Background: In areas with poor vaccination rates, diphtheria, a dangerous acute infectious disease brought on by Corynebacterium diphtheria, remains a threat. Due to low vaccination uptake and undeveloped immunity, children under five are especially at risk. Objective: risk factors and describing the clinical characteristics of diphtheria in children under five who were enrolled in De Martino Hospital in Mogadishu were the objectives of this study. Methods: Eighty confirmed cases of diphtheria participated in a descriptive cross-sectional investigation. Structured questionnaires and a review of medical records were used to gather data. Age, gender, immunization status, clinical characteristics, complications, and results were among the variables evaluated. Findings: Of the 80 children, 43.8% were younger than two years old, and 35.0% were between three and four years old. With 50.0% of the population being female and 48.8% being male, the gender distribution was almost equal. Only 15.0% of people were fully vaccinated, 21.3% were partially vaccinated, and 63.8% were not immunized. The two most common symptoms were fever (100%) and sore throat (100%). The following conditions were also quite common: dysphagia (93.8%), respiratory distress (98.8%), cervical lymphadenopathy (96.3%), and pseudo membrane development (98.8%). 25% of patients had myocarditis, and 75% of patients experienced respiratory problems. Residence of the patients (45.0%) resided in Yaqshid, followed by 16.3% from Karaan and 8.8% from Shibis. Smaller proportions of patients came from Dharkenley (6.3%), Celasha Biyaha (5.0%), Deynile (3.8%), Hodan (3.8%), and other areas including Kaxda, Hilwa, Sh. Dhexe, Hirshabele, Balcad, and Tabelaha, each contributing 2.5% to 1.3% of cases. This distribution indicates that Yaqshiid and Karaan were the most affected areas, suggesting a potential geographic clustering of cases., 76.3% recovered from the disease, while 23.8% did not. 77.5% was survived, while 22.5% was died, children who were not vaccinated having a higher death rate. Conclusion: diphtheria is still a serious public health issue in Somalia affecting children under five. The most frequent clinical symptoms were fever, sore throat, and pseudo membrane formation, while the main risk factors were found to be incomplete immunization, malnutrition, and delayed healthcare-seeking behavior. Improved immunization campaigns, early diagnosis, and prompt treatment treatments are critically needed, as highlighted by the high case fatality rate.
| Published in | Science Discovery Medicine (Volume 1, Issue 1) |
| DOI | 10.11648/j.sdmed.20260101.11 |
| Page(s) | 1-6 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Diphtheria, Outbreak, Risk Factors, Children Under Five, Demertinho, Mogadishu, Somalia
Clinical presentation of Diphtheria patients | Frequency | Percentages % | |
|---|---|---|---|
fever of the patient | yes | 80 | 100.0% |
no | 0 | 0.0% | |
sore throat of the patient | yes | 80 | 100.0% |
no | 0 | 0.0% | |
pseudo membranous formation of the patient | yes | 79 | 98.8% |
no | 1 | 1.3% | |
cervical lymphadenopathy of the patient | yes | 77 | 96.3% |
no | 3 | 3.8% | |
difficult breathing of the patient | yes | 79 | 98.8% |
no | 1 | 1.3% | |
dysphagia of the patient | yes | 75 | 93.8% |
no | 5 | 6.3% | |
Risk factors of Diphtheria of Diphtheria | Frequency | Percentages % | |
|---|---|---|---|
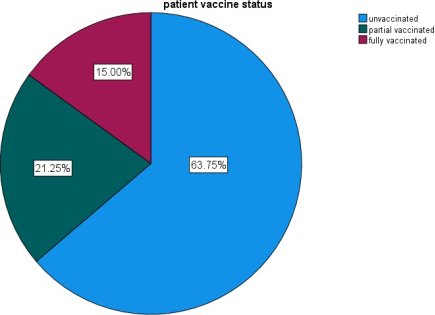
Patient vaccine status | Unvaccinated | 51 | 63.7% |
Partial vaccinated | 17 | 21.3% | |
Fully vaccinated | 12 | 15.0% | |
Travel history | No | 16 | 20.0% |
Yes | 64 | 80.0% | |
Contact history | No | 26 | 32.5% |
Yes | 54 | 67.5% | |
WHO | World Health Organization |
CFR | Case Fatality Rate |
EPI | Expanded Programme on Immunization |
VPD | Vaccine-Preventable Disease |
SPSS | Statistical Package for the Social Sciences |
PENTA | Pentavalent Vaccine |
DTP3 | Diphtheria-Tetanus-Pertussis Vaccine (3rd Dose) |
NIS | Newly Independent States |
SAM | Severe Acute Malnutrition |
| [1] | Centers for Disease Control and Prevention. (2024). Diphtheria. |
| [2] | World Health Organization. (2024). Diphtheria fact sheet. |
| [3] | Brown, K., & Lee, T. (2022). Clinical features of diphtheria in pediatric patients. Pediatric Infectious Disease Journal, 41(4), 312–318. |
| [4] | Mohamed, A., & Hassan, M. (2025). Childhood diphtheria in Somalia: Challenges and solutions. Somalia Medical Journal, 12(1), 45–53. |
| [5] |
Susanti R, Ifroh RH, Noviasty R, Muhamad Ramdan I, Susanti R, Ifroh RH, et al. Risk factors for diphtheria outbreak in children aged 1-10 years in East Kalimantan Province, Indonesia [version 1; peer review: 2 approved] Iwan Muhamad Ramdan. F1000 Research. 2019; 7(0): 1–10. Available from:
https://www.cdc.gov/diphtheria/about/diagnosis-treatment.html |
| [6] | Murhekar M V., Bitragunta S. Persistence of diphtheria in India. Indian J Community Med. 2011; 36(2): 164–5. |
| [7] | Bisgard KM, Rhodes P, Hardy IRB, Litkina IL, Filatov NN, Monisov AA, et al. Diphtheria Toxoid Vaccine Effectiveness: A Case-Control Study in Russia. J Infect Dis. 2000 Feb 1; 181(Supplement_1): S184–7. Available from: |
| [8] | Ramdan IM, Susanti R, Ifroh RH, Noviasty R. Risk factors for diphtheria outbreak in children aged 1-10 years in East Kalimantan Province, Indonesia. F1000 Research. 2018; 7(May): 1–10. |
| [9] | Rintani A, Mintarsih T, Rbm YM, Siregar JS, Widodo AP, Biasa L, et al. Risk Factors Associated To Diphtheria Outbreak in Developing Countries Faktor-Faktor Risiko Yang Berhubungan Dengan Kejadian. 2018; 9(2): 83–95. |
| [10] | Garib Z, Danovaro-Holliday MC, Tavarez Y, Leal I, Pedreira C. Diphtheria in the Dominican Republic: reduction of cases following a large outbreak. Rev Panam Salud Publica. 2015 Oct; 38(4): 292–9. |
| [11] | Sadoh A, Sadoh W. Diphtheria mortality in Nigeria: the need to stock diphtheria antitoxin. African J Clin Exp Microbiol. 2011; 12(2): 82–5. |
| [12] | Gowin E, Wysocki J, Kaluzna E, Swiatek-Koscielna B, Wysocka-Leszczynska J, Michalak M, et al. Does vaccination ensure protection? Assessing diphtheria and tetanus antibody levels in a population of healthy children: A cross-sectional study. Med (United States). 2016; 95(49): e5571. |
| [13] | Patil N, Gawade N, Gaidhane A, Syed Z. Investigating diphtheria outbreak: A qualitative study in rural area. Int J Med Sci Public Heal. 2014; 3(4): 513. |
| [14] | Castelli F, Sulis G. Migration and infectious diseases. Clin Microbiol Infect [Internet]. 2017; 23(5): 283–9. Available from: |
| [15] | Husada D, Primayani D, Marbun K, Kartina L, Puspitasari D, Tirthaningsih NW, et al. Risk factors of diphtheria carriers in Indonesian children. Southeast Asian J Trop Med Public Health. 2018; 49(4): 660–9. |
| [16] | Shedaiwah S, Alsharabi H, Anam L, Al Amad MA. Risk factors of diphtheria outbreak in damt district of Al Dhalea Governorate, 2023 -Yemen: a case–control study. BMC Infect Dis. 2024; 24(1). Available from: |
| [17] | Arguni E, Karyanti MR, Satari HI, Hadinegoro SR. Diphtheria outbreak in Jakarta and Tangerang, Indonesia: Epidemiological and clinical predictor factors for death. PLoS One. 2021; 16(2 February): 1–11. Available from: |
| [18] | Harapan H, Anwar S, Dimiati H, Hayati Z, Mudatsir M. Diphtheria outbreak in Indonesia, 2017: An outbreak of an ancient and vaccine-preventable disease in the third millennium. Clin Epidemiol Glob Heal. 2019; 7(2): 261–2. Available from: |
| [19] | Oduoye MO, Musa ZM, Tunde AM, Nazir A, Cakwira H, Abdulkareem L, et al. The recent outbreak of diphtheria in Nigeria is a public health concern for all. Int J Surg Glob Heal. 2023; 6(5). |
APA Style
Abshir, S. A., Mahamuud, I. M., Mahamuud, F. A., Sheikhow, M. G. (2026). Risk Factors Associated with Diphtheria Outbreak Among Patients Under 5 Years Attending de Martino Hospital Mogadishu, Somalia. Science Discovery Medicine, 1(1), 1-6. https://doi.org/10.11648/j.sdmed.20260101.11
ACS Style
Abshir, S. A.; Mahamuud, I. M.; Mahamuud, F. A.; Sheikhow, M. G. Risk Factors Associated with Diphtheria Outbreak Among Patients Under 5 Years Attending de Martino Hospital Mogadishu, Somalia. Sci. Discov. Med. 2026, 1(1), 1-6. doi: 10.11648/j.sdmed.20260101.11
@article{10.11648/j.sdmed.20260101.11,
author = {Saciid Abdullahi Abshir and Ibrahim Mahamud Mahamuud and Faduma Ahmed Mahamuud and Mohamed Gedi Sheikhow},
title = {Risk Factors Associated with Diphtheria Outbreak Among Patients Under 5 Years Attending de Martino Hospital Mogadishu, Somalia},
journal = {Science Discovery Medicine},
volume = {1},
number = {1},
pages = {1-6},
doi = {10.11648/j.sdmed.20260101.11},
url = {https://doi.org/10.11648/j.sdmed.20260101.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sdmed.20260101.11},
abstract = {Background: In areas with poor vaccination rates, diphtheria, a dangerous acute infectious disease brought on by Corynebacterium diphtheria, remains a threat. Due to low vaccination uptake and undeveloped immunity, children under five are especially at risk. Objective: risk factors and describing the clinical characteristics of diphtheria in children under five who were enrolled in De Martino Hospital in Mogadishu were the objectives of this study. Methods: Eighty confirmed cases of diphtheria participated in a descriptive cross-sectional investigation. Structured questionnaires and a review of medical records were used to gather data. Age, gender, immunization status, clinical characteristics, complications, and results were among the variables evaluated. Findings: Of the 80 children, 43.8% were younger than two years old, and 35.0% were between three and four years old. With 50.0% of the population being female and 48.8% being male, the gender distribution was almost equal. Only 15.0% of people were fully vaccinated, 21.3% were partially vaccinated, and 63.8% were not immunized. The two most common symptoms were fever (100%) and sore throat (100%). The following conditions were also quite common: dysphagia (93.8%), respiratory distress (98.8%), cervical lymphadenopathy (96.3%), and pseudo membrane development (98.8%). 25% of patients had myocarditis, and 75% of patients experienced respiratory problems. Residence of the patients (45.0%) resided in Yaqshid, followed by 16.3% from Karaan and 8.8% from Shibis. Smaller proportions of patients came from Dharkenley (6.3%), Celasha Biyaha (5.0%), Deynile (3.8%), Hodan (3.8%), and other areas including Kaxda, Hilwa, Sh. Dhexe, Hirshabele, Balcad, and Tabelaha, each contributing 2.5% to 1.3% of cases. This distribution indicates that Yaqshiid and Karaan were the most affected areas, suggesting a potential geographic clustering of cases., 76.3% recovered from the disease, while 23.8% did not. 77.5% was survived, while 22.5% was died, children who were not vaccinated having a higher death rate. Conclusion: diphtheria is still a serious public health issue in Somalia affecting children under five. The most frequent clinical symptoms were fever, sore throat, and pseudo membrane formation, while the main risk factors were found to be incomplete immunization, malnutrition, and delayed healthcare-seeking behavior. Improved immunization campaigns, early diagnosis, and prompt treatment treatments are critically needed, as highlighted by the high case fatality rate.},
year = {2026}
}
TY - JOUR T1 - Risk Factors Associated with Diphtheria Outbreak Among Patients Under 5 Years Attending de Martino Hospital Mogadishu, Somalia AU - Saciid Abdullahi Abshir AU - Ibrahim Mahamud Mahamuud AU - Faduma Ahmed Mahamuud AU - Mohamed Gedi Sheikhow Y1 - 2026/02/25 PY - 2026 N1 - https://doi.org/10.11648/j.sdmed.20260101.11 DO - 10.11648/j.sdmed.20260101.11 T2 - Science Discovery Medicine JF - Science Discovery Medicine JO - Science Discovery Medicine SP - 1 EP - 6 PB - Science Publishing Group UR - https://doi.org/10.11648/j.sdmed.20260101.11 AB - Background: In areas with poor vaccination rates, diphtheria, a dangerous acute infectious disease brought on by Corynebacterium diphtheria, remains a threat. Due to low vaccination uptake and undeveloped immunity, children under five are especially at risk. Objective: risk factors and describing the clinical characteristics of diphtheria in children under five who were enrolled in De Martino Hospital in Mogadishu were the objectives of this study. Methods: Eighty confirmed cases of diphtheria participated in a descriptive cross-sectional investigation. Structured questionnaires and a review of medical records were used to gather data. Age, gender, immunization status, clinical characteristics, complications, and results were among the variables evaluated. Findings: Of the 80 children, 43.8% were younger than two years old, and 35.0% were between three and four years old. With 50.0% of the population being female and 48.8% being male, the gender distribution was almost equal. Only 15.0% of people were fully vaccinated, 21.3% were partially vaccinated, and 63.8% were not immunized. The two most common symptoms were fever (100%) and sore throat (100%). The following conditions were also quite common: dysphagia (93.8%), respiratory distress (98.8%), cervical lymphadenopathy (96.3%), and pseudo membrane development (98.8%). 25% of patients had myocarditis, and 75% of patients experienced respiratory problems. Residence of the patients (45.0%) resided in Yaqshid, followed by 16.3% from Karaan and 8.8% from Shibis. Smaller proportions of patients came from Dharkenley (6.3%), Celasha Biyaha (5.0%), Deynile (3.8%), Hodan (3.8%), and other areas including Kaxda, Hilwa, Sh. Dhexe, Hirshabele, Balcad, and Tabelaha, each contributing 2.5% to 1.3% of cases. This distribution indicates that Yaqshiid and Karaan were the most affected areas, suggesting a potential geographic clustering of cases., 76.3% recovered from the disease, while 23.8% did not. 77.5% was survived, while 22.5% was died, children who were not vaccinated having a higher death rate. Conclusion: diphtheria is still a serious public health issue in Somalia affecting children under five. The most frequent clinical symptoms were fever, sore throat, and pseudo membrane formation, while the main risk factors were found to be incomplete immunization, malnutrition, and delayed healthcare-seeking behavior. Improved immunization campaigns, early diagnosis, and prompt treatment treatments are critically needed, as highlighted by the high case fatality rate. VL - 1 IS - 1 ER -
School of Medicine and Surgery, University of Somalia, Mogadishu, Somalia
School of Medicine and Surgery, University of Somalia, Mogadishu, Somalia
School of Medicine and Surgery, University of Somalia, Mogadishu, Somalia
School of Medicine and Surgery, University of Somalia, Mogadishu, Somalia;School of Medicine and Surgery, Somaville University, Mogadishu, Somalia
Information