Abstract
Severe hypertension is associated with a two-fold increase in relative risk of death. Interventions to date fail to achieve sustained improvement in blood pressure, particularly in regional areas of high social disparity. Growing evidence points to multiple psychological, social and morbidity factors as contributors to the onset of and trajectory of hypertension. This study aims to examine the association of psychosocial factors and multimorbidity with response to treatment and treatment outcomes in the management of severe hypertensive patients providing updated knowledge and recommendations to improve their quality of care. We employed a hospital based comparative cross-sectional study using a quantitative and qualitative approach. Semi-structured questionnaires were used to collect information from 733 severe hypertensive patients attending cardiology clinics in two tertiary health institutions in southeastern Nigeria. Data collected was transcribed, coded, and analysed with IBM SPSS version 23 software with appropriate descriptive tools used in presenting findings. We observed a significant association between age of the respondents and their response to treatment. Overweight/obese respondents were 1.5times less likely to respond to treatment. These findings add to existing knowledge provoking thoughtful discussions among relevant public health actors and stakeholders to update management policies for severe hypertension.
Keywords
Psychosocial Factors, Multimorbidity Severe Hypertension, Treatment Outcome
1. Introduction
Hypertension is a prevalent cardiovascular long-term condition worldwide and is associated with a high rate of multimorbidity and psychosocial factors. Multimorbidity increases with age, ethnicity, and social deprivation. Previous studies have yielded conflicting findings about the relationship between multimorbidity and blood pressure control.
| [1] | C. Sarkar, H. Dodhia, J. Crompton, P. Schofield, P. White, C. Millett, M. Ashworth. (2015). Hypertension- A cross sectional study of the role of multimorbidity in blood pressure control. BMC Fam Pract. https://doi.org/10.1186/s12875-015-0313-y |
[1]
There is no doubt that hypertension has a complex multifactorial aetiology, involving genetic factors, dysfunction in a few biochemical and physiological regulatory processes, and lifestyle factors including diet, physical exercise, and body weight. Psychosocial factors must be placed within this broader context and be seen as part of the risk profile of the individual.
| [13] | Pilic, L., Pedlar, C. R., and Mavrommatis, Y. (2016). Salt-sensitive hypertension: mechanisms and effects of dietary and other lifestyle factors. Nutr. Rev 74, 645–658. https://doi.org/10.1093/nutrit/nuw028 |
[13]
Hypertension (HTN) is the single most important factor driving the high rates of Cardiovascular Death (CVD)-related mortality and health care expenditures
| [2] | Okubadejo, N. U., Ozoh, O. B., Ojo, O. O. et al. (2019). Prevalence of hypertension and blood pressure profile amongst urban-dwelling adults in Nigeria: a comparative analysis based on recent guideline recommendations. Clin Hypertens 25, https://doi.org/10.1186/s40885-019-0112-1 |
[2]
While research shows that its management is improving, we still lack a comprehensive understanding of the factors that contribute to the disease onset, trajectory of progression and patient outcomes. A substantial body of evidence supports the role of psychosocial factors (i.e., occupational stress) as primary risk factors for HTN.
| [2] | Okubadejo, N. U., Ozoh, O. B., Ojo, O. O. et al. (2019). Prevalence of hypertension and blood pressure profile amongst urban-dwelling adults in Nigeria: a comparative analysis based on recent guideline recommendations. Clin Hypertens 25, https://doi.org/10.1186/s40885-019-0112-1 |
[2]
As a result, Hypertension guidelines recommend psychosocial intervention as a means to prevent or delay the onset of HTN.
| [3] | J. Tran, R. Norton, D. Canoy, J. R. A. Solares, N. Conrad, M. Nazarzadeh, F. Raimondi, G. Salimi-Khorshidi, A. Rodgers, K. Rahimi. (2021). Multi-morbidity and blood pressure trajectories in hypertensive patients: A multiple landmark cohort study. https://doi.org/10.1371/journal.pmed.1003674 |
[3]
. The prevalence of comorbidity among people with hypertension is more common than those individuals with a normal blood pressure.
| [4] | Noh, J., Kim, H. C., Shin, A., Yeom, H., Jang, S. Y., Lee, J. H., Kim, C., & Suh, I. (2016). Prevalence of Comorbidity among People with Hypertension: The Korea National Health and Nutrition Examination Survey 2007-2013. Korean circulation journal, 46(5), 672–680. https://doi.org/10.4070/kcj.2016.46.5.672 |
[4]
Multimorbidity is a frequent and crucial factor to consider as it results in the increasing complexity of care associated with severe hypertension requiring more complex strategies to achieve effective care. Previous studies have yielded conflicting findings about the relationship between MM and blood pressure (BP) control
| [1] | C. Sarkar, H. Dodhia, J. Crompton, P. Schofield, P. White, C. Millett, M. Ashworth. (2015). Hypertension- A cross sectional study of the role of multimorbidity in blood pressure control. BMC Fam Pract. https://doi.org/10.1186/s12875-015-0313-y |
| [7] | Paulsen, M. S, Andersen M, Thomsen J. L, Schroll H, Larsen PV, Lykkegaard J., et al. (2013) Multimorbidity and Blood Pressure Control in 37 651 Hypertensive Patients from Danish General Practice. Journal of the American Heart Association. https://www.ahajournals.org/doi/10.1161/JAHA.112.004531 |
[1, 7]
.
Behavioral factors may play a role in established hypertension through their impact on baroreceptor activity, blood volume adjustments, or sodium retention. Findings suggest that the Type A coronary-prone behavior pattern is related to blood pressure levels, and there is some evidence that personality variables may be related to blood pressure levels in certain physiological subtypes of essential hypertensives.
Previous studies have examined few psychosocial factors, which limits the ability to fully capture the extent to which psychological conditions predicts blood pressure (BP) outcomes
| [5] | C. D. Ford, M. Sims, J. C. Higginbotham, M. R. Crowther, S. B. Wyatt, S. K. Musani, T. J. Payne, E. R. Fox, J. M. Parton. (2016) Psychosocial Factors Are Associated with Blood Pressure Progression Among African Americans in the Jackson Heart Study. American Journal of Hypertension. https://doi.org/10.1093/ajh/hpw013 |
[5]
It is proposed that psychological factors in hypertension will be most profitably studied when individual differences in both physiological and psychological dimensions are assessed in conjunction with the manipulations of laboratory stressors.
. In a study conducted, psychosocial and socioeconomic factors, as well as physical factors, is said to influence blood pressure control in moderate and severe essential hypertension.
| [6] | Caldwell JR, Theisen V, Kaunisto C. A, Reddy PJ, Smythe PS, Smith DW. (1983) Psychosocial factors influence control of moderate and severe hypertension. Soc Sci Med. https://doi.org/10.1016/0277-9536(83)90028-x PMID: 6879236. |
[6]
Although the aetiology of hypertension has been widely studied during the last decades, it remains far to be completely understood, as it results from a complicated interaction of genetic and several environmental risk factors. Furthermore, the development of HTN is associated with several demographic, lifestyle, and psychosocial variables
Risk factors, such as psychosocial ones and mental disorders, have also been investigated by several authors, nevertheless the relation with HTN results less clear and, sometimes, controversial
| [15] | Mermerelis, A., Kyvelou, S. M., Vellinga, A., Papageorgiou, C., Stefanadis, C., and Douzenis, A. (2016). Association between anxiety and depression symptoms with resistant hypertension and central hemodynamics: a pilot study. Hellenic J. Cardiol. 57, 203–204. https://doi.org/10.1016/j.hjc.2016.07.004 |
| [16] | Ventura, H. O., and Lavie, C. J. (2016). Impact of comorbidities in hypertension. Curr. Opin. Cardiol. 31, 374–375. https://doi.org/10.1097/HCO.0000000000000302 |
| [17] | Lijing L. Yan, Kiang L, Karen A. Matthews; et al (2003). The Coronary Artery Risk Development in Young Adults (CARDIA) study. JAMA https://jamanetwork.com/journals/jama/fullarticle/197528 |
[15-17]
While research shows that HTN management is improving, we still lack a comprehensive understanding of the factors that contribute to the disease onset, trajectory of progression and patient outcomes. Despite evidence on the effectiveness of lifestyle measures and antihypertensive medication, hypertension management remains challenging
| [10] | Bhattarai S, Bajracharya S, Shrestha A, et al (2023) Facilitators and barriers to hypertension management in urban Nepal: findings from a qualitative study Open Heart; 10: e002394. https://doi.org/10.1136/openhrt-2023-002394 |
[10]
Understanding of the complexity in managing hypertension demands an integrated approach considering the individual, and structural factors and how their interaction affects patients.
This study sought to evaluate the association between psychosocial factors and multi-morbidities and how it affects the treatment outcomes in severe hypertensive patients.
2. Methods
This research was conducted in two tertiary health institutions in Enugu state, South-eastern Nigeria. For this study, the University of Nigeria Teaching hospital and the Enugu state University Teaching hospitals were used. Enugu State is seen as the heart of Igboland, the cultural region of south-eastern Nigeria and is noted to have the tenth highest Human Development Index in Nigeria.
2.2. Data Collection Methods
Data collection was done using Interviewer-administered semi-structured questionnaires which were completed by the respondents. The study design hinged on using quantitative and qualitative methods.
The study population comprised of patients attending the cardiology outpatient clinic with focus on hypertensive patients and particularly those with severe hypertension in both hospitals.
The selection of respondents for the interview was through a two-stage sampling technique. The first stage involved stratification of patients into levels of hypertension for those attending the teaching hospital during the study period, severe hypertension was measured as 180/110 mmHg. The second stage was a simple random selection of 733 study participants from the total study population gotten from the two teaching hospitals during the 6 months period. This was shared in a 2:1 ratio between the University of Nigeria Teaching hospital and Enugu state University Teaching hospital (489 and 244 respectively). The questionnaires were administered to respondents at the calculated sample interval until the sample size for each of the sub-group is reached. The first (index) patient in each subgroup was selected using simple random sampling by balloting and subsequent patients were selected by adding the sample intervals until sample size was obtained.
Table 1. Number of respondents by Tertiary hospital.
Stage One | UNTH Cardiology outpatient hypertensive patients (Feb-May 2023) Classification into mild, moderate, severe. | ESUSTH Cardiology outpatient hypertensive patients (Feb -May 2023) Classification into mild, moderate, severe |
Stage Two | Random selection | Severe HTN n= 489 | Random selection | Severe HTN n= 244 |
2.5. Ethical Considerations
The Research approval was obtained from the Health Research and Ethics Committee of the University of Nigeria Teaching Hospital Enugu and the Enugu State University Teaching hospital prior to the commencement of the data collection. Participants were made to give their consent or otherwise to the study. Only participants who consented were involved in this study and their anonymity, privacy and confidentiality was respected.
Data collected were transcribed, coded, and analysed both manually and with Statistical Package for Social Sciences (SSPS Inc, Chicago, IL) version 23 statistical software. Body Mass Index (BMI) was classified using WHO classification. Mean values and standard deviations were used to calculate continuous variables and then compared using ANOVA or two sample t-test. Categorical variables were compared using the nonparametric tests-Chi-squares. Cross-tabulation was used to analyse relationships. Pearson's correlation for parametric and Spearman' rho correlation for nonparametric data was used to assess relationships. Significant variables were then analysed using stepwise method of multiple linear regression. All tests were two-tailed with P <.05 taken as statistically significant. Visualizable analysis of the collected data was made. Multiple Logistics regression was used to quantify effect of associated factors with response to treatment while adjusted from demographic characteristics. Furthermore, Binary Logistics Regression was used to quantify the impact of response to treatment on the treatment outcomes.
3. Results
A total of 733 respondents attending cardiology outpatient clinics were administered semi-structured questionnaire by 7 trained research assistants in two tertiary health facilities in Enugu state Nigeria. The content of the questionnaire was adapted from previous similar studies. The questionnaire was in 6 sections. The first section assessed their socio-demographic characteristic, the second assessed their psychosocial characteristics, The third assessed their health status with emphasis on the presence comorbidities and multi-morbidities, the fourth addressed factors affecting their access and response to treatment, the fifth assessed their perceived response to treatment and the last section reviewed the outcomes following treatment received over the study period between February-August 2023.
Participants’ sociodemographic characteristics shows closeness in gender participation among the respondents (Male 48%, Female 52%). It was observed that 10% of respondents were aged 15-45years, 38% were 46-60 years old and more than half (52%) of respondents were above 60years. Few, (6%) of respondents had no formal education, 26% had primary education, secondary (29%) and tertiary (39%). Most, 71% of respondents were married and 97% were Christians. It was observed that most of the respondents were traders (27.6%) followed by civil servants (19.8%).
Table 2. Socio-demographic Characteristics.
Characteristics | N | Percentage (%) |
Age | | |
15-45years | 76 | 10.4 |
46-60years | 274 | 37.5 |
>60years | 381 | 52.1 |
Sex | | |
Female | 382 | 52.3 |
Male | 349 | 47.7 |
Highest Educational Status | | |
No Formal Education | 41 | 5.6 |
Primary Education | 188 | 25.7 |
Secondary | 214 | 29.3 |
Tertiary | 288 | 39.4 |
Marital Status | | |
Divorced | 7 | 1.0 |
Married | 520 | 71.1 |
Separated | 5 | 0.7 |
Single | 49 | 6.7 |
Widowed | 150 | 20.5 |
Religion | | |
Christianity | 707 | 96.7 |
Islam | 13 | 1.8 |
Others | 7 | 1.0 |
Traditional | 4 | 0.5 |
3.1. Psychosocial Characteristics
9 in 10 respondents had at least one child, 6% ever experienced domestic violence, about 45% had friend/family that died in the past 12 months. Also, 3 in 10 respondents felt depressed about life situation, 6% of respondents/family members were diagnosed of depression, of which 11% were admitted while medication was prescribed to 42%. Psychologically, 59% of respondents were tired for no good reason, 68% almost nervous and 81% were so nervous that nothing could calm it down. Most times, majority of respondents felt hopeless (90%), fidgety (71%), so restless (80%), depressed (90%), worthless (91) and 65% mostly felt that everything was an effort while 83% felt so sad that nothing could cheer it up all the time.
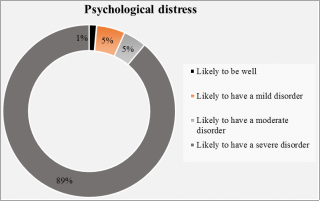
Figure 1. Psychological distress.
Overall, most (89%) of the respondents were likely to have a severe psychological distress, it was moderate and mild among 5% each while only 1% were likely to be well.
Our respondents reported several co-morbidities, diabetes was the highest, 18% followed by Osteo/Rheumatoid Arthritis (16%), Ulcer/stomach disease (15%), back pain (10%) and the least was liver disease (1.2%). It was reported that 8% of respondents were diagnosed with hypertension less than one year ago, 2-3 years (16%), 4-5years (24%) and 52% had been managing hypertension for the past 6years or above. 11% of the respondents were obese, 32% had overweight and 54% had normal weight while only 3% were underweight.
3.3. Response to Treatment
Majority (67%) agreed that the treatment worked for them, 64% received help they came for, 62% were being well informed on their treatment protocol, symptoms had subsided among 69%, BP was under control among 58%, 62% had not reported any new symptom and 59% of the respondents had not had a very high BP in the past two weeks.
Treatment outcomes show that 19% of the respondents experienced an unwanted or adverse side effects of medications, 8% developed multi-morbidity, 4% had heart failure, 16% had very BP and 3% had evidence of end organ damage. Overall, 89% of the patients survived after 3-6months treatment follow up.
Figure 2. Response to treatment. Overall, 7 in 10 respondents responded to treatment.
It was shown that 66% of the respondents did medical check-up 1-2times in a year, 20% did it 3times or more while 15% did not do medical check-up in a year. Also, 38% of respondents did follow up visit in 6-12months, 20% did it monthly while only 1% never done follow up visit. Majority, 93% of the respondents reported regular use of medication, 8% had never missed medication while 85% had missed the medication 1-3times and the remaining 7% had missed the medication more than 3times. Half of the respondents had a review with the cardiologist 1-2times (45%) and more than 2times (5%).
Table 3. Access to treatment.
Characteristics | N | Percentage (%) |
Frequency of medical check-up in a year | | |
1-2 times | 479 | 65.5 |
3 times or more | 146 | 20.0 |
None | 106 | 14.5 |
Frequency of follow up visits | | |
I have not done follow up visit | 6 | 0.8 |
3 monthly | 115 | 15.7 |
Every 2 weeks | 54 | 7.4 |
In 4-6 months | 129 | 17.6 |
in 6-12 months | 281 | 38.4 |
Monthly | 146 | 20.0 |
Took medications regularly | | |
Yes | 676 | 92.5 |
No | 55 | 7.5 |
No. of times respondents missed medications | | |
None | 59 | 8.1 |
1-3 times | 619 | 84.7 |
>3 times | 53 | 7.3 |
No. of times respondents had a review with the cardiologist | | |
1-2 Times | 327 | 44.7 |
3 times or more | 40 | 5.5 |
None | 364 | 49.8 |
There was a significant association between age of the patients and response to treatment (X2=7.025, p=0.030). Also, overweight/obesity was significantly associated with response to treatment (X2=3.888, p=0.049). After adjustment for age of respondents, it was discovered that overweight/obese respondents were 1.5times (1/0.677) less likely to respond to treatment (OR=0.677, CI=0.469- 0.979). It was also observed that response to treatment was significantly associated with reduction in heart failure (X2=16.303, p< 0.001). Patients who responded to treatment were 5.5times (1/0.183) less likely to have heart failure compared to those that did not respond to treatment (OR=0.183, CI= 0.073 0.456). Response to treatment was also significantly associated with reduction in further complications (X2=34.423, p<0.001). Patients who responded to treatment were 5.6times (1/0.178) less likely to develop complications like ischemic heart disease, myocardial infarction, Cerebrovascular disease, atrial fibrillation, peripheral artery disease and chronic renal disease compared to those that did not respond to treatment (OR=0.178, CI=0.095-0.335). There was no significant association between response to treatment and survival among patients.
Outcome measure
The primary outcome measure was optimal BP control. Patient-reported outcomes reviewed patients’ perspectives on their health status, providing opportunities to improve their quality of care.
4. Discussions
Overall, psychosocial characteristics showed no significant relationship with response to treatment and outcomes in patients with severe hypertension. However, most (89%) of the respondents with severe hypertension, were likely to have a severe psychological distress, it was moderate and mild among 5% each while only 1% were likely to be well using the Kessler Psychological Distress Scale. This is similar to a previous study done, as an in depth understanding of the underlying nature of the existing relationships amongst psychosocial factors such as job strain, job satisfaction, work stress, anxiety, and severe hypertension remains still unclear and difficult to fully understand and draw conclusions because of the several complicated and confounding factors
| [9] | Svetkey, L. P, Pollak. K. I, Yancy, W. S. (2009) Hypertension improvement project: Randomized trial of quality improvement for physicians and lifestyle modification for patients. Hypertension 54: 1226–33. https://doi.org/10.1161/HYPERTENSIONAHA.109.134874 |
[9]
. Psychological factors may act through many different complex mechanisms.
One premise is that stress and adverse experiences predispose to behavioral risk factors, such as smoking, substance use, poor diet, and sedentary lifestyle
| [8] | Maatouk, I., Herzog, W., Böhlen, F., Quinzler, R., Löwe, B., Saum, K. U., et al. (2016). Association of hypertension with depression, and generalized anxiety symptoms in a large population-based sample of older adults. J. Hypertens. 34, 1711–1720. https://doi.org/10.1097/HJH.0000000000001006 |
[8]
These people with poor psychosocial health may also have limited access to care. From this study, overweight/obesity was significantly associated with respond to treatment (X
2= 3.888, p=0.049). The role of psychosocial factors, such as the type A behavior pattern, depressive symptoms (depression), and anxiety, in the aetiology of hypertension is supported by many epidemiological investigations.
Most psychosocial risk factors are studied individually, but many of these psychosocial characteristics have been noted to be highly correlated.
This study has demonstrated that while psychosocial factors play a huge role as potential risk factors in the onset and progression of hypertension, its effect on the final treatment outcome in patients remains unclear as it involves a complex interplay of various risk factors.
In this study, respondents reported several comorbidities and multimorbidity’s. Overall prevalence of multimorbidity was 55%. Diabetes was the most reported comorbidity 18% followed by Osteo/Rheumatoid Arthritis (16%), Ulcer/stomach disease (15%), back pain (10%) and the least was liver disease (1.2%). It was observed that 11% of the respondents were obese, 32% had overweight and 54% had normal weight while only 3% were underweight. We noted that 65% of those who reported comorbidities had multimorbidity’s (more than two chronic conditions) Overall, there was no direct association of multimorbidity and patient related outcomes in hypertension, however, overweight/obesity was significantly associated with response to treatment (X2=3.888, p=0.049). Also, after adjustment for age of respondents, it was discovered that overweight/obese respondents were 1.5times (1/0.677) less likely to respond to treatment (OR=0.677, CI= 0.469-0.979).
According to an earlier study done, comorbidities concordant with hypertension have been conceptualized as those having a similar pathophysiologic profile, while the discordant comorbidities have no direct relationship or similarity with hypertension in the overall pathophysiologic profile. Such categorization of co-morbidities could facilitate an examination of the relationship between the type of comorbidities and hypertension control.
| [19] | Adeloye D, Owolabi EO, Ojji DB, Auta A, Dewan MT, Olanrewaju TO, et al. (2021) Prevalence, awareness, treatment, and control of hypertension in Nigeria in 1995 and 2020: a systematic analysis of current evidence. J Clin Hypertens (Greenwich) 23(5): 963–977. https://doi.org/10.1111/jch.14220 |
[19]
In another study done, it was noted that blood pressure levels at which patients were diagnosed with hypertension varied substantially according to the presence of comorbidities and were lowest in patients with multi-morbidity suggesting that early selection bias of hypertension diagnosis at different BP levels was a key determinant of long-term differences in BP by comorbidity status and that the lack of a more rapid decline in SBP in those with multi-morbidity provided some reassurance for BP treatment in these high-risk individuals.
| [3] | J. Tran, R. Norton, D. Canoy, J. R. A. Solares, N. Conrad, M. Nazarzadeh, F. Raimondi, G. Salimi-Khorshidi, A. Rodgers, K. Rahimi. (2021). Multi-morbidity and blood pressure trajectories in hypertensive patients: A multiple landmark cohort study. https://doi.org/10.1371/journal.pmed.1003674 |
[3]
Overall from this study, there was no significant association between the presence of multi-morbidities and treatment outcome among respondents. There is also a higher probability of hypertension control among patients with any comorbidity and this could be due to their greater exposure to the health system. The importance of multimorbidity in the managing cardiovascular risk factors and diseases is complex but it is a key component of primary care and there is a need to incorporate it into clinical guidance, training, and improvement initiatives.
5. Conclusion
The study has examined the association between psychosocial factors and multi-morbidities and how they affect patient related outcomes in severe hypertensive patients attending tertiary health institutions in Southeastern Nigeria. Hypertension has remained the most common cardiovascular disease in Nigeria contributing to a large non-communicable disease burden. A community-based study of rural and semiurban population in Enugu, Nigeria put the prevalence of hypertension in Nigeria at 32.8%
. It is important that policy makers closely assess how the interplay of these factors influence the management and treatment outcomes for people living with this condition. This concerned effort will be pivotal in reducing morbidity, mortality as well as impact on the quality and their overall outlook of life. There is a need to design health policies that can reduce the disease burden of hypertension. Successfully implementing any changes and health policies in the management of severe hypertension must involve full engagement and active participation of the relevant stakeholders as well as monitoring and evaluation to ascertain its efficacy. This intervention should be focused on health promotion and reducing the disease burden and mortality.
6. Study Limitations
The research did not categorize and classify comorbidities and multimorbidity’s according to their pathophysiological profiles and this could influence the overall outcome of the study. An in-depth classification would have given a more defined association between the variables.
7. Recommendations
Based on the findings from this study, we recommend that this study be extended to other parts of the country to understand in a wider context how these factors influence patient management and treatment outcomes in hypertension.
1) Further research should consider categorization of co-morbidities to facilitate an examination of the relationship between the type of comorbidities and hypertension control which is not investigated in this study.
2) This research should be implemented in other countries in Africa especially in low-income regions for result comparison as there could be variations in the findings.
3) Psychosocial pathways are significant in mediating the effects of social determinants (social, environmental, economic, political, and cultural factors) on health. Even with their significance, these pathways are often not clearly recognised as a key component of the framework of causes from social determinants to health outcomes. Psychosocial pathways need clearer clarification and an enhanced recognition in policy and practice to reduce health inequalities. Further research should be done for a deeper understanding on its influence.
Abbreviations
BMI: Body Mass Index
BP: Blood Pressure
CAD: Coronary Artery Disease
CHD: Congenital Heart Disease
CH: Congestive Heart Failure
CVD: Cardiovascular Disease
SBP: Systolic Blood Pressure
DBP: Diastolic Blood Pressure
ECG: Electrocardiogram
HTN: Hypertension
IHD: Ischemic Heart Disease
KPDS: Kessler Psychological Distress Scale
MM: Multimorbidity
SPSS: Statistical Package for Social Sciences
WHO: World Health Organization
Acknowledgments
Special thanks to the Nigerian Health Research and Ethics Committee of the Federal Ministry of Health and the Health Research and Ethics Committee of the University of Nigeria Teaching Hospital Enugu and the Enugu State University Teaching hospital for their approval and support in the data collections and to all others who contributed to the success of this research.
Conflicts of Interest
The authors declare no conflict of interest.
References
| [1] |
C. Sarkar, H. Dodhia, J. Crompton, P. Schofield, P. White, C. Millett, M. Ashworth. (2015). Hypertension- A cross sectional study of the role of multimorbidity in blood pressure control. BMC Fam Pract.
https://doi.org/10.1186/s12875-015-0313-y
|
| [2] |
Okubadejo, N. U., Ozoh, O. B., Ojo, O. O. et al. (2019). Prevalence of hypertension and blood pressure profile amongst urban-dwelling adults in Nigeria: a comparative analysis based on recent guideline recommendations. Clin Hypertens 25,
https://doi.org/10.1186/s40885-019-0112-1
|
| [3] |
J. Tran, R. Norton, D. Canoy, J. R. A. Solares, N. Conrad, M. Nazarzadeh, F. Raimondi, G. Salimi-Khorshidi, A. Rodgers, K. Rahimi. (2021). Multi-morbidity and blood pressure trajectories in hypertensive patients: A multiple landmark cohort study.
https://doi.org/10.1371/journal.pmed.1003674
|
| [4] |
Noh, J., Kim, H. C., Shin, A., Yeom, H., Jang, S. Y., Lee, J. H., Kim, C., & Suh, I. (2016). Prevalence of Comorbidity among People with Hypertension: The Korea National Health and Nutrition Examination Survey 2007-2013. Korean circulation journal, 46(5), 672–680.
https://doi.org/10.4070/kcj.2016.46.5.672
|
| [5] |
C. D. Ford, M. Sims, J. C. Higginbotham, M. R. Crowther, S. B. Wyatt, S. K. Musani, T. J. Payne, E. R. Fox, J. M. Parton. (2016) Psychosocial Factors Are Associated with Blood Pressure Progression Among African Americans in the Jackson Heart Study. American Journal of Hypertension.
https://doi.org/10.1093/ajh/hpw013
|
| [6] |
Caldwell JR, Theisen V, Kaunisto C. A, Reddy PJ, Smythe PS, Smith DW. (1983) Psychosocial factors influence control of moderate and severe hypertension. Soc Sci Med.
https://doi.org/10.1016/0277-9536(83)90028-x
PMID: 6879236.
|
| [7] |
Paulsen, M. S, Andersen M, Thomsen J. L, Schroll H, Larsen PV, Lykkegaard J., et al. (2013) Multimorbidity and Blood Pressure Control in 37 651 Hypertensive Patients from Danish General Practice. Journal of the American Heart Association.
https://www.ahajournals.org/doi/10.1161/JAHA.112.004531
|
| [8] |
Maatouk, I., Herzog, W., Böhlen, F., Quinzler, R., Löwe, B., Saum, K. U., et al. (2016). Association of hypertension with depression, and generalized anxiety symptoms in a large population-based sample of older adults. J. Hypertens. 34, 1711–1720.
https://doi.org/10.1097/HJH.0000000000001006
|
| [9] |
Svetkey, L. P, Pollak. K. I, Yancy, W. S. (2009) Hypertension improvement project: Randomized trial of quality improvement for physicians and lifestyle modification for patients. Hypertension 54: 1226–33.
https://doi.org/10.1161/HYPERTENSIONAHA.109.134874
|
| [10] |
Bhattarai S, Bajracharya S, Shrestha A, et al (2023) Facilitators and barriers to hypertension management in urban Nepal: findings from a qualitative study Open Heart; 10: e002394.
https://doi.org/10.1136/openhrt-2023-002394
|
| [11] |
Harrell, J. P. (1980). Psychological factors and hypertension: A status report. Psychological Bulletin, 87(3), 482–501.
https://doi.org/1c0.1037/0033-2909.87.3.482
|
| [12] |
Andrew Steptoe (2000) Psychosocial factors in the development of hypertension, Annals of Medicine, 32: 5, 371-375,
https://doi.org/10.3109/07853890008995940
|
| [13] |
Pilic, L., Pedlar, C. R., and Mavrommatis, Y. (2016). Salt-sensitive hypertension: mechanisms and effects of dietary and other lifestyle factors. Nutr. Rev 74, 645–658.
https://doi.org/10.1093/nutrit/nuw028
|
| [14] |
Graham, N., and Smith, D. J. (2016). Comorbidity of depression and anxiety disorders in patients with hypertension. J. Hypertens. 34, 397–398.
https://doi.org/10.1097/HJH.0000000000000850
|
| [15] |
Mermerelis, A., Kyvelou, S. M., Vellinga, A., Papageorgiou, C., Stefanadis, C., and Douzenis, A. (2016). Association between anxiety and depression symptoms with resistant hypertension and central hemodynamics: a pilot study. Hellenic J. Cardiol. 57, 203–204.
https://doi.org/10.1016/j.hjc.2016.07.004
|
| [16] |
Ventura, H. O., and Lavie, C. J. (2016). Impact of comorbidities in hypertension. Curr. Opin. Cardiol. 31, 374–375.
https://doi.org/10.1097/HCO.0000000000000302
|
| [17] |
Lijing L. Yan, Kiang L, Karen A. Matthews; et al (2003). The Coronary Artery Risk Development in Young Adults (CARDIA) study. JAMA
https://jamanetwork.com/journals/jama/fullarticle/197528
|
| [18] |
Mini G K, Mohan M, Sarma P S, Thankappan K. R. (2021) Multimorbidity and Blood pressure control Results of a cross-sectional study among schoolteachers in Kerala India. Indian J Public Health.
https://www.ijph.in/article.asp?issn=0019557X;year=2021;volume=65;issue=2;spage=190;epage=193;aulast=Mini
|
| [19] |
Adeloye D, Owolabi EO, Ojji DB, Auta A, Dewan MT, Olanrewaju TO, et al. (2021) Prevalence, awareness, treatment, and control of hypertension in Nigeria in 1995 and 2020: a systematic analysis of current evidence. J Clin Hypertens (Greenwich) 23(5): 963–977.
https://doi.org/10.1111/jch.14220
|
| [20] |
Ulasi II, Ijoma CK, Onodugo OD. (2010) A community-based study of hypertension and cardio-metabolic syndrome in semi-urban and rural communities in Nigeria. BMC Health Services Research. 10, article 71
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2858142
|
Cite This Article
-
APA Style
Nwaike, S. O., Daniel, E. O., Lamidi, S., Tomori, M. O., Avwerhota, M., et al. (2024). A Qualitative Analysis of the Association of Treatment Outcomes, Psychosocial Factors, and Multimorbidity in Severe Hypertensive Patients Attending Health Institutions in Southeast Nigeria. Journal of Family Medicine and Health Care, 10(2), 23-30. https://doi.org/10.11648/j.jfmhc.20241002.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Nwaike, S. O.; Daniel, E. O.; Lamidi, S.; Tomori, M. O.; Avwerhota, M., et al. A Qualitative Analysis of the Association of Treatment Outcomes, Psychosocial Factors, and Multimorbidity in Severe Hypertensive Patients Attending Health Institutions in Southeast Nigeria. J. Fam. Med. Health Care 2024, 10(2), 23-30. doi: 10.11648/j.jfmhc.20241002.12
Copy
|
Download
AMA Style
Nwaike SO, Daniel EO, Lamidi S, Tomori MO, Avwerhota M, et al. A Qualitative Analysis of the Association of Treatment Outcomes, Psychosocial Factors, and Multimorbidity in Severe Hypertensive Patients Attending Health Institutions in Southeast Nigeria. J Fam Med Health Care. 2024;10(2):23-30. doi: 10.11648/j.jfmhc.20241002.12
Copy
|
Download
-
@article{10.11648/j.jfmhc.20241002.12,
author = {Sylvia Oluchi Nwaike and Ebenezer Obi Daniel and Sheriff Lamidi and Michael Olabode Tomori and Michael Avwerhota and Israel Olukayode Popoola and Adebanke Adetutu Ogun and Aisha Oluwakemi Salami and Olukayode Oladeji Alewi},
title = {A Qualitative Analysis of the Association of Treatment Outcomes, Psychosocial Factors, and Multimorbidity in Severe Hypertensive Patients Attending Health Institutions in Southeast Nigeria
},
journal = {Journal of Family Medicine and Health Care},
volume = {10},
number = {2},
pages = {23-30},
doi = {10.11648/j.jfmhc.20241002.12},
url = {https://doi.org/10.11648/j.jfmhc.20241002.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jfmhc.20241002.12},
abstract = {Severe hypertension is associated with a two-fold increase in relative risk of death. Interventions to date fail to achieve sustained improvement in blood pressure, particularly in regional areas of high social disparity. Growing evidence points to multiple psychological, social and morbidity factors as contributors to the onset of and trajectory of hypertension. This study aims to examine the association of psychosocial factors and multimorbidity with response to treatment and treatment outcomes in the management of severe hypertensive patients providing updated knowledge and recommendations to improve their quality of care. We employed a hospital based comparative cross-sectional study using a quantitative and qualitative approach. Semi-structured questionnaires were used to collect information from 733 severe hypertensive patients attending cardiology clinics in two tertiary health institutions in southeastern Nigeria. Data collected was transcribed, coded, and analysed with IBM SPSS version 23 software with appropriate descriptive tools used in presenting findings. We observed a significant association between age of the respondents and their response to treatment. Overweight/obese respondents were 1.5times less likely to respond to treatment. These findings add to existing knowledge provoking thoughtful discussions among relevant public health actors and stakeholders to update management policies for severe hypertension.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - A Qualitative Analysis of the Association of Treatment Outcomes, Psychosocial Factors, and Multimorbidity in Severe Hypertensive Patients Attending Health Institutions in Southeast Nigeria
AU - Sylvia Oluchi Nwaike
AU - Ebenezer Obi Daniel
AU - Sheriff Lamidi
AU - Michael Olabode Tomori
AU - Michael Avwerhota
AU - Israel Olukayode Popoola
AU - Adebanke Adetutu Ogun
AU - Aisha Oluwakemi Salami
AU - Olukayode Oladeji Alewi
Y1 - 2024/05/10
PY - 2024
N1 - https://doi.org/10.11648/j.jfmhc.20241002.12
DO - 10.11648/j.jfmhc.20241002.12
T2 - Journal of Family Medicine and Health Care
JF - Journal of Family Medicine and Health Care
JO - Journal of Family Medicine and Health Care
SP - 23
EP - 30
PB - Science Publishing Group
SN - 2469-8342
UR - https://doi.org/10.11648/j.jfmhc.20241002.12
AB - Severe hypertension is associated with a two-fold increase in relative risk of death. Interventions to date fail to achieve sustained improvement in blood pressure, particularly in regional areas of high social disparity. Growing evidence points to multiple psychological, social and morbidity factors as contributors to the onset of and trajectory of hypertension. This study aims to examine the association of psychosocial factors and multimorbidity with response to treatment and treatment outcomes in the management of severe hypertensive patients providing updated knowledge and recommendations to improve their quality of care. We employed a hospital based comparative cross-sectional study using a quantitative and qualitative approach. Semi-structured questionnaires were used to collect information from 733 severe hypertensive patients attending cardiology clinics in two tertiary health institutions in southeastern Nigeria. Data collected was transcribed, coded, and analysed with IBM SPSS version 23 software with appropriate descriptive tools used in presenting findings. We observed a significant association between age of the respondents and their response to treatment. Overweight/obese respondents were 1.5times less likely to respond to treatment. These findings add to existing knowledge provoking thoughtful discussions among relevant public health actors and stakeholders to update management policies for severe hypertension.
VL - 10
IS - 2
ER -
Copy
|
Download