Abstract
Improving health outcomes and lowering human immunodeficiency virus (HIV) transmission among people living with human immunodeficiency virus (PLHIV) requires achieving viral load suppression. In this study, people living with HIV in Zambia's Chingola District had their survival rates and factors related to viral suppression assessed. The research aimed at analysing factors associated with time to viral suppression among PLHIV in Chingola District using survival analysis. A retrospective cohort study design was used, utilising 385 clinical records of PLHIV in Chingola district, with the focus on 15 months period (January 2022 to April 2023). Cox proportional hazards regression models and Kaplan-Meier survival analysis were used as statistical techniques. The age group 50+ years accounted the highest proportion (45.5%), while 40–49 age group accounted for the least proportion (15.3%). Males dominated (56.6%) whereas 43.4% were females. The median time to attain viral suppression was 12 months. Consequently, frequent clinic visits significantly decreased suppression time (aHR = 2.026, p = 0.001), and PLHIV with comorbidity experienced faster viral suppression (aHR = 1.438, p = 0.017). None substance users had 1.392 times increased chances of achieving Viral load suppression higher than substance users (aHR = 1.392, p = 0.036). The intervention that increased the chance of suppression was case conferencing (aHR = 7.309, p = 0.001). The results highlighted how crucial it is to design interventions specifically for high-risk groups to enhance viral load results. Suggestions include implementing focused interventions for PLHIV with comorbidities and substance abusers, expanding case conferences, and fortifying adherence support networks.
|
Published in
|
World Journal of Public Health (Volume 10, Issue 4)
|
|
DOI
|
10.11648/j.wjph.20251004.19
|
|
Page(s)
|
524-531 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Adherence, HIV, Viral Load Suppression, Survival Analysis, Zambia
1. Introduction
Past research has demonstrated the global importance of antiretroviral therapy (ART) in attaining viral load control and suppression
| [1] | Boerma RS, Boender TS, Bussink AP, Calis JC, Bertagnolio S, Rinke de Wit TF, et al. Suboptimal viral suppression rates among HIV-infected children in low- and middle-income countries: a meta-analysis. AIDS. 2016; 30(15): 2305-14. |
| [2] | Byrd KK, Hou JG, Hazen R, Kirkham H, Suzuki S, Clay PG, et al. Antiretroviral adherence level necessary for HIV viral suppression using real-world data. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2019; 82(3): 245-51. |
[1, 2]
. In a worldwide setting, it was shown two decades ago by that longevity of viral load suppression with multi-drug ART over a three-year period
| [3] | Cochran WG. Sampling Techniques. 3rd ed. New York: Wiley; 1977. |
[3]
. According to literature the likelihood of viral load failure reduces with prolonged suppression, highlighting the significance of continued antiretroviral therapy
| [4] | Creswell JW, Creswell JD. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches. 5th ed. Thousand Oaks: Sage; 2018. |
[4]
.
Globally, HIV/AIDS continues to be a major public health concern, with sub-Saharan Africa suffering the most. In the region, there were over 25.6 million people with HIV as of 2021. The adult HIV prevalence rate of Zambia, which is situated in this high-prevalence area, is 11.1%
| [5] | Damulak PP, Ismail S, Abdul Manaf R, Mohd Said S, Agbaji O. Interventions to improve adherence to antiretroviral therapy (ART) in sub-Saharan Africa: An updated systematic review. International journal of environmental research and public health. 2021; 18(5): 2477. |
[5]
. The HIV management landscape in sub-Saharan Africa has changed significantly. High rates of viremia and resistance during first-line ART were discovered in earlier research conducted in South Africa, indicating early difficulties in ART treatment
| [6] | Dessie G, Wagnew F, Mulugeta H, Amare D, Jara D, Leshargie CT, et al. The effect of poor retention to care on virologic failure among people living with HIV/AIDS in Ethiopia: a systematic review and meta-analysis. AIDS Research and Therapy. 2020; 17: 45. |
| [7] | Desta AA, Woldearegay TW, Futwi N, Gebrehiwot GT, Gebru GG, Berhe AA, et al. HIV virological non-suppression and its associated factors in children on antiretroviral therapy at a major treatment centre in Southern Ethiopia: a cross-sectional study. BMC Infectious Diseases. 2019; 19: 60. |
[6, 7]
. While studies underscored the crucial significance of prompt retention in HIV care for the purpose of suppressing viral infection, promoting a test-and-treat strategy to enhance results in the area
| [8] | Hoffmann CJ, Charalambous S, Thio CL, Martin DJ, Pemba L, Fielding KL, et al. Hepatitis B virus infection and response to antiretroviral therapy (ART) in a South African ART program. Clinical Infectious Diseases. 2008; 47(11): 1479-85. |
[8]
.
Results from a meta-analysis found that HIV-infected children in low- and middle-income countries have inadequate viral suppression rates, underscoring the need for specialised therapy
| [9] | Ioannou P, Vouidaski E, Voulgaridi I, Karakonstantis S, Kofteridis D, Samonis G, et al. Frequency of clinic visits and HIV viral load suppression among people living with HIV: a simple clinical predictive model. AIDS Care. 2020; 32(5): 616-22. |
[9]
. The multidimensional character of viral load suppression in the region was illustrated by in Ethiopia, identified parameters linked with virological non-suppression, including socio-economic position and adherence levels
| [10] | Kanters S, Park JJ, Chan K, Socias ME, Ford N, Forrest JI, et al. Interventions to improve adherence to antiretroviral therapy: a systematic review and network meta-analysis. The Lancet HIV. 2017; 4(1): e31-e40. |
[10]
. The necessity for context-specific interventions to improve ART outcomes in sub-Saharan Africa is highlighted by these contemporary studies
| [11] | Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. Journal of the American Statistical Association. 1958; 53(282): 457-81. |
[11]
.
Although ART is widely accessible in Zambia, treatment outcomes are impacted by socioeconomic factors and discrepancies in healthcare access
| [12] | Kayukwa A, Butts SA, Barylski NA, Alcaide ML, Rodriguez VJ, Chitalu N, et al. HIV prevention among Zambian itinerant workers: challenges and solutions. Journal of health care for the poor and underserved. 2019; 30(1): 358-77. |
| [20] | Mulenga LB, Hines JZ, Stafford KA, Dzekedzeke K, Sivile S, Lindsay B, et al. A Comparison of 2016 and 2021 Population-Based HIV Impact Assessments in Zambia: Changes in HIV Prevalence, Incidence, and Viral Load Suppression. AIDS. 2022; 36(Suppl 1): S1-S9. |
[12, 20]
. Like many other places, Chingola District experiences particular difficulties, such as socioeconomic hurdles, limits in the healthcare infrastructure, and inconsistency in PLHIVs’ adherence to ART
| [13] | Kleinbaum DG, Klein M. Survival Analysis: A Self-Learning Text. 3rd ed. New York: Springer; 2012. |
| [14] | Lima VD, Harrigan R, Bangsberg DR, Hogg RS, Gross R, Yip B, et al. The combined effect of modern highly active antiretroviral therapy regimens and adherence on mortality over time. Journal of Infectious Diseases. 2010; 202(5): 750-9. |
[13, 14]
.
The HIV epidemic in Zambia offers special difficulties as well as chances for action. The influence of behavioural determinants on ART outcomes was highlighted by a previous study on HIV-infected injectable drug users, which demonstrated significant longitudinal changes in care participation and viral suppression
| [15] | Mesic A, Halim N, MacLeod W, Haker C, Mwansa M, Biemba G. Post handout/brand friends, Facilitators and barriers to adherence to antiretroviral therapy and retention in care among adolescents living with HIV/AIDS in Zambia: a mixed method study. AIDS and Behaviour. 2019; 23: 2618-28. |
[15]
. The difficulty of attaining long-term viral suppression in Zambia was highlighted by this preliminary study.
More thorough assessments have been presented by recent studies. Critical limitations in ART delivery and adherence were identified using a multistage-sampling-based technique to estimate retention and viral suppression rates
| [16] | Mills EJ, Lester R, Thorlund K, Lorenzi M, Muldoon K, Kanters S, et al. Interventions to promote adherence to antiretroviral therapy in Africa: a network meta-analysis. The Lancet HIV. 2014; 1(3): e104-11. |
[16]
. This is consistent with the findings of Byrd
et al., who highlighted the contribution of community-based interventions to increased viral suppression and adherence
| [17] | Ministry of Health Zambia. Zambia Population-Based HIV Impact Assessment (ZAMPHIA) 2016. Lusaka: Ministry of Health; 2019. |
[17]
. These recent studies emphasise how crucial it is to incorporate behavioural, clinical, and socioeconomic aspects into ART management plans in Zambia. Therefore, this research used survival analysis to pinpoint how demographic, clinical and behavioural factors related to the duration of viral load suppression, which can help improve public health initiatives in Zambia and other comparable settings.
2. Methods and Materials
2.1. Study Design
This was a retrospective cohort study that was conducted in selected health facilities [Chawama, Chiwempala, and Kabundi-East Clinic] of Chingola district in Zambia, which aimed at identifying factors influencing the time to viral suppression among PLHIV for 15 months between January 2022 to April 2023.
2.2. Study Population
The study population included all individuals who were HIV-infected and receiving ART in Chingola District selected health facilities, whose population remained unknown due to fluctuations in Smart Care but meet the inclusion criteria in the research
| [18] | Mody A, Sikazwe I, Czaicki N, Wa Mwanza M, Savory T, Sikombe K, et al. Estimating real-world impact of expanded eligibility for antiretroviral treatment: Evidence from a regression discontinuity design in Zambia. PLoS Medicine. 2018; 15(6): e1002574. |
| [19] | Mugavero MJ, Amico KR, Horn T, Thompson MA. The state of engagement in HIV care in the United States: from cascade to continuum to control. Clinical Infectious Diseases. 2013; 57(8): 1164-71. |
[18, 19]
.
2.3. Inclusion and Exclusion Criteria
The inclusion criteria comprised HIV-positive individuals aged 18 years and above who were initiated on ART and had at least one documented viral load result during the study period in selected Chingola facilities. Exclusion criteria included patients with incomplete records, transferred-out cases, and those without follow-up viral load data. Further, using the inclusion and exclusion criteria approach above, 385 patient records were utilised to ensure a comprehensive representation across the demographic and health statues from the clinical records of PLHIV in Chingola
| [21] | Musonda J. An Investigation on Factors causing Non-Adherence of Ant-Retro Viral Therapy (Art) among HIV Patients in Nchanga North General Hospital-Chingola, Zambia. Lusaka: University of Zambia; 2019. |
[21]
.
2.4. Data Analysis
The study population was described using descriptive statistics such as means, medians, percentages and frequencies. The data was collected from SmartCare. The predominant data source was medical records and patient registries due to their thorough and systematically documented nature. The variables were Demographic characteristics (age, sex, marital status, profession, residential area), Clinical parameters (initial viral load, CD4 count, type of ART regimen, presence of comorbidities such as tuberculosis or diabetes), Treatment history (date of ART initiation, patterns of adherence, missed appointments, changes in regimens), and Monitoring viral load calendars (e.g., time intervals between tests, suppression status, episodes of viral rebound).
Data analysis techniques included the use of survival analysis, cox proportional hazards regression using STATA/MP17 software packages
| [22] | Mwansa M, McLeod W, Halim N, Biemba G, Shiliya N, Mwanza A, et al. Below is a list of links to PEPFAR Materials and tools that you can use to view and search for various PEPFAR documents, guidelines, and publications. Washington: PEPFAR; 2017. |
[22]
, these methods were used to examine the time to viral load suppression and identify the significant predictors. This model was chosen for its abilities to handle censored data and simultaneously assess the impact of multiple covariates on survival time. The hazard function was expressed as:
h(t)=h0(t)exp(b1X1+b2X2+b3X3+…+bnXn)
The Kaplan-Meier technique was used to estimate survival functions, providing the probability of the individuals who were not viral suppressed over time
| [23] | Nance RM, Delaney JC, Simoni JM, Wilson IB, Mayer KH, Whitney BM, et al. Temporal trends in virologic suppression among HIV-infected individuals in care in the United States, 1997 to 2015: a cohort study. Annals of Internal Medicine. 2018; 169(6): 376-84. |
[23]
. This method accommodated censored data and allowing for a visual representation of the survival probabilities over time.
3. Results
3.1. Background and Descriptive Statistics
Table 1, the age distribution indicated that those aged 50 years and older accounted for the highest proportion of the interpreted age group (45.5%), suggesting that older people constitute a large proportion of the ART clientele population in Chingola District. In contrast, the 40–49 age group accounted for the least proportion (15.3%), suggesting potential differences in the HIV burden or healthcare-seeking behaviours that may exist across age cohorts. The gender distribution was male dominated (56.6%) with 43.4% being female.
Marital status was another salient characteristic, with 80.0% of patients entered as married, indicating a high rate of partner cohabitation among HIV-positive individuals. Conversely, the fewest participants were widowed (3.4%), possibly either simply owing to lower life expectancy among HIV-positive widows/widowers where they survive, and/or trends towards remarriage. In terms of economic stability, 45.5% of respondents were financially unstable while 54.5% were stable.
Table 1. Background and descriptive.
Background characteristics | Freq. | Percent |
Age | | |
20-29 | 78 | 20.3 |
30-39 | 73 | 19.0 |
40-49 | 59 | 15.3 |
50 and above | 175 | 45.5 |
Sex | | |
Female | 167 | 43.4 |
Male | 218 | 56.6 |
Marital status | | |
Never married | 40 | 10.4 |
Married | 308 | 80.0 |
Divorced | 24 | 6.2 |
Widowed | 13 | 3.4 |
Economic stability | | |
No | 175 | 45.5 |
Yes | 210 | 54.5 |
Total | 385 | 100 |
Table 2. Log-rank Test of survival estimate of time to viral load suppression by sex.
Sex | Observed events | Expected events | p-value |
Female | 91 | 91.6 | 0.9343 |
Male | 114 | 113.4 | |
3.2. Survival Function and Hazard Rate of Time to Viral Load Suppression Among HIV-infected Individuals
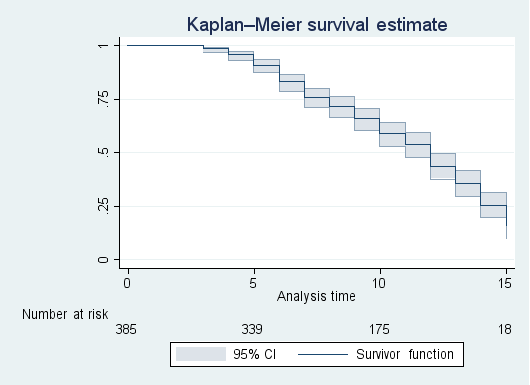
Figure 1 shows the Kaplan-Meier survival estimate for the time to viral load suppression in HIV patients. On median survival probability, half (50%) of the patients had their viral load suppressed by approximately end of 12 months after ART initiation. The small confidence intervals demonstrate the accuracy of survival estimates.
Figure 1. Kaplan-Meier survival estimate of time to viral suppression.
3.2.1. Survival Estimates of Time to Viral Load Suppression by Sex
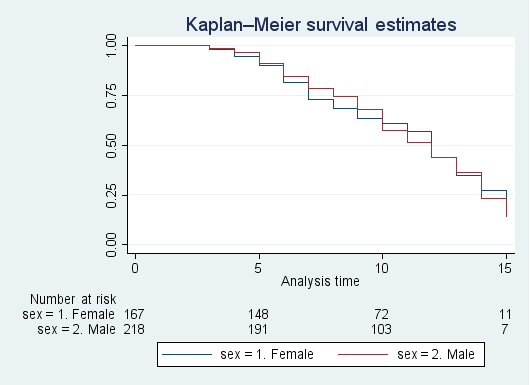
Figure 2 shows the Kaplan-Meier survival estimate of HIV patients' time to reduction in viral load of HIV by sex. Since the curves cross, it cannot be concluded which survival rate estimations were different. The log-rank test was performed to determine whether the survival function of time to viral load suppression is the same for males and females.
Figure 2. Kaplan-Meier survival estimate of time to viral suppression by sex.
3.2.2. Log-rank Test of Survival Estimate of Time to Viral Load Suppression by Sex
Table 2 indicates that the log-rank test results assessing time to viral load suppression for males and females fail to show statistical significance (
p = 0.9343). As such, patients’ sex does not statistically affect the longitudinality of the viral load to be suppressed, manifested by the fact that the survival function does not differ significantly across sexes.
3.3. Demographic, Clinical, and Behavioural Factors Associated with Shorter or Longer Time to Viral Load Suppression
The cox proportional hazards regression model of demographic, clinical and behavioural characteristics and the adjusted hazard ratios for time to viral load suppression are shown in
table 3 after adjustment for other model variables.
There was no significant association between age and the timing of viral load suppression. Older patients (30 – 39: aHR = 0.920, 40 – 49: aHR = 0.819, 50+: aHR = 0.783) had lower hazard ratios when compared to individuals aged 20-29. Sex did not significantly influence time to viral load suppression, with males having a hazard ratio of 0.972 (95% CI: 0.731–1.293, p = 0.847) compared to females. Further, marital status showed no significant association with time to viral load suppression. Compared to those who never married, married (aHR = 1.247, 95% CI: 0.755 - 2.062, p = 0.389), divorced (aHR = 0.952, 95% CI: 0.425 - 2.131, p = 0.904), and widowed patients (aHR = 1.005, 95% CI: 0.992 - 1.010, p = 0.991) had no statistically significant differences in viral load suppression rates.
Furthermore, economic stability was not significantly associated with time to viral load suppression. Patients who were economically stable had higher likelihood of viral load suppression compared to those who were not economically stable (aHR = 1.120, 95% CI: 0.840–1.493, p = 0.442). The health facility attended by the patient did not significantly influence time to viral load suppression. Patients at Chiwempala (aHR = 0.788, 95% CI: 0.553 - 1.123, p = 0.187) and Kabundi (aHR = 1.151, 95% CI: 0.804 - 1.648, p = 0.441) had lower hazard ratios and showed no statistically significant differences compared to those at Chawama health facility.
By ART regimen, the patients belonging to the 2nd line ART regimen were 1.151 times higher to have their viral load suppression (aHR = 1.151, 95% CI: 0.778–1.704, p = 0.482), compared to those in 1st line. However, the difference was not statically significant. Baseline viral load (aHR = 1.000, p = 0.516) and CD4 count (aHR = 1.000, p = 0.641) were not significantly associated with time to viral load suppression. Patients who had other diseases aside HIV had a significantly shorter time to viral load suppression (aHR = 1.438, 95% CI: 1.067–1.939, p = 0.017) compared to those who never had any other diseases.
Additionally, patients who frequently visited the clinic appointments were 2.026 times more likely have shorter time to viral load suppression, compared to those with less frequent visits (aHR = 2.026, 95% CI: 1.511–2.716, p < 0.001). Patients who reported no substance use had a significantly shorter time to viral suppression compared to substance users (aHR = 1.392, 95% CI: 1.022–1.895, p = 0.036). Patients with medium sexual activity had a significant slightly shorter time to viral suppression compared to those with high sexual activity (aHR = 1.090, 95% CI: 0.735–1.616, p = 0.036).
3.4. Effect of Interventions on Time to Viral Load Suppression Using Survival Analysis
The results in
table 4 of the Cox proportional hazards regression analysis show the effect of various interventions on the time to viral load suppression in individuals. The analysis state that case conferencing is reported to have resulted in a significant increase in the likelihood of viral load suppression compared to no meeting attendance for the case-conferencing participants (aHR = 7.309, 95% CI: 4.559–11.717,
P < 0.001).
The number of Enhanced Adherence Counselling (EAC) Sessions attended by the patient is not statistically significant on the time to viral load suppression (aHR = 1.001, 95% CI: 0.996-1.006, p = 0.634). Patients who do not know about HIV viral load have less, but not significant, likelihood of getting viral load suppression than knowledgeable patients (aHR = 0.780, 95% CI: 0.450-1.351, p = 0.375).
Membership in support groups does not affect time to viral load suppression significantly from being outside support groups (aHR = 0.973, 95% CI: 0.739-1.281, p = 0.844). Patients on nutritional support were less likely to be virally suppressed compared to those who did not receive nutritional support (aHR = 0.988, 95% CI: 0.747-1.306, p = 0.932).
4. Discussion
This study examined the time to viral suppression among people living with HIV (PLHIV) in Chingola District, Zambia using survival analysis techniques. The Median time from diagnosis to viral suppression was 12 months, with no significant sex difference between males and females, consistent with Kanters
et al. | [24] | Phillips AN, Staszewski S, Weber R, Kirk O, Francioli P, Miller V, et al. HIV viral load response to antiretroviral therapy according to the baseline CD4 cell count and viral load. BMJ. 2001; 322(7286): 289-93. |
[24]
finding of no differences by sex within Sub-Saharan Africa; Mills
et al. | [25] | Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. 9th ed. Philadelphia: Lippincott Williams & Wilkins; 2012. |
[25]
, because of their higher adherence, females suppress early. Sikazwe
et al. | [15] | Mesic A, Halim N, MacLeod W, Haker C, Mwansa M, Biemba G. Post handout/brand friends, Facilitators and barriers to adherence to antiretroviral therapy and retention in care among adolescents living with HIV/AIDS in Zambia: a mixed method study. AIDS and Behaviour. 2019; 23: 2618-28. |
[15]
who found that equal access to HIV care reduces gender disparities, though contrasting with
| [25] | Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. 9th ed. Philadelphia: Lippincott Williams & Wilkins; 2012. |
[25]
who found that women suppressed earlier due to higher adherence.
Cox proportional hazards regression showed no strong associations between demographic factors (age, sex, marital status, economic stability) and time to viral suppression, although a trend toward slower suppression with increasing age was noted, similar to Sikazwe
et al. | [15] | Mesic A, Halim N, MacLeod W, Haker C, Mwansa M, Biemba G. Post handout/brand friends, Facilitators and barriers to adherence to antiretroviral therapy and retention in care among adolescents living with HIV/AIDS in Zambia: a mixed method study. AIDS and Behaviour. 2019; 23: 2618-28. |
[15]
. Zhang
et al. | [26] | Sikazwe I, Eshun-Wilson I, Sikombe K, Czaicki N, Somwe P, Mody A, et al. Retention and viral suppression in a cohort of HIV patients on antiretroviral therapy in Zambia: Regionally representative estimates using a multistage-sampling-based approach. PLoS Medicine. 2019; 16(5): e1002813. |
[26]
proposed that biological difficulties in older patients may postpone suppression. Substance use was highly linked with delayed suppression, which is consistent with Damulak
et al. | [27] | UNAIDS. UNAIDS Data 2020. Geneva: Joint United Nations Programme on HIV/AIDS; 2020. |
[27]
. Frequent clinic visits were associated with faster suppression, supporting previous research findings
| [28] | Vu GT, Tran BX, Hoang CL, Hall BJ, Phan HT, Ha GH, et al. Global research on quality of life of patients with HIV/AIDS: is it socio-culturally addressed? (GAPRESEARCH). International journal of environmental research and public health. 2020; 17(6): 2127. |
| [29] | Westergaard RP, Hess T, Astemborski J, Mehta SH, Kirk GD. Longitudinal changes in engagement in care and viral suppression for HIV-infected injection drug users. AIDS. 2013; 27(16): 2559-66. |
[28, 29]
. Unlike Mody
et al. | [30] | World Health Organization. Global health sector strategies on, respectively, HIV, viral hepatitis and sexually transmitted infections for the period 2022-2030. Geneva: World Health Organization; 2022. |
[30]
, timing of suppression was independent of baseline viral load and CD4 count, possibly due to regional ART regimen differences or more clinical attention to sicker patients, explaining co-morbidities’ association with faster suppression.
The effectiveness of interdisciplinary treatment was shown in China by Zhang
et al. | [26] | Sikazwe I, Eshun-Wilson I, Sikombe K, Czaicki N, Somwe P, Mody A, et al. Retention and viral suppression in a cohort of HIV patients on antiretroviral therapy in Zambia: Regionally representative estimates using a multistage-sampling-based approach. PLoS Medicine. 2019; 16(5): e1002813. |
[26]
where case conferencing and other therapies significantly reduced the time to achieve viral suppression
| [26] | Sikazwe I, Eshun-Wilson I, Sikombe K, Czaicki N, Somwe P, Mody A, et al. Retention and viral suppression in a cohort of HIV patients on antiretroviral therapy in Zambia: Regionally representative estimates using a multistage-sampling-based approach. PLoS Medicine. 2019; 16(5): e1002813. |
[26]
. More focused counselling increased the number of suppressors, but better adherence EAC had little impact which may suggest delivery inequitably biased impact
| [31] | Zhang J, Olatosi B, Yang X, Weissman S, Li Z, Hu J, et al. Studying patterns and predictors of HIV viral suppression using A Big Data approach: a research protocol. BMC Infectious Diseases. 2022; 22: 122. |
[31]
. Focusing patient encouragement of the viral load and dietary aid or aid groups hardly influenced suppression time. This argument supports previous research and contradicts other findings that suggest the benefit of ART regimens, or the method of intervention implementation diverged differently
| [25] | Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. 9th ed. Philadelphia: Lippincott Williams & Wilkins; 2012. |
[25]
.
This study contributes local data on survival patterns and factors linked to viral suppression in Chingola District. Kaplan-Meier analysis revealed a 50% suppression by 12 months. More frequent clinic visits quadrupled suppression speed (aHR=2.026), whereas case conferencing increased suppression odds more than sevenfold (aHR=7.309). ART universal access also enhanced suppression (aHR=1.392).
5. Conclusion
The findings contribute to the emerging body knowledge of survival trends and time to viral load suppression among PLWHIV in Chingola District. Importantly, median time to viral suppression was 12 months, demonstrating that ART works to achieve viral load suppression in all people living with HIV.
A multivariate analysis identified several factors that were critical for achieving viral suppression, including more frequent visits to the clinic and integrated care models like case conferencing and multidisciplinary meetings. Demographic and clinical characteristics (such as age, sex, economic status, etc.) had no apparent effects on the time to suppress.
Nonetheless, high-risk PLHIV with substance abuse backgrounds and those with several comorbidities were recognized to need proactive measures to improve their treatment outcome. The results indicate both a need to develop targeted treatment strategies as well as to design public health interventions to sustainably improve viral suppression and health-related quality of life among PLWHIV in the Chingola District.
5.1. Limitations
1) Lack Randomization: Considering this study was observational and retrospective, it lacked the randomisation perspective, which could have resulted in skewed treatment effect estimates.
2) Change in Treatment Guidelines: HIV programming treatment recommendations and practices are constantly evolving.
5.2. Recommendations for Future Research
Longitudinal Study of Intervention Efficacy: are models such as case conferencing and adherence counselling on viral suppression.
5.3. Ethics Approval
In reference to this paper, ethical approval was obtained from the National Health Research Authority (NHRA) and University of Lusaka, Research Ethics Committee (UNILUS-REC) approval number FWA00033228-461(08)/(08)/{2024} as per standard procedures. The Ministry of Health (MoH) was consulted for administrative permission to get access to medical records of patients at specific Health Facilities where the study was conducted. This also ensured informed consent, as each health facility received a complete overview of the study's objectives, methods, risks, and potential benefits. Patient’s record remained anonymous during the study, and data was de-identified to maintain participant confidentiality. Following these precautions, it ensured that participants were protected, ethical standards were maintained, and the integrity of the research results was validated.
Abbreviations
AIDS | Acquired Immunodeficiency Syndrome |
ART | Antiretroviral Therapy |
CD4 count | Cluster Differentiation 4 |
HIV | Human Immunodeficiency Virus |
MoH | Ministry of Health |
NHRA-Z | National Health Research Authority-Zambia |
PLHIV | Person or People Living with HIV |
PEPFER | United States Presidential Emergency Plan for AIDS Relief |
MER | Monitoring, Evaluation and Reporting |
UNAID | United Nations Aid |
UNILUSREC | University of Lusaka Research Ethical Committee |
VL | Viral Load |
VLC | Viral Load Coverage |
VLS | Viral Load Suppression |
WHO | World Health Organization |
ZNPHI | Zambia National Public Health Institute |
Funding
No funding received.
Author Contributions
Bryson Musonda: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Software, Visualization, Writing – original draft
Eustarckio Kazonga: Formal Analysis, Project administration, Software, Supervision, Writing – review & editing
Tyson Chipokoso: Investigation, Methodology, Validation, Visualization, Writing – review & editing
Kelvin Mwangilwa: Investigation, Methodology, Validation, Visualization, Writing – review & editing
Thanthwe Mangani: Investigation, Methodology, Validation, Writing – review & editing
Kawanga Lackeby: Investigation, Methodology, Validation, Writing – review & editing
Conflicts of Interest
The authors declare no conflict of interest.
References
| [1] |
Boerma RS, Boender TS, Bussink AP, Calis JC, Bertagnolio S, Rinke de Wit TF, et al. Suboptimal viral suppression rates among HIV-infected children in low- and middle-income countries: a meta-analysis. AIDS. 2016; 30(15): 2305-14.
|
| [2] |
Byrd KK, Hou JG, Hazen R, Kirkham H, Suzuki S, Clay PG, et al. Antiretroviral adherence level necessary for HIV viral suppression using real-world data. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2019; 82(3): 245-51.
|
| [3] |
Cochran WG. Sampling Techniques. 3rd ed. New York: Wiley; 1977.
|
| [4] |
Creswell JW, Creswell JD. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches. 5th ed. Thousand Oaks: Sage; 2018.
|
| [5] |
Damulak PP, Ismail S, Abdul Manaf R, Mohd Said S, Agbaji O. Interventions to improve adherence to antiretroviral therapy (ART) in sub-Saharan Africa: An updated systematic review. International journal of environmental research and public health. 2021; 18(5): 2477.
|
| [6] |
Dessie G, Wagnew F, Mulugeta H, Amare D, Jara D, Leshargie CT, et al. The effect of poor retention to care on virologic failure among people living with HIV/AIDS in Ethiopia: a systematic review and meta-analysis. AIDS Research and Therapy. 2020; 17: 45.
|
| [7] |
Desta AA, Woldearegay TW, Futwi N, Gebrehiwot GT, Gebru GG, Berhe AA, et al. HIV virological non-suppression and its associated factors in children on antiretroviral therapy at a major treatment centre in Southern Ethiopia: a cross-sectional study. BMC Infectious Diseases. 2019; 19: 60.
|
| [8] |
Hoffmann CJ, Charalambous S, Thio CL, Martin DJ, Pemba L, Fielding KL, et al. Hepatitis B virus infection and response to antiretroviral therapy (ART) in a South African ART program. Clinical Infectious Diseases. 2008; 47(11): 1479-85.
|
| [9] |
Ioannou P, Vouidaski E, Voulgaridi I, Karakonstantis S, Kofteridis D, Samonis G, et al. Frequency of clinic visits and HIV viral load suppression among people living with HIV: a simple clinical predictive model. AIDS Care. 2020; 32(5): 616-22.
|
| [10] |
Kanters S, Park JJ, Chan K, Socias ME, Ford N, Forrest JI, et al. Interventions to improve adherence to antiretroviral therapy: a systematic review and network meta-analysis. The Lancet HIV. 2017; 4(1): e31-e40.
|
| [11] |
Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. Journal of the American Statistical Association. 1958; 53(282): 457-81.
|
| [12] |
Kayukwa A, Butts SA, Barylski NA, Alcaide ML, Rodriguez VJ, Chitalu N, et al. HIV prevention among Zambian itinerant workers: challenges and solutions. Journal of health care for the poor and underserved. 2019; 30(1): 358-77.
|
| [13] |
Kleinbaum DG, Klein M. Survival Analysis: A Self-Learning Text. 3rd ed. New York: Springer; 2012.
|
| [14] |
Lima VD, Harrigan R, Bangsberg DR, Hogg RS, Gross R, Yip B, et al. The combined effect of modern highly active antiretroviral therapy regimens and adherence on mortality over time. Journal of Infectious Diseases. 2010; 202(5): 750-9.
|
| [15] |
Mesic A, Halim N, MacLeod W, Haker C, Mwansa M, Biemba G. Post handout/brand friends, Facilitators and barriers to adherence to antiretroviral therapy and retention in care among adolescents living with HIV/AIDS in Zambia: a mixed method study. AIDS and Behaviour. 2019; 23: 2618-28.
|
| [16] |
Mills EJ, Lester R, Thorlund K, Lorenzi M, Muldoon K, Kanters S, et al. Interventions to promote adherence to antiretroviral therapy in Africa: a network meta-analysis. The Lancet HIV. 2014; 1(3): e104-11.
|
| [17] |
Ministry of Health Zambia. Zambia Population-Based HIV Impact Assessment (ZAMPHIA) 2016. Lusaka: Ministry of Health; 2019.
|
| [18] |
Mody A, Sikazwe I, Czaicki N, Wa Mwanza M, Savory T, Sikombe K, et al. Estimating real-world impact of expanded eligibility for antiretroviral treatment: Evidence from a regression discontinuity design in Zambia. PLoS Medicine. 2018; 15(6): e1002574.
|
| [19] |
Mugavero MJ, Amico KR, Horn T, Thompson MA. The state of engagement in HIV care in the United States: from cascade to continuum to control. Clinical Infectious Diseases. 2013; 57(8): 1164-71.
|
| [20] |
Mulenga LB, Hines JZ, Stafford KA, Dzekedzeke K, Sivile S, Lindsay B, et al. A Comparison of 2016 and 2021 Population-Based HIV Impact Assessments in Zambia: Changes in HIV Prevalence, Incidence, and Viral Load Suppression. AIDS. 2022; 36(Suppl 1): S1-S9.
|
| [21] |
Musonda J. An Investigation on Factors causing Non-Adherence of Ant-Retro Viral Therapy (Art) among HIV Patients in Nchanga North General Hospital-Chingola, Zambia. Lusaka: University of Zambia; 2019.
|
| [22] |
Mwansa M, McLeod W, Halim N, Biemba G, Shiliya N, Mwanza A, et al. Below is a list of links to PEPFAR Materials and tools that you can use to view and search for various PEPFAR documents, guidelines, and publications. Washington: PEPFAR; 2017.
|
| [23] |
Nance RM, Delaney JC, Simoni JM, Wilson IB, Mayer KH, Whitney BM, et al. Temporal trends in virologic suppression among HIV-infected individuals in care in the United States, 1997 to 2015: a cohort study. Annals of Internal Medicine. 2018; 169(6): 376-84.
|
| [24] |
Phillips AN, Staszewski S, Weber R, Kirk O, Francioli P, Miller V, et al. HIV viral load response to antiretroviral therapy according to the baseline CD4 cell count and viral load. BMJ. 2001; 322(7286): 289-93.
|
| [25] |
Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice. 9th ed. Philadelphia: Lippincott Williams & Wilkins; 2012.
|
| [26] |
Sikazwe I, Eshun-Wilson I, Sikombe K, Czaicki N, Somwe P, Mody A, et al. Retention and viral suppression in a cohort of HIV patients on antiretroviral therapy in Zambia: Regionally representative estimates using a multistage-sampling-based approach. PLoS Medicine. 2019; 16(5): e1002813.
|
| [27] |
UNAIDS. UNAIDS Data 2020. Geneva: Joint United Nations Programme on HIV/AIDS; 2020.
|
| [28] |
Vu GT, Tran BX, Hoang CL, Hall BJ, Phan HT, Ha GH, et al. Global research on quality of life of patients with HIV/AIDS: is it socio-culturally addressed? (GAPRESEARCH). International journal of environmental research and public health. 2020; 17(6): 2127.
|
| [29] |
Westergaard RP, Hess T, Astemborski J, Mehta SH, Kirk GD. Longitudinal changes in engagement in care and viral suppression for HIV-infected injection drug users. AIDS. 2013; 27(16): 2559-66.
|
| [30] |
World Health Organization. Global health sector strategies on, respectively, HIV, viral hepatitis and sexually transmitted infections for the period 2022-2030. Geneva: World Health Organization; 2022.
|
| [31] |
Zhang J, Olatosi B, Yang X, Weissman S, Li Z, Hu J, et al. Studying patterns and predictors of HIV viral suppression using A Big Data approach: a research protocol. BMC Infectious Diseases. 2022; 22: 122.
|
Cite This Article
-
APA Style
Musonda, B., Chipokoso, T., Mwangilwa, K., Mangani, T., Mwadetsa, S. D., et al. (2025). Factors Associated with Time to Viral Load Suppression Among People Living with HIV in Chingola District: A Retrospective Cohort Study. World Journal of Public Health, 10(4), 524-531. https://doi.org/10.11648/j.wjph.20251004.19
 Copy
|
Copy
|
 Download
Download
ACS Style
Musonda, B.; Chipokoso, T.; Mwangilwa, K.; Mangani, T.; Mwadetsa, S. D., et al. Factors Associated with Time to Viral Load Suppression Among People Living with HIV in Chingola District: A Retrospective Cohort Study. World J. Public Health 2025, 10(4), 524-531. doi: 10.11648/j.wjph.20251004.19
Copy
|
Download
AMA Style
Musonda B, Chipokoso T, Mwangilwa K, Mangani T, Mwadetsa SD, et al. Factors Associated with Time to Viral Load Suppression Among People Living with HIV in Chingola District: A Retrospective Cohort Study. World J Public Health. 2025;10(4):524-531. doi: 10.11648/j.wjph.20251004.19
Copy
|
Download
-
@article{10.11648/j.wjph.20251004.19,
author = {Bryson Musonda and Tyson Chipokoso and Kelvin Mwangilwa and Thanthwe Mangani and Sandra Diana Mwadetsa and Kawanga Lackeby and Innocent Mwaba and Norah Ndambo and Rabson Kanyinji and Paul Kasinde and Andrew Phiri and Moses Mwale and Hiwena Malawo and Marvis Mbewe and Eustarckio Kazonga},
title = {Factors Associated with Time to Viral Load Suppression Among People Living with HIV in Chingola District: A Retrospective Cohort Study
},
journal = {World Journal of Public Health},
volume = {10},
number = {4},
pages = {524-531},
doi = {10.11648/j.wjph.20251004.19},
url = {https://doi.org/10.11648/j.wjph.20251004.19},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20251004.19},
abstract = {Improving health outcomes and lowering human immunodeficiency virus (HIV) transmission among people living with human immunodeficiency virus (PLHIV) requires achieving viral load suppression. In this study, people living with HIV in Zambia's Chingola District had their survival rates and factors related to viral suppression assessed. The research aimed at analysing factors associated with time to viral suppression among PLHIV in Chingola District using survival analysis. A retrospective cohort study design was used, utilising 385 clinical records of PLHIV in Chingola district, with the focus on 15 months period (January 2022 to April 2023). Cox proportional hazards regression models and Kaplan-Meier survival analysis were used as statistical techniques. The age group 50+ years accounted the highest proportion (45.5%), while 40–49 age group accounted for the least proportion (15.3%). Males dominated (56.6%) whereas 43.4% were females. The median time to attain viral suppression was 12 months. Consequently, frequent clinic visits significantly decreased suppression time (aHR = 2.026, p = 0.001), and PLHIV with comorbidity experienced faster viral suppression (aHR = 1.438, p = 0.017). None substance users had 1.392 times increased chances of achieving Viral load suppression higher than substance users (aHR = 1.392, p = 0.036). The intervention that increased the chance of suppression was case conferencing (aHR = 7.309, p = 0.001). The results highlighted how crucial it is to design interventions specifically for high-risk groups to enhance viral load results. Suggestions include implementing focused interventions for PLHIV with comorbidities and substance abusers, expanding case conferences, and fortifying adherence support networks.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Factors Associated with Time to Viral Load Suppression Among People Living with HIV in Chingola District: A Retrospective Cohort Study
AU - Bryson Musonda
AU - Tyson Chipokoso
AU - Kelvin Mwangilwa
AU - Thanthwe Mangani
AU - Sandra Diana Mwadetsa
AU - Kawanga Lackeby
AU - Innocent Mwaba
AU - Norah Ndambo
AU - Rabson Kanyinji
AU - Paul Kasinde
AU - Andrew Phiri
AU - Moses Mwale
AU - Hiwena Malawo
AU - Marvis Mbewe
AU - Eustarckio Kazonga
Y1 - 2025/11/14
PY - 2025
N1 - https://doi.org/10.11648/j.wjph.20251004.19
DO - 10.11648/j.wjph.20251004.19
T2 - World Journal of Public Health
JF - World Journal of Public Health
JO - World Journal of Public Health
SP - 524
EP - 531
PB - Science Publishing Group
SN - 2637-6059
UR - https://doi.org/10.11648/j.wjph.20251004.19
AB - Improving health outcomes and lowering human immunodeficiency virus (HIV) transmission among people living with human immunodeficiency virus (PLHIV) requires achieving viral load suppression. In this study, people living with HIV in Zambia's Chingola District had their survival rates and factors related to viral suppression assessed. The research aimed at analysing factors associated with time to viral suppression among PLHIV in Chingola District using survival analysis. A retrospective cohort study design was used, utilising 385 clinical records of PLHIV in Chingola district, with the focus on 15 months period (January 2022 to April 2023). Cox proportional hazards regression models and Kaplan-Meier survival analysis were used as statistical techniques. The age group 50+ years accounted the highest proportion (45.5%), while 40–49 age group accounted for the least proportion (15.3%). Males dominated (56.6%) whereas 43.4% were females. The median time to attain viral suppression was 12 months. Consequently, frequent clinic visits significantly decreased suppression time (aHR = 2.026, p = 0.001), and PLHIV with comorbidity experienced faster viral suppression (aHR = 1.438, p = 0.017). None substance users had 1.392 times increased chances of achieving Viral load suppression higher than substance users (aHR = 1.392, p = 0.036). The intervention that increased the chance of suppression was case conferencing (aHR = 7.309, p = 0.001). The results highlighted how crucial it is to design interventions specifically for high-risk groups to enhance viral load results. Suggestions include implementing focused interventions for PLHIV with comorbidities and substance abusers, expanding case conferences, and fortifying adherence support networks.
VL - 10
IS - 4
ER -
Copy
|
Download