Cervical masses are defined as a set of benign or malignant neoformations developed in the neck, in its medial or lateral part, from the different anatomical structures that form the neck (vessels, nerves, lymph nodes, viscera, muscles). We conducted a descriptive retrospective study in the Otorhinolaryngology and Head and Neck Surgery Department of Gabriel Touré University Hospital in Bamako from 2008 to 2017. We collected 51 cases with clinical, paraclinical, and treatment data. Females were the most represented (72.5%), the mean age was 48.5 years, and the range was from 6 to 86 years. 38 cases were cervical masses of the medial compartment, 13 cases were cervical masses of the lateral compartment. Thyroid gallbladder adenoma accounted for 30 cases, or 58.82%, followed by pleomorphic parotid adenoma with 10 cases, or 19.60%. Total thyroidectomy was the most commonly performed type of surgery with 22 cases or 43.14%, followed by total parotidectomy with 11 cases or 21.57%. All our patients treated with thyroidectomy received hormone replacement therapy. The outcome was good in 40 cases, or 78.43% with unilateral recurrent paralysis in 02 cases, 01 case of peripheral facial paralysis, 06 cases of facial paresis.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Cervical masses are defined as a set of benign or malignant neoformations developed in the neck, in its medial or lateral part, and this from the different anatomical structures that form the neck (vessels, nerves, lymph nodes, viscera, muscles)
[1]
David SF, Mary EF. Thyroglossal duct anomalies and other semi-congenital anomalies in pediatrics. Surge 2006. Vol: 157. Ref: 55.
[2]
Turkington JR, Paterson A, Sweeney LE, Thornbury GD. Neck masses in children. Br J Radial 2005, 78: 75-85.
[1, 2]
. In this region, the development of a mass opens a very wide field of diagnostic hypotheses, ranging from the accompaniment of lymphadenopathy to a tumor manifestation
[1]
David SF, Mary EF. Thyroglossal duct anomalies and other semi-congenital anomalies in pediatrics. Surge 2006. Vol: 157. Ref: 55.
[1]
. The progressive development of masses leads to compression of the surrounding organs which manifests clinically by dyspnea, dysphonia or dysphagia
[3]
T. Kennel, R. Garrel, V. Costes, P. Boisselier, L. Crampette, V. Favier, Carcinomas of unknown primary origin of the head and neck French Annals of Otorhinolaryngology and Head and Neck Pathology, 136, 2019 Pages 184-192.
P. Costa de Araujo, O. Battisti. How to explore cervical masses in children. Rev Med Liège 2010; 65: 1: 40-45.
[3, 4]
. Surgery remains an important part of the management of these cervical masses, and the diversity of its clinical and radiological presentations is the main reason for diagnostic and therapeutic challenges
[5]
Murat S, Sedar B, Selkut L, Mehmet AS. Unusual presentation and location of thyroglossary duct cyst in children. Otolaryngology Head Neck Surg 2007, 136: 854-5.
[5]
.
In Mali, there are no studies on cervical masses as a semiological entity and which constitute an increasingly frequent reason for consultation in the otolaryngology department of the Gabriel Touré University Hospital. Our objective was to study the diagnostic and therapeutic aspects of cervical masses in the department.
2. Materials and Methods
We conducted a descriptive retrospective study carried out in the otolaryngology department of the Gabriel Touré University Hospital in Bamako over 08 years from January 1, 2009 to December 31, 2017. Were included in our study all patients admitted to the department with a cervical mass who were operated on with the result of the anatomopathology of the surgical specimen available. The file included parameters such as complete epidemio-clinical, paraclinical and therapeutic data. Were excluded from our study All cases of cervical adenopathy, any mass for which the medical file is incomplete and the histological results unavailable were excluded. We did not have a fixed sample size because the study was conducted over a given period, i.e. 08 years. The data were entered and analyzed on SPSS software.
3. Results
3.1. Sociodemographic Characteristics
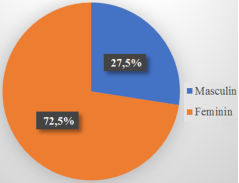
We collected 51 cases of cervical mass. The hospital prevalence was 1.9% of all ENT hospitalizations. The female sex was the most represented with 72.5% (Figure 1) with a sex ratio of 0.37. The age group [60 to 74 years] represented 47.1% of cases, with extreme ages from 6 to 86 years for a mean age of 48.5 years.
All 51 of these patients consulted for a neck mass or another symptom associated with a neck mass. The duration of evolution was greater than 3 months in 86.3% of patients.
Associated clinical signs were palpitations 54.9%; neck pain 23.5%; dyspnea 9.8%; dysphonia 5.9% and dysphagia 5.9%. The mass was mobile during ingestion in 62.7% of cases.
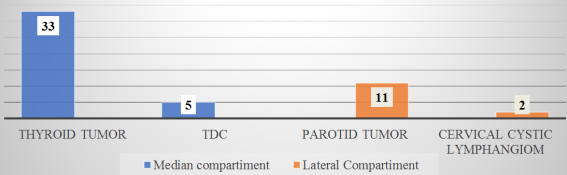
In 64.7% of cases (38 cases), the mass was located in the medial compartment of the neck (Figure 2).
The histological types found (Table 3) were thyroid vesicular adenoma 30 cases, pleomorphic adenoma of the parotid 10 cases; thyroglossal cyst (TTC) 05 cases, papillary thyroid carcinoma 03 cases, cervical cystic lymphangioma 02 cases and adenoid cystic carcinoma of the parotid 01 case. All our patients benefited from cervical ultrasound. A cervical CT scan completed the ultrasound result in two cases. Thyroid hormones were normal in 32 cases. Preoperative assessments were normal in all our patients. The surgical interventions performed are thyroidectomy 33 cases (total 22 cases; subtotal 07 cases; lobectomy 04 cases), parotidectomy (total parotidectomy: 10 cases and exofacial: 01 case), KTT cure 05 cases and cervicotomy for the exeresis of cervical cystic lymphangioma 02 cases. The postoperative course was simple in 80% of cases, we had 02 cases of unilateral recurrent paralysis, 01 case of peripheral facial paralysis, 06 cases of facial paresis.
Figure 2. Distribution of patients according to neck region.
Table 2. Types of surgery performed.
Type of surgery
Absolute frequency (%)
Relative frequency (%)
Total thyroidectomy
22
43.14
Subtotal thyroidectomy
07
13.7
Lobectomy
04
8
TDC Cure
05
9.8
Total parotidectomy
10
19.6
Exofacial parotidectomy
01
1.96
Excision of cervical cystic lymphangioma
02
3.9
Total
51
100
Table 3. Distribution of histological types according to sex.
Sex
Histological type
Male
Female
Total
Papillary thyroid carcinomas
0
3
3
Adenoid cystic carcinoma
0
1
1
Pleomorphic adenomas of the parotid gland
3
7
10
Thyroid gallbladder adenomas
6
24
30
Simple cervical cystic lymphangioma
2
0
2
Thyroglossal duct cyst
3
2
5
Total
14
37
51
NB: Degree of freedom = 5, p = 0.05, X2 = 8.86, the null hypothesis is rejected so there is a correlation between sex and the histological types of cervical masses.
Source: ENT and CCF department of UHC Gabriel Toure.
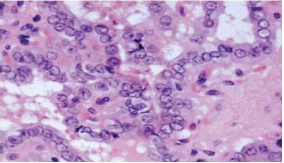
Figure 4. Histological appearance of a papillary thyroid carcinoma, the architecture is in the form of papillae with characteristic overlapping nuclei showing nuclear incisures and nuclear pseudo-inclusions.
4. Discussions
4.1. Sociodemographic Aspects
During our study period, we recorded 51 cases of cervical masses. The hospital prevalence was 1.9% of all ENT hospitalizations. This figure appears to be slightly higher than that of Schlumberger M et al, who found a prevalence of 1.2% of cervical masses in their series of 53 patients at a 3-year interval, and that of Shekar D et al, who found 1.6% of cervical masses in a study of 58 patients at a 5-year interval
[6]
Schlumberger M, et al. Thyroid tumors. 2003. nat clin pract Endocrinol Metab. 2008; 66-70.
[7]
Shekar D, Tufail P, Diane A, Suresh K, MukherJI. Papillary carcinoma in a giant thyroglossal duct cyst. Journal of Clinical Imaging 24(2000): 75-77.
[6, 7]
. In our study, the female sex was predominant, 72.5%, with a sex ratio of 0.37. These data corroborate with those of Schlumberger M et al, who found a female predominance
[6]
Schlumberger M, et al. Thyroid tumors. 2003. nat clin pract Endocrinol Metab. 2008; 66-70.
[6]
. In our study, the age group [60-74 years] was the most represented, representing 47.1% of the population and the extremes ranging from 6 years to 85 years. The average age of our sample was 48.5 years. On the other hand, in the Kisra M study carried out in Rabat on 53 patients, the age group [10-15 years] was the most represented, representing 49.1% of the population with an average age of discovery of 5.86 years
[8]
Kisra M. Cervical masses in children: approximately 53 cases. Rabat (Morocco), Medical thesis, University of Rabat 2013, 1-47.
[8]
. The age of discovery of cervical masses in our patients varies from one pathology to another.
In our sample, 4/5 of the patients were aged less than 10 years at the time of diagnosis of thyroglossal duct cyst (TDC). These thyroglossal duct cysts are a congenital anomaly characterized by the persistence of the thyroid gland migration duct and are found mainly in young children, most often before the age of 10 years in the literature
Gupta P, Maddalozzo J. Preoperative ultrasound in suspected thyroglossal duct cysts. Otolaryngology Arch Head Neck Surgery 2001; 127: 200-2.
[9, 10]
.
In our study, 33 patients had a thyroid body tumor, or 64.7% of the sample, and the female sex was the majority. This result is consistent with that of Mc Call et al
[11]
WassefM, Vielh P. Cervical cystic lesions. Ann des pathologies 2008, 28: 84-6.
[11]
. Thyroid tumors are common in women and several factors are known such as hormonal factor, genetics, dietary habits and exposure to ionizing radiation.
Cervical cystic lymphangioma represented 02 cases or 3.92% of the sample and all these patients were under 14 years old. This result is significantly lower than that of Chafik W et al, whose average age was 23 years. Our result is close to that of Nguema et al, who found in their series an average age of less than 12 years
[12]
Mohamed Mliha Touati et al. Thyroid carcinomas: epidemiological, clinical and therapeutic profiles, based on 102 cases. Pan African Medical Journal. 2015; 21: 59.
Chafik W. Cystic cervical lymphangioma in children (approximately 25 cases). Medical thesis, Mohammed V University, Faculty of Medicine and Pharmacy of Rabat, 2000, no. 55.
[12, 13]
.
4.2. Diagnostic and Therapeutic Aspects
Palpitations were present in 54.9% of patients, this sign is part of the clinical manifestations of hyperthyroidism especially in the toxic thyroid nodule. Other associated signs were neck pain 23.5%; dyspnea 9.8%; dysphonia 5.9% and dysphagia 5.9% which can be related either to compression of the upper aerodigestive tract by the mass, or to nervous infiltration or to a secondary location of a malignant tumor. The clinical appearance of the mass is a prognostic factor, it allows the surgeon to be guided by its mobility, illustrating its non-adherence to neighboring organs
[14]
Miloundjaa J, ManfoumbiNgomaa AB, MbaEllab, NguemaEdzangL, N'zoubaA. Cystic cervicofacial lymphangiomas in children in Gabon. Annals of otorhinolaryngology and cervicofacial surgery, 124(2007), 277-284.
[14]
.
All our patients underwent ultrasound of the mass. Cervical ultrasound is the first-line examination in the majority of cases of cervical masses because it is non-invasive, less expensive and more accessible. It determines the size of the lesion, its relationship to the vessels and the aerodigestive axis, as well as the damage caused to the fat
[15]
Fontanel J, Poitou F, Klossek J. Tumors of the salivary glands. EMC Oto-rhino-laryngie (Paris, France) 20628-B10-1995, 10.
[15]
. In the case of thyroid nodules, microcalcification, central vascularization, irregular contour and shape of the nodule are signs of malignancy by ultrasound
[16]
Prophylaxis of iodine deficiency disorders (IDD) by silicone iodine diffusers introduced into wells and boreholes. Thesis med Bamako 1989, M59.
[16]
. On ultrasound, cervical cystic lymphangiomas give the appearance of a compressible multilobed lateral cystic mass with thin septa
[17]
S., Djafarou, BA, Inoussa, BD, Timi, N. and Sani, R. (2020). Six-Year Review of Thyroglossal Tract Cyst Surgery at the ENT and Head and Neck Surgery Department of the National Hospital of Niamey (Niger). HEALTH SCIENCES AND DISEASES, 21(5).
. In the presence of parotid masses, ultrasound allows to know the heterogeneous or homogeneous appearance, the echogenicity or even the regular borders with the facial nerve. In front of the thyroglossal duct cyst, ultrasound showed a well-defined, median, anechoic cystic subcutaneous mass
[15]
Fontanel J, Poitou F, Klossek J. Tumors of the salivary glands. EMC Oto-rhino-laryngie (Paris, France) 20628-B10-1995, 10.
[15]
.
A computed tomography scan was performed in the 02 patients with cervical cystic lymphangioma. This is a crucial examination in the management of large and compressive masses at the cervicothoracic level and in other locations, as it allows the exploration of the primary tumor and any cranio-orbital and epidural bone extension
[13]
Chafik W. Cystic cervical lymphangioma in children (approximately 25 cases). Medical thesis, Mohammed V University, Faculty of Medicine and Pharmacy of Rabat, 2000, no. 55.
[13]
.
Histology was performed on all 51 patients in our study, and the histological types found were 3 cases of vesicular adenoma of the thyroid gland, 03 cases of papillary carcinoma of the thyroid, 10 cases of pleomorphic adenoma of the parotid gland, 05 cases of thyroglossal duct cyst, 02 cases of cervical cystic lymphangioma with respectively and 1 case of adenoid cystic carcinoma of the parotid gland. Kisra M et al found the following histological forms: thyroglossal duct cyst 18 cases, differentiated thyroid cancer 10 cases and cystic lymphangioma 07 cases
[7]
Shekar D, Tufail P, Diane A, Suresh K, MukherJI. Papillary carcinoma in a giant thyroglossal duct cyst. Journal of Clinical Imaging 24(2000): 75-77.
[7]
.
In our series, all patients underwent surgery, and this surgery depended on the location and extension of the mass. The surgical approach to masses varies depending on their location. Thus, the surgical approach was the Kocher type incision in all cases of median compartment masses, Paul André L in surgery for cystic lymphangioma and Redon S in cases of parotid tumors. Thyroid surgery was performed in 33 cases including 22 cases of total thyroidectomy, 7 cases of subtotal and 4 cases of lobectomy. Total or subtotal thyroidectomy is performed in the case of multinodular nodules or malignant thyroid tumors, while lobectomy is performed in the case of a lesion limited to a single lobule
[18]
Tunkel DE, Domenach EE. Radioisotopic prion scintigraphy of the thyroid gland at thyroglossal duct excision. Arch Otorhinolaryngology Head Neck. 1998, 124: 597-599.
[18]
.
Thyroglossal duct cyst excision in our study was performed using the Sistrunk technique involving hyoid bone dissection and systematic hyoid bone removal. The choice of this technique has been widely shared in the literature
[15]
Fontanel J, Poitou F, Klossek J. Tumors of the salivary glands. EMC Oto-rhino-laryngie (Paris, France) 20628-B10-1995, 10.
[15]
.
In our series, in the case of pleomorphic adenomas of the parotid gland, an exofacial parotidectomy was performed in only one case, a total parotidectomy was performed in 10 cases. The surgical approach to the parotid gland in the literature is dominated by total parotidectomy with a high rate of pleomorphic adenomas of the parotid gland, exofacial parotidectomy is reserved for lesions limited to the superficial lobe
[19]
Petelle B, Sauvaget E and Tran Ba Huy P. Parotidectomies. Encycl Méd Chir (Elsevier SAS, Paris, all rights reserved), Surgical Techniques - Head and Neck, 46-510, 2003, 11 p.
[19]
. All cases of cervical cystic lymphangioma in our series underwent surgical excision by cervicotomy. This surgery depends on the skill of the surgeon in relation to the characteristics of the cervical cystic lymphangioma, the same observation has been made in the literature
[17]
S., Djafarou, BA, Inoussa, BD, Timi, N. and Sani, R. (2020). Six-Year Review of Thyroglossal Tract Cyst Surgery at the ENT and Head and Neck Surgery Department of the National Hospital of Niamey (Niger). HEALTH SCIENCES AND DISEASES, 21(5).
We had complications such as unilateral inferior laryngeal nerve (ILN) paralysis in 2 cases of papillary thyroid carcinoma, total peripheral facial paralysis (FP) in one case of adenoid cystic carcinoma of the parotid gland and then in 6 cases of facial paresis which all recovered within 3 months to 6 months. Unilateral ILN paralysis was observed in 2 patients with papillary thyroid carcinoma which represents 3.2% of ILN dissected during our thyroidectomy cases. The risk of inferior laryngeal paralysis varies from 1 to 5% in the literature according to the experience of the surgeon
[20]
Remacle M., Lawson G. Laryngeal paralysis. EMC (Elsevier SAS, Paris), Otorhinolaryngology, 20-675-A-10, 2006.
[20]
. In both of our cases, we demonstrated intraoperative infiltration of the inferior laryngeal nerve by the tumor.
Infiltration of the facial nerve in malignant tumors of the parotid gland is very common, especially in cases of adenoid cystic carcinoma, and preservation of the nerve is difficult on the carcinological level
[19]
Petelle B, Sauvaget E and Tran Ba Huy P. Parotidectomies. Encycl Méd Chir (Elsevier SAS, Paris, all rights reserved), Surgical Techniques - Head and Neck, 46-510, 2003, 11 p.
[19]
. The facial nerve was infiltrated in one case of adenoid cystic carcinoma, which led to its intraoperative sacrifice; however, cases of paresthesia are due to intraoperative lengthening or compression, as in these cases recovery is possible afterwards.
5. Conclusion
Cervical masses are one of the most common reasons for ENT and head and neck consultations. Their symptoms are often very rich and require a very good knowledge of anatomy, physiology, and pathophysiology. Etiologies can range from a benign tumor to cancer. Imaging and histology are essential for diagnosis. The prognosis is excellent if treatment is performed early; the occurrence of complications depends on the surgeon's experience and delay in treatment. The fear of malignancy should be a constant concern for the ENT or head and neck practitioner, who must not forget a multidisciplinary approach in this context.
Abbreviations
ENT-HNS
Ear Noose Throat and Head and Neck Surgery
TDC
Thyroglossal Duct Cyst
UHC
University Hospital Center
ILN
Inferior Laryngeal Nerve
FP
Facial Paralysis
Author Contributions
Diamouténé Boubacar Sidiki: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Writing - original draft
Konate Oumar: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Writing - original draft
David SF, Mary EF. Thyroglossal duct anomalies and other semi-congenital anomalies in pediatrics. Surge 2006. Vol: 157. Ref: 55.
[2]
Turkington JR, Paterson A, Sweeney LE, Thornbury GD. Neck masses in children. Br J Radial 2005, 78: 75-85.
[3]
T. Kennel, R. Garrel, V. Costes, P. Boisselier, L. Crampette, V. Favier, Carcinomas of unknown primary origin of the head and neck French Annals of Otorhinolaryngology and Head and Neck Pathology, 136, 2019 Pages 184-192.
P. Costa de Araujo, O. Battisti. How to explore cervical masses in children. Rev Med Liège 2010; 65: 1: 40-45.
[5]
Murat S, Sedar B, Selkut L, Mehmet AS. Unusual presentation and location of thyroglossary duct cyst in children. Otolaryngology Head Neck Surg 2007, 136: 854-5.
[6]
Schlumberger M, et al. Thyroid tumors. 2003. nat clin pract Endocrinol Metab. 2008; 66-70.
[7]
Shekar D, Tufail P, Diane A, Suresh K, MukherJI. Papillary carcinoma in a giant thyroglossal duct cyst. Journal of Clinical Imaging 24(2000): 75-77.
[8]
Kisra M. Cervical masses in children: approximately 53 cases. Rabat (Morocco), Medical thesis, University of Rabat 2013, 1-47.
Gupta P, Maddalozzo J. Preoperative ultrasound in suspected thyroglossal duct cysts. Otolaryngology Arch Head Neck Surgery 2001; 127: 200-2.
[11]
WassefM, Vielh P. Cervical cystic lesions. Ann des pathologies 2008, 28: 84-6.
[12]
Mohamed Mliha Touati et al. Thyroid carcinomas: epidemiological, clinical and therapeutic profiles, based on 102 cases. Pan African Medical Journal. 2015; 21: 59.
Chafik W. Cystic cervical lymphangioma in children (approximately 25 cases). Medical thesis, Mohammed V University, Faculty of Medicine and Pharmacy of Rabat, 2000, no. 55.
[14]
Miloundjaa J, ManfoumbiNgomaa AB, MbaEllab, NguemaEdzangL, N'zoubaA. Cystic cervicofacial lymphangiomas in children in Gabon. Annals of otorhinolaryngology and cervicofacial surgery, 124(2007), 277-284.
[15]
Fontanel J, Poitou F, Klossek J. Tumors of the salivary glands. EMC Oto-rhino-laryngie (Paris, France) 20628-B10-1995, 10.
[16]
Prophylaxis of iodine deficiency disorders (IDD) by silicone iodine diffusers introduced into wells and boreholes. Thesis med Bamako 1989, M59.
[17]
S., Djafarou, BA, Inoussa, BD, Timi, N. and Sani, R. (2020). Six-Year Review of Thyroglossal Tract Cyst Surgery at the ENT and Head and Neck Surgery Department of the National Hospital of Niamey (Niger). HEALTH SCIENCES AND DISEASES, 21(5).
Tunkel DE, Domenach EE. Radioisotopic prion scintigraphy of the thyroid gland at thyroglossal duct excision. Arch Otorhinolaryngology Head Neck. 1998, 124: 597-599.
[19]
Petelle B, Sauvaget E and Tran Ba Huy P. Parotidectomies. Encycl Méd Chir (Elsevier SAS, Paris, all rights reserved), Surgical Techniques - Head and Neck, 46-510, 2003, 11 p.
[20]
Remacle M., Lawson G. Laryngeal paralysis. EMC (Elsevier SAS, Paris), Otorhinolaryngology, 20-675-A-10, 2006.
Sidiki, D. B., Oumar, K., Issa, K. F., Ibrahim, D., Drissa, K., et al. (2025). Cervical Masses: Epidemiological, Diagnostic and Therapeutic Aspects: 51 Cases. International Journal of Otorhinolaryngology, 11(2), 18-23. https://doi.org/10.11648/j.ijo.20251102.13
Sidiki, D. B.; Oumar, K.; Issa, K. F.; Ibrahim, D.; Drissa, K., et al. Cervical Masses: Epidemiological, Diagnostic and Therapeutic Aspects: 51 Cases. Int. J. Otorhinolaryngol.2025, 11(2), 18-23. doi: 10.11648/j.ijo.20251102.13
@article{10.11648/j.ijo.20251102.13,
author = {Diamouténé Boubacar Sidiki and Konate Oumar and Kone Fatogoma Issa and Dicko Ibrahim and Konate Drissa and Ouane Aissata and Coulibaly Assitan Kolé and Dicko Hawa and Coulibaly Oumou and Traoré Kadidiatou and Ganaba Abdoulaye Modibo and Cisse Naouma and Konate N'faly and Diarra Kassim and Guindo Boubacary and Soumaoro Siaka and Singaré Kadidiatou and Keita Mohamed Amadou},
title = {Cervical Masses: Epidemiological, Diagnostic and Therapeutic Aspects: 51 Cases
},
journal = {International Journal of Otorhinolaryngology},
volume = {11},
number = {2},
pages = {18-23},
doi = {10.11648/j.ijo.20251102.13},
url = {https://doi.org/10.11648/j.ijo.20251102.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijo.20251102.13},
abstract = {Cervical masses are defined as a set of benign or malignant neoformations developed in the neck, in its medial or lateral part, from the different anatomical structures that form the neck (vessels, nerves, lymph nodes, viscera, muscles). We conducted a descriptive retrospective study in the Otorhinolaryngology and Head and Neck Surgery Department of Gabriel Touré University Hospital in Bamako from 2008 to 2017. We collected 51 cases with clinical, paraclinical, and treatment data. Females were the most represented (72.5%), the mean age was 48.5 years, and the range was from 6 to 86 years. 38 cases were cervical masses of the medial compartment, 13 cases were cervical masses of the lateral compartment. Thyroid gallbladder adenoma accounted for 30 cases, or 58.82%, followed by pleomorphic parotid adenoma with 10 cases, or 19.60%. Total thyroidectomy was the most commonly performed type of surgery with 22 cases or 43.14%, followed by total parotidectomy with 11 cases or 21.57%. All our patients treated with thyroidectomy received hormone replacement therapy. The outcome was good in 40 cases, or 78.43% with unilateral recurrent paralysis in 02 cases, 01 case of peripheral facial paralysis, 06 cases of facial paresis.},
year = {2025}
}
TY - JOUR
T1 - Cervical Masses: Epidemiological, Diagnostic and Therapeutic Aspects: 51 Cases
AU - Diamouténé Boubacar Sidiki
AU - Konate Oumar
AU - Kone Fatogoma Issa
AU - Dicko Ibrahim
AU - Konate Drissa
AU - Ouane Aissata
AU - Coulibaly Assitan Kolé
AU - Dicko Hawa
AU - Coulibaly Oumou
AU - Traoré Kadidiatou
AU - Ganaba Abdoulaye Modibo
AU - Cisse Naouma
AU - Konate N'faly
AU - Diarra Kassim
AU - Guindo Boubacary
AU - Soumaoro Siaka
AU - Singaré Kadidiatou
AU - Keita Mohamed Amadou
Y1 - 2025/08/07
PY - 2025
N1 - https://doi.org/10.11648/j.ijo.20251102.13
DO - 10.11648/j.ijo.20251102.13
T2 - International Journal of Otorhinolaryngology
JF - International Journal of Otorhinolaryngology
JO - International Journal of Otorhinolaryngology
SP - 18
EP - 23
PB - Science Publishing Group
SN - 2472-2413
UR - https://doi.org/10.11648/j.ijo.20251102.13
AB - Cervical masses are defined as a set of benign or malignant neoformations developed in the neck, in its medial or lateral part, from the different anatomical structures that form the neck (vessels, nerves, lymph nodes, viscera, muscles). We conducted a descriptive retrospective study in the Otorhinolaryngology and Head and Neck Surgery Department of Gabriel Touré University Hospital in Bamako from 2008 to 2017. We collected 51 cases with clinical, paraclinical, and treatment data. Females were the most represented (72.5%), the mean age was 48.5 years, and the range was from 6 to 86 years. 38 cases were cervical masses of the medial compartment, 13 cases were cervical masses of the lateral compartment. Thyroid gallbladder adenoma accounted for 30 cases, or 58.82%, followed by pleomorphic parotid adenoma with 10 cases, or 19.60%. Total thyroidectomy was the most commonly performed type of surgery with 22 cases or 43.14%, followed by total parotidectomy with 11 cases or 21.57%. All our patients treated with thyroidectomy received hormone replacement therapy. The outcome was good in 40 cases, or 78.43% with unilateral recurrent paralysis in 02 cases, 01 case of peripheral facial paralysis, 06 cases of facial paresis.
VL - 11
IS - 2
ER -
Sidiki, D. B., Oumar, K., Issa, K. F., Ibrahim, D., Drissa, K., et al. (2025). Cervical Masses: Epidemiological, Diagnostic and Therapeutic Aspects: 51 Cases. International Journal of Otorhinolaryngology, 11(2), 18-23. https://doi.org/10.11648/j.ijo.20251102.13
Sidiki, D. B.; Oumar, K.; Issa, K. F.; Ibrahim, D.; Drissa, K., et al. Cervical Masses: Epidemiological, Diagnostic and Therapeutic Aspects: 51 Cases. Int. J. Otorhinolaryngol.2025, 11(2), 18-23. doi: 10.11648/j.ijo.20251102.13
@article{10.11648/j.ijo.20251102.13,
author = {Diamouténé Boubacar Sidiki and Konate Oumar and Kone Fatogoma Issa and Dicko Ibrahim and Konate Drissa and Ouane Aissata and Coulibaly Assitan Kolé and Dicko Hawa and Coulibaly Oumou and Traoré Kadidiatou and Ganaba Abdoulaye Modibo and Cisse Naouma and Konate N'faly and Diarra Kassim and Guindo Boubacary and Soumaoro Siaka and Singaré Kadidiatou and Keita Mohamed Amadou},
title = {Cervical Masses: Epidemiological, Diagnostic and Therapeutic Aspects: 51 Cases
},
journal = {International Journal of Otorhinolaryngology},
volume = {11},
number = {2},
pages = {18-23},
doi = {10.11648/j.ijo.20251102.13},
url = {https://doi.org/10.11648/j.ijo.20251102.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijo.20251102.13},
abstract = {Cervical masses are defined as a set of benign or malignant neoformations developed in the neck, in its medial or lateral part, from the different anatomical structures that form the neck (vessels, nerves, lymph nodes, viscera, muscles). We conducted a descriptive retrospective study in the Otorhinolaryngology and Head and Neck Surgery Department of Gabriel Touré University Hospital in Bamako from 2008 to 2017. We collected 51 cases with clinical, paraclinical, and treatment data. Females were the most represented (72.5%), the mean age was 48.5 years, and the range was from 6 to 86 years. 38 cases were cervical masses of the medial compartment, 13 cases were cervical masses of the lateral compartment. Thyroid gallbladder adenoma accounted for 30 cases, or 58.82%, followed by pleomorphic parotid adenoma with 10 cases, or 19.60%. Total thyroidectomy was the most commonly performed type of surgery with 22 cases or 43.14%, followed by total parotidectomy with 11 cases or 21.57%. All our patients treated with thyroidectomy received hormone replacement therapy. The outcome was good in 40 cases, or 78.43% with unilateral recurrent paralysis in 02 cases, 01 case of peripheral facial paralysis, 06 cases of facial paresis.},
year = {2025}
}
TY - JOUR
T1 - Cervical Masses: Epidemiological, Diagnostic and Therapeutic Aspects: 51 Cases
AU - Diamouténé Boubacar Sidiki
AU - Konate Oumar
AU - Kone Fatogoma Issa
AU - Dicko Ibrahim
AU - Konate Drissa
AU - Ouane Aissata
AU - Coulibaly Assitan Kolé
AU - Dicko Hawa
AU - Coulibaly Oumou
AU - Traoré Kadidiatou
AU - Ganaba Abdoulaye Modibo
AU - Cisse Naouma
AU - Konate N'faly
AU - Diarra Kassim
AU - Guindo Boubacary
AU - Soumaoro Siaka
AU - Singaré Kadidiatou
AU - Keita Mohamed Amadou
Y1 - 2025/08/07
PY - 2025
N1 - https://doi.org/10.11648/j.ijo.20251102.13
DO - 10.11648/j.ijo.20251102.13
T2 - International Journal of Otorhinolaryngology
JF - International Journal of Otorhinolaryngology
JO - International Journal of Otorhinolaryngology
SP - 18
EP - 23
PB - Science Publishing Group
SN - 2472-2413
UR - https://doi.org/10.11648/j.ijo.20251102.13
AB - Cervical masses are defined as a set of benign or malignant neoformations developed in the neck, in its medial or lateral part, from the different anatomical structures that form the neck (vessels, nerves, lymph nodes, viscera, muscles). We conducted a descriptive retrospective study in the Otorhinolaryngology and Head and Neck Surgery Department of Gabriel Touré University Hospital in Bamako from 2008 to 2017. We collected 51 cases with clinical, paraclinical, and treatment data. Females were the most represented (72.5%), the mean age was 48.5 years, and the range was from 6 to 86 years. 38 cases were cervical masses of the medial compartment, 13 cases were cervical masses of the lateral compartment. Thyroid gallbladder adenoma accounted for 30 cases, or 58.82%, followed by pleomorphic parotid adenoma with 10 cases, or 19.60%. Total thyroidectomy was the most commonly performed type of surgery with 22 cases or 43.14%, followed by total parotidectomy with 11 cases or 21.57%. All our patients treated with thyroidectomy received hormone replacement therapy. The outcome was good in 40 cases, or 78.43% with unilateral recurrent paralysis in 02 cases, 01 case of peripheral facial paralysis, 06 cases of facial paresis.
VL - 11
IS - 2
ER -