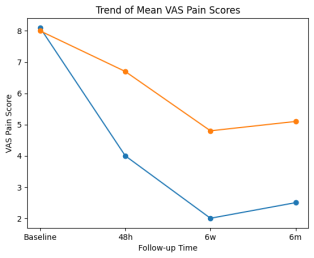
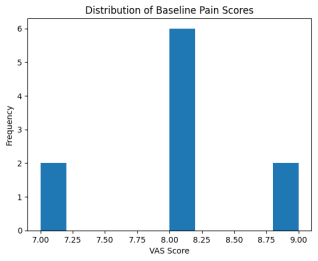
Myofascial pain syndrome (MPS) is one of the most common causes of chronic neck and shoulder pain encountered in clinical practice; however, despite its high prevalence, it is frequently underdiagnosed because of overlapping clinical presentations with other musculoskeletal and neurological disorders. The condition is characterized by hyperirritable trigger points within skeletal muscles that produce localized tenderness, referred pain, restricted mobility, and functional impairment. This prospective controlled observational study aimed to evaluate the clinical outcomes of aggressive multimodal therapy compared with conventional conservative treatment in patients with cervicothoracic MPS. Sixty patients diagnosed with cervicothoracic MPS were enrolled and allocated into two groups: Group A (n = 30) received aggressive multimodal therapy, while Group B (n = 30) received conventional conservative treatment. Baseline evaluation included assessment of pain intensity using the Visual Analog Scale (VAS), cervical range of motion measurements, and trigger point mapping, with follow-up assessments conducted at 48 hours, 6 weeks, and 6 months. Baseline pain intensity was comparable between the two groups, with mean VAS scores of 8.1 in Group A and 8.0 in Group B. The intervention group demonstrated significantly greater pain reduction at all follow-up time points, with mean VAS scores decreasing to 4.0 versus 6.7 at 48 hours, 2.0 versus 4.8 at 6 weeks, and 2.5 versus 5.1 at 6 months in Groups A and B, respectively. Significant clinical improvement was observed in 80% of patients receiving aggressive multimodal therapy compared with 40% of those receiving conventional treatment (p < 0.001). These findings suggest that aggressive multimodal therapy, consisting of trigger point injections and structured rehabilitation, provides superior pain relief and functional recovery compared with conventional conservative management in patients with cervicothoracic myofascial pain syndrome.
| Published in | Rehabilitation Science (Volume 11, Issue 2) |
| DOI | 10.11648/j.rs.20261102.12 |
| Page(s) | 37-43 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Myofascial Pain, Trigger Point Injection, Neck and Shoulder Pain, Posture, Pain
Group | Treatment | Patients |
|---|---|---|
Group A | Aggressive multimodal therapy | 30 |
Group B | Conventional conservative therapy | 30 |
Variable | Group A | Group B |
|---|---|---|
Patients | 30 | 30 |
Mean age | 38.6 ± 9.2 | 39.1 ± 8.7 |
Female | 21 (70%) | 20 (67%) |
Male | 9 (30%) | 10 (33%) |
Mean symptom duration | 15 ± 6 months | 14 ± 7 months |
Time | Group A | Group B |
|---|---|---|
Baseline | 8.1 | 8.0 |
48 hours | 4.0 | 6.7 |
6 weeks | 2.0 | 4.8 |
6 months | 2.5 | 5.1 |
Outcome | Group A | Group B |
|---|---|---|
Significant improvement | 24 (80%) | 12 (40%) |
Moderate improvement | 4 (13%) | 10 (33%) |
Mild improvement | 2 (7%) | 8 (27%) |
Outcome | Group A | Group B |
|---|---|---|
Improved ROM | 25 (83%) | 15 (50%) |
No change | 5 (17%) | 15 (50%) |
Variable | Beta | p-value |
|---|---|---|
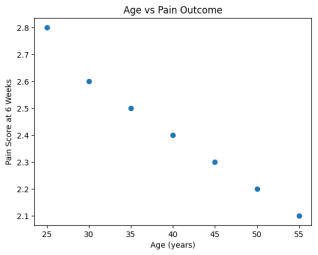
Age | 0.12 | 0.18 |
Baseline VAS | 0.44 | 0.01 |
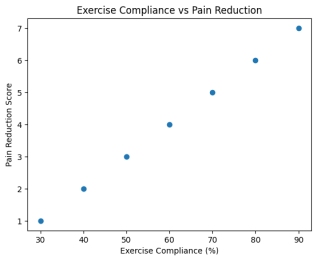
Exercise compliance | −0.56 | 0.003 |
Factor | Patients | Percentage |
|---|---|---|
Prolonged computer use | 16 | 53% |
Poor workstation ergonomics | 18 | 60% |
Forward head posture | 20 | 67% |
Smartphone overuse | 14 | 47% |
Overhead activity | 9 | 30% |
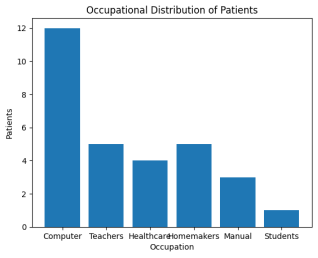
Occupation | Patients | Percentage |
|---|---|---|
Computer professionals | 12 | 40% |
Teachers | 5 | 17% |
Healthcare workers | 4 | 13% |
Homemakers | 5 | 17% |
Manual workers | 3 | 10% |
Students | 1 | 3% |
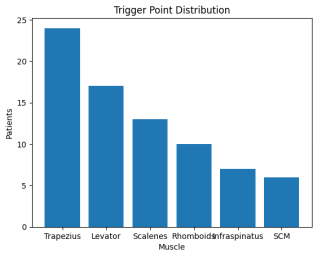
Muscle | Patients | Percentage |
|---|---|---|
Upper trapezius | 24 | 80% |
Levator scapulae | 17 | 57% |
Scalenes | 13 | 43% |
Rhomboids | 10 | 33% |
Infraspinatus | 7 | 23% |
Sternocleidomastoid | 6 | 20% |
MPS | Myofascial Pain Syndrome |
VAS | Visual Analog Scale |
NSAIDs | Nonsteroidal Anti-inflammatory Drugs |
| [1] | Travell JG, Simons DG. Myofascial Pain and Dysfunction: The Trigger Point Manual. Baltimore: Williams & Wilkins; 1999. |
| [2] | Simons DG. Review of enigmatic myofascial trigger points as a common cause of musculoskeletal pain and dysfunction. Journal of Electromyography and Kinesiology. 2004, 14(1), 95–107. |
| [3] | Gerwin RD. Classification, epidemiology, and natural history of myofascial pain syndrome. Current Pain and Headache Reports. 2001, 5(5), 412–420. |
| [4] | Dommerholt J, Fernández-de-las-Peñas C. Trigger point dry needling: an evidence and clinical-based approach. Journal of Bodywork and Movement Therapies. 2013, 17(1), 131–138. |
| [5] | Wheeler AH. Botulinum toxin A for the treatment of chronic neck pain. Clinical Journal of Pain. 2001, 17(4 Suppl), S76–S82. |
| [6] | Shah JP, Gilliams EA. Uncovering the biochemical milieu of myofascial trigger points using in vivo microdialysis: an application of muscle pain concepts to myofascial pain syndrome. Archives of Physical Medicine and Rehabilitation. 2008, 89(1), 16–23. |
| [7] | Fernández-de-las-Peñas C, Dommerholt J. Myofascial trigger points: peripheral or central phenomenon? Current Pain and Headache Reports. 2014, 18(10), 395. |
| [8] | Mense S. Muscle pain: mechanisms and clinical significance. Deutsches Ärzteblatt International. 2008, 105(12), 214–219. |
| [9] | Baldry P. Management of myofascial trigger point pain. Acupuncture in Medicine. 2002, 20(1), 2–10. |
| [10] | Fischer AA. Pressure threshold measurement for diagnosis of myofascial pain syndrome and evaluation of treatment results. Pain. 1987, 30(1), 115–126. |
| [11] | Fernández-de-las-Peñas C, Cuadrado ML, Pareja JA. Myofascial trigger points, neck mobility, and forward head posture in chronic tension-type headache. Headache. 2006, 46(3), 454–460. |
APA Style
Singh, S. (2026). Clinical Outcomes of Aggressive Multimodal Management in Cervicothoracic Myofascial Pain Syndrome: A Prospective Controlled Observational Study. Rehabilitation Science, 11(2), 37-43. https://doi.org/10.11648/j.rs.20261102.12
ACS Style
Singh, S. Clinical Outcomes of Aggressive Multimodal Management in Cervicothoracic Myofascial Pain Syndrome: A Prospective Controlled Observational Study. Rehabil. Sci. 2026, 11(2), 37-43. doi: 10.11648/j.rs.20261102.12
@article{10.11648/j.rs.20261102.12,
author = {Sonu Singh},
title = {Clinical Outcomes of Aggressive Multimodal Management in Cervicothoracic Myofascial Pain Syndrome:
A Prospective Controlled Observational Study},
journal = {Rehabilitation Science},
volume = {11},
number = {2},
pages = {37-43},
doi = {10.11648/j.rs.20261102.12},
url = {https://doi.org/10.11648/j.rs.20261102.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.rs.20261102.12},
abstract = {Myofascial pain syndrome (MPS) is one of the most common causes of chronic neck and shoulder pain encountered in clinical practice; however, despite its high prevalence, it is frequently underdiagnosed because of overlapping clinical presentations with other musculoskeletal and neurological disorders. The condition is characterized by hyperirritable trigger points within skeletal muscles that produce localized tenderness, referred pain, restricted mobility, and functional impairment. This prospective controlled observational study aimed to evaluate the clinical outcomes of aggressive multimodal therapy compared with conventional conservative treatment in patients with cervicothoracic MPS. Sixty patients diagnosed with cervicothoracic MPS were enrolled and allocated into two groups: Group A (n = 30) received aggressive multimodal therapy, while Group B (n = 30) received conventional conservative treatment. Baseline evaluation included assessment of pain intensity using the Visual Analog Scale (VAS), cervical range of motion measurements, and trigger point mapping, with follow-up assessments conducted at 48 hours, 6 weeks, and 6 months. Baseline pain intensity was comparable between the two groups, with mean VAS scores of 8.1 in Group A and 8.0 in Group B. The intervention group demonstrated significantly greater pain reduction at all follow-up time points, with mean VAS scores decreasing to 4.0 versus 6.7 at 48 hours, 2.0 versus 4.8 at 6 weeks, and 2.5 versus 5.1 at 6 months in Groups A and B, respectively. Significant clinical improvement was observed in 80% of patients receiving aggressive multimodal therapy compared with 40% of those receiving conventional treatment (p < 0.001). These findings suggest that aggressive multimodal therapy, consisting of trigger point injections and structured rehabilitation, provides superior pain relief and functional recovery compared with conventional conservative management in patients with cervicothoracic myofascial pain syndrome.},
year = {2026}
}
TY - JOUR T1 - Clinical Outcomes of Aggressive Multimodal Management in Cervicothoracic Myofascial Pain Syndrome: A Prospective Controlled Observational Study AU - Sonu Singh Y1 - 2026/07/08 PY - 2026 N1 - https://doi.org/10.11648/j.rs.20261102.12 DO - 10.11648/j.rs.20261102.12 T2 - Rehabilitation Science JF - Rehabilitation Science JO - Rehabilitation Science SP - 37 EP - 43 PB - Science Publishing Group SN - 2637-594X UR - https://doi.org/10.11648/j.rs.20261102.12 AB - Myofascial pain syndrome (MPS) is one of the most common causes of chronic neck and shoulder pain encountered in clinical practice; however, despite its high prevalence, it is frequently underdiagnosed because of overlapping clinical presentations with other musculoskeletal and neurological disorders. The condition is characterized by hyperirritable trigger points within skeletal muscles that produce localized tenderness, referred pain, restricted mobility, and functional impairment. This prospective controlled observational study aimed to evaluate the clinical outcomes of aggressive multimodal therapy compared with conventional conservative treatment in patients with cervicothoracic MPS. Sixty patients diagnosed with cervicothoracic MPS were enrolled and allocated into two groups: Group A (n = 30) received aggressive multimodal therapy, while Group B (n = 30) received conventional conservative treatment. Baseline evaluation included assessment of pain intensity using the Visual Analog Scale (VAS), cervical range of motion measurements, and trigger point mapping, with follow-up assessments conducted at 48 hours, 6 weeks, and 6 months. Baseline pain intensity was comparable between the two groups, with mean VAS scores of 8.1 in Group A and 8.0 in Group B. The intervention group demonstrated significantly greater pain reduction at all follow-up time points, with mean VAS scores decreasing to 4.0 versus 6.7 at 48 hours, 2.0 versus 4.8 at 6 weeks, and 2.5 versus 5.1 at 6 months in Groups A and B, respectively. Significant clinical improvement was observed in 80% of patients receiving aggressive multimodal therapy compared with 40% of those receiving conventional treatment (p < 0.001). These findings suggest that aggressive multimodal therapy, consisting of trigger point injections and structured rehabilitation, provides superior pain relief and functional recovery compared with conventional conservative management in patients with cervicothoracic myofascial pain syndrome. VL - 11 IS - 2 ER -
Department of Physical Medicine & Rehabilitation, Mahatma Gandhi Medical College & Hospital, Jaipur, India
Information