Platypnea-Orthodeoxia syndrome (POS), an exceptionally uncommon condition, is characterized by decreased oxygen saturation in an upright posture with corresponding improvement in the supine position. Recently, an 85-year-old female patient presented for surgery due to a left femoral neck fracture. Following successful tracheal intubation and anesthesia induction, the ventilator indicated an airway pressure of 15mmHg. While in the right lateral decubitus position, the patient developed hypoxia despite normal arterial blood pressure and symmetrical breath sounds. Attempts to alleviate the hypoxia through pure oxygen ventilation, tympanic lung ventilation, and high-frequency ventilation were unsuccessful. Subsequently, there was a notable decrease in both blood pressure and heart rate, prompting an immediate halt to the surgery and repositioning the patient to the supine position. This resulted in the normalization of the patient's heart rate, oxygen saturation, and blood pressure. To investigate the etiology, a TEE probe was inserted, revealing the presence of a patent foramen ovale (PFO) and a significant right-to-left shunt while the patient was in the lateral position. The procedure was performed in a specific right lateral decubitus position. This case may represent a unique manifestation of POS syndrome, expanding the differential diagnosis for intraoperative position-related hypoxemia. Given the severe hypoxemia observed with intraoperative positional changes, a strong suspicion of POS syndrome is warranted.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
. The most frequent cause of POS is patent foramen ovale (PFO)
[2]
Verdoia M, Viola O, et. al. Managing Congenital Heart Defects in Elderly: The Platypnea-Orthodeoxia Syndrome in Underestimated Patent Foramen Ovale. Angiology. 2023 Aug 31: 33197231199229.
. However, the PFO patients experienced very uncommon chronic hypoxemia while in the right lateral decubitus posture. As far as we are aware, previous cases were identified and managed using imaging and clinical signs of upright hypoxia
[3]
Sitbon S, Ou P, Nguyen C, et. al. Four-Dimensional Flow Magnetic Resonance Imaging Features of a Platypnea-Orthodeoxia Syndrome Caused by a Patent Foramen Ovale. Circ Cardiovasc Imaging. 2023 Jul; 16(7): 601-603.
. A considerable preoperative diagnostic hurdle is posed by extended bed rest. The diagnosis and treatment of severe intraoperative posture-related hypoxemia present a significant challenge. We provide a case of chronic intraoperative hypoxia in a patient who also had aortic root dilatation, coupled PFO, right mediastinum displacement, and aberrant liver positioning. Written informed consent was obtained from the patient for the publication of this case report.
2. Case Presentation
An 85-year-old woman was getting ready for surgery to repair a fall-related fracture to her left femoral neck. She had previously been diagnosed with hypertension, Meniere's disease, lumbar disc herniation, liver cirrhosis, kidney stones, and renal cysts. Upon physical examination, it was determined that she was 145 cm tall, weighed 40 kg, had a blood pressure of 159/59 mm Hg, breathed at a rate of 18 breaths per minute, and had a heart rate of 60 beats per minute. Both lungs produced slightly coarse breath sounds. No notable abnormalities were found in the preoperative laboratory tests. The lower lobes of both lungs were the focus of the general chest computed tomography (CT), which verified the presence of inflammation in both lungs. Moreover, it supported the mediastinum's right deviation. Transthoracic echocardiography revealed an enlarged left heart (Left ventricle LV 51 Left Atrium LA43); thickening of the basal segment of the ventricular septum (interventricular septum IVS=9-12); mild to moderate mitral regurgitation; decreased diastolic function (E/e'=18); and moderate to severe aortic valve regurgitation. A left-sided double-action artificial femoral head replacement was planned for the patient who had a left femoral neck fracture.
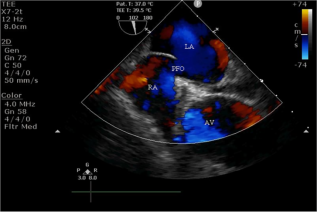
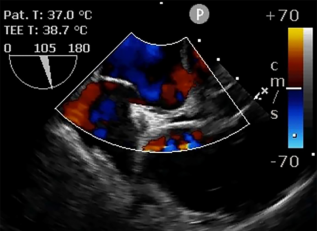
The patient was admitted to the operating room with an oxygen saturation of 92% on air, and breath sounds in both lungs were symmetrical but slightly coarse. Arterial blood gases showed a partial pressure of oxygen of 68 mmHg and PCO2 of 37 mmHg after invasive arterial blood pressure monitoring. During induction of anesthesia, 0.15 mg/kg cis-atracurium, 0.4 µg/kg sufentanil, and 0.2 mg/kg etomidate injection were administered. After successful intubation, the tidal volume of mechanical ventilation was 7 ml/kg, the airway pressure was 15 mmHg, the oxygen concentration was 50%, and no significant abnormalities were observed in the vital signs. After the right lateral decubitus position, the patient presented with sustained low oxygen saturation and normal arterial blood pressure which lasted up to 45 minutes. Arterial blood gas analysis suggested PO2 was 55.1mmHg, and SPO2 was sustained at the range of 82%-92%. In meanwhile, adjustment of oxygen concentration to 100%, intravenous hydrocortisone infusion, and changed to manual high-frequency ventilation were noneffective. During this period, systolic blood pressure was in the range of 123 to 153 mmHg, and diastolic blood pressure was in the range of 70 to 80 mmHg. However, it was effective to use ephedrine to raise the level of higher blood pressure which could elevate oxygen saturation. Suddenly, heart rate, oxygen saturation, and blood pressure decreased, the surgery was stopped immediately and the body position was changed to the supine position. The above management measures resulted in the patient's oxygen saturation rising to 100% and other vital signs returning to normal. TEE was checked in detail. (Figure 1). TEE suggested the presence of a large PFO and a left-to-right shunt in the supine position. At this point, the patient needed to close the wound, so the patient was tilted 30° to the right, and oxygen saturation remained at 100%. TEE suggested a small amount of right-to-left shunting in the PFO (Figure 2). In the right lateral decubitus position, the patient's oxygenation could not be maintained, so TEE was not performed.
Figure 1. Doppler image in the supine position. LA: Left Atrium; PFO: Patent foramen ovale; RA: Right Atrium; AV: Aortic Valve. Large left-to-right shunt through the PFO in the supine position.
Figure 2. Doppler image at 30 degrees tilt to the right. Right-to-left shunt in the PFO is observed.
When the patient was conscious, the tracheal tube was removed from the operating room. And arterial blood gas indicated PO2 49.9mmHg. When the patient was in the upright position in the general ward, the patient developed significant shortness of breath and no significant respiratory distress in the supine position. The patient was discharged from the hospital after 35 days.
3. Discussion
POS is a syndrome of hypoxia accompanied by postural changes. POS has no clear diagnostic criteria. Based on the literature review, possible criteria include: (1) decreased noninvasive oxygen saturation in the upright position and recovered in the supine position
; (2) Arterial PO2 was significantly lower in the upright position compared to the supine position
[5]
Hashimoto M, Okawa Y, et al. Platypnea-orthodeoxia syndrome combined with constrictive pericarditis after coronary artery bypass surgery. J Thorac Cardiovasc Surg. 2006; 132(5): 1225-1226.
However, cases of decreased oxygen saturation in the lateral recumbent position had also been reported and very few cases of intraoperative lateral hypoxia had been reported. In the present case, there was insufficient evidence of hypoxia in the upright position
[6]
Ribeiro R, Fialho I, et. al. Platypnea-Orthodeoxia Syndrome: A Case of Persistent Hypoxemia in an Elderly Patient. Circulation. 2021 Aug 3; 144(5): 395-398.
, but the mechanism of hypoxaemia in the lateral position may be similar to the upright position. We discuss the pathophysiology of this case in terms of POS pathophysiology.
The possible pathophysiological causes are intracardiac shunt (PFO, ASD, or atrial septal aneurysm (ASA) with fenestration), pulmonary diseases with ventilation/perfusion mismatch (High V/Q ratio, and low V/Q ratio
[7]
Kass M, Grocott HP, et al. Constellation of Stroke, Pulmonary Embolism, and Platypnea Orthodeoxia Syndrome: The Elusive Patent Foramen Ovale. JACC Cardiovasc Interv. 2021 Jul 26; 14(14): e165-e167.
Additionally, the possible pathophysiological cause is the right-to-left shunt due to PFO in the right lateral position. Due to the low diagnostic sensitivity of TTE for PFO as well as shunts, the prevalence of PFO observed by TTE contrast was reported to be lower than that observed by TEE (14.9% vs. 24.3%)
[8]
Koutroulou I, Tsivgoulis G, et al. Epidemiology of Patent Foramen Ovale in General Population and in Stroke Patients: A Narrative Review. Front Neurol. 2020 Apr 28; 11: 281.
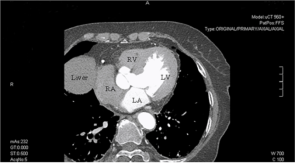
Figure 4. Preoperative imaging findings. Enhanced computed tomography (CT) scan. The right deviation of the mediastinum is suggested.
Factors without pulmonary hypertension that the right-to-left shunt include: (1) During positive pressure ventilation in the right lateral position, Intrathoracic positive pressure results in right heart compression, increased right atrial pressure, and appeared right-to-left shunt. Possible causes of right heart compression are short stature, diaphragm elevation, liver compression, and positive pressure ventilation
[9]
Othman F, Bailey B, et al. Platypnea-Orthodeoxia Syndrome in the Setting of Patent Foramen Ovale Without Pulmonary Hypertension or Major Lung Disease. J Am Heart Assoc. 2022 Aug 2; 11(15): e024609.
. From the CT mediastinal window, we can see the smaller right atrium and the compression of the right atrium by the liver (Figure 3). As well, the right deviation of the mediastinum was observed. (Figure 4) (2) Dilation of the aortic root may lead to a leftward shift of the interatrial septum, which may widen the gap in the PFO as well as provide for increased right atrial pressure, thereby increasing the right-to-left shunt
[10]
Agrawal A, Palkar A, et al. The multiple dimensions of Platypnea-Orthodeoxia syndrome: A review. Respir Med. 2017; 129: 31-38.
. We can see the dilated aortic root from the intraoperative TEE examination as well as the mediastinal window of the chest CT.
In the absence of pulmonary hypertension, PFO causes a left-to-right shunt due to higher left heart pressure than the right heart
[11]
Jung SY, Kim NK, et. al. Transcatheter treatment of atrial septal defect presenting with platypnea-orthodeoxia syndrome. Korean Circ J. 2015 Mar; 4 5(2): 169-73.
. In right de-cubitus, the liver was in full contact with the right atrium resulting which increased right heart pressure. The patient had no previous history of liver disease, but on CT the liver was found to be in close apposition to the right atrium, which may be associated with the right diaphragm elevation. A few case studies reported POS with hemidiaphragmatic elevation, especially triggered by hemidiaphragmatic paralysis
[12]
Neuvillers L, Masri A, et al. Platypnea-orthodeoxia syndrome: comprehensive analysis by multimodal imaging. Eur Heart J. 2021 Oct 7; 42(38): 3995.
. After the onset of muscle relaxants, the patient's diaphragm was relaxed and the postural pad elevated the relaxed diaphragm in the right lateral position. This may be the cause of diaphragm elevation in this case. Likewise, the above was aggravated by the rightward deviation of the mediastinum and aortic root dilation. In addition, smaller right atria were more likely to be compressed. These are why right heart pressure increases in the right lateral decubitus position and a right-to-left shunt occurs.
The strange phenomenon of reduced oxygen saturation but normal blood pressure occurred intraoperatively. This may be because a large amount of unoxygenated blood flow reached the left heart directly through the PFO, and the normal output of the left heart ensured normal blood pressure. After 45 minutes, prolonged hypoxia resulted in decreased cardiac pump function, decreased cardiac output, and a rapid drop in blood pressure.
During the patient's hypoxia, we tried to raise the blood pressure to a higher level using ephedrine, and oxygen saturation was briefly improved. Ephedrine has an α agonist effect, the pharmacological effect that causes pulmonary vasoconstriction and reduces intrapulmonary shunts as well as temporarily increasing left atrial pressure and reducing intracardiac right-to-left shunts. Successful reversal of right-to-left shunt to improve oxygen saturation has been reported in an elderly patient with POS using 5 μg/hr norepinephrine
[13]
Zhou J, He J, et al. Case report: Unusual cause of refractory hypoxemia after pacemaker lead extraction. Front Cardiovasc Med. 2023 Aug 14; 10: 1237595.
However, intracardiac shunts can only be resolved by PFO closure. PFO closure was rejected due to the patient's advanced age and good post-operative recovery
[15]
Shah AH, Osten M, et al. Percutaneous intervention to treat platypnea-orthodeoxia syndrome: the Toronto Experience. JACC Cardiovasc Interv. 2016; 9: 1928–1938.
This case is a severely underestimated PFO-associated POS syndrome. The diagnosis of intraoperative hypoxaemia was difficult due to the lack of sensitivity of preoperative TTE to PFO. PFO-related POS syndrome is highly suspected if position-related hypoxaemia is present intraoperatively. It was managed by changing the position as well as assisting the diagnosis by TEE.PFO as well as position was one of the causes of hypoxaemia, but some structural cardiac problems leading to enlarged patent foramen ovale in lateral position may have been overlooked. Subtle changes in cardiac structure in lateral recumbency may require more advanced investigations to realise.
Abbreviations
POS: Platypnea-Orthodeoxia
PFO: Patent Foramen Ovale
TEE: Transesophageal Echocardiography
TTE: Trans-Thoracic Echocardiography
CT: Chest Computed Tomography
ASA: Atrial Septal Aneurysm
LV: Left Ventricle
LA: Left Atrium
IVS: Interventricular Septum
Ethics Approval and Consent to Participate
All clinical practices were conducted by the principles of the Declaration of Helsinki.
Author Contributions
Guowei Wu: Writing - original draft, Visualization
Hongwei Xu: Writing - review & editing
Funding
This case report was not funded by any funding.
Data Availability Statement
The datasets are available from the corresponding author on request.
Conflicts of Interest
The authors declared that they have no competing interests.
References
[1]
Shiraishi Y, Hakuno D, et al. Platypnea-orthodeoxia syndrome due to PFO and aortic dilation. JACC Cardiovasc Imaging. 2012; 5(5): 570-571.
Verdoia M, Viola O, et. al. Managing Congenital Heart Defects in Elderly: The Platypnea-Orthodeoxia Syndrome in Underestimated Patent Foramen Ovale. Angiology. 2023 Aug 31: 33197231199229.
Sitbon S, Ou P, Nguyen C, et. al. Four-Dimensional Flow Magnetic Resonance Imaging Features of a Platypnea-Orthodeoxia Syndrome Caused by a Patent Foramen Ovale. Circ Cardiovasc Imaging. 2023 Jul; 16(7): 601-603.
Hashimoto M, Okawa Y, et al. Platypnea-orthodeoxia syndrome combined with constrictive pericarditis after coronary artery bypass surgery. J Thorac Cardiovasc Surg. 2006; 132(5): 1225-1226.
Ribeiro R, Fialho I, et. al. Platypnea-Orthodeoxia Syndrome: A Case of Persistent Hypoxemia in an Elderly Patient. Circulation. 2021 Aug 3; 144(5): 395-398.
Koutroulou I, Tsivgoulis G, et al. Epidemiology of Patent Foramen Ovale in General Population and in Stroke Patients: A Narrative Review. Front Neurol. 2020 Apr 28; 11: 281.
Othman F, Bailey B, et al. Platypnea-Orthodeoxia Syndrome in the Setting of Patent Foramen Ovale Without Pulmonary Hypertension or Major Lung Disease. J Am Heart Assoc. 2022 Aug 2; 11(15): e024609.
Jung SY, Kim NK, et. al. Transcatheter treatment of atrial septal defect presenting with platypnea-orthodeoxia syndrome. Korean Circ J. 2015 Mar; 4 5(2): 169-73.
Zhou J, He J, et al. Case report: Unusual cause of refractory hypoxemia after pacemaker lead extraction. Front Cardiovasc Med. 2023 Aug 14; 10: 1237595.
Shah AH, Osten M, et al. Percutaneous intervention to treat platypnea-orthodeoxia syndrome: the Toronto Experience. JACC Cardiovasc Interv. 2016; 9: 1928–1938.
Wu, G., Xu, H. (2024). Intraoperative Hypoxemia in the Right Lateral Decubitus Position: A Case Report. International Journal of Anesthesia and Clinical Medicine, 12(1), 33-37. https://doi.org/10.11648/j.ijacm.20241201.17
Wu, G.; Xu, H. Intraoperative Hypoxemia in the Right Lateral Decubitus Position: A Case Report. Int. J. Anesth. Clin. Med.2024, 12(1), 33-37. doi: 10.11648/j.ijacm.20241201.17
Wu G, Xu H. Intraoperative Hypoxemia in the Right Lateral Decubitus Position: A Case Report. Int J Anesth Clin Med. 2024;12(1):33-37. doi: 10.11648/j.ijacm.20241201.17
@article{10.11648/j.ijacm.20241201.17,
author = {Guowei Wu and Hongwei Xu},
title = {Intraoperative Hypoxemia in the Right Lateral Decubitus Position: A Case Report
},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {12},
number = {1},
pages = {33-37},
doi = {10.11648/j.ijacm.20241201.17},
url = {https://doi.org/10.11648/j.ijacm.20241201.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20241201.17},
abstract = {Platypnea-Orthodeoxia syndrome (POS), an exceptionally uncommon condition, is characterized by decreased oxygen saturation in an upright posture with corresponding improvement in the supine position. Recently, an 85-year-old female patient presented for surgery due to a left femoral neck fracture. Following successful tracheal intubation and anesthesia induction, the ventilator indicated an airway pressure of 15mmHg. While in the right lateral decubitus position, the patient developed hypoxia despite normal arterial blood pressure and symmetrical breath sounds. Attempts to alleviate the hypoxia through pure oxygen ventilation, tympanic lung ventilation, and high-frequency ventilation were unsuccessful. Subsequently, there was a notable decrease in both blood pressure and heart rate, prompting an immediate halt to the surgery and repositioning the patient to the supine position. This resulted in the normalization of the patient's heart rate, oxygen saturation, and blood pressure. To investigate the etiology, a TEE probe was inserted, revealing the presence of a patent foramen ovale (PFO) and a significant right-to-left shunt while the patient was in the lateral position. The procedure was performed in a specific right lateral decubitus position. This case may represent a unique manifestation of POS syndrome, expanding the differential diagnosis for intraoperative position-related hypoxemia. Given the severe hypoxemia observed with intraoperative positional changes, a strong suspicion of POS syndrome is warranted.
},
year = {2024}
}
TY - JOUR
T1 - Intraoperative Hypoxemia in the Right Lateral Decubitus Position: A Case Report
AU - Guowei Wu
AU - Hongwei Xu
Y1 - 2024/04/28
PY - 2024
N1 - https://doi.org/10.11648/j.ijacm.20241201.17
DO - 10.11648/j.ijacm.20241201.17
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 33
EP - 37
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20241201.17
AB - Platypnea-Orthodeoxia syndrome (POS), an exceptionally uncommon condition, is characterized by decreased oxygen saturation in an upright posture with corresponding improvement in the supine position. Recently, an 85-year-old female patient presented for surgery due to a left femoral neck fracture. Following successful tracheal intubation and anesthesia induction, the ventilator indicated an airway pressure of 15mmHg. While in the right lateral decubitus position, the patient developed hypoxia despite normal arterial blood pressure and symmetrical breath sounds. Attempts to alleviate the hypoxia through pure oxygen ventilation, tympanic lung ventilation, and high-frequency ventilation were unsuccessful. Subsequently, there was a notable decrease in both blood pressure and heart rate, prompting an immediate halt to the surgery and repositioning the patient to the supine position. This resulted in the normalization of the patient's heart rate, oxygen saturation, and blood pressure. To investigate the etiology, a TEE probe was inserted, revealing the presence of a patent foramen ovale (PFO) and a significant right-to-left shunt while the patient was in the lateral position. The procedure was performed in a specific right lateral decubitus position. This case may represent a unique manifestation of POS syndrome, expanding the differential diagnosis for intraoperative position-related hypoxemia. Given the severe hypoxemia observed with intraoperative positional changes, a strong suspicion of POS syndrome is warranted.
VL - 12
IS - 1
ER -
Wu, G., Xu, H. (2024). Intraoperative Hypoxemia in the Right Lateral Decubitus Position: A Case Report. International Journal of Anesthesia and Clinical Medicine, 12(1), 33-37. https://doi.org/10.11648/j.ijacm.20241201.17
Wu, G.; Xu, H. Intraoperative Hypoxemia in the Right Lateral Decubitus Position: A Case Report. Int. J. Anesth. Clin. Med.2024, 12(1), 33-37. doi: 10.11648/j.ijacm.20241201.17
Wu G, Xu H. Intraoperative Hypoxemia in the Right Lateral Decubitus Position: A Case Report. Int J Anesth Clin Med. 2024;12(1):33-37. doi: 10.11648/j.ijacm.20241201.17
@article{10.11648/j.ijacm.20241201.17,
author = {Guowei Wu and Hongwei Xu},
title = {Intraoperative Hypoxemia in the Right Lateral Decubitus Position: A Case Report
},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {12},
number = {1},
pages = {33-37},
doi = {10.11648/j.ijacm.20241201.17},
url = {https://doi.org/10.11648/j.ijacm.20241201.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20241201.17},
abstract = {Platypnea-Orthodeoxia syndrome (POS), an exceptionally uncommon condition, is characterized by decreased oxygen saturation in an upright posture with corresponding improvement in the supine position. Recently, an 85-year-old female patient presented for surgery due to a left femoral neck fracture. Following successful tracheal intubation and anesthesia induction, the ventilator indicated an airway pressure of 15mmHg. While in the right lateral decubitus position, the patient developed hypoxia despite normal arterial blood pressure and symmetrical breath sounds. Attempts to alleviate the hypoxia through pure oxygen ventilation, tympanic lung ventilation, and high-frequency ventilation were unsuccessful. Subsequently, there was a notable decrease in both blood pressure and heart rate, prompting an immediate halt to the surgery and repositioning the patient to the supine position. This resulted in the normalization of the patient's heart rate, oxygen saturation, and blood pressure. To investigate the etiology, a TEE probe was inserted, revealing the presence of a patent foramen ovale (PFO) and a significant right-to-left shunt while the patient was in the lateral position. The procedure was performed in a specific right lateral decubitus position. This case may represent a unique manifestation of POS syndrome, expanding the differential diagnosis for intraoperative position-related hypoxemia. Given the severe hypoxemia observed with intraoperative positional changes, a strong suspicion of POS syndrome is warranted.
},
year = {2024}
}
TY - JOUR
T1 - Intraoperative Hypoxemia in the Right Lateral Decubitus Position: A Case Report
AU - Guowei Wu
AU - Hongwei Xu
Y1 - 2024/04/28
PY - 2024
N1 - https://doi.org/10.11648/j.ijacm.20241201.17
DO - 10.11648/j.ijacm.20241201.17
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 33
EP - 37
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20241201.17
AB - Platypnea-Orthodeoxia syndrome (POS), an exceptionally uncommon condition, is characterized by decreased oxygen saturation in an upright posture with corresponding improvement in the supine position. Recently, an 85-year-old female patient presented for surgery due to a left femoral neck fracture. Following successful tracheal intubation and anesthesia induction, the ventilator indicated an airway pressure of 15mmHg. While in the right lateral decubitus position, the patient developed hypoxia despite normal arterial blood pressure and symmetrical breath sounds. Attempts to alleviate the hypoxia through pure oxygen ventilation, tympanic lung ventilation, and high-frequency ventilation were unsuccessful. Subsequently, there was a notable decrease in both blood pressure and heart rate, prompting an immediate halt to the surgery and repositioning the patient to the supine position. This resulted in the normalization of the patient's heart rate, oxygen saturation, and blood pressure. To investigate the etiology, a TEE probe was inserted, revealing the presence of a patent foramen ovale (PFO) and a significant right-to-left shunt while the patient was in the lateral position. The procedure was performed in a specific right lateral decubitus position. This case may represent a unique manifestation of POS syndrome, expanding the differential diagnosis for intraoperative position-related hypoxemia. Given the severe hypoxemia observed with intraoperative positional changes, a strong suspicion of POS syndrome is warranted.
VL - 12
IS - 1
ER -