Glossopharyngeal neuralgia (GPN) is characterized by paroxysmal, severe, and lancinating pain at the base of the tongue and throat on one side, often radiating to the oropharynx or ear. The intensity of the pain can be debilitating and, in severe cases, may be accompanied by potentially life-threatening conditions such as cardiac arrhythmias and syncope, significantly impacting the patient's quality of life. The incidence of GPN is low, and there is limited clinical awareness and understanding of the condition, leading to a high rate of misdiagnosis. In recent years, pulsed radiofrequency has emerged as an effective and minimally invasive treatment modality for the management of GPN. We report a case of a 56-year-old male patient with recurrent glossopharyngeal neuralgia accompanied by syncope. The patient tested positive for the topical application of local anesthetics, and cranial nerve magnetic resonance imaging (MRI) revealed compression of the right glossopharyngeal nerve by a small blood vessel. Both 24-hour Holter monitoring and video electroencephalography (EEG) showed no abnormalities. In addition to treatment with carbamazepine and pregabalin, the patient's pain as well as syncope resolved after two sessions of CT (ComputedTomography)-guided pulsed radiofrequency (PRF) therapy of the glossopharyngeal nerve. Clinicians should be aware of the rare clinical occurrence of glossopharyngeal neuralgia with syncope. PRF is a measure of safe and effective which could be considered the first choice for minimally invasive therapy.
| Published in | International Journal of Medical Case Reports (Volume 3, Issue 2) |
| DOI | 10.11648/j.ijmcr.20240302.12 |
| Page(s) | 18-21 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Glossopharyngeal Neuralgia, Syncope, Pulsed Radiofrequency
GPN | Glossopharyngeal Neuralgia |
PRF | Pulsed Radiofrequency |
MRI | Magnetic Resonance Imaging |
EEG | Electroencephalography |
AICA | Anterior Inferior Cerebellar Artery |
CT | Computed Tomography |
| [1] | Harris W. Persistent pain in lesions of the peripheral and central nervous system. Br Med J. 1921 Nov 26; 2(3178): 896-900. |
| [2] | Van Hecke O, Austin SK, Khan RA, et al. Neuropathic pain in the general population: a systematic review of epidemiological studies. Pain. 2014 Apr; 155(4): 654-662. |
| [3] | Takaya N, Sumiyoshi M, Nakata Y. Prolonged cardiac arrest caused by glossopharyngeal neuralgia. Heart. 2003 Apr; 89(4): 381. |
| [4] | Naeem A, Adelman EE. Glossopharyngeal Neuralgia Associated With Bradycardia and syncope-a Case Report. Neurohospitalist. 2022 Jul; 12(3): 553-555. |
| [5] | Robertson C. Cranial Neuralgias. Continuum (Minneap Minn). 2021 Jun 1; 27(3): 665-685. |
| [6] | Guan Xiaoxue, Yang Jun. A Case Report of Glossopharyngeal Neuralgia Complicated by Recurrent Syncope Episodes. Journal of Neural Injury and Functional Reconstruction, 2021, 16(5): 308-310. |
| [7] | Amthor KF, Eide PK. Glossopharygeal neuralgia. Tidsskr Nor Laegeforen, 2003 Dec 4; 123(23): 3381-3383. PMID: 14713973. |
| [8] | Reddy GD, Viswanathan A. Trigeminal and glossopharyngeal neuralgia. Neurol Clin. 2014 May; 32(2): 539-52. |
| [9] | Wang Xiaoqiang, Yin Wenjie, Tian Chuan, et al. Microvascular Decompression for the Treatment of Glossopharyngeal Neuralgia: A Report of 20 Cases. Chinese Journal of Minimally Invasive Surgery, 2022, 22(5). |
| [10] | Martínez-González JM, Martínez-Rodríguez N, Calvo-Guirado JL, et al. Glossopharyngeal neuralgia: a presentation of 14 cases. J Oral Maxillofac Surg. 2011 Jun; 69(6): e38-41. |
| [11] | Ma Y, Li YF, Wang QC, et al. Neurosurgical treatment of glossopharyngeal neuralgia: analysis of 103 cases. J Neurosurg. 2016 Apr; 124(4): 1088-92. |
| [12] | Cosman ER Jr, Cosman ER Sr. Electric and thermal field effects in tissue around radiofrequency electrodes. Pain Med. 2005 Nov-Dec; 6(6): 405-24. |
| [13] | Song L, He L, Pei Q, et al. CT-guided percutaneous radiofrequency thermocoagulation for glossopharyngeal neuralgia: A retrospective clinical study of 117 cases. Clin Neurol Neurosurg. 2019 Mar; 178: 42-45. |
| [14] | Erdine S, Yucel A, Cimen A, et al. Effects of pulsed versus conventional radiofrequency current on rabbit dorsal root ganglion morphology. Eur J Pain. 2005 Jun; 9(3): 251-6. |
| [15] | Zhang W, He C. Clinical Efficacy of Pulsed Radiofrequency Combined with Intravenous Lidocaine Infusion in the Treatment of Subacute Herpes Zoster Neuralgia. Pain Res Manag. 2022 Apr 11; 2022: 5299753. |
APA Style
Jia, W., Xiaoqian, Y., Jun, L. (2024). Case Report: Radiofrequency Pulsed Therapy for Glossopharyngeal Neuralgia with Associated Syncope. International Journal of Medical Case Reports, 3(2), 18-21. https://doi.org/10.11648/j.ijmcr.20240302.12
ACS Style
Jia, W.; Xiaoqian, Y.; Jun, L. Case Report: Radiofrequency Pulsed Therapy for Glossopharyngeal Neuralgia with Associated Syncope. Int. J. Med. Case Rep. 2024, 3(2), 18-21. doi: 10.11648/j.ijmcr.20240302.12
AMA Style
Jia W, Xiaoqian Y, Jun L. Case Report: Radiofrequency Pulsed Therapy for Glossopharyngeal Neuralgia with Associated Syncope. Int J Med Case Rep. 2024;3(2):18-21. doi: 10.11648/j.ijmcr.20240302.12
@article{10.11648/j.ijmcr.20240302.12,
author = {Wang Jia and Yu Xiaoqian and Li Jun},
title = {Case Report: Radiofrequency Pulsed Therapy for Glossopharyngeal Neuralgia with Associated Syncope
},
journal = {International Journal of Medical Case Reports},
volume = {3},
number = {2},
pages = {18-21},
doi = {10.11648/j.ijmcr.20240302.12},
url = {https://doi.org/10.11648/j.ijmcr.20240302.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmcr.20240302.12},
abstract = {Glossopharyngeal neuralgia (GPN) is characterized by paroxysmal, severe, and lancinating pain at the base of the tongue and throat on one side, often radiating to the oropharynx or ear. The intensity of the pain can be debilitating and, in severe cases, may be accompanied by potentially life-threatening conditions such as cardiac arrhythmias and syncope, significantly impacting the patient's quality of life. The incidence of GPN is low, and there is limited clinical awareness and understanding of the condition, leading to a high rate of misdiagnosis. In recent years, pulsed radiofrequency has emerged as an effective and minimally invasive treatment modality for the management of GPN. We report a case of a 56-year-old male patient with recurrent glossopharyngeal neuralgia accompanied by syncope. The patient tested positive for the topical application of local anesthetics, and cranial nerve magnetic resonance imaging (MRI) revealed compression of the right glossopharyngeal nerve by a small blood vessel. Both 24-hour Holter monitoring and video electroencephalography (EEG) showed no abnormalities. In addition to treatment with carbamazepine and pregabalin, the patient's pain as well as syncope resolved after two sessions of CT (ComputedTomography)-guided pulsed radiofrequency (PRF) therapy of the glossopharyngeal nerve. Clinicians should be aware of the rare clinical occurrence of glossopharyngeal neuralgia with syncope. PRF is a measure of safe and effective which could be considered the first choice for minimally invasive therapy.
},
year = {2024}
}
TY - JOUR T1 - Case Report: Radiofrequency Pulsed Therapy for Glossopharyngeal Neuralgia with Associated Syncope AU - Wang Jia AU - Yu Xiaoqian AU - Li Jun Y1 - 2024/08/15 PY - 2024 N1 - https://doi.org/10.11648/j.ijmcr.20240302.12 DO - 10.11648/j.ijmcr.20240302.12 T2 - International Journal of Medical Case Reports JF - International Journal of Medical Case Reports JO - International Journal of Medical Case Reports SP - 18 EP - 21 PB - Science Publishing Group SN - 2994-7049 UR - https://doi.org/10.11648/j.ijmcr.20240302.12 AB - Glossopharyngeal neuralgia (GPN) is characterized by paroxysmal, severe, and lancinating pain at the base of the tongue and throat on one side, often radiating to the oropharynx or ear. The intensity of the pain can be debilitating and, in severe cases, may be accompanied by potentially life-threatening conditions such as cardiac arrhythmias and syncope, significantly impacting the patient's quality of life. The incidence of GPN is low, and there is limited clinical awareness and understanding of the condition, leading to a high rate of misdiagnosis. In recent years, pulsed radiofrequency has emerged as an effective and minimally invasive treatment modality for the management of GPN. We report a case of a 56-year-old male patient with recurrent glossopharyngeal neuralgia accompanied by syncope. The patient tested positive for the topical application of local anesthetics, and cranial nerve magnetic resonance imaging (MRI) revealed compression of the right glossopharyngeal nerve by a small blood vessel. Both 24-hour Holter monitoring and video electroencephalography (EEG) showed no abnormalities. In addition to treatment with carbamazepine and pregabalin, the patient's pain as well as syncope resolved after two sessions of CT (ComputedTomography)-guided pulsed radiofrequency (PRF) therapy of the glossopharyngeal nerve. Clinicians should be aware of the rare clinical occurrence of glossopharyngeal neuralgia with syncope. PRF is a measure of safe and effective which could be considered the first choice for minimally invasive therapy. VL - 3 IS - 2 ER -
Department of Pain Management, West China Hospital, Sichuan University, Chengdu, China
Department of Pain Management, West China Hospital, Sichuan University, Chengdu, China
Department of Pain Management, West China Hospital, Sichuan University, Chengdu, China
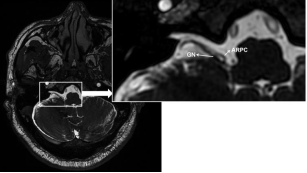
Figure 1. Magnetic resonance cranial nerve hydrography revealed that the right glossopharyngeal nerve was closely adhered to and compressed by the anterior inferior cerebellar artery (AICA).

Figure 2. Under CT guidance, the radiofrequency needle was advanced near the middle segment of the styloid process. Pulsed radiofrequency treatment was initiated after inducing abnormal sensations in the area supplied by the glossopharyngeal nerve.
Information

