Pulmonary alveolar microlithiasis (PAM) is one of the rare lung diseases, in which an otherwise healthy individual develops diffuse alveolar calcifications. It is reported to be caused by mutation of the SLC34A2 gene. Patients who are eventually diagnosed with PAM usually present late when progression to cor pulmonale has already developed, or for other reasons not related to the disease itself when their clinical work up results incidentally reveal much worse findings than the patient’s actual state. Unlike the familiar information that no effective treatment other than lung transplant, cardiokinetics, diuretics, oxygen, and repeated bronchoalveolar lavage were reported with relatively satisfactory results and chest X-ray changes. In this report, we focus on the relation between clinical, radiologic and histologic findings, in which clinical scenario was first mistaken for interstitial fibrosis or suspected metastasis, and on literature review. Chest radiography, bronchoalveolar lavage and lung wedge biopsy were the main steps to reach the diagnosis of PAM. Gradual improvement after conservative treatment was noted prior to discharge. Then clinic appointment for follow up and family members surveillance was scheduled. A rare disease incidentally diagnosed by high awareness of the attending physician and simple methods that points to a question of disease prevalence in Jordan.
| Published in | Science Journal of Clinical Medicine (Volume 13, Issue 4) |
| DOI | 10.11648/j.sjcm.20241304.13 |
| Page(s) | 76-80 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Lung Calcification, Pulmonary Alveolar Microlithiasis, Stone Lung
PAM | Pulmonary Alveolar Microlithiasis |
CT | Computed Tomography |
BAL | Bronchoalveolar Lavage |
HRCT | High Resolution Computed Tomography |
| [1] | Haddad RM, Al-Momani JA, Al-Omari AH, AlSuleihat AS, Alnadi KM, Alsaidah N, Alelaimat AF, Obeidat TA. Pulmonary Alveolar Microlithiasis: a Case Report in King Hussein Medical Center (KHMC), Amman, Jordan. Med Arch. 2020 Feb; 74(1): 69-72. |
| [2] | Jindal A, Rahulan V, Balasubramani G, Dutta P, Attawar S. Pulmonary alveolar microlithiasis: A rare disease treated with lung transplantation, first case from India. Lung India. 2019 Nov-Dec; 36(6): 546-549. |
| [3] | Puhr L. Microlithiasis alveolaris pulmonum. Virchows Arch Pathol Anat. 1933; 290: 156–160. |
| [4] | Kashyap S, Mohapatra PR. Pulmonary alveolar microlithiasis. Lung India. 2013 Apr; 30(2): 143-7. |
| [5] | Nicholson, A. G., & Rice, A. J. (2013). Chapter 10 Interstitial lung diseases/Pulmonary alveolar microlithiasis. In Spencer’s Pathology of the Lung (Sixth Edition, pp. 394–394). essay, CAMBRIDGE UNIVERSITY PRESS. |
| [6] | Enemark A, Jönsson ÅLM, Kronborg-White S, Bendstrup E. Pulmonary Alveolar Microlithiasis - A Review. Yale J Biol Med. 2021 Dec 29; 94(4): 637-644. PMID: 34970102; PMCID: PMC8686773. |
| [7] | de Oliveira Mekonnen A, Schwerk N, Schütz K, Schramm L, Dreissig A, Grewendorf S, Sukdolak C, Dopfer C, Auber B, von Hardenberg S, Happle C. Pulmonary Alveolar Microlithiasis: A novel patient and brief review of the literature. Klin Padiatr. 2022 Sep; 234(5): 317-319. English. |
| [8] | Shaw BM, Shaw SD, McCormack FX. Pulmonary Alveolar Microlithiasis. Semin Respir Crit Care Med. 2020 Apr; 41(2): 280-287. |
| [9] | Saito A, McCormack FX. Pulmonary Alveolar Microlithiasis. Clin Chest Med. 2016 Sep; 37(3): 441-8. |
| [10] | Kosciuk P, Meyer C, Wikenheiser-Brokamp KA, McCormack FX. Pulmonary alveolar microlithiasis. Eur Respir Rev. 2020 Nov 27; 29(158): 200024. |
| [11] | Tachibana T, Hagiwara K, Johkoh T. Pulmonary alveolar microlithiasis: Review and management. Curr Opin Pulm Med. 2009; 15: 486–90. |
| [12] | Castellana G, Castellana G, Gentile M, Castellana R, Resta O. Pulmonary alveolar microlithiasis: Review of the 1022 cases reported worldwide. Eur Respir Rev. 2015; 24: 607–20. |
| [13] | Jönsson ÅL, Simonsen U, Hilberg O, Bendstrup E. Pulmonary alveolar microlithiasis: Two case reports and review of the literature. Eur Respir Rev. 2012; 21: 249–256. |
| [14] | Mariotta S, Guidi L, Mattia P, et al. Pulmonary microlithiasis. Report of two cases. Respiration. 1997; 64(2): 165–169. |
| [15] | Ferreira Francisco FA, Pereira e Silva JL, Hochhegger B, Zanetti G, Marchiori E. Pulmonary alveolar microlithiasis. State-of-the-art review. Respir Med. 2013 Jan; 107(1): 1-9. |
APA Style
Alakhras, B. R., Habashneh, O., Yaghi, A. B., Daseh, A., Alkilani, A. (2024). Pulmonary Alveolar Microlithiasis: An Incidental Case Report from Jordan with Literature Review. Science Journal of Clinical Medicine, 13(4), 76-80. https://doi.org/10.11648/j.sjcm.20241304.13
ACS Style
Alakhras, B. R.; Habashneh, O.; Yaghi, A. B.; Daseh, A.; Alkilani, A. Pulmonary Alveolar Microlithiasis: An Incidental Case Report from Jordan with Literature Review. Sci. J. Clin. Med. 2024, 13(4), 76-80. doi: 10.11648/j.sjcm.20241304.13
AMA Style
Alakhras BR, Habashneh O, Yaghi AB, Daseh A, Alkilani A. Pulmonary Alveolar Microlithiasis: An Incidental Case Report from Jordan with Literature Review. Sci J Clin Med. 2024;13(4):76-80. doi: 10.11648/j.sjcm.20241304.13
@article{10.11648/j.sjcm.20241304.13,
author = {Basheer Radi Alakhras and Omar Habashneh and Ahmad Basim Yaghi and Abdallah Daseh and Adham Alkilani},
title = {Pulmonary Alveolar Microlithiasis: An Incidental Case Report from Jordan with Literature Review
},
journal = {Science Journal of Clinical Medicine},
volume = {13},
number = {4},
pages = {76-80},
doi = {10.11648/j.sjcm.20241304.13},
url = {https://doi.org/10.11648/j.sjcm.20241304.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjcm.20241304.13},
abstract = {Pulmonary alveolar microlithiasis (PAM) is one of the rare lung diseases, in which an otherwise healthy individual develops diffuse alveolar calcifications. It is reported to be caused by mutation of the SLC34A2 gene. Patients who are eventually diagnosed with PAM usually present late when progression to cor pulmonale has already developed, or for other reasons not related to the disease itself when their clinical work up results incidentally reveal much worse findings than the patient’s actual state. Unlike the familiar information that no effective treatment other than lung transplant, cardiokinetics, diuretics, oxygen, and repeated bronchoalveolar lavage were reported with relatively satisfactory results and chest X-ray changes. In this report, we focus on the relation between clinical, radiologic and histologic findings, in which clinical scenario was first mistaken for interstitial fibrosis or suspected metastasis, and on literature review. Chest radiography, bronchoalveolar lavage and lung wedge biopsy were the main steps to reach the diagnosis of PAM. Gradual improvement after conservative treatment was noted prior to discharge. Then clinic appointment for follow up and family members surveillance was scheduled. A rare disease incidentally diagnosed by high awareness of the attending physician and simple methods that points to a question of disease prevalence in Jordan.
},
year = {2024}
}
TY - JOUR T1 - Pulmonary Alveolar Microlithiasis: An Incidental Case Report from Jordan with Literature Review AU - Basheer Radi Alakhras AU - Omar Habashneh AU - Ahmad Basim Yaghi AU - Abdallah Daseh AU - Adham Alkilani Y1 - 2024/12/16 PY - 2024 N1 - https://doi.org/10.11648/j.sjcm.20241304.13 DO - 10.11648/j.sjcm.20241304.13 T2 - Science Journal of Clinical Medicine JF - Science Journal of Clinical Medicine JO - Science Journal of Clinical Medicine SP - 76 EP - 80 PB - Science Publishing Group SN - 2327-2732 UR - https://doi.org/10.11648/j.sjcm.20241304.13 AB - Pulmonary alveolar microlithiasis (PAM) is one of the rare lung diseases, in which an otherwise healthy individual develops diffuse alveolar calcifications. It is reported to be caused by mutation of the SLC34A2 gene. Patients who are eventually diagnosed with PAM usually present late when progression to cor pulmonale has already developed, or for other reasons not related to the disease itself when their clinical work up results incidentally reveal much worse findings than the patient’s actual state. Unlike the familiar information that no effective treatment other than lung transplant, cardiokinetics, diuretics, oxygen, and repeated bronchoalveolar lavage were reported with relatively satisfactory results and chest X-ray changes. In this report, we focus on the relation between clinical, radiologic and histologic findings, in which clinical scenario was first mistaken for interstitial fibrosis or suspected metastasis, and on literature review. Chest radiography, bronchoalveolar lavage and lung wedge biopsy were the main steps to reach the diagnosis of PAM. Gradual improvement after conservative treatment was noted prior to discharge. Then clinic appointment for follow up and family members surveillance was scheduled. A rare disease incidentally diagnosed by high awareness of the attending physician and simple methods that points to a question of disease prevalence in Jordan. VL - 13 IS - 4 ER -
Pathology Department, Albasheer Hospital, Amman, Jordan
Pathology Department, Albasheer Hospital, Amman, Jordan
Radiology Department, Albasheer Hospital, Amman, Jordan
Faculty of Medicine, Hashemite University, Zarqa, Jordan
Department of General Surgery, Albasheer Hospital, Amman, Jordan
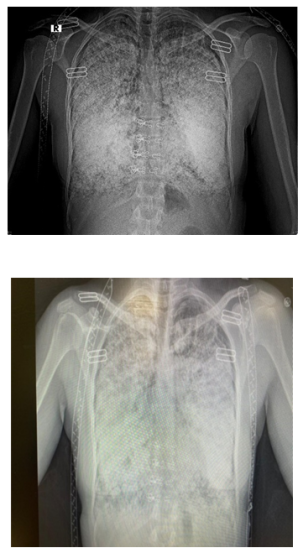
Figure 1. Chest x-ray images showing sand storm appearance in both lung fields.
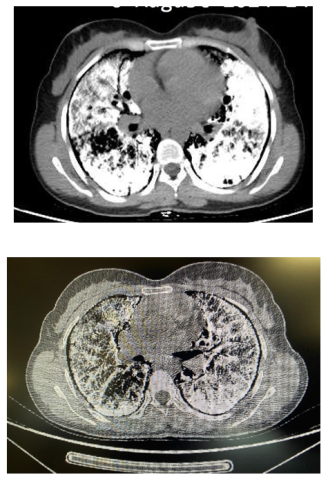
Figure 2. HRCT showing extensive sand-like calcifications of the lung parenchyma with the black pleura sign.

Figure 3. 40x magnification of lung tissue showing diffuse alveolar basophilic calcifications.
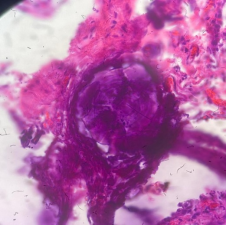
Figure 4. 400x magnification of the concentric laminated calcified concretions.
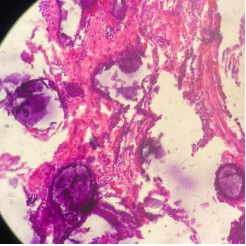
Figure 5. 100x magnification showing interstitial fibrosis and minimal inflammation with intra-alveolar calcifications.
Information

