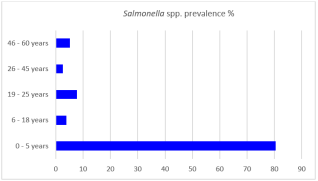
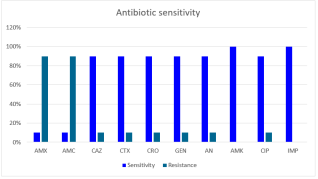
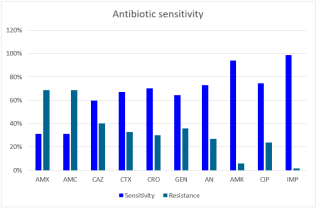
Background: Salmonella spp. are leading causes of gastroenteritis and typhoid fever worldwide, with hospital-acquired infections posing significant clinical challenges. The emergence of antibiotic resistance among clinical isolates has been increasingly recognized as a major contributor to treatment failure in affected patients. Objective: This study aimed to determine the prevalence and antimicrobial resistance patterns of Salmonella spp. isolated from clinical specimens at the National Hospital of Niamey, Niger. Method: Stool and blood samples were collected from patients presenting with clinical signs of enteric fever or gastroenteritis. Salmonella spp. was identified via standard microbiological methods, and antimicrobial susceptibility testing was performed via the disk diffusion method on Mueller‒Hinton agar in accordance with Clinical and Laboratory Standards Institute (CLSI) guidelines. Extended-spectrum beta-lactamase (ESBL) production was confirmed by a double-disk synergy test, which assessed the enhancement of inhibition zones between amoxicillin/clavulanic acid and third-generation cephalosporins. Results: Seventy-seven Salmonella isolates were recovered, yielding an overall prevalence of 2.55%. The majority of the isolates (80.52%) were obtained from children under 5 years of age. High resistance rates were observed against amoxicillin and amoxicillin/clavulanic acid (79% each). Multidrug resistance (resistance to ≥3 antibiotic classes) was detected in 25.97% of the isolates, whereas 35% were resistant to at least two antibiotics. Notably, 5.19% of the isolates were confirmed as ESBL-producing strains. Conclusion: These findings highlight the significant burden of multidrug-resistant Salmonella spp., including ESBL producers, in the clinical setting of Niamey. The high prevalence of resistance to commonly used antibiotics underscores the urgent need for enhanced antimicrobial resistance surveillance, rational antibiotic use, and infection control strategies to curb the spread of resistant strains in healthcare and community environments.
| Published in | International Journal of Microbiology and Biotechnology (Volume 11, Issue 2) |
| DOI | 10.11648/j.ijmb.20261102.14 |
| Page(s) | 76-84 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Salmonella spp., Clinical Isolates, Antimicrobial Resistance, Multidrug Resistance, Extended-spectrum Beta-lactamases (ESBL), Niger
Sample types | Sample numbers | Salmonella spp. prevalence% (n) |
|---|---|---|
Stool samples | 2,837 | 2.22 (60) |
Blood samples | 187 | 5.35 (10) |
Total | 3,024 | 2.55 (77) |
Samples origin | Salmonella spp. prevalence% (n) |
|---|---|
Pediatrics A office | 23.38 (18) |
Pediatrics B office | 1.30 (1) |
Pediatric referral office | 31.17 (24) |
Medicine B office | 3.90 (3) |
External | 40.26 (31) |
Number of resistant antibiotics | Resistance of Salmonella spp% (n) |
|---|---|
10 | 1.30 (1) |
9 | 2.60 (2) |
8 | 12.99 (10) |
7 | 3.90 (3) |
6 | 3.90 (3) |
5 | 1.30 (1) |
4 | 2.60 (2) |
3 | 9.09 (7) |
2 | 35.06 (27) |
1 | 6.49 (5) |
Samples types | MDR Salmonella spp. | Salmonella spp. ESBL |
|---|---|---|
Stool samples | 24.67% (19) | 5.19% (4) |
Blood samples | 1.30% (1) | 0.00% (0) |
Total | 25.97% (20) | 5.19% (4) |
AMR | Antimicrobial Resistance |
MDR | Multidrug Resistance |
ESBL | Extended-Spectrum Beta-Lactamase |
CLSI | Clinical and Laboratory Standards Institute |
CA-SFM | Antibiogram Committee of the French Society for Microbiology |
DDST | Double-Disk Synergy Test |
API 20E | Analytical Profile Index 20 Enterobacteriaceae |
SFM | French Society for Microbiology |
EUCAST | European Committee on Antimicrobial Susceptibility Testing |
LaBESTA | Laboratory of Molecular Biology, Epidemiology and Surveillance of Foodborne Bacteria and Viruses |
NNH | Niamey National Hospital |
GRH | General Reference Hospital |
| [1] | Ghoddusi, A., Nayeri Fasaei, B., Zahraei Salehi, T., & Akbarein, H. Serotype distribution and antimicrobial resistance of Salmonella isolate in human, chicken, and cattle in Iran. Archives of Razi Institute, 2019; 74(3), 259–266. |
| [2] | Chaudhari, R., Singh, K., & Kodgire, P. Biochemical and molecular mechanisms of antibiotic resistance in Salmonella spp. Research in Microbiology, 2023; 174(1–2), 103985. |
| [3] | Shu-kee, E., Priyia, P., Nurul-Syakima, A. B. M., Hooi-leng, S., Kok-Gang, C., & Learn-Han, L. Salmonella: A review on pathogenesis, epidemiology and antibiotic resistance. Frontiers in Life Science, 2015; 8(3), 284–293. |
| [4] | WHO (World Health Organization). Typhoid fever and other invasive salmonellosis. WHO Surveillance Standards, 2018. |
| [5] | Post, A. S., Diallo, S. N., Guiraud, I., Lompo, P., Tahita, M. C., Maltha, J., & Jacobs, J. Supporting evidence for a human reservoir of invasive non-Typhoidal Salmonella from household samples in Burkina Faso. PLoS Neglected Tropical Diseases, 2019; 13(10), e0007782. |
| [6] | Murray, C. J., Ikuta, K. S., Sharara, F., Swetschinski, L., Aguilar, G. R., Gray, A., & Tasak, N. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. The Lancet, 2022; 399(10325), 629–655. |
| [7] | WHO, FAO, OIE, UN. Antimicrobial Resistance and the United Nations Sustainable Development Cooperation Framework. Geneva: WHO, 2021. |
| [8] | Bonilla-Caballero, M. A., Lozano-Puentes, M. P., Ospina, M. A., & Varón-López, M. First report of multidrug-resistant Salmonella Infantis in broiler litter in Tolima, Colombia. Veterinary World, 2022; 15(6), 1557–1562. |
| [9] | Konaté, A., Guessennd, N. K., Kouadio, F. K., Dembélé, R., Kagambèga, A., et al. Epidemiology and Resistance Phenotypes of Salmonella spp. Strains Responsible for Gastroenteritis in Children Less Than Five Years of Age in Ouagadougou, Burkina Faso. Archives of Clinical Microbiology, 2019; 10(2), 90. |
| [10] | Illa, M., Diallo, B. A., Sani, O., Bassira, I., Abdoulaye, O., & Eric, A. Antibiotic resistance of Salmonella and Shigella, isolated from diarrheal children under five years old at the national hospital of Niamey (Niger). European Journal of Pharmaceutical and Medical Research, 2022; 9(8), 558–564. |
| [11] |
Food and Drug Administration. (2007). Salmonella (Chapter 5). In Bacteriological analytical manual.
https://www.fda.gov/food/laboratory-methods-food/bam-chapter-5-salmonella |
| [12] |
Clinical and Laboratory Standards Institute. Principles and Procedures for Blood Cultures; Approved Guideline. CLSI document M47-A. Wayne, PA: Clinical and Laboratory Standards Institute; 2007.
https://clsi.org/standards/products/microbiology/documents/m47/ |
| [13] | Biomerieux. (n.d.). API 20E instructions for use (REF 20100). Marcy-l'Étoile, France: biomerieux SA. Accessed on |
| [14] | Antibiogram Committee of the French Society for Microbiology (CA-SFM/EUCAST). Recommandations V1.0 Mars 2017. Paris: SFM, 2017. |
| [15] | Kariuki, S., Mbae, C., Onsare, R., Kavai, S. M., Wairimu, C., Ngetich, R., & Dougan, G. Multidrug-resistant nontyphoidal Salmonella hotspots as targets for vaccine use in management of infections in endemic settings. Clinical Infectious Diseases, 2019; 68(Suppl 1), S10–S16. |
| [16] | Bouda, S. C., Kagambega, A., Bonifait, L., Le Gall, F., Ibrahim, H. B., Bako, E., & Barro, N. Prevalence and Antimicrobial Resistance of Salmonella enterica Isolated from Chicken and Guinea Fowl in Burkina Faso. International Journal of Microbiology and Biotechnology, 2019; 4(3), 64–71. |
| [17] | Dembele R., Konate, A., Soulama, I., Kagambèga, A., Kabore, W. A. D., &Cisse, H. Prevalence of Multidrug-resistant Salmonella enterica and associated factors among under five children with diarrhea in rural Burkina Faso. Clinical and Biotechnology Microbiology, 2018; 3(1), 566–576. |
| [18] | Maharjan, A., Dhungel, B., Bastola, A., Thapa Shrestha, U., Adhikari, N., Banjara, M. R., & Rijal, K. R. Antimicrobial susceptibility pattern of Salmonella spp. isolated from enteric fever patients in Nepal. Infectious Disease Reports, 2021; 13(2), 388–400. |
| [19] | Ngogo, F. A., Abade, A. M., Rumisha, S. F., Mizinduko, M. M., & Majigo, M. V. Factors associated with Salmonella infection in patients with gastrointestinal complaints seeking health care at Regional Hospital in Southern Highland of Tanzania. BMC Infectious Diseases, 2020; 20(1), 1–8. |
| [20] | Harb, A., Abraham, S., Rusdi, B., Laird, T., O’dea, M., & Habib, I. Molecular detection and epidemiological features of selected bacterial, viral, and parasitic enteropathogens in stool specimens from children with acute diarrhea in Thi-Qar Governorate, Iraq. International Journal of Environmental Research and Public Health, 2019; 16(9), 1573. |
| [21] | Kashosi, T. M., Muhandule, A. B., Mwenebitu, D. L., Mihuhi, N., Mutendela, J. K., & Mubagwa, K. Antimicrobial resistance of Salmonella spp. strains isolated from blood cultures in Bukavu, DR Congo. Pan African Medical Journal, 2018; 29(1), 1–8. |
| [22] | Akinkunmi, F., Ajoseh, S., Fakorede, C., Abegunrin, R., Salami, W., Lawal, A., & Akinyemi, K. Prevalence of Salmonella blood-stream infection and antimicrobial resistance in Lagos, Nigeria. Infection Epidemiology and Microbiology, 2023; 9(1), 0-0. |
| [23] | Bastola, A., Pyakurel, P., Rayamajhi, R. B., Shrestha, S., Thekkur, P., Pandey, B., & Edwards, J. K. High Resistance of Salmonella spp. In addition, Shigella spp. in Blood and Stool Cultures from the Sukraraj Tropical and Infectious Disease Hospital, Kathmandu, Nepal, 2015–2019. Tropical Medicine and Infectious Disease, 2021; 6(2), 59. |
| [24] | Ndip, R., Awah, L., Ghogomu, S., Cho-Ngwa, F., & Ngemenya, M. Isolation and molecular identification of Salmonella with high multidrug resistance to first line typhoid antibiotics in Southwest Cameroon. Microbes and Infectious Diseases, 2022; 3(4), 988–997. |
| [25] | Diarra, B., Guindo, I., Koné, B., Dembélé, M., Cissé, I., Thiam, S., & Djimde, A. High frequency of antimicrobial resistance in Salmonella and Escherichia coli causing diarrheal diseases at the Yirimadio community health facility, Mali. BMC Microbiology, 2024; 24(1), 35. |
| [26] | Hugho, E. A., Kumburu, H. H., Thomas, K., Lukambagire, A. S., Wadugu, B., Amani, N., & Mmbaga, B. T. High diversity of Salmonella spp. from children with diarrhea, food, and environmental sources in Kilimanjaro–Tanzania: one health approach. Frontiers in Microbiology, 2024; 14, 1277019. |
| [27] | Abbasi, E., & Ghaznavi-Rad, E. Quinolone resistant Salmonella species isolated from pediatric patients with diarrhea in central Iran. BMC Gastroenterology, 2021; 21, 1–6. |
| [28] | Mina, S. A., Hasan, M. Z., Hossain, A. Z., Barua, A., Mirjada, M. R., & Chowdhury, A. M. A. The prevalence of multidrug-resistant Salmonella typhi isolated from blood sample. Microbiology Insights, 2023; 16, 11786361221150760. |
| [29] | Zaki, S. A., & Karande, S. Multidrug-resistant typhoid fever: a review. Journal of Infection in Developing Countries, 2011; 5(5), 324–337. |
| [30] | Ramatla, T., Khasapane, N. G., Mlangeni, L. N., Mokgokong, P., Ramaili, T., Ndou, R., & Thekisoe, O. Detection of Salmonella Pathogenicity Islands and Antimicrobial Resistance Genes in Salmonella enterica Serovars Enteritidis and Typhimurium Isolated from Broiler Chickens. Antibiotics, 2024; 13(5), 458. |
| [31] | Amare, A., Eshetie, S., Kasew, D., Amare, A., Abebe, W., & Moges, F. Prevalence of Salmonella spp., Shigella spp., and intestinal parasites among food handlers working in University of Gondar student’s cafeteria, Northwest Ethiopia. Frontiers in Public Health, 2024; 12. |
| [32] | Primeau, C. A., Bharat, A., Janecko, N., Carson, C. A., Mulvey, M., Reid-Smith, R., & Parmley, E. J. Integrated surveillance of extended-spectrum beta-lactamase (ESBL)-producing Salmonella and Escherichia coli from humans and animal species raised for human consumption in Canada from 2012 to 2017. Epidemiology and Infection, 2023; 151, e14. |
| [33] | Saechue, B., Atwill, E. R., & Jeamsripong, S. Occurrence and molecular characteristics of antimicrobial resistance, virulence factors, and extended-spectrum β-lactamase (ESBL) producing Salmonella enterica and Escherichia coli isolated from the retail produce commodities in Bangkok, Thailand. Heliyon, 2024; 10(5), e29345. |
| [34] | Akinyemi, K. O., Al-Khafaji, N. S., Al-Alaq, F. T., Fakorede, C. O., Al-Dahmoshi, H. O., Iwalokun, B. A., & Saki, M. Extended-spectrum beta-lactamases encoding genes among Salmonella enterica serovar Typhi isolates in patients with typhoid fever from four academic medical centers in Lagos, Nigeria. Revista de Investigación Clínica, 2022; 74(3), 165–171. |
| [35] | Goravey, W., Tsui, C. K., Ali, G. A., Najim, M. S., Shunnar, K., Ibrahim, E. B., & Hadi, H. A. Clinical, phenotypic, and genotypic characteristics of ESBL-producing Salmonella enterica bloodstream infections from Qatar. IJID Regions, 2024; 11, 100368. |
APA Style
Fody, A. M., Yaou, C., Bawa, H. I., Boubou, L., Halawen, M. A., et al. (2026). Antimicrobial Resistance Profiles of Salmonella spp. Isolated from Clinical Samples in Niamey, Niger. International Journal of Microbiology and Biotechnology, 11(2), 76-84. https://doi.org/10.11648/j.ijmb.20261102.14
ACS Style
Fody, A. M.; Yaou, C.; Bawa, H. I.; Boubou, L.; Halawen, M. A., et al. Antimicrobial Resistance Profiles of Salmonella spp. Isolated from Clinical Samples in Niamey, Niger. Int. J. Microbiol. Biotechnol. 2026, 11(2), 76-84. doi: 10.11648/j.ijmb.20261102.14
@article{10.11648/j.ijmb.20261102.14,
author = {Alio Mahamadou Fody and Chaibou Yaou and Hadiza Ibrahim Bawa and Laouali Boubou and Mohamed Alassane Halawen and Ramatou Sidikou and Hassimi Sadou and Nicolas Barro},
title = {Antimicrobial Resistance Profiles of Salmonella spp. Isolated from Clinical Samples in Niamey, Niger},
journal = {International Journal of Microbiology and Biotechnology},
volume = {11},
number = {2},
pages = {76-84},
doi = {10.11648/j.ijmb.20261102.14},
url = {https://doi.org/10.11648/j.ijmb.20261102.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmb.20261102.14},
abstract = {Background: Salmonella spp. are leading causes of gastroenteritis and typhoid fever worldwide, with hospital-acquired infections posing significant clinical challenges. The emergence of antibiotic resistance among clinical isolates has been increasingly recognized as a major contributor to treatment failure in affected patients. Objective: This study aimed to determine the prevalence and antimicrobial resistance patterns of Salmonella spp. isolated from clinical specimens at the National Hospital of Niamey, Niger. Method: Stool and blood samples were collected from patients presenting with clinical signs of enteric fever or gastroenteritis. Salmonella spp. was identified via standard microbiological methods, and antimicrobial susceptibility testing was performed via the disk diffusion method on Mueller‒Hinton agar in accordance with Clinical and Laboratory Standards Institute (CLSI) guidelines. Extended-spectrum beta-lactamase (ESBL) production was confirmed by a double-disk synergy test, which assessed the enhancement of inhibition zones between amoxicillin/clavulanic acid and third-generation cephalosporins. Results: Seventy-seven Salmonella isolates were recovered, yielding an overall prevalence of 2.55%. The majority of the isolates (80.52%) were obtained from children under 5 years of age. High resistance rates were observed against amoxicillin and amoxicillin/clavulanic acid (79% each). Multidrug resistance (resistance to ≥3 antibiotic classes) was detected in 25.97% of the isolates, whereas 35% were resistant to at least two antibiotics. Notably, 5.19% of the isolates were confirmed as ESBL-producing strains. Conclusion: These findings highlight the significant burden of multidrug-resistant Salmonella spp., including ESBL producers, in the clinical setting of Niamey. The high prevalence of resistance to commonly used antibiotics underscores the urgent need for enhanced antimicrobial resistance surveillance, rational antibiotic use, and infection control strategies to curb the spread of resistant strains in healthcare and community environments.},
year = {2026}
}
TY - JOUR T1 - Antimicrobial Resistance Profiles of Salmonella spp. Isolated from Clinical Samples in Niamey, Niger AU - Alio Mahamadou Fody AU - Chaibou Yaou AU - Hadiza Ibrahim Bawa AU - Laouali Boubou AU - Mohamed Alassane Halawen AU - Ramatou Sidikou AU - Hassimi Sadou AU - Nicolas Barro Y1 - 2026/06/26 PY - 2026 N1 - https://doi.org/10.11648/j.ijmb.20261102.14 DO - 10.11648/j.ijmb.20261102.14 T2 - International Journal of Microbiology and Biotechnology JF - International Journal of Microbiology and Biotechnology JO - International Journal of Microbiology and Biotechnology SP - 76 EP - 84 PB - Science Publishing Group SN - 2578-9686 UR - https://doi.org/10.11648/j.ijmb.20261102.14 AB - Background: Salmonella spp. are leading causes of gastroenteritis and typhoid fever worldwide, with hospital-acquired infections posing significant clinical challenges. The emergence of antibiotic resistance among clinical isolates has been increasingly recognized as a major contributor to treatment failure in affected patients. Objective: This study aimed to determine the prevalence and antimicrobial resistance patterns of Salmonella spp. isolated from clinical specimens at the National Hospital of Niamey, Niger. Method: Stool and blood samples were collected from patients presenting with clinical signs of enteric fever or gastroenteritis. Salmonella spp. was identified via standard microbiological methods, and antimicrobial susceptibility testing was performed via the disk diffusion method on Mueller‒Hinton agar in accordance with Clinical and Laboratory Standards Institute (CLSI) guidelines. Extended-spectrum beta-lactamase (ESBL) production was confirmed by a double-disk synergy test, which assessed the enhancement of inhibition zones between amoxicillin/clavulanic acid and third-generation cephalosporins. Results: Seventy-seven Salmonella isolates were recovered, yielding an overall prevalence of 2.55%. The majority of the isolates (80.52%) were obtained from children under 5 years of age. High resistance rates were observed against amoxicillin and amoxicillin/clavulanic acid (79% each). Multidrug resistance (resistance to ≥3 antibiotic classes) was detected in 25.97% of the isolates, whereas 35% were resistant to at least two antibiotics. Notably, 5.19% of the isolates were confirmed as ESBL-producing strains. Conclusion: These findings highlight the significant burden of multidrug-resistant Salmonella spp., including ESBL producers, in the clinical setting of Niamey. The high prevalence of resistance to commonly used antibiotics underscores the urgent need for enhanced antimicrobial resistance surveillance, rational antibiotic use, and infection control strategies to curb the spread of resistant strains in healthcare and community environments. VL - 11 IS - 2 ER -
Department of Life and Earth Sciences, Abdou Moumouni University, Niamey, Niger;Department of Life and Earth Sciences, Joseph Ki-Zerbo University, Ouagadougou, Burkina Faso;Department of Chemistry, Abdou Moumouni University, Niamey, Niger
Department of Chemistry, Abdou Moumouni University, Niamey, Niger
Department of Life and Earth Sciences, Ledea Bernard Ouedraogo University, Ouahigouya, Burkina Faso
Bacteriology Laboratory of Niamey National Hospital (NNH), Niamey, Niger
Microbiology Laboratory of the General Reference Hospital (GRH), Niamey, Niger
Department of Biology, Abdou Moumouni University, Niamey, Niger
Department of Chemistry, Abdou Moumouni University, Niamey, Niger
Department of Life and Earth Sciences, Joseph Ki-Zerbo University, Ouagadougou, Burkina Faso
Information