Slums and informal settlements are residential areas physically and socially disintegrated. In spite of this, inadequate health-related data on slum areas and informal settlements has led to inappropriate and unrealistic allocation of healthcare resources by the public and private health providers. This study investigates the patronage pattern and accessibility of healthcare facilities to residents of urban slums and Informal settlements in Ibadan Metropolis, a rapidly growing urban area in Nigeria facing challenges related to urbanization and healthcare infrastructure. Data were collected from both primary and secondary sources. Structured questionnaire was administered on 1,389 residents of the slummy neighbourhoods and informal settlements in Ibadan metropolis, and obtained data were analyzed using descriptive and inferential statistics. Results revealed that out of 109 neighbourhoods, 42.1% were categorized as slummy neighbourhoods, 36.7% as slums/informal settlements, while 21.2% were informal settlement using slummy and informality conditions respectively. Results revealed that distance to health facility (β= -0.353, p<0.05), educational qualification (β=-0.063, p<0.05) and household size (β= -0.052, p<0.05) had an inverse relationship with patronage of health facilities, while age (β=0.086, p< 0.05) had a positive relationship. It was also revealed that access to PHC and dispensary/clinic in slummy neighbouhoods and slum/informal settlements is higher compared to informal settlements in the study area. The study therefore recommends implementation of slum improvement program for the slummy and slums/informal neighbourhoods, provision of additional healthcare facilities to be located especially in the slummy neighbourhoods and informal settlements to ensure equitable distribution.
| Published in | Urban and Regional Planning (Volume 9, Issue 3) |
| DOI | 10.11648/j.urp.20240903.12 |
| Page(s) | 71-87 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Urban Slum, Informal Settlements, Patronage Pattern, Accessibility, Healthcare Facilities, Ibadan Metropolis, Nigeria
SN | Neighbourhoods | *Slummy Condition (Poor water/Sanitation) (%) | **Informality Condition (Bld Without Plg/Approval) (%) | a | b | ab | c |
|---|---|---|---|---|---|---|---|
1 | Oniyanrin, Inalende, | 63.3 | 56.0 | √ | √ | √ | |
2 | Mokola | 54.0 | 56.0 | √ | √ | √ | |
3 | Secretariat | 38.0 | 35.4 | √ | |||
4 | Sabo Quart | 54.4 | 58.0 | √ | √ | √ | |
5 | Oke-Itunu, | 57.0 | 67.0 | √ | √ | √ | |
6 | Sango | 58.0 | 71.2 | √ | √ | √ | |
7 | Emmanuel | 32.2 | 35.0 | √ | |||
8 | Polytechnic | 35.0 | 40.6 | √ | |||
9 | University of Ibadan | 28.0 | 33.0 | √ | |||
10 | Abadina Quarters | 27.0 | 30.3 | √ | |||
11 | Coca-Cola | 39.5 | 56.0 | √ | |||
12 | Bodija Estate (Old) | 37.0 | 34.4 | √ | |||
13 | Samonda, Aerodrome, | 32.0 | 38.0 | √ | |||
14 | Adeoyo, | 56.4 | 60.2 | √ | √ | √ | |
15 | Yemetu | 58.0 | 63.0 | √ | √ | √ | |
16 | UCH | 31.0 | 55.4 | √ | |||
17 | Ikolaba, Idi-Ape, Oluwo | 32.3 | 37.0 | √ | |||
18 | Agodi GRA | 28.0 | 32.0 | √ | |||
19 | Igosun, Kambi, | 61.4 | 65.2 | √ | √ | √ | |
20 | Ashi | 41.0 | 46.0 | √ | |||
21 | New Bodija | 29.0 | 34.0 | √ | |||
22 | Bodija Railway | 31.1 | 54.3 | √ | |||
23 | Bashorun | 41.0 | 45.0 | √ | |||
24 | Agbowo, Orogun | 53.0 | 59.4 | √ | √ | √ | |
25 | Orogun Express | 49.3 | 53.0 | √ | √ | ||
26 | Ojoo Orogun Side | 46.0 | 48.4 | √ | |||
27 | Labiran | 67.0 | 72.0 | √ | √ | √ | |
28 | Aremo | 56.0 | 60.3 | √ | √ | √ | |
29 | Oje | 57.4 | 62.0 | √ | √ | √ | |
30 | Agugu | 60.0 | 65.0 | √ | √ | √ | |
31 | Ita-Bale, | 60.0 | 71.4 | √ | √ | √ | |
32 | Belyerunka, | 59.2 | 64.0 | √ | √ | √ | |
33 | Kosodo, Oja-Igbo | 64.0 | 60.8 | √ | √ | √ | |
34 | Ile-Aperin, | 62.3 | 58.0 | √ | √ | √ | |
35 | Adekile, Koloko | 67.0 | 49.0 | √ | |||
36 | Oluyoro Hospital | 66.0 | 71.7 | √ | √ | √ | |
37 | Oke-Adu, | 61.0 | 68.0 | √ | √ | √ | |
38 | Oke-Irefin Itutaba | 68.3 | 69.0 | √ | √ | √ | |
39 | Oke-Offa Atipe | 69.0 | 71.5 | √ | √ | √ | |
40 | Abayomi, Iwo Road, | 56.3 | 65.0 | √ | √ | √ | |
41 | Basorun, Idi-Ape, Oyo | 47.0 | 52.4 | √ | |||
42 | Holy Trinity, Onipepeye | 39.0 | 41.0 | √ | |||
43 | Yanbule, Basorun MKT | 37.0 | 36.0 | √ | |||
44 | Eleta, Labo, | 69.0 | 74.6 | √ | √ | √ | |
45 | Oke-Oluokun | 64.4 | 74.0 | √ | √ | √ | |
46 | Ile-Tuntun, Ode-Aje, | 63.0 | 76.3 | √ | √ | √ | |
47 | Odinjo, Idi-Aro, | 62.3 | 59.0 | √ | √ | √ | |
48 | Oranyan, Omiyale, | 58.3 | 59.4 | √ | √ | √ | |
49 | Oniyere, Modina, | 59.2 | 62.0 | √ | √ | √ | |
50 | Oja-Oba, Laamo | 71.0 | 68.7 | √ | √ | √ | |
51 | Elekuro, Labo, | 67.0 | 76.0 | √ | √ | √ | |
52 | Academy, Ifedapo, | 63.4 | 65 | √ | √ | √ | |
53 | Kudeti, Bode | 43.0 | 58.0 | √ | |||
54 | Olorunsogo Molete | 41.2 | 54.0 | √ | |||
55 | Osungbade, | 57,0 | 63.0 | √ | √ | √ | |
56 | Felele/Express | 39.3 | 35.4 | √ | |||
57 | Ilupeju, Fajemisi | 37.3 | 53,0 | √ | |||
58 | Odo-Oba | 56.0 | 65.0 | √ | √ | √ | |
59 | Sanyo | 57.0 | 63.2 | √ | √ | ||
60 | Orita-Challenge | 39.0 | 55.0 | √ | |||
61 | Felele Rab | 38.4 | 39.0 | √ | |||
62 | Ayeye, Agbaje | 67.0 | 78.4 | √ | √ | √ | |
63 | Agbede-Adodo, | 59.5 | 64.0 | √ | √ | √ | |
64 | Agbeni, Ile-Adebisi | 59.0 | 63.0 | √ | √ | √ | |
65 | Ekotedo, | 54.0 | 64.2 | √ | √ | √ | |
66 | Inalende, | 62.0 | 51.0 | √ | |||
67 | Onireke GRA, | 30.4 | 35.0 | √ | |||
68 | Idikan | 57.0 | 67.4 | √ | √ | √ | |
69 | Links Reservation | 34.0 | 40.0 | √ | |||
70 | Letmuck Barracks | 35.0 | 38.0 | √ | |||
71 | Eleyele, Benjamin | 38.3 | 42.5 | √ | |||
72 | Olopomewa | 43.0 | 58.0 | √ | √ | ||
73 | Eleyele Water Works | 36.0 | 54.0 | √ | √ | ||
74 | Eleyele Police Barracks, | 34.3 | 36.0 | √ | |||
75 | Jericho Nursing Home | 32.0 | 38.3 | √ | |||
76 | Idi-Ishin, Omo Oba | 35.0 | 46.0 | √ | |||
77 | NIHORT Quarters | 32.0 | 38.4 | √ | |||
78 | Adamasigba | 39.4 | 35.0 | √ | |||
79 | Alekuso, Akinyo | 62.0 | 58.0 | √ | √ | √ | |
80 | Isale-Osi, Born-Photo | 65.0 | 72.5 | √ | √ | √ | |
81 | Foko, Asaka | 64.0 | 68.0 | √ | √ | √ | |
82 | Oke-Ado | 52.4 | 59.0 | √ | √ | √ | |
83 | Imale-Nfalafia, | 45.0 | 49.0 | √ | |||
84 | Joyce-B, | 41.0 | 45.3 | √ | |||
85 | Ososami, | 39.2 | 56.0 | √ | |||
86 | Elewura, | 41.0 | 54.0 | √ | |||
87 | Akinyemi, D-Rovans | 39.4 | 57.0 | √ | |||
88 | Oluyole Estate | 38.0 | 46.3 | √ | |||
89 | Liberty Layout, | 34.0 | 40.0 | √ | |||
90 | Ile-Oba, Ile-Ida, | 67.0 | 79.0 | √ | √ | √ | |
91 | Idi-Arere, Olokobi | 64.0 | 76.0 | √ | √ | √ | |
92 | Popoyemoja | 63.3 | 75.4 | √ | √ | √ | |
93 | Molete, U.M.C. P | 42.0 | 49.0 | √ | |||
94 | Anfani Layout, | 41.0 | 48.0 | √ | |||
95 | Orita-Ikereku, | 42.0 | 47.3 | √ | |||
96 | Agbokojo, Ita-Maya, | 65.1 | 60.0 | √ | √ | √ | |
97 | Oke-Bola, Seventh D | 43.0 | 54.3 | √ | |||
98 | Iyaganku GRA, | 34.0 | 39.2 | √ | |||
99 | A.I R & T, OYSADEP | 35.0 | 40.0 | √ | |||
100 | Apata, Aba-Alamu, | 57.0 | 55.0 | √ | √ | √ | |
101 | Adifase, Bora | 58.3 | 55.2 | √ | √ | √ | |
102 | Alalubosa, Railway | 32.0 | 39.0 | √ | |||
103 | Odo-Ana, | 58.2 | 56.0 | √ | √ | √ | |
104 | Idi-Ishin, NIHORT | 37.0 | 40.0 | √ | |||
105 | Aleshinloye Market, | 38.0 | 39.0 | √ | |||
106 | J. Allen, Seventh | 35.1 | 37.0 | √ | |||
107 | Ogunpa Cathedral | 41.0 | 55.2 | √ | |||
108 | Gbagi, Ogunpa | 60.1 | 61.0 | √ | √ | √ | |
109 | Ago-Taylor, | 41.4 | 54.0 | √ | |||
Total | 4823.5 | 5725.4 |
Variable | Neighbourhood | |||||||
|---|---|---|---|---|---|---|---|---|
Slum | Slum/informal | Informal | Total | |||||
F | % | F | % | F | % | F | % | |
Age | ||||||||
18-25 | 40 | 2.9 | 40 | 2.9 | 12 | 0.9 | 92 | 6.6 |
26-35 | 240 | 17.3 | 222 | 16.0 | 80 | 5.7 | 542 | 39.0 |
36-45 | 256 | 18.4 | 243 | 17.5 | 89 | 6.4 | 588 | 42.3 |
46-55 | 50 | 3.6 | 51 | 3.7 | 19 | 1.4 | 120 | 3.4 |
56 and above | 28 | 2.0 | 10 | 0.7 | 9 | 0.6 | 47 | 3.4 |
Total | 614 | 44.2 | 566 | 40.7 | 209 | 15.0 | 1389 | 100 |
Gender | ||||||||
Male | 360 | 25.9 | 323 | 23.3 | 121 | 8.8 | 804 | 57.9 |
Female | 254 | 18.3 | 243 | 17.5 | 88 | 6.3 | 585 | 42.1 |
Total | 614 | 44.2 | 566 | 40.7 | 209 | 15.0 | 1389 | 100 |
Education | ||||||||
Non Formal | 137 | 9.9 | 78 | 5.6 | 22 | 1.5 | 237 | 17.1 |
Primary | 84 | 6.0 | 77 | 5.5 | 19 | 1.4 | 180 | 13.0 |
Secondary | 139 | 10.0 | 215 | 15.5 | 28 | 4.4 | 415 | 29.9 |
ND/NCE | 125 | 9.0 | 96 | 6.9 | 32 | 3.2 | 265 | 19.1 |
BSC/HND | 117 | 8.4 | 85 | 6.1 | 62 | 4.4 | 263 | 18.9 |
Post-Graduate | 12 | 0.9 | 15 | 1.1 | 2 | 0.2 | 29 | 2.1 |
Total | 614 | 44.2 | 566 | 40.7 | 209 | 15.0 | 1389 | 100 |
Occupation | ||||||||
Student/apprentice | 76 | 5.5 | 99 | 7.1 | 24 | 1.7 | 208 | 15.0 |
Unemployed | 83 | 6.0 | 28 | 2.0 | 15 | 1.1 | 133 | 9.6 |
Personal business | 376 | 27.1 | 306 | 22.0 | 57 | 4.1 | 786 | 56.6 |
Public employee | 57 | 4.1 | 117 | 8.4 | 27 | 1.9 | 219 | 15.8 |
Retiree | 18 | 1.3 | 16 | 1.2 | 2 | 0.1 | 38 | 2.7 |
Others | 4 | 0.3 | 0 | 0 | 0 | 0 | 5 | 0.4 |
Total | 614 | 44.2 | 566 | 40.7 | 125 | 9.0 | 1389 | 100 |
Variable | Neighbourhood | |||||||
|---|---|---|---|---|---|---|---|---|
Slum | Slum/informal | Informal | Total | |||||
F | % | F | % | F | % | F | % | |
Marital Status | ||||||||
Single | 88 | 6.3 | 76 | 5.5 | 17 | 1.2 | 193 | 13.9 |
Married | 483 | 34.8 | 458 | 33.0 | 104 | 7.5 | 1110 | 79.9 |
Divorced | 27 | 1.9 | 14 | 1.0 | 3 | 0.2 | 48 | 3.5 |
Separated | 16 | 1.2 | 18 | 1.3 | 1 | 0.1 | 38 | 2.7 |
Total | 614 | 44.2 | 566 | 40.7 | 125 | 9.0 | 1389 | 100 |
Location of health facility | ||||||||
Within Neighbourhhod | 518 | 37.3 | 539 | 38.8 | 111 | 8.0 | 1248 | 89.8 |
Outside Neighbourhood | 96 | 6.9 | 27 | 1.9 | 14 | 1.0 | 141 | 10.2 |
Total | 614 | 44.2 | 566 | 40.7 | 125 | 9.0 | 1389 | 100 |
Cost of travel to nearest health facility | ||||||||
₦100 or less | 176 | 12.7 | 188 | 13.5 | 34 | 2.4 | 417 | 30.0 |
₦101-300 | 286 | 20.6 | 237 | 17.1 | 72 | 5.2 | 633 | 45.6 |
₦301-500 | 133 | 9.6 | 99 | 7.1 | 15 | 1.1 | 266 | 19.2 |
₦501-1000 | 17 | 1.2 | 34 | 2.4 | 2 | 0.1 | 60 | 4.3 |
Above ₦1000 | 2 | 0.1 | 8 | 0.6 | 2 | 0.1 | 11 | 0.9 |
Total | 614 | 44.2 | 566 | 40.7 | 125 | 9.0 | 1389 | 100 |
Amount spent on health treatment in the last one month | ||||||||
Less than ₦5000 | 408 | 29.4 | 355 | 25.6 | 81 | 5.8 | 906 | 65.2 |
₦6000-20000 | 198 | 14.3 | 192 | 13.8 | 44 | 3.2 | 455 | 32.8 |
₦20001-50000 | 8 | 0.6 | 19 | 1.4 | 0 | 0.0 | 28 | 2.0 |
Total | 614 | 44.2 | 566 | 40.7 | 125 | 9.0 | 1389 | 100 |
Variable | Slum | Slum/informal | Informal |
|---|---|---|---|
Household Size (Mean) | 5.5902 | 5.0212 | 4.9016 |
Monthly income (Mean) | ₦35,156 | ₦43,024 | ₦76,433 |
Solid Waste Disposal | Neighbourhood | |||||||
|---|---|---|---|---|---|---|---|---|
Slum Neighbourhoods | Slum/informal Neighbourhoods | Informal Settlement | Total | |||||
F | % | F | % | F | % | F | % | |
Dumped in Nearby Stream/River | 144 | 10.4 | 45 | 3.2 | 24 | 1.7 | 222 | 16 |
Dispose beside the building | 334 | 24.0 | 249 | 17.9 | 34 | 2.4 | 651 | 46.9 |
Dump in waste bin | 102 | 7.3 | 237 | 17.1 | 44 | 3.2 | 422 | 30.4 |
Burn on the main access road | 30 | 2.2 | 32 | 2.3 | 20 | 1.4 | 83 | 6.0 |
Others | 4 | 0.3 | 3 | 0.2 | 3 | 0.2 | 11 | 0.8 |
Total | 614 | 44.2 | 566 | 40.7 | 125 | 9.0 | 1389 | 100 |
Availability of drainage | ||||||||
YES | 307 | 22.1 | 378 | 27.2 | 75 | 5.4 | 816 | 58.7 |
NO | 307 | 22.1 | 188 | 13.5 | 50 | 3.6 | 573 | 41.3 |
Total | 614 | 44.2 | 566 | 40.7 | 125 | 9.0 | 1389 | 100 |
General Environmental Conditions | ||||||||
Good | 66 | 4.8 | 149 | 10.7 | 28 | 2.0 | 268 | 19.3 |
Fair | 221 | 15.9 | 366 | 26.3 | 60 | 4.3 | 691 | 49.7 |
Poor | 327 | 23.5 | 51 | 3.7 | 37 | 2.7 | 430 | 31.0 |
Total | 614 | 44.2 | 566 | 40.7 | 125 | 9.0 | 1389 | 100 |
Accessibility | ||||||||
Footpath | 290 | 20.9 | 249 | 17.9 | 73 | 5.3 | 642 | 46.2 |
Earthward | 200 | 14.4 | 218 | 15.7 | 19 | 1.4 | 467 | 33.6 |
Paveward | 124 | 8.9 | 99 | 7.1 | 33 | 2.4 | 280 | 20.2 |
Total | 614 | 44.2 | 566 | 40.7 | 125 | 9.0 | 1389 | 100 |
Building Approval | ||||||||
YES | 170 | 12.2 | 323 | 23.3 | 57 | 4.1 | 592 | 42.6 |
NO | 444 | 32.0 | 243 | 17.5 | 68 | 4.9 | 797 | 57.4 |
Total | 614 | 44.2 | 566 | 40.7 | 125 | 9.0 | 1389 | 100 |
Independent Variables (Predictors) | Dispensary | PHC | General Hospital | Tertiary Hospital | Specialist Hospital |
|---|---|---|---|---|---|
Standardized Coefficients (Beta) | |||||
Gender | (.021) | (-.063)** | (-.032) | (-.050) | (.005) |
Age | (.086)** | (.044) | (.064)** | (-.004) | (.048) |
Educational qualifications | (-.063)** | (-.078)** | (-.013) | (.015) | (.030) |
Household size | (-.014) | (.016) | (-.052)** | (-.005) | (-.020) |
Average monthly income | (-.012) | (-.012) | (.136)** | (.211)** | (.210)** |
Average distance to the health facility | (-.353)** | (-.084)** | (-.171)** | (-.102)** | (-.211)** |
Location of the health facility | (-.029) | (-.038) | (.257_** | (.108)** | (.124)** |
R =0.421a | R=0.186a | R=0.367a | R=0.313a | R=0.395a | |
Type of Health Facility | Type of Neighbourhood | Mean patronage | Std. Deviation | Std. Error | F | Sig | Tukey B Post-hoc comparison test | |
|---|---|---|---|---|---|---|---|---|
Sub-set 1 | Sub -set 2 | |||||||
Dispensary | Slum settlement | 2.6873 | .98766 | .03986 | 9.194 | 0.000** | 2.6873 | |
Slum/informal settlement | 2.6378 | 1.04479 | .04392 | 2.6378 | ||||
Informal settlement | 3.1520 | 1.07054 | .09575 | 3.1520 | ||||
Total | 2.7156 | 1.02162 | .02741 | |||||
Primary Healthcare Centre | Slum settlement | 3.3844 | .84654 | .03416 | 3.235 | 0.022** | 3.3844 | |
Slum/informal settlement | 3.3799 | .96609 | .04061 | 3.3799 | ||||
Informal settlement | 3.1360 | .96172 | .08602 | 3.1360 | ||||
Total | 3.3657 | .90715 | .02434 | |||||
General Hospital | Slum settlement | 2.4837 | .96203 | .03882 | .910 | 0.436 | 2.4837 | |
Slum/informal settlement | 2.4240 | .88870 | .03735 | 2.4240 | ||||
Informal settlement | 2.4480 | 1.02749 | .09190 | 2.4480 | ||||
Total | 2.4622 | .93108 | .02498 | |||||
Tertiary Hospital | Slum settlement | 1.6401 | .88069 | .03554 | 3.994 | 0.008** | 1.6401 | |
Slum/informal settlement | 1.6696 | .96231 | .04045 | 1.6696 | ||||
Informal settlement | 1.8880 | .99366 | .08888 | 1.8880 | ||||
Total | 1.6904 | .94094 | .02525 | |||||
Specialist Hospital | Slum settlement | 1.5554 | .89189 | .03599 | 9.226 | 0.000** | 1.5554 | |
Slum/informal settlement | 1.6643 | 1.02207 | .04296 | 1.6643 | ||||
Informal settlement | 2.0320 | 1.17731 | .10530 | 2.0320 | ||||
Total | 1.6602 | .99480 | .02669 | |||||
Type of health facility | Neighbourhood | Chi-square (X) | Sig | |||
|---|---|---|---|---|---|---|
Slum settlement | Slum/informal settlement | Informal settlement | Total | |||
Dispensary/clinic | 160 | 143 | 84 | 387 | 134.323a | .000 |
41.3% | 37.0% | 21.8% | 100.0% | |||
Primary health centre | 308 | 342 | 93 | 743 | ||
41.5% | 46.0% | 12.5% | 100.0% | |||
General Hospital | 81 | 45 | 15 | 141 | ||
57.4% | 31.9% | 10.6% | 100.0% | |||
Teaching Hospital | 1 | 5 | 55 | 61 | ||
1.6% | 8.2% | 90.2% | 100.0% | |||
Specialist Hospital | 9 | 31 | 16 | 56 | ||
16.1% | 55.4% | 28.6% | 100.0% | |||
Total | 613 | 566 | 209 | 1388 | ||
44.2% | 40.8% | 15.1% | 100.0% | |||
| [1] |
Adebayo AM, Asuzu MC. (2015). Utilisation of a community-based health facility in a low-income urban community in Ibadan, Nigeria. African Journal of Primary Health Care & Family Medicine. (1).
https://doi.org/10.4102/phcfm.v7i1.735 PMID: 26245600; PMCID: PMC4564905. |
| [2] | Ajibade, F. O., & Ogunmola, J. O. (2020). Spatial analysis of healthcare facilities distribution and accessibility in Ibadan, Nigeria. International Journal of Health Geographics, 19(1), 1-16. |
| [3] | Akintola, F. O. 1994. Flooding Phenomenon in Ibadan Region. In Ibadan Region, edited by M. O. Filani, 244–255. Ibadan: Rex Charles Publications & Connel Publications. |
| [4] | Ayiti, O. M. (2024). Impacts of Decaying Infrastructure in Urban Areas of Ibadan, Oyo State, Nigeria. International Journal of Academic Research in Public Policy and Governace, 10(1), 1–10. |
| [5] | Babalola, S., & Fakayode, O. (2019). Urban slums and informal settlements in Ibadan: Implications for sustainable development. Journal of Sustainable Development in Africa, 21(4), 62-80. |
| [6] | Fayehun O., Ajisola M., Uthman O., Oyebode O., Oladejo A., Taiwo O., Odunbanjo, O., Harris B., Lilford R., Omigbodun. (2022). A contextual exploration of healthcare service use in urban slums in Nigeria. |
| [7] | Gidado, S. O., & Ayanwale, A. B. (2022). Patronage patterns of healthcare facilities among urban slum residents in Ibadan Metropolis, Nigeria. Nigerian Journal of Health Sciences, 20(1), 45-57. |
| [8] | Jazat Joseph P., Ogunbode Timothy O.,. Akande John A (2023). Assessment of sociological indices affecting environmental pollution in Iwo, Nigeria. Environmental Quality Management Volume 33, Issue 1 p. 157-164. |
| [9] | Jelili M. O. (2006). Environmental and Socio-economic Dimension of Begging in Ogbomoso and Ilorin; Unpublished M. Tech Dissertation, Ladoke Akintola University of Technology (LAUTECH), Ogbomoso. |
| [10] | Ogunmola, J. O., & Oladosu, Y. S. (2021). Accessibility to healthcare services and its implications for health outcomes in urban slums: A case study of Ibadan Metropolis, Nigeria. African Geographical Review, 40(2), 212-229. |
| [11] | Olaniyan, O. S., & Omotosho, B. A. (2018). Healthcare-seeking behavior among residents of urban slums in Ibadan Metropolis, Nigeria. Journal of Public Health in Africa, 9(2), 785-797. |
| [12] | Olugbamila, O. B. (2018). “Spatial Distribution and Accessibility to Healthcare Facilities in Akure South Local Government Area of Ondo State,”AnaleleUniversitatii din Oradea, Seria Geografie, Vol. 28, Issue. 1, pp. 7-18. |
| [13] | Patel, S., Sandbrook, C., & Fisher, J. (2011). Addressing urban poverty in the global South: Experiences from the urban poor in the Eastern Cape, South Africa. Urban Forum, 22(3), 253-270. |
APA Style
Adejare, J. A., Jelili, M. O., Muili, A. B. (2024). Patronage Pattern and Accessibility of Healthcare Facilities in Urban Slums and Informal Settlements in Ibadan Metropolis. Urban and Regional Planning, 9(3), 71-87. https://doi.org/10.11648/j.urp.20240903.12
ACS Style
Adejare, J. A.; Jelili, M. O.; Muili, A. B. Patronage Pattern and Accessibility of Healthcare Facilities in Urban Slums and Informal Settlements in Ibadan Metropolis. Urban Reg. Plan. 2024, 9(3), 71-87. doi: 10.11648/j.urp.20240903.12
AMA Style
Adejare JA, Jelili MO, Muili AB. Patronage Pattern and Accessibility of Healthcare Facilities in Urban Slums and Informal Settlements in Ibadan Metropolis. Urban Reg Plan. 2024;9(3):71-87. doi: 10.11648/j.urp.20240903.12
@article{10.11648/j.urp.20240903.12,
author = {Jacob Ayorinde Adejare and Musibau Omoakin Jelili and Akeem Bamidele Muili},
title = {Patronage Pattern and Accessibility of Healthcare Facilities in Urban Slums and Informal Settlements in Ibadan Metropolis
},
journal = {Urban and Regional Planning},
volume = {9},
number = {3},
pages = {71-87},
doi = {10.11648/j.urp.20240903.12},
url = {https://doi.org/10.11648/j.urp.20240903.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.urp.20240903.12},
abstract = {Slums and informal settlements are residential areas physically and socially disintegrated. In spite of this, inadequate health-related data on slum areas and informal settlements has led to inappropriate and unrealistic allocation of healthcare resources by the public and private health providers. This study investigates the patronage pattern and accessibility of healthcare facilities to residents of urban slums and Informal settlements in Ibadan Metropolis, a rapidly growing urban area in Nigeria facing challenges related to urbanization and healthcare infrastructure. Data were collected from both primary and secondary sources. Structured questionnaire was administered on 1,389 residents of the slummy neighbourhoods and informal settlements in Ibadan metropolis, and obtained data were analyzed using descriptive and inferential statistics. Results revealed that out of 109 neighbourhoods, 42.1% were categorized as slummy neighbourhoods, 36.7% as slums/informal settlements, while 21.2% were informal settlement using slummy and informality conditions respectively. Results revealed that distance to health facility (β= -0.353, p<0.05), educational qualification (β=-0.063, p<0.05) and household size (β= -0.052, p<0.05) had an inverse relationship with patronage of health facilities, while age (β=0.086, p< 0.05) had a positive relationship. It was also revealed that access to PHC and dispensary/clinic in slummy neighbouhoods and slum/informal settlements is higher compared to informal settlements in the study area. The study therefore recommends implementation of slum improvement program for the slummy and slums/informal neighbourhoods, provision of additional healthcare facilities to be located especially in the slummy neighbourhoods and informal settlements to ensure equitable distribution.
},
year = {2024}
}
TY - JOUR T1 - Patronage Pattern and Accessibility of Healthcare Facilities in Urban Slums and Informal Settlements in Ibadan Metropolis AU - Jacob Ayorinde Adejare AU - Musibau Omoakin Jelili AU - Akeem Bamidele Muili Y1 - 2024/07/29 PY - 2024 N1 - https://doi.org/10.11648/j.urp.20240903.12 DO - 10.11648/j.urp.20240903.12 T2 - Urban and Regional Planning JF - Urban and Regional Planning JO - Urban and Regional Planning SP - 71 EP - 87 PB - Science Publishing Group SN - 2575-1697 UR - https://doi.org/10.11648/j.urp.20240903.12 AB - Slums and informal settlements are residential areas physically and socially disintegrated. In spite of this, inadequate health-related data on slum areas and informal settlements has led to inappropriate and unrealistic allocation of healthcare resources by the public and private health providers. This study investigates the patronage pattern and accessibility of healthcare facilities to residents of urban slums and Informal settlements in Ibadan Metropolis, a rapidly growing urban area in Nigeria facing challenges related to urbanization and healthcare infrastructure. Data were collected from both primary and secondary sources. Structured questionnaire was administered on 1,389 residents of the slummy neighbourhoods and informal settlements in Ibadan metropolis, and obtained data were analyzed using descriptive and inferential statistics. Results revealed that out of 109 neighbourhoods, 42.1% were categorized as slummy neighbourhoods, 36.7% as slums/informal settlements, while 21.2% were informal settlement using slummy and informality conditions respectively. Results revealed that distance to health facility (β= -0.353, p<0.05), educational qualification (β=-0.063, p<0.05) and household size (β= -0.052, p<0.05) had an inverse relationship with patronage of health facilities, while age (β=0.086, p< 0.05) had a positive relationship. It was also revealed that access to PHC and dispensary/clinic in slummy neighbouhoods and slum/informal settlements is higher compared to informal settlements in the study area. The study therefore recommends implementation of slum improvement program for the slummy and slums/informal neighbourhoods, provision of additional healthcare facilities to be located especially in the slummy neighbourhoods and informal settlements to ensure equitable distribution. VL - 9 IS - 3 ER -
Department of Urban and Regional Planning, Ladoke Akintola University of Technology, Ogbomoso, Nigeria
Department of Urban and Regional Planning, Ladoke Akintola University of Technology, Ogbomoso, Nigeria
Department of Urban and Regional Planning, Ladoke Akintola University of Technology, Ogbomoso, Nigeria
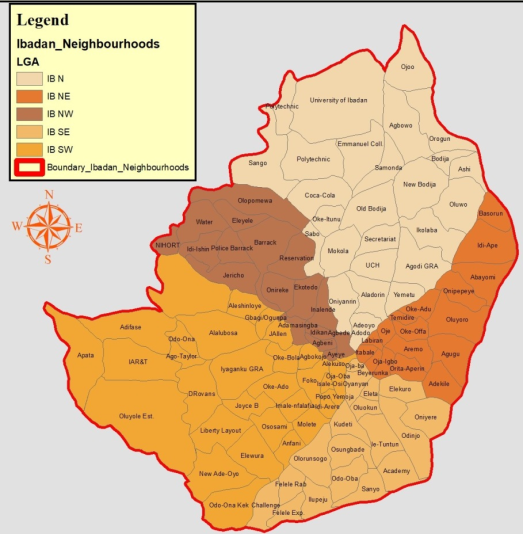
Figure 1. Five Urban Local Government Areas of Ibadan City and the respective Neighbourhoods.
Figure 2. Urban City System.
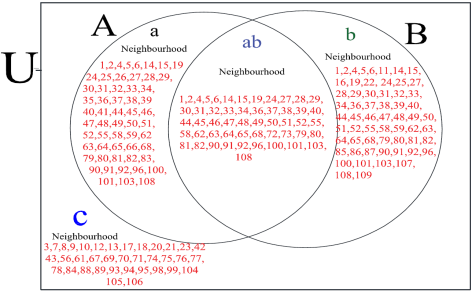
Figure 3. Categorization of Urban Neighborhoods into Slums and Informal Settlements within Ibadan Metropolis (Neigh. 1-109).

Figure 4. Slum Neighbourhood in Bere, Ibadan.

Figure 5. Informal Settlement at Molete, Ibadan.
Information

