1. Introduction
Tuberculosis (TB) remains a pressing public health issue, requiring attention beyond its biomedical dimensions. Living with TB involves navigating a complex web of challenges that extend beyond physical symptoms. The disease carries significant social, emotional, and economic implications for affected individuals and their communities
| [1] | Yang H, Ruan X, Li W, Xiong J, Zheng Y. Global, regional, and national burden of tuberculosis and attributable risk factors for 204 countries and territories, 1990-2021: a systematic analysis for the Global Burden of Diseases 2021 study. BMC Public Health. 2024; 24(1): 3111. |
[1]
.
According to the World Health Organization, about a quarter of the global population is estimated to be infected with TB bacteria
. About 5-10% of people infected with TB will eventually get symptoms and develop TB disease
| [3] | Salisu, H. M. Ojule, I. N. Adeniji, F. O.and Kwakye, G. K. 2020. Prevalence and trend of TB/HIV co-infection in Suhum Municipality, Ghana,” PLoS One, vol. 17, no. 7, pp. 1-12, 2022 http://dx.doi.org/10.1371/journal.pgph.0000378 |
[3]
. Tuberculosis (TB) is indeed a significant public health concern in Ghana, contributing to high rates of illness and death. The disease burden in Ghana is substantial, with a high incidence and mortality rate. In 2020, Ghana had an estimated TB incidence of 143 per 100,000 population and a mortality rate of 49 per 100,000, meaning a third of TB cases in Ghana die from the infection
| [3] | Salisu, H. M. Ojule, I. N. Adeniji, F. O.and Kwakye, G. K. 2020. Prevalence and trend of TB/HIV co-infection in Suhum Municipality, Ghana,” PLoS One, vol. 17, no. 7, pp. 1-12, 2022 http://dx.doi.org/10.1371/journal.pgph.0000378 |
| [4] | Appiah MA, Arthur JA, Asampong E, Kamau EM, Gborgblorvor D, Solaga P, et al. Health service providers’ perspective on barriers and strategies to tuberculosis treatment adherence in Obuasi Municipal and Obuasi East District in the Ashanti region, Ghana: a qualitative study. Discov Heal Syst [Internet]. 2024; 3(1). Available from: https://doi.org/10.1007/s44250-024-00088-4 |
[3, 4]
. The World Health Organization (WHO) recommends that TB care should be comprehensive, incorporating not only medical treatment but also social, economic, and psychological support to improve patient outcomes and enhance their quality of life. According to the Ghana National Tuberculosis Control Programme (GNTCP), TB patients should receive standardized care, including free diagnosis and treatment, nutritional support, and regular follow-ups to ensure adherence and minimize treatment default rates. The National TB Control Program (NTP) in Ghana emphasizes the need for integrated, patient-centered care and prevention, as well as bold policies and supportive systems to address the disease burden
| [5] | Health MOF. REPUBLIC OF GHANA WORKPLACE HIV AND TB POLICY FOR THE HEALTH. |
[5]
.
In 2020, WHO estimated that there were 10 million new TB cases globally, with over 1.4 million TB-related deaths. Sub-Saharan Africa carries a substantial share of this burden, including Ghana, which recorded over 30,000 new TB cases in 2020
| [1] | Yang H, Ruan X, Li W, Xiong J, Zheng Y. Global, regional, and national burden of tuberculosis and attributable risk factors for 204 countries and territories, 1990-2021: a systematic analysis for the Global Burden of Diseases 2021 study. BMC Public Health. 2024; 24(1): 3111. |
| [2] | WHO. Tuberculosis @ www.who.int [Internet]. Tuberculosis: Key facts. 2021. Available from: http://www.who.int/mediacentre/factsheets/fs104/en/ |
[1, 2]
.
Tamale Teaching Hospital is located in the Northern Region of Ghana and plays a critical role in addressing the healthcare needs of a diverse and underserved population. Various risk factors, such as overcrowded living conditions, malnutrition, coexisting conditions like HIV/AIDS, and restricted access to medical services, all contribute to high TB incidence and the challenges patients face
| [3] | Salisu, H. M. Ojule, I. N. Adeniji, F. O.and Kwakye, G. K. 2020. Prevalence and trend of TB/HIV co-infection in Suhum Municipality, Ghana,” PLoS One, vol. 17, no. 7, pp. 1-12, 2022 http://dx.doi.org/10.1371/journal.pgph.0000378 |
| [6] | Louisa Q., Tumo E. Health-related quality of life of persons living with tuberculosis: A cross sectional study. Journal of clinical tuberculosis and other mycobacterial diseases. 28 (2022) 100324. |
[3, 6]
.
Beyond physical symptoms, TB imposes a severe emotional strain on patients. Many individuals experience anxiety and fear after diagnosis, worrying about their health and the impact on their families. The stigma associated with TB exacerbates these emotional struggles, leading to social isolation and discrimination within their communities
| [7] | Lönnroth K, Migliori GB, Abubakar I, D’Ambrosio L, De Vries G, Diel R, et al. Towards tuberculosis elimination: An action framework for low-incidence countries. Eur Respir J. 2015; 45(4): 928-52. |
| [8] | Craig GM, Daftary A, Engel N, O’Driscoll S, Ioannaki A. Tuberculosis stigma as a social determinant of health: a systematic mapping review of research in low incidence countries. Int J Infect Dis [Internet]. 2017; 56: 90-100. Available from: http://dx.doi.org/10.1016/j.ijid.2016.10.011 |
[7, 8]
. Psychologically, the prolonged and demanding TB treatment regimen creates significant stress and depression among patients. The frequent intake of medications, often accompanied by side effects, adds to treatment fatigue and increases the likelihood of non-adherence
| [9] | Ashaba C, Musoke D, Wafula ST, Konde-Lule J. Stigma among tuberculosis patients and associated factors in urban slum populations in Uganda. Afr Health Sci. 2021; 21(4): 1640-50. |
[9]
. These challenges are further compounded by socio-economic constraints, such as poverty, which limits access to proper nutrition and healthcare services, worsening health outcomes for TB patients
| [10] | Kipp AM, Pungrassami P, Stewart PW, Chongsuvivatwong V, Strauss RP, Van Rie A. Study of tuberculosis and AIDS stigma as barriers to tuberculosis treatment adherence using validated stigma scales. Int J Tuberc Lung Dis. 2011; 15(11): 1540-5. |
| [11] | Tanimura T, Jaramillo E, Weil D, Raviglione M, Lönnroth K. Financial burden for tuberculosis patients in low-and middle-income countries: a systematic review. Eur Respir J. 2014; 43(6): 1763-75. |
[10, 11]
.
Socially, the stigma surrounding TB affects how patients are treated by others, harming their relationships and economic opportunities
| [10] | Kipp AM, Pungrassami P, Stewart PW, Chongsuvivatwong V, Strauss RP, Van Rie A. Study of tuberculosis and AIDS stigma as barriers to tuberculosis treatment adherence using validated stigma scales. Int J Tuberc Lung Dis. 2011; 15(11): 1540-5. |
[10]
. Discrimination in workplaces and social settings further isolates individuals, reducing their ability to seek timely medical care and adhere to treatment. The economic impact of TB is severe, often affecting already vulnerable populations and leading to income loss and financial strain on families.
Given these multifaceted challenges, it is crucial to document and understand the holistic experiences of TB patients at Tamale Teaching Hospital. By uncovering these dimensions, healthcare professionals can design interventions that will address not only the biological aspects of the disease but also the social and psychological well-being of patients. These insights can inform policies and practices aimed at optimizing patient outcomes and creating a supportive environment for TB patients at Tamale Teaching Hospital and similar settings globally.
A comprehensive understanding of TB patients lived experiences within the specific context of Tamale Teaching Hospital is essential. Documenting the emotional, psychological, social, and economic dimensions of their experiences will help provide recommendations to mitigate the impact of TB on their quality of life and improve their overall well-being.
Theoretical Framework
The theoretical framework for investigating the lived experiences of tuberculosis (TB) patients at the Tamale Teaching Hospital is the theory of health belief.
| [14] | Marahatta SB, Yadav RK, Giri D, Lama S, Rijal KR, Mishra SR, et al. Barriers in the access, diagnosis and treatment completion for tuberculosis patients in central and western Nepal: A qualitative study among patients, community members and health care workers. PLoS One. 2020; 15(1): e0227293. |
| [13] | Green EC, Murphy EM, Gryboski K. The Health Belief Model. Wiley Encycl Heal Psychol. 2020; (May 2022): 211-4. |
[14, 13]
has it that HBM is one of the common concepts used in the frameworks to analyse health behaviour. This approach will aid understanding of the complex repercussions of TB on patients' life, including social and economic ramifications, family relationships, employment, income, and social support networks.
The Health Belief Model (HBM) is essential in evaluating patients’ beliefs and actions related to TB treatment. According to HBM, individuals' health behaviors are impacted by their views of the severity of an illness, their susceptibility to it, the rewards of acting, and the barriers to taking that action
| [13] | Green EC, Murphy EM, Gryboski K. The Health Belief Model. Wiley Encycl Heal Psychol. 2020; (May 2022): 211-4. |
[13].
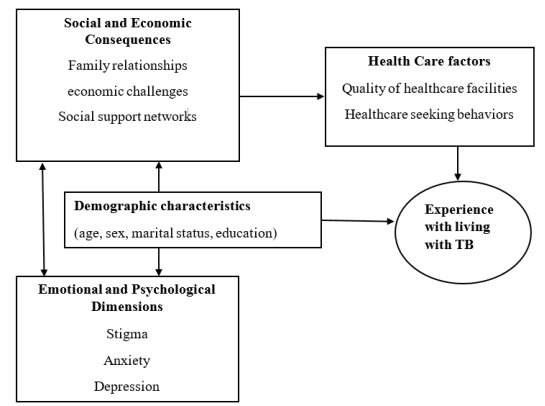
Applying HBM to TB patients helps in exploring how patients perceive the seriousness of TB and their vulnerability to its complications, their beliefs about the advantages of adhering to TB treatment regimens, and the challenges they face in accessing treatment, such as financial constraints, stigma, and transportation issues. Understanding these beliefs can drive actions targeted at increasing treatment adherence and health outcomes. Below are the constructions of HBM.
1) Perceived Susceptibility - Patients’ beliefs about their risk of developing or worsening TB.
2) Perceived Severity - How seriously they view the disease and its potential consequences.
3) Perceived Benefits - Beliefs about the effectiveness of TB treatment and health-seeking behaviors.
4) Perceived Barriers - Challenges patients face in accessing and adhering to treatment.
5) Cues to Action - Factors that trigger or motivate patients to seek care and continue treatment.
6) Self-Efficacy - Confidence in their ability to manage their condition and adhere to treatment.
Figure 1. Conceptual Framework.
2. Methods
2.1. Study Setting
The study setting is the Tamale Teaching Hospital. The Tamale Teaching Hospital is located in Tamale in the Northern region of Ghana and operates as a referral centre for the three northern regions of the country. As a teaching hospital, TTH boasts a well-established healthcare infrastructure, encompassing diagnostic facilities, treatment options, and support services, and act as a point of referral for TB in the region.
2.2. Study Design
A qualitative research approach was used to investigate the lived experiences of people with TB in the Tamale Teaching Hospital, considering the concerns that this study aimed to address.
The study employs Phenomenological Research Design to allow the researcher to describe participants lived experiences concerning TB patients in the Tamale Teaching Hospital.
Phenomenological research design is focused on exploring and understanding human experiences. This method aims to take information from the participants' own narrations and experiences, capturing their perceptions and emotions regarding a particular situation. In the context of investigating the lived experiences of TB patients in the TTH, phenomenological research design is particularly suitable. This method allows researchers to gain insights into the personal and lived experiences of these patients, providing a rich, nuanced understanding of the influence of TB on their lives.
Creswell
| [48] | Creswell, J. W., Fetters M. D., & Ivankova N. V. (2004). Designing a mixed methods study in primary care. The Annals of Family medicine, 2(1), 7-12. |
[48]
, asserts that a description offered by the researcher in a phenomenological study “culminates in the essence of the experiences for several individuals who have all experienced the phenomenon.” Thus, the study will describe the lived experiences of people who suffer TB in the TTH. The literature suggests that this study strategy is the best one for studying social and human problems that affect the entire population or a subset of the society
| [14] | Marahatta SB, Yadav RK, Giri D, Lama S, Rijal KR, Mishra SR, et al. Barriers in the access, diagnosis and treatment completion for tuberculosis patients in central and western Nepal: A qualitative study among patients, community members and health care workers. PLoS One. 2020; 15(1): e0227293. |
[14]
.
2.3. Study Population
The study population consists solely of tuberculosis (TB) patients receiving treatment at the Tamale Teaching Hospital and nurses providing healthcare.
2.4. Data Collection Tools
The primary data collection tool for this study was interview guide. The interview guide was carefully designed to explore the lived experiences of TB patients at Tamale Teaching Hospital. The interview guide was developed based on key themes identified from the literature, including psychosocial challenges, economic burdens, adherence to treatment, and perceptions of healthcare services.
The interview guide was pretested on a small group of TB patients outside the study area to ensure clarity and appropriateness of the questions. Adjustments were made based on participant feedback to refine the wording of questions and improve data collection efficiency. The final version of the guide included probes to encourage detailed responses and ensure that all relevant aspects of the research objectives were explored.
2.5. Sampling Procedure
Participants were selected using purposive sampling. This method allowed the researchers to deliberately select TB patients who could provide rich, relevant, and diverse insights into the study topic.
2.6. Data Collection Procedure
Data collection involved in-depth face-to-face interviews, conducted in a private and comfortable setting at Tamale Teaching Hospital to ensure confidentiality. The interviews were conducted in the preferred language of the participants (English or a local language), with a trained interpreter assisting when necessary. Each interview lasted approximately 30 to 45 minutes and was audio-recorded with the consent of the participants. Field notes were also taken to capture non-verbal cues and additional observations.
To ensure consistency and reliability in data collection, the researcher personally conducted all interviews using the semi-structured interview guide. After each interview, data were transcribed verbatim and translated into English language for analysis. Participants were given the opportunity to review and clarify their responses where necessary.
2.7. Data Quality Control
The following strategies were employed to enhance credibility, transferability, dependability, and confirmability of the study:
1. Credibility - The researchers engaged with participants to build trust and gain deeper insights into their lived experiences. Triangulation was applied by using multiple sources of data, including in-depth interviews and field observations, to validate the findings. Participants reviewed and confirmed the accuracy of the transcribed interviews, ensuring that their perspectives were correctly represented.
2. Transferability - The findings were contextualized historically, socially, and culturally, ensuring that they accurately reflect the lived realities of TB patients and could inform similar studies in other resource-limited settings.
3. Dependability - Dependability was ensured by maintaining clear and systematic documentation of the research process.
4. Confirmability - To establish confirmability, efforts were made to ensure that the study’s findings were neutral and free from researcher bias.
2.8. Ethical Consideration
Approval to carry out the research was sought from the ethical and review committee of the University for Development Studies to ensure adherence to ethical standards. Furthermore, before data collection, I introduced myself and elucidated the study's objectives to the respondents at any stage of the interview. Each participant provided both verbal and written consent. Strict confidentiality measures were applied to safeguard the treated information.
Informed Consent
Before responding to the questionnaire, consent forms were made available for respondents to sign. The consent form explicitly conveyed that participation in the research was entirely voluntary, and individuals had the option to refrain from answering if they found the questions to be intimidating or uncomfortable. Participants were assured that they could choose to partake or decline from the study without facing any form of punishment.
2.9. Data Analysis Plan
The data collected from the in-depth interviews were analyzed using thematic analysis. The analysis process began with data familiarization, where the researcher transcribed all interviews verbatim and carefully read through the transcripts multiple times to gain a deep understanding of the data. Audio recordings were replayed to ensure accuracy in transcription, and field notes were incorporated to capture non-verbal cues and contextual information.
The researchers moved on to theme identification, where related codes were grouped into broader themes that captured key aspects of TB patients’ experiences. The themes were reviewed against the original data to confirm their relevance and coherence, and any overlapping or redundant themes were merged or refined. Sub-themes were also identified to provide a deeper understanding of specific aspects within the broader themes.
3. Results
3.1. Socio-demographic Features of Respondent
The socio-demographic features encompassed variables such as the age group, gender, and educational qualifications of the respondents. Additionally, data regarding the respondents' occupations and the duration since the diagnosis of the patient's condition were collected. Despite these variables not being primary objectives of the study, information was sought on them due to their potential influence on the study's outcomes.
Table 1. Socio-demographic characteristics of respondents.
Participant No. | Age (in years) | Sex | Marital Status | Qualification | Occupation |
1 | 27 | M | Single | SSSCE | Farmer |
2 | 32 | F | Married | SSSCE | Trader |
3 | 28 | M | Single | HND | Poultry Farmer |
4 | 29 | M | Widow | Bachelors | Accountant |
5 | 45 | M | Single | HND | Metal Works |
6 | 37 | F | Married | SSSCE | Trader |
7 | 26 | F | Married | Bachelors | Teacher |
8 | 39 | M | Married | Bachelors | Businessman |
9 | 34 | M | Single | SSSCE | Galamsay Miner |
10 | 30 | M | Married | SSSCE | Driver |
11 | 31 | M | Divorced | Bachelors | Security Guard |
12 | 28 | M | Married | HND | Shop Attendant |
Field Survey, (2023)
Most respondents who participated in the study were males (n = 8/12). The majority of individuals are in their late 20s or early 30s (n=10/12), the results show that respondents are with different levels of education, ranging from SSSCE (Senior Secondary School Certificate Examination) with (n = 5/12), HND (Higher National Diploma) with frequency of (n = 3/12) and Bachelors (n = 4/8).
3.2. Themes and Sub-themes of the Study
Analysis of respondents’ experiences gave rise to four major themes and a total of ten sub-themes which are presented in
Table 2 below:
Table 2. Themes and sub-themes. Themes and sub-themes. Themes and sub-themes.
Themes | Sub-themes |
The lived experiences of TB patients at the Tamale Teaching Hospital | Patient's reaction after being diagnosed of TB |
Experience of stigma or discrimination |
Psychosocial, economic, and healthcare-related factors influencing TB patients | Economic challenges |
Psychosocial consequences |
Difficulty coping with medical guidelines on TB |
How TB patients navigate challenges and coping mechanisms | Financial support from friends and family |
Support from healthcare professionals |
Patients' Perspectives on the Effectiveness and side effects of TB treatment | Patients’ awareness/knowledge of TB |
Respondents’ perceptions about TB treatment |
Challenges with TB drugs |
3.2.1. The Lived Experiences of TB Patients at the Tamale Teaching Hospital
The lived experiences of the patients were assessed and each of them gave a narration of how the condition started. They went further to narrate the experience they are going through following the genesis of their condition. Based on this, the following subthemes emerged: how they got diagnosed with the condition and their reaction after being diagnosed with TB, and experiences (stigma or discrimination) they went through following their diagnosis.
3.2.2. Patients’ Reaction After Being Diagnosed with TB
Participants were asked about their initial reactions and feelings after they first received tuberculosis diagnosis. It came to most of them as a very big surprise as they never expected to fall victim to such an illness. Some of them were scared and thought that it could be the end of their lives while a section of them were thinking about the possibility of infecting other members of their families. Statements made by the clients are reported below:
“Initially, I felt scared and uncertain about how to manage this condition. Sincerely speaking, I initially felt confused and uncertain about how to cope with the diagnosis. I also felt anxious and overwhelmed by the diagnosis” (Participant 5).
Another participant had this to say:
“Eiih madam, this was tough for me. Initially, I felt shocked and scared upon receiving my diagnosis. I was really concern about the potential spread of the disease to my family and friends because I coughed for weeks before going to the hospital” (Participant 2).
A participant narrates the following in an in-depth interview:
“At first, I experienced feelings of fear and uncertainty regarding how to manage this condition. To be honest, my initial reaction was one of confusion and uncertainty about how to navigate the diagnosis. Additionally, I felt a sense of anxiety and being overwhelmed by the situation” (Participant 10).
Experience of Stigma or Discrimination
Findings indicated that majority of the TB patients face some forms of stigma and discrimination at a point in time during their plight. Some of these experiences were direct and others were indirect. Take into consideration the following testimonies given by two of the study respondents:
“Since I was diagnosed of TB, people I used to live with were not happy to be in the same room or area with me. I was abandoned like a piece of rug. Some of my friends and neighbors were treatment me like an animal” (Participant 1).
“When I was diagnosed of TB, I took a sick leave from work for about 3 weeks. When I reported to work after the leave, what I observed in my office was total discrimination not just to me but to every sick person. The moment I entered the office on the first day, they started living one-by-one. Hmmmm, I really had a terrible feeling about them” (Participant 12).
Despite the stigma and discrimination experienced by some TB patients, a number of them reported that they lived peacefully with their close friends and neighbors and never suffered any discrimination. This can be traced in the transcripts below:
“No no no, none at all, my family have really been supportive and the nurses at this center are caring and give us our medication and everything, I haven’t experienced any stigma or discrimination from anyone” (Participant 4).
“No madam, I cannot remember of a stigmatization from anyone. My wife and kids are isolated from me, but they still show me love. The health professionals here are good go to us and the in-charge is strict on all the nurses to nice to us and give us the best care possible” (Participant 5).
“No, not at all. My family has been incredibly supportive, and the nurses at this center are caring and provide us with our medication and everything we need. I haven't encountered any stigma or discrimination from anyone” (Participant 8).
3.2.3. Psychosocial, Economic, and Healthcare-related Factors Influencing TB Patients
The researcher sought to investigate the social and economic impacts of TB on patients. From the analysis of participants’ inputs, three sub-themes emerged: economic challenges, social consequences, and difficulty adhering to medical advice.
(i). Economic Challenges
The study respondents were reported to have faced diverse economic difficulties due to their illness. Many of them were not able to engage in any income generating activity due to the restrictions posed by the condition. To some extent, the high cost of TB medications coupled with high transport fares to and from the hospital further aggravated their economic plight. Below were some of the statements the patients made regarding their economic experiences after being diagnosed with TB:
“Because I have been cautioned distance myself from people, I have not been able to go work again. Hmmm, madam, it hasn’t been that easy and even some of the drugs are very costly” (Participant 1).
“eiih, and some of drugs are very expense. In fact, my family and I are already struggling to make ends meet. So, it has not been easy for me. But what can I say, I thank God for the grace so far. I’m improving daily. My office hasn’t provided any financial assistance oooh. But my family members are supporting small” (Participant 3).
A 39-year-old client narrated his economic experience as follows:
“The cost of some medications is quite high, and my family and I are already struggling to make ends meet. It's been a difficult situation, but I am thankful for God's grace as I am improving daily. Unfortunately, my office hasn't provided any financial assistance. However, my family members are offering some support, albeit in smaller amounts” (Participant 8).
Notwithstanding the financial difficulties reported by many of the respondents, a 34-year-old man explained that the condition has not affected his income. The client further highlighted that he gets support from close relatives and for that matter does not really feel the burden of the condition:
“Certainly, My sister. I don't have much to share, but the TB diagnosis and treatment have not had a substantial impact on my social relationships or employment status. Nevertheless, I've had to allocate more money than usual for medication and transportation. But all the same, I have been getting financial support from my family members and close friends which makes me feels somehow better financially” (Participant 9).
(ii). Psychosocial Consequences
The participants provided insights into how TB has affected their social relationships, including interactions with family, friends, and the community. This was what they had to say.
“Eiih madam, hmmm, this disease has significantly affected my social relationships. I isolated myself from my family and friends since I was diagnosed TB positive which has been very challenging. This has brought some tension in our relationship (marriage) as we struggle to balance my health needs with our daily routines” (Participant 1).
This participant said thus:
“Oh, my sister, hmm, the diagnosis and treatment of this illness have greatly influenced my social connections. I've had to distance myself from my family and friends for an extended period, which has been quite difficult. It also affects my wife and children as they need to care for me while avoiding contact with others. This has caused some strain in our relationships as we try to manage my health requirements alongside our daily responsibilities” (Participant 6).
In addition, the diagnosis of TB has further affected respondents’ ability to take part in congregational worships as well as participate in social gatherings such as weddings and naming ceremonies. One respondent lamented that:
“Hmmmm, don’t mention madam. Since the day I was confirmed positive for TB, I have stopped going to the mosque. Even attending naming ceremonies has become a problem. I just have to be living indoors: no one comes to me neither can I go to anyone” (Participant 6).
(iii). Difficulty Coping with Medical Guidelines on TB
The medical recommendation to keep a distance from people was a big challenge to some of the respondents. Several of them mentioned that they live in a single room with their families making it difficult to abide by the medical advice on social distancing. These are some of the reports given by the clients:
“I live in a small house with my wife and children, which is overcrowded. This has made it difficult to follow the isolation guidelines recommended by the hospital, as there is no separate room for me to stay in” (Participant 12).
“I have three children currently and I live with them including my wife in a single room. Because of this, it has been very challenging to adhere to the isolation guidelines recommended by the hospital as there isn't a separate room for me” (Participant 8).
3.2.4. How TB Patients Navigate Challenges and Coping Mechanisms
Giving the several challenges faced by people living with TB, the study explored how patients navigate those challenges and the coping mechanisms they employ in living with and managing the condition. In all, three sub-themes emerged under this heading: Financial support from family and friends, support from healthcare professionals, and emotional support from friends and family.
(i). Financial Support from Friends and Family
Not a single patient interviewed in this study reported being able to pay for their TB treatment on their own. Nearly all of them admitted to depending on their family in one way or another, whether it was for unofficial financial transfers in the form of loans or gifts or for providing care and replacement labor. According to one participant:
“Actually, my family have been so supportive throughout this time. As I told you earlier, I lost my job due to this condition and if not for the support I get from my family, I don’t think I would have been alive up to this time. Almost every month, I receive some token from my siblings which I use to support my treatment” (Participant 5).
“My family have been supportive. My mother in-law wakes up early to prepare the children for school. She assists me in my household chores and sometimes even wash my clothing” (Participant 2).
Also, some of the respondents stated that they supported their treatment with money they borrowed from their friends.
“Madam, you know that it is not easy to lend a person money these days due to trust issues. But thanks to my friends, they have strong trust in me. Anytime I call any of them for money, they don’t hesitate to respond to me. Even in some situations, some of them will even tell me not to pay back. I am grateful for the love they have shown me” (Participant 1).
(ii). Support from Healthcare Professionals
Treatment of TB patients in this study was characterized by positive experience with nurses and doctors. Findings of this study indicated that the patients experienced a lot of support from and care from the healthcare professionals. The following quotes are testimonies given by some respondents regarding their interactions with the professionals:
“The healthcare providers here are good people and very supportive. They treat us like their own and seem to understand our culture. They are very polite and always motivate us to take our drugs” (Participant 7).
“Well madam, the nurses try their best for us by giving us information about the medication regimen and instructions on managing side effects. They also provide nutritional advice and counseling on lifestyle changes to improve our overall health” (Participant 2).
The respondents were also happy about the level of professionalism demonstrated by some of the nurses and doctors at the TB clinic.
“They (nurses and doctors) are always ready to listen to us. Anytime I come for my medications, they speak to me politely and always make sure that all my concerns are addressed before leaving the facility” (Participant 3).
One 37-year-old woman commented that the support she receives from the nurses is what is keeping her stick to the treatment regimen.
“Hamm, madam, if not for the support and encouragement given by the nurses, I don’t think I could have followed the treatment regimen. They are always open and friendly” (Participant 6).
3.2.5. Patients' Perspectives on the Effectiveness and Side Effects of TB Treatment
This aspect of the study was conducted on three main questions: knowledge level on the condition, perceptions of treatment effectiveness and side effects and advice and insights for others facing TB diagnosis. That is, three sub-themes emerged under this theme: knowledge on TB, patients’ perceptions about TB treatment, side effects encountered due to treatment, and patents’ advice/recommendation for others.
(i). Patients’ Awareness/Knowledge of TB
When participants’ knowledge level on TB was assessed, a section of them demonstrated adequate knowledge of the condition. According to their reports, some of them were aware of the condition even before they were diagnosed. Television and health centers were the main sources of information for patients who demonstrated good knowledge of the condition. Quotes of patients’ remarks are as follows:
‘‘Ooooooh for me, I knew about TB before my diagnosis. There used to be an advert on TV about. Tuberculosis is a curable disease, visits your nearest hospital for free treatment, if you have TB. So, when I was informed, I had TB, I was not so worried because it can be treated. But I had to stop drinking and smoking, which was difficult’’ (Participant 3).
‘‘I was aware of TB before, but it never crossed my mind that it could be the cause of my concerns until I was diagnosed” (Participant 7).
‘‘Oh, in my case, I was already aware of TB before my diagnosis. There used to be a TV advert about it. "Tuberculosis is a curable disease; visit your nearest hospital for free treatment if you have TB." So, when I was informed that I had TB, I wasn't overly concerned because I knew it could be treated” (Participant 8).
Furthermore, some respondents were able to mention some common signs and symptoms associated with the condition as follows:
“…The symptoms seemed similar to those of catarrh and cough, and initially, I thought it was just a common cold (Participant 7)”.
“Most of the symptoms were like those of catarrh and cough and I told it was common cold’’ (Participant 2).
Notwithstanding that, several of the participants mentioned that they never heard of tuberculosis until they were diagnosed. A 37-year-old woman lamented her lack of knowledge of the condition emphasizing that if she knew about it earlier, shoe could all possible means to prevent it:
‘‘Sincerely speaking I did not know about TB. it was when I was taken to the Tema general hospital and diagnosed that they told me it was serious disease and if not treated early can kill me. Hmmmm madam, if I knew about this disease earlier, I could try my best possible to prevent it’’ (Participant 6).
(ii). Respondents’ Perceptions About TB Treatment
Again, when participants were asked about how they perceive the effectiveness of the tuberculosis treatment they are receiving, these were what they had to say.
“The treatment is incredibly effective, my sister. We are truly thankful for the support provided by the nurses here” (Participant 10).
“I am very happy with the treatment so far and I have seen a massive improvement in my condition since I started taking it” (Participant 12).
Some of the respondents went a little further to narrate how the TB treatment has aided them in improving their breathing pattern:
“Yes, my daughter, I am pleased with the treatment progress. Initially, I struggled to breathe and needed oxygen, but now I no longer require it, which is a significant improvement” (Participant 5).
“Yes madam, I am happy about the treatment so far. When I came, I couldn’t breathe well and was on oxygen but now I am not and that is massive improvement’’ (Participant 3).
(iii). Challenges with TB Drugs
Moreover, the nature of the challenges/side effects encountered by respondents while taking the TB medications were also explored in this arm of the study. When they were asked if they have experienced any side effects from their tuberculosis medications, almost all of them responded in affirmation. Meanwhile, the common side effects reported by the study respondents were fatigue and nausea. A detailed narration of their responses is highlighted in the transcripts below:
“Hmmm madam, yes. As for the side effects, I think we all experience it just that the way we feel about it may be different. For me, I sometimes feel like vomiting, feeling of tiredness and stress” (Participant 4).
“Yes, sister, I am dealing with side effects such as weakness, tiredness, and the challenge of consistently being on medication” (Participant 10).
‘‘Madam, I am experiencing side effects. I always feel like vomiting, dizziness, and fatigue. It is not easy at all but what can we do? (rhetorical question)’ (Participant 1).
That said, some of the patients were of the view that they don’t even care about the side effects they get from the drugs so far as it will get them cured. According to one 45-year-old man:
” Treatment so far has been very effective, but I just want to get better, I’m not really concern about the side effects of the medications” (Participant 5).
4. Discussion
The diagnosis of TB came to most of the respondents as a very big surprise as they never expected to fall victim to such an illness. Some of them were scared and thinking that it could be the end of their life while a section of them were thinking about the possibility of infecting other members of their families. In other places like Nepal, people exposed to TB patients were also afraid to go for check-up due to the misconceptions and fear attached to the disease
| [15] | Chang SH, Cataldo JK. A systematic review of global cultural variations in knowledge, attitudes and health responses to tuberculosis stigma. Int J Tuberc lung Dis. 2014; 18(2): 168-73. |
[15]
. This forced some patients to resort to traditional healers and only report to the hospital with associated complications.
Furthermore, the findings of this study indicated that majority of the TB patients face some form of stigma and discrimination at a point in time during their plight. Some of these experiences were direct and others were indirect. The current finding is replicated in previous literature
| [16] | Tadesse S. Stigma against tuberculosis patients in Addis Ababa, Ethiopia. PLoS One. 2016; 11(4): e0152900. |
[16]
. In other studies, some of the stigma-related perceptions attached to TB were the assumption that TB patients are careless and responsible for their sickness, the association drawn between HIV, TB and immoral behavior, and the perception that TB is incurable
| [17] | Lee L, Tung H, Chen S, Fu C. Perceived stigma and depression in initially diagnosed pulmonary tuberculosis patients. J Clin Nurs. 2017; 26(23-24): 4813-21. |
| [18] | Chen X, Du L, Wu R, Xu J, Ji H, Zhang Y, et al. Tuberculosis-related stigma and its determinants in Dalian, Northeast China: a cross-sectional study. BMC Public Health. 2021; 21: 1-10. |
| [19] | Cremers AL, de Laat MM, Kapata N, Gerrets R, Klipstein-Grobusch K, Grobusch MP. Assessing the consequences of stigma for tuberculosis patients in urban Zambia. PLoS One. 2015; 10(3): e0119861. |
| [20] | Duko B, Bedaso A, Ayano G, Yohannis Z. Perceived stigma and associated factors among patient with tuberculosis, Wolaita Sodo, Ethiopia: Cross‐sectional study. Tuberc Res Treat. 2019; 2019(1): 5917537. |
[17-20]
. The stigma and discrimination attached to TB plays a crucial role in affecting patients’ adherence to their medication regimen. Elsewhere, TB patients refused to disclose their status due to the fear of stigma and discrimination
| [21] | Thomas BE, Shanmugam P, Malaisamy M, Ovung S, Suresh C, Subbaraman R, et al. Psycho-socio-economic issues challenging multidrug resistant tuberculosis patients: a systematic review. PLoS One. 2016; 11(1): e0147397. |
[21]
. This justifies the need to expand mass sensitization on TB to erase the negative and false perceptions associated with victims of TB.
The study respondents were reported to have faced diverse economic difficulties due to their illness. Many of them said they were not able to engage in any income generating activity due to the restrictions posed by the condition. Although some aspects of TB treatment are offered free of charge in public health facilities, patents incurred embedded costs related to transport fares and food. Our result is similar to what was reported in previous studies
| [22] | Oshi D, Chukwu J, Nwafor C, Chukwu NE, Meka AO, Anyim M, et al. Support and unmet needs of patients undergoing multidrug‐resistant tuberculosis (MDR‐TB) treatment in southern Nigeria. Int J Health Plann Manage. 2020; 35(4): 832-42. |
| [23] | Tadesse T, Demissie M, Berhane Y, Kebede Y, Abebe M. Long distance travelling and financial burdens discourage tuberculosis DOTs treatment initiation and compliance in Ethiopia: a qualitative study. BMC Public Health. 2013; 13: 1-7. |
[22, 23]
. Similarly in Ethiopia, TB exposed individuals delayed seeking medical attention at the health facilities and even those on treatment failed to go for reviews because they couldn’t afford the high transport fares
| [24] | Onazi O, Gidado M, Onazi M, Daniel O, Kuye J, Obasanya O, et al. Estimating the cost of TB and its social impact on TB patients and their households. Public Heal action. 2015; 5(2): 127-31. |
[24]
. Despite most TB patients losing their jobs in Nigeria, the cost of treating TB keeps soaring where each patient is expected to spend about US$52.02 in order to access treatment
| [25] | Foster N, Vassall A, Cleary S, Cunnama L, Churchyard G, Sinanovic E. The economic burden of TB diagnosis and treatment in South Africa. Soc Sci Med. 2015; 130: 42-50. |
[25]
. In South Africa, poorer patients incurred higher direct costs during treatment than those who were less poor
| [26] | Alene KA, Clements ACA, McBryde ES, Jaramillo E, Lönnroth K, Shaweno D, et al. Mental health disorders, social stressors, and health-related quality of life in patients with multidrug-resistant tuberculosis: a systematic review and meta-analysis. J Infect. 2018; 77(5): 357-67. |
[26]
.
In other jurisdictions, TB patients had to take loans and/or sell their property in order to cover the cost of their treatment
| [12] | Biermann O, Lönnroth K, Caws M, Viney K. Factors influencing active tuberculosis case-finding policy development and implementation: A scoping review. BMJ Open. 2019; 9(12): 1-12. |
[12]
. More so, the interplay between TB and poverty is well documented. Tanimura et al.,
| [12] | Biermann O, Lönnroth K, Caws M, Viney K. Factors influencing active tuberculosis case-finding policy development and implementation: A scoping review. BMJ Open. 2019; 9(12): 1-12. |
[12]
. argue that TB is both a cause and consequence of poverty and the high TB burden in low-income settings such as sub-Saharan Africa is an indication of this
| [12] | Biermann O, Lönnroth K, Caws M, Viney K. Factors influencing active tuberculosis case-finding policy development and implementation: A scoping review. BMJ Open. 2019; 9(12): 1-12. |
[12]
. Given the financial catastrophes associated with this condition, there is a need to ensure that TB patients and affected families receive appropriate income replacement and other social protection interventions.
Furthermore, the participants in this study provided insights into how TB has affected their social relationships, including interactions with family, friends, and the community. In addition, the diagnosis of TB has further affected respondents’ ability to take part in congregational worships as well as participate in social gatherings such as weddings and naming ceremonies. Likewise, social isolation was cited in a systematic review article as a factor that affects TB patients’ emotional status and wellbeing
| [27] | Kaliakbarova G, Pak S, Zhaksylykova N, Raimova G, Temerbekova B, Van Den Hof S. Psychosocial support improves treatment adherence among MDR-TB patients: experience from East Kazakhstan. Open Infect Dis J. 2013; 7(1): 60-4. |
[27]
. Meanwhile, psychosocial support is noted to improve TB patients’ adherence to the treatment therapy
| [28] | Yellappa V, Lefèvre P, Battaglioli T, Narayanan D, Van der Stuyft P. Coping with tuberculosis and directly observed treatment: a qualitative study among patients from South India. BMC Health Serv Res. 2016; 16: 1-11. |
[28]
.
Coping mechanisms are means by which people mitigate some of the experiences of stigma. People with stronger coping mechanisms are known to have better treatment outcomes
| [29] | Bieh KL, Weigel R, Smith H. Hospitalized care for MDR-TB in Port Harcourt, Nigeria: a qualitative study. BMC Infect Dis. 2017; 17: 1-9. |
[29]
. There are several studies that explored the strategies TB patients use to cope with the catastrophes that come with their condition
| [29] | Bieh KL, Weigel R, Smith H. Hospitalized care for MDR-TB in Port Harcourt, Nigeria: a qualitative study. BMC Infect Dis. 2017; 17: 1-9. |
| [30] | Horter S, Stringer B, Venis S, du Cros P. “I can also serve as an inspiration”: A qualitative study of the TB&Me blogging experience and its role in MDR-TB treatment. PLoS One. 2014; 9(9): e108591. |
| [31] | Mukerji R, Turan JM. Exploring manifestations of TB-related stigma experienced by women in Kolkata, India. Ann Glob Heal. 2018; 84(4): 727. |
[29-31]
. Mukerji and Turan cited in their study that people with stronger coping mechanisms are known to have better treatment outcomes
| [32] | Ayé R, Wyss K, Abdualimova H, Saidaliev S. Factors determining household expenditure for tuberculosis and coping strategies in Tajikistan. Trop Med Int Heal. 2011; 16(3): 307-13. |
[32]
.
In this study, financial and emotional support from family, friends, and healthcare professionals served as better coping mechanisms adopted by the respondents. This finding is consistent with previously conducted studies in other places like Tajikistan
| [33] | Numpong S, Kengganpanich M, Kaewkungwal J, Pan-Ngum W, Silachamroon U, Kasetjaroen Y, et al. Confronting and coping with multidrug-resistant tuberculosis: Life experiences in Thailand. Qual Health Res. 2022; 32(1): 159-67. |
[33]
and Thailand
| [34] | Makhfudli AFR, Sukartini T, Asmoro CP. Family Support and Coping Mechanisms in Patients with Pulmonary Tuberculosis. 2018. |
[34]
. Similarly, the current result is resonated in Indonesia where Family support received by TB patients comes from the support of nuclear families who live in one house, who understand the healthy development of respondents and generally provide informational, instrumental and emotional support
| [35] | Saqib SE, Ahmad MM, Amezcua-Prieto C. Economic burden of tuberculosis and its coping mechanism at the household level in Pakistan. Soc Sci J. 2018; 55(3): 313-22. |
[35]
. In coping with the financial difficulties associated with TB treatment, patients in Pakistan borrowed money from their close friends to support their expenses
| [36] | Yesuf Y, Wondimu H, Demeke A. A new look to the coping strategy preferences of TB patients: Qualitative Explorations among TB patients in Northwestern Ethiopia. Int J Infect Dis. 2018; 73: 343. |
[36]
which is consistent with findings of the current study.
Conversely, the current finding contradicts a study in India where TB patients reported prayer as a source of strength and a helpful means to combat the negative experiences of their condition
| [32] | Ayé R, Wyss K, Abdualimova H, Saidaliev S. Factors determining household expenditure for tuberculosis and coping strategies in Tajikistan. Trop Med Int Heal. 2011; 16(3): 307-13. |
[32]
. Likewise in Ethiopia, resorting to religious camps was a cognitive measure adopted by TB clients in attempts to cope with the sickness
| [37] | Barnhoorn F, Adriaanse H. In search of factors responsible for noncompliance among tuberculosis patients in Wardha District, India. Soc Sci Med. 1992; 34(3): 291-306. |
[37]
. A very old Indian study dated back to the pre-DOT (Directly Observed Therapy) era explained that TB patients who use coping mechanisms such as social isolation and prayer were more likely to be non-compliant with their treatment regimen
| [38] | Pramanik D, Ghosh JR. Knowledge and awareness of tuberculosis among pulmonary tuberculosis patients in a rural area of West Bengal. SAARC J Tuberc Lung Dis HIV/AIDS. 2015; 12(2): 13-9. |
[38]
. Given this context, one can argue that TB patients in the current study setting (Tamale Teaching Hospital) are less likely to be non-compliant with their medications since none of these mechanisms were reported by them. Elsewhere in Pakistan, some TB victims (33.3% of who were from lower income quintile) went further to withdraw their children from school as a means of coping with the economic burden posed by their condition
| [36] | Yesuf Y, Wondimu H, Demeke A. A new look to the coping strategy preferences of TB patients: Qualitative Explorations among TB patients in Northwestern Ethiopia. Int J Infect Dis. 2018; 73: 343. |
[36]
.
According to the reports gathered from the respondents of this study, some of them were aware of the condition even before they were diagnosed while others got to know about it after their diagnosis. This finding is in-line with a cross-sectional study in West Bengal (India) where the proportion of TB clients who demonstrated some level of awareness about their condition prior to the diagnosis was almost equal to those who knew nothing about it
| [39] | Das R, Baidya S. A study on knowledge of pulmonary tuberculosis and DOTS among pulmonary tuberculosis patients in west Tripura district, India. SAARC J Tuberc Lung Dis HIV/AIDS. 2015; 12(1): 1-7. |
[39]
. According to Das & Baidya
| [40] | Mangesho PE, Shayo EH, Makunde WH, Keto GB, Mandara CI, Kamugisha ML, et al. Commnity knowledge, attitudes and practices towards tberculosis and its treatment inMpwapwa District, central Tanzania. Tanzan J Health Res. 2007; 9(1): 38-43. |
[40]
, TB patients who mostly demonstrate adequate knowledge about their condition are more likely to be those who have higher educational attainment. Additionally, this study found television and health centers as the main sources of information for TB patients regarding their condition which is similar to the results of another study
| [39] | Das R, Baidya S. A study on knowledge of pulmonary tuberculosis and DOTS among pulmonary tuberculosis patients in west Tripura district, India. SAARC J Tuberc Lung Dis HIV/AIDS. 2015; 12(1): 1-7. |
[39]
. Contrary to this finding is a study in Tanzania where family and friends were the most significant sources of information on TB, with health facilities rated the least
| [41] | Tachfouti N, Slama K, Berraho M, Nejjari C. The impact of knowledge and attitudes on adherence to tuberculosis treatment: a case-control study in a Moroccan region. Pan Afr Med J. 2012; 12(1). |
[41]
.
Furthermore, the respondents in the current study expressed great satisfaction towards the TB treatment and services indicating how the medication has improved their health which is at par with what TB patients in Morocco also reported
| [42] | Tesfahuneygn G, Medhin G, Legesse M. Adherence to Anti-tuberculosis treatment and treatment outcomes among tuberculosis patients in Alamata District, northeast Ethiopia. BMC Res Notes. 2015; 8: 1-11. |
[42]
. A similar research in Ethiopia
| [43] | Nezenega ZS, Perimal-Lewis L, Maeder AJ. Factors influencing patient adherence to tuberculosis treatment in Ethiopia: a literature review. Int J Environ Res Public Health. 2020; 17(15): 5626. |
[43]
reviewed records of over four thousand TB patients and found that the overall treatment success rate was more than ninety percent which further buttresses the claims made by the respondents in the current study. Interestingly, majority of the patients in their study who had unsuccessful treatment were those who defaulted
| [43] | Nezenega ZS, Perimal-Lewis L, Maeder AJ. Factors influencing patient adherence to tuberculosis treatment in Ethiopia: a literature review. Int J Environ Res Public Health. 2020; 17(15): 5626. |
[43]
. This points out the need to strengthen the DOTs strategy to reduce the incidence of defaulting and thus, improve the success rate of the TB treatment.
As replicated in the present survey, prior literature highlighted side effects of the TB drugs (such as nausea, drowsiness, fatigue) among several other factors that hinder adherence to the treatment regimen
| [44] | Bhatt CP, Kc B. Side effects associated with drugs used in treatment of multi drug resistant tuberculosis and treatment related factors of multi drug resistant tuberculosis patients In Kathmandu valley. SAARC J Tuberc Lung Dis HIV/AIDS. 2017; 14(1): 1-6. |
| [45] | Oh AL, Makmor-Bakry M, Islahudin F, Wong ICK. Prevalence and predictive factors of tuberculosis treatment interruption in the Asia region: a systematic review and meta-analysis. BMJ Glob Heal. 2023; 8(1): e010592. |
| [46] | Pontali E, Raviglione MC, Migliori GB. Regimens to treat multidrug-resistant tuberculosis: past, present and future perspectives. Eur Respir Rev. 2019; 28(152). |
[44-46]
. The negative implication of this is that it makes patients reluctant to follow the medication regimen (defaulting) which could lead to multi-drug resistance tuberculosis
| [47] | Creswell, J. W. (2014). Research design: Qualitative, quantitative, and mixed methods approach. Sage Publications. |
[47]
. To curb this, it will therefore be prudent to give supplemental medications to the patients which could handle the side effects of the TB treatment but will not necessarily reduce its efficacy.