 50-year-old female who had clinical features initially suspected to be a spinal cord lesion but eventually proven with laboratory parameters and histological analysis of resected tissue specimen to be in keeping with Neuromyelitis Optica spectrum disorder.
VL - 9
IS - 1
ER -
Azode, K. M., Balogun, S. A., Komolafe, M. A., Olasode, B. J., Komolafe, E. O. (2025). Diagnostic Dilemma in the Management of a Cervical Spinal Cord Lesion: A Case Report of Neuromyelitis Optica Spectrum Disorder. International Journal of Neurosurgery, 9(1), 23-29. https://doi.org/10.11648/j.ijn.20250901.14
Azode, K. M.; Balogun, S. A.; Komolafe, M. A.; Olasode, B. J.; Komolafe, E. O. Diagnostic Dilemma in the Management of a Cervical Spinal Cord Lesion: A Case Report of Neuromyelitis Optica Spectrum Disorder. Int. J. Neurosurg.2025, 9(1), 23-29. doi: 10.11648/j.ijn.20250901.14
Azode KM, Balogun SA, Komolafe MA, Olasode BJ, Komolafe EO. Diagnostic Dilemma in the Management of a Cervical Spinal Cord Lesion: A Case Report of Neuromyelitis Optica Spectrum Disorder. Int J Neurosurg. 2025;9(1):23-29. doi: 10.11648/j.ijn.20250901.14
@article{10.11648/j.ijn.20250901.14,
author = {Kelechi Michael Azode and Simon Adewale Balogun and Morenikeji Adeyoyin Komolafe and Babatunde Josiah Olasode and Edward Oluwole Komolafe},
title = {Diagnostic Dilemma in the Management of a Cervical Spinal Cord Lesion: A Case Report of Neuromyelitis Optica Spectrum Disorder
},
journal = {International Journal of Neurosurgery},
volume = {9},
number = {1},
pages = {23-29},
doi = {10.11648/j.ijn.20250901.14},
url = {https://doi.org/10.11648/j.ijn.20250901.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijn.20250901.14},
abstract = {Neuromyelitis Optica spectrum disorder is a condition in which antibodies are elaborated against aquaporin water channels in the end foot processes of astrocytes due to autoimmune dysregulation thereby initiating a cascade of neuroinflammatory events that culminates in astrocytic injury, dysfunctional axonal blebs and demyelination of the central nervous system neurons. Its cervical spine symptom may sometimes mimic a similar presentation of a cervical spine lesion, this is further underscored by its core clinical magnetic resonance image feature of longitudinally extensive transverse myelitis bearing radiologic similarities with an intramedullary spinal cord lesion thereby resonating the need to maintain a high index of suspicion when evaluating patients with either conditions. Laboratory elucidation of increased titers of aquaporin -4 immunoglobulin and seronegativity for oligoclonal bands is the diagnostic hallmark of the condition and helps differentiate it from similar conditions such as multiple sclerosis and myelin oligodendrocyte glycoprotein disorder. While the mainstay of treatment involves the use of steroids, immunosuppressive therapy and plasmapheresis, it is pertinent to highlight that surgery may have a potential benefit in patients with acute exacerbations of symptoms attributable to cervical spine compressive myelopathy due to the disease. We report a case of a 50-year-old female who had clinical features initially suspected to be a spinal cord lesion but eventually proven with laboratory parameters and histological analysis of resected tissue specimen to be in keeping with Neuromyelitis Optica spectrum disorder.
},
year = {2025}
}
TY - JOUR
T1 - Diagnostic Dilemma in the Management of a Cervical Spinal Cord Lesion: A Case Report of Neuromyelitis Optica Spectrum Disorder
AU - Kelechi Michael Azode
AU - Simon Adewale Balogun
AU - Morenikeji Adeyoyin Komolafe
AU - Babatunde Josiah Olasode
AU - Edward Oluwole Komolafe
Y1 - 2025/04/19
PY - 2025
N1 - https://doi.org/10.11648/j.ijn.20250901.14
DO - 10.11648/j.ijn.20250901.14
T2 - International Journal of Neurosurgery
JF - International Journal of Neurosurgery
JO - International Journal of Neurosurgery
SP - 23
EP - 29
PB - Science Publishing Group
SN - 2640-1959
UR - https://doi.org/10.11648/j.ijn.20250901.14
AB - Neuromyelitis Optica spectrum disorder is a condition in which antibodies are elaborated against aquaporin water channels in the end foot processes of astrocytes due to autoimmune dysregulation thereby initiating a cascade of neuroinflammatory events that culminates in astrocytic injury, dysfunctional axonal blebs and demyelination of the central nervous system neurons. Its cervical spine symptom may sometimes mimic a similar presentation of a cervical spine lesion, this is further underscored by its core clinical magnetic resonance image feature of longitudinally extensive transverse myelitis bearing radiologic similarities with an intramedullary spinal cord lesion thereby resonating the need to maintain a high index of suspicion when evaluating patients with either conditions. Laboratory elucidation of increased titers of aquaporin -4 immunoglobulin and seronegativity for oligoclonal bands is the diagnostic hallmark of the condition and helps differentiate it from similar conditions such as multiple sclerosis and myelin oligodendrocyte glycoprotein disorder. While the mainstay of treatment involves the use of steroids, immunosuppressive therapy and plasmapheresis, it is pertinent to highlight that surgery may have a potential benefit in patients with acute exacerbations of symptoms attributable to cervical spine compressive myelopathy due to the disease. We report a case of a 50-year-old female who had clinical features initially suspected to be a spinal cord lesion but eventually proven with laboratory parameters and histological analysis of resected tissue specimen to be in keeping with Neuromyelitis Optica spectrum disorder.
VL - 9
IS - 1
ER -