Abstract
On July 7, 2022, a blood sample from a resident of Adansi North District, Ashanti region of Ghana, tested positive for Marburg virus disease. Within 24 hours of confirmation, a rapid outbreak response was initiated. This report presents results of response activities conducted to adequately response to the outbreak. A regional rapid response team was activated consisting of specialized teams to conduct case finding, case management and isolation, contact listing and follow up, sample collection and testing, and community engagement. Support from the National Surveillance Department and WHO were provided. An investigation was also carried out to identify the potential source of infection. Laboratory virus isolation and sequencing were performed by the NMIMR and corroborated by the Institute Pasteur in Dakar to identify the strain of Marburg virus. One hundred and ninety-eight closed contacts were epidemiologically investigated, with blood samples of sixteen (16) randomly selected tested for MVD. Standard case definition of MVD was used to screen all. No case was suspected based on the case definition used. Two closed contacts were confirmed as MVD after the follow- up. Of the three confirmed MVD cases, two died, yielding a case fatality rate of 67.0%. All three cases form a single nuclear family and 50% (2/3) of the MVD cases were male. The cases had clinical symptoms of fever, chills, general malaise, and bleeding from the nose and mouth. Genetic sequencing results indicated that the Marburg virus genomes were related to the sequence from the 2021 outbreak and overall, group with sequences obtained from bats in Sierra Leone and an outbreak that occurred in Angola in 2004-2005. This outbreak of MVD occurred as a family cluster with no additional transmission outside of the three related cases. Rapid case detection, prompt laboratory testing at the NMIMR and presence of pre-trained, well-prepared national and district rapid response teams facilitated the containment and control of this outbreak.
Keywords
Case, Marburg, Outbreak, Surveillance, Ghana
1. Introduction
Marburg hemorrhagic fever (Marburg HF), first recognized in 1967, is a rare but severe hemorrhagic fever which affects both humans and non-human primates
. The first ever human outbreak occurred simultaneously in laboratories in Marburg and Frankfurt, Germany and in Belgrade, Yugoslavia (now Serbia) when thirty-one laboratory workers became ill after they had been exposed to imported African green monkeys or their tissues while conducting research to produce vaccines and sera and later infecting several medical personnel and family members who had cared for them
. The first three (3) patients in Marburg and another three patients in Frankfurt had had direct contact with the green monkeys, handling materials or their organs from the same group of monkeys from Uganda
. Subsequently, outbreaks and sporadic cases have been reported in Angola, the Democratic Republic of the Congo, Kenya, South Africa (in a person with recent travel history to Zimbabwe) and Uganda. In 2008, two independent cases were reported in travelers who had visited a cave inhabited by Rousettus bat colonies in Uganda
.
In Africa, the first recognized outbreak of Marburg virus disease since the original epidemic in West Germany and Yugoslavia in 1967, occurred in South Africa in February 1975. The primary case was in a young Australian man, who was admitted to the Johannesburg Hospital after having toured Rhodesia. Two secondary cases occurred, one being in the first patient's travelling companion, and the other in a nurse
| [11] | Trappler, B., Clausen, L., Meyers, A. M., Kew, M. C., Bothwell, T. H., Sher, R., Miller, G. B., Schneider, J., & Gear, J. H. S. (1975). Outbreak of Marburg virus disease in Johannesburg. British Medical Journal, 4(5995), 489–493.
https://doi.org/10.1136/bmj.4.5995.489 |
[11]
.
Transmission of Marburg viral disease is in two phases. The initial human infection results from prolonged exposure to mines or caves inhabited by Rousettus bat colonies. After this occurrence, Marburg spreads through human-to-human transmission via direct contact (through broken skin or mucous membranes) with the blood, secretions, organs or other bodily fluids of infected people, and with surfaces and materials (e.g. bedding, clothing) contaminated with these fluids
. In Congo, the primary risk of transmission of Marburg virus to humans was identified to have likely occurred via exposure to a still unidentified reservoir in the local mines. Secondary transmission appears to be less common with Marburg virus than with Ebola virus, the other known filovirus
| [5] | Bausch, D. G., Borchert, M., Grein, T., Roth, C., Swanepoel, R., Libande, M. L., Talarmin, A., Bertherat, E., Muyembe-Tamfum, J. J., Tugume, B., Colebunders, R., Kondé, K. M., Pirard, P., Olinda, L. L., Rodier, G. R., Campbell, P., Tomori, O., Ksiazek, T. G., & Rollin, P. E. (2003). Risk Factors for Marburg Hemorrhagic Fever, Democratic Republic of the Congo. In Emerging Infectious Diseases (Vol. 9, Issue 12).
https://doi.org/10.3201/eid0912.030355 |
[5]
. Marburg virus can be transmitted sexually, and studies of Ebolavirus have shown that viral RNA can be detected in semen for up to 407 days
| [10] | Nyakarahuka, L., Shoemaker, T. R., Balinandi, S., Chemos, G., Kwesiga, B., Mulei, S., Kyondo, J., Tumusiime, A., Kofman, A., Masiira, B., Whitmer, S., Brown, S., Cannon, D., Chiang, C. F., Graziano, J., Morales-Betoulle, M., Patel, K., Zufan, S., Komakech, I., … Lutwama, J. J. (2018). Marburg virus disease outbreak in Kween District Uganda, 2017: Epidemiological and laboratory findings. PLoS Neglected Tropical Diseases, 13(3). https://doi.org/10.1371/journal.pntd.0007257 |
[10]
.
Bats have been implicated as likely natural reservoir hosts based most recently on an investigation of cases among miners infected in 2007 at the Kitaka mine, Uganda, which contained a large population of Marburg virus infected
Rousettus aegyptiacus fruit bats. After a Q-RT-PCR analysis of 1,622 bats were captured and tested for Marburg virus using the liver and spleen tissues indicated approximately 2.5% of the bats being actively infected with Marburg virus consistent with Q-RT-PCR-positive lung, kidney, colon and reproductive tissues found in oral, urine, fecal or sexual transmissions of the infected individuals
| [3] | Amman, B. R., Carroll, S. A., Reed, Z. D., Sealy, T. K., Balinandi, S., Swanepoel, R., Kemp, A., Erickson, B. R., Comer, J. A., Campbell, S., Cannon, D. L., Khristova, M. L., Atimnedi, P., Paddock, C. D., Kent Crockett, R. J., Flietstra, T. D., Warfield, K. L., Unfer, R., Katongole-Mbidde, E., … Towner, J. S. (2012). Seasonal Pulses of Marburg Virus Circulation in Juvenile Rousettus aegyptiacus Bats Coincide with Periods of Increased Risk of Human Infection. PLoS Pathogens, 8(10).
https://doi.org/10.1371/journal.ppat.1002877 |
[3]
. The incubation periods for Marburg infections resulting from well-defined exposures ranged from 5–9 days, and 3–13 days
| [8] | Kortepeter, M. G., Dierberg, K., Shenoy, E. S., & Cieslak, T. J. (2020). Marburg virus disease: A summary for clinicians. International Journal of Infectious Diseases, 99.
https://doi.org/10.1016/j.ijid.2020.07.042 |
[8]
but can last from 2–21 days and infected individuals are not viremic until initial symptom onset
| [10] | Nyakarahuka, L., Shoemaker, T. R., Balinandi, S., Chemos, G., Kwesiga, B., Mulei, S., Kyondo, J., Tumusiime, A., Kofman, A., Masiira, B., Whitmer, S., Brown, S., Cannon, D., Chiang, C. F., Graziano, J., Morales-Betoulle, M., Patel, K., Zufan, S., Komakech, I., … Lutwama, J. J. (2018). Marburg virus disease outbreak in Kween District Uganda, 2017: Epidemiological and laboratory findings. PLoS Neglected Tropical Diseases, 13(3). https://doi.org/10.1371/journal.pntd.0007257 |
[10]
.
Marburg virus starts with high fever, headache, and fatigue. Many infected people have severe hemorrhagic symptoms within seven days. The mortality rates ranged from 24% to 88% in past outbreak, depending on case management
| [1] | Aborode, A. T., Wireko, A. A., Bel-Nono, K. N., Quarshie, L. S., Allison, M., & Bello, M. A. (2022). Marburg virus amidst COVID-19 pandemic in Guinea: Fighting within the looming cases. In International Journal of Health Planning and Management (Vol. 37, Issue 1).
https://doi.org/10.1002/hpm.3332 |
[1]
. Other features of the illness included myalgia, vomiting and diarrhoea, hepatitis, a characteristic maculopapular rash, leucopenia, thrombocytopenia, and a bleeding tendency
| [11] | Trappler, B., Clausen, L., Meyers, A. M., Kew, M. C., Bothwell, T. H., Sher, R., Miller, G. B., Schneider, J., & Gear, J. H. S. (1975). Outbreak of Marburg virus disease in Johannesburg. British Medical Journal, 4(5995), 489–493.
https://doi.org/10.1136/bmj.4.5995.489 |
[11]
. The disease is characterized by a relatively small reproduction number and by a relatively long generation time. Such factors, along with the extremely high severity and fatality, support the rare occurrence of large epidemics in human populations
.
Ghana on the 15th of July 2022 declared outbreak of Marburg Disease in the Adansi North district in the Ashanti Region of Ghana. During a zoom meeting on the outbreak, it was mentioned that the two (2) cases reported to St. Benito Menni Hospital, Dompoase on the 26th and 28th June 2022. Samples were picked and the results were positive for Marburg disease. Both cases died few days later.
This report seeks to document the activities conducted during the outbreak to provide logical evidence for further response activities to adequately combat infectious diseases.
2. Methods
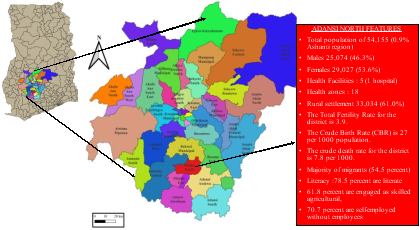
Figure 1. Map of the Adansi North District in Ghana.
2.1. Description of the Outbreak Area
The Adansi North District, located between Longitude 1.50W, latitude 1.4 N and Longitude 1.5W latitude 6.30 N was created by a Legislative Instrument (LI 1758) dated 17th February 2004. The District Capital is located at Fomena with a population of 54,155 representing 0.9 percent of the region’s total population. Males constitute 46.3 percent and females represent 53.6 percent. Sixty one percent of the population is rural according to 2021 population and Housing Census (PHC 2021). The administrative head of the district is at Fomena, which is located 70 km from Kumasi on the Cape Coast main road.
2.2. Public Health Actions Undertaken
The actions were taken based on the levels of implementation. The levels were District/Facility, Regional and National.
At the district level activities were focused to enhance community engagement, monitoring of all contacts for 42 days, provision of psychological support to families, facilitation, and training of CBSVs to do case search, contact tracing, and risk communication activities.
The Regional level led the supervision and monitoring, issuance of alerts to all districts, conducted further investigations on the outbreak, supported the district to conduct active clinical records review and sensitization of clinical staff, supported with contact tracing and follow-up and the training of on community-based surveillance for volunteers and supervisors.
Additionally, regional rapid response team (RRT) was constituted to support the Adansi North district for surveillance, risk communication, and contact tracing.
At the national level, another rapid response team involving staff at the national Ghana Health Service headquarters and Partners were constituted to support the regional and district response teams for detailed investigations. Community engagements with Intensive risk communication in the affected region, identification of community of interest and the listing of contacts, Heightened Community Based Surveillance in the affected district and Facility-based orientation of health staff on standard case definition of VHFs and other epidemic prone diseases were conducted by the national office.
Provision of more PPEs and other logistics by GHS/MOH and Partners, Development of training tools and education materials, facilitation of Transportation of samples to NMIMR.
National Response Plan was developed to enhance coordination with Savannah and Western Region Regional Health Directorates, ensure provision of logistics including PPEs. Environmental Assessment by Wildlife at affected districts (Adansi North, Bekwai, Prestea Huni Valley, Sawla Tuna Kalba) to promote collaboration with Wildlife and Partners to conduct a nationwide Risk Assessment.
2.2.1. Health Staff Sensitization
Figure 2. Sensitization of Health staff and Training of community volunteers for contact tracing.
Health staff from the Adansi North District, Bekwai in the Ashanti region as well as those in the resident district of the case which is the Prestea Huni Valley Municipality in the western region of Ghana were all oriented on the Marburg disease. The officers included persons who are involved in surveillance activities to enhance their capacity in conducting active records review and conduct contact tracing activities. The clinical staff were provided insights into the signs and symptoms of the disease. They were also oriented on the diagnosis, sample taking and case management practices including supportive treatment. The laboratory staff were oriented on sample taking, specimen packaging, temperature medium and transportation to the designated laboratory (Noguchi Memorial Institute for Medical Research).
Another section of training was provided for community-based surveillance officers to support with contact training, case search and support community activities. They were equipped to support community sensitization and awareness creation.
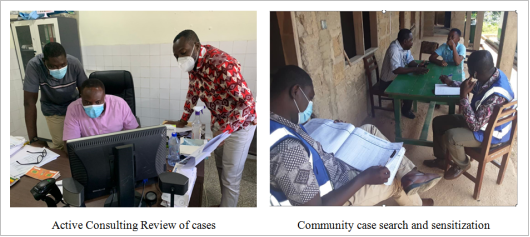
2.2.2. Stakeholders and Community Engagement
Engagement with community members and well-meaning people were immediately initiated to forestall calm and install confidence in the health team to control the outbreak. This was necessary to harness community support and resources to aid in the field investigation. It provided the epidemiologists and disease control officers to sensitize the leaders on the outbreak, the diagnosis process, treatment available and preventive measures instituted.
Figure 3. Stakeholders and Community Engagement.
3. Findings
3.1. Case History
The Adansi North District and Bekwai Municipal were the initial epicentre of this Marburg viral disease outbreak. However, investigations shown later that the cases were imported from the Prestea Huni Valley in the Western Region, and Sawla Tuna Kalba in the Savanna Regions of Ghana.
The two (2) cases were confirmed by Noguchi Memorial Institute for Medical Research as Marburg Virus Disease on 7th July 2022 pending corroboration by the Institute Pasteur in Dakar in line with standard protocol. The first case was subsequently corroborated by Institute Pasteur in Dakar (IPD) on 15th July 2022 to be indeed Marburg viral disease. The common signs and symptoms were fever, malaise, reddish eyes, and bleeding from the nose and mouth.
Several contacts were identified and screened. One close contact (a one-year two-month-old son of the case) got ill after the maximum incubation period, admitted on 17 July 2022, and died on the third day of admission. He tested positive together with his close contact, the mother, a 24-year-old female and wife of the disease (1st case).
3.2. Contact Tracing and Sample Collection
Contact tracing was initiated soon after the confirmation. The search for the source of infection for the first case was linked to the Mfante Akura community in Prestea Huni Valley municipal which was outside the jurisdiction of the Ashanti Region. This necessitated the regional team to alert Prestea Huni Valley Municipal in the Western region of Ghana to visit the deceased community for further investigation. The Ashanti regional team focused on Adansi North District and the Bekwai Municipal.
Implementation of several interventions were focused on three regions Ashanti, Savannah and Western. A cumulative list of 118 contacts in 3 districts in the 3 regions was identified, 50 from Ashanti, 48 from Savannah and 20 from the Western regions of Ghana. 19 of the contacts were Health Care Workers, and 99 were close family members, household, or community contacts. All contacts completed the mandatory 21-day follow-up as of the 21st of July 2022. They all didn’t show any sign and symptoms of the disease and therefore were discharged.
Additional 80 contacts were identified in the Savannah Region and were followed up among which 11 were Health Care Workers.
Figure 4. Contact Tracing.
Sample collections were conducted by trained laboratory officers who were part of the response team. All samples collected were shipped to the Noguchi Memorial Institute for Medical research for viral identification and genomic sequencing.
3.3. Case Management
The first suspected case was provisionally diagnosed as Acute Gastro-enteritis and later revised to upper GIT bleed based on signs and symptoms of vomiting, bloody watery diarrhoea, history of fever, chills, generalized malaise, dysuria, bleeding from the nose and mouth, reddish and swollen eyes, bleeding from the abdomen. Medication given were, IV ciprofloxacin 400mg, IV metoclopramide 10mg start, IV metronidazole 500mg, Normal Saline, Ringer’s lactate, IV Buscopan 40mg, Paracetamol 1g tds, vitamin K, passed N-G tube.
The second suspected case, a 51 years old, male, reported at Benito Menni Hospital on 28th June 2022 at 9: 30am. The case presented with abdominal pain, difficulty in breathing, fever, generalized malaise, bleeding from the nose and mouth, redness of the eye. Provisional diagnosis was Upper GIT bleed. The case was IV omeprazole, IV Normal Saline 2L, IV Ringers lactate 2L, IV Buscopan 40mg b.d., syrup antacid 15 mls t.i.d. The case died on 28th June 2022.
The wife and mother of the son of the index case who were part of those screened were later confirmed to be positive. The child shown signs of diarrhoea with some dehydration. These cases received adequate supportive treatment and monitoring by health officials. The child died on 19th July 2022, but the woman survived.
3.4. Active Case Search in Consulting Rooms
Case search was conducted in consulting rooms of the St. Benito Menni Hospital which suspected the case. This was conducted by teams from the region and National Surveillance Department of the Ghana Health Service. This was to identify cases that were missed. At the end of the records review sessions, no cases were missed from the consulting room register review and there were no suspected or probable cases been missed hence follow-up of cases not been carried out.
Figure 5. Active Case Review.
4. Discussion
We investigated a case of Marburg viral disease in the Adansi North District of the Ashanti region of Ghana. This is the first time in the Marburg disease's history that Ghana has had an outbreak. This outbreak however is the second in West Africa, after the first was detected in the year 2021 in Guinea
| [7] | Kika, T. (n.d.). First Infant Dies From Marburg Outbreak, Virus Related to Ebola. |
[7]
. The disease was first identified in early July in two deceased men, ages 26 and 51. The second case, 51-year-old male with a known chronic disease and not linked to the first case was however re-tested and the repeated result from NMIMR on 28
th July was negative for Marburg viral disease. An additional fatality was later confirmed in late July, with a fourth being reported on 28
th July 2022 by the Ghana Health Service. The fourth victim was a 14-month-old boy, making it the first infant death caused by this latest Marburg outbreak. The health service explained that the infant was, in fact, the son of the 26-year-old man who was one of the outbreak's first victims
| [4] | Balibouse, D. (Reuters/Aljazeera). (n.d.). Child infected with Marburg virus dies in Ghana World Health Organization News Al Jazeera. |
[4]
.
Disease surveillance reports at the regional health directorate of the Ashanti region shows on 28th June 2022, the Medical Director of St. Benito Menni Hospital, Dompoase, the first referral hospital in the Adansi North District, notified the District Director of Health Service (DDHS) of two patients with fever, history of fever, chills, general malaise, bleeding from the nose and mouth, bloody stools among others. Since these signs and symptoms are characteristic of viral haemorrhagic fever, in addition to the information that one out of the two cases had died, the situation was immediately considered as a public health emergency. Hence, on the same day, 28th June 2022, a disease outbreak investigative team was immediately constituted to visit the health facility for further investigations. Later in the day the second suspected case also died.
According to report received, the index suspected case started experiencing clinical symptoms in the early hours of 26th June 2022, and reported to St. Benito Menni Hospital, at 11.30 am on 26th June 2022. He was admitted and treated according to the provisional diagnosis of acute Gastro-enteritis, which was later revised to upper GIT bleeding and medication initiated but died at 4.30pm some 29 hours after on 27th June 2022. The second suspected case also started experiencing the same clinical symptoms in the early hours of 28th June 2022, and reported to St. Benito Menni Hospital, at 9.30 am on 28th June 2022, where he was admitted with the provisional diagnosis of upper GIT bleeding and medication initiated but also died at 8.30pm about 11 hours later 28th of June 2022. These incidents prompted the surveillance team to initiate investigations.
On the 29th of June 2022, blood samples were taken from the two diseased and sent alongside with their case-based forms to the Noguchi Memorial Institute for Medical Research (NMIMR), the designated laboratory for viral haemorrhagic fever investigations for the identification of the possible causative agent that may be responsible for the clinical presentations and death of the cases.
While waiting for laboratory confirmation of the suspected cases, the households of the two cases were identified and placed under strict surveillance. Daily calls were made to the family heads to promptly identify the appearance of clinical presentations among any of these household contacts. All clinicians in the index health facility and the three other health centers in the district, were sensitized on the suspected case definition of fever, history of fever, chills, general malaise, bleeding from the nose, eye and mouth, bloody stools, abdominal pain to ensure case finding, management and notification. The Regional Director of Health Service through the Deputy Director of Public Health were promptly notified of the occurrence of the two suspected viral hemorrhagic fever cases on 28th June 2022. The suspected case investigation forms were submitted to the Regional Disease Control Unit along with preliminary case investigation report.
Findings on the environmental risk Assessment for exposure to the causative organism indicated that these two suspected cases aged 26 years and 51 years have neither attended any funerals nor been exposed to any dead carcasses of bush animals to enable possible exposure to any infectious agents of haemorrhagic fevers or any other related causative agents. These two individuals were not related nor connected in any way by family, place of residence and even district of residence. The index case is a resident of Kusa in the Adansi North District with a history of travel from Bogoso in the western region, while the second case resides in Bogyawe/Ankaase which is in Bekwai Municipal. The only connection they have is that of occupation: they are both farmers, but they practice their trade in different locations thus Kusa in the Adansi North District and Bogyawe/Ankaase in the Bekwai Municipal.
The case was a farmer who had travelled from Bogoso in the Western Region to Kusa, Fomena, got sick and was hospitalized. He died shortly and was sent to a mortuary at Adiembra, a community in the neighboring Adansi Asokwa District to the reported district. The remains were taken to Savanna region where he was buried.
5. Conclusion
This report presents evidence on the current Marburg viral disease outbreak in the Ashanti region of Ghana, response activities conducted, surveillance and contact tracing activities, environmental risk assessment, stakeholders’ engagement, case management and public health actions undertaken to control the outbreak and restore health to the affected regions. The intensified outbreak response activities and contact tracing activities conducted by the epidemiologists and disease surveillance from the Ashanti Regional Health Directorate Rapid Response Team with support from National Surveillance Department and partner World Health Organization, a total of one hundred and ninety-eight (198) contacts were traced among them were thirty (30) health care workers and one twenty-eight (168) closed family members. Daily monitoring of temperature and general health and wellbeing were undertaken by healthcare staff in the affected districts. Samples from 16 contacts including health care workers were randomly tested and all were negative.
Two of the initial 118 contacts that were identified and followed up later tested positive making a total of three (3) confirmed cases in Ghana. Hence, case 2 thus was a one-year two-month-old contact of Case 1 (son of Case 1) who got ill and was admitted on 17 July 2022. He died on the third day of admission. The last case (case 3) was a 24-year-old female (mother of Case 2 and wife of Case 1). She was managed in a government-designated isolation center, with full implementation of strict infection prevention and control measures. Two deaths occurred in this outbreak resulting in a fatality of 67.0%. The Marburg virus responsible for this outbreak is related to the sequence in 2021 outbreak and group of sequences obtained from bats in Sierra Leone and an outbreak that occurred in Angola in 2004-2005
.
The Ashanti Region Health Directorate together with its National Surveillance Department and partners demonstrated capacity to respond to public health emergencies. Our resilient health system was responsible for the early detection of and prompt response to outbreaks including the current Marburg viral disease. On 16 September 2022, the Ministry of Health (MoH) of Ghana declared the end of the Marburg Virus Disease (MVD) outbreak that affected the country’s Ashanti, Savannah, and Western regions. In accordance with WHO recommendations the declaration was made 42 days (twice the maximum incubation period for Marburg infection) after the second negative test of the last confirmed case on 5 August 2022
.
The environmental risk of exposure of this outbreak could not be ascertained; therefore community surveillance was strengthened with the training of more community surveillance officers to continue case search and health education to unearth any sign and symptoms for prompt and effective response activities.
Abbreviations
CBSVs | Community Based Surveillance and Volunteers |
DDHS | District Director of Health Service |
GIT | Gastrointestinal Tract |
GHS/MOH | Ghana Health Service/Ministry of Health |
IV | Intravenous |
LI | Legislative Instrument |
MVD | Marburg Virus Disease |
NMIMR | Noguchi Memorial Institute for Medical Research |
PHC | Population and Housing Census |
PPE | Personal Protective Equipment |
Q-RT-PCR | Quantitative Reverse Transcription Polymerase Chain Reaction |
WHO | World Health Organization |
Conflicts of Interest
The authors declare that have no competing interests.
References
| [1] |
Aborode, A. T., Wireko, A. A., Bel-Nono, K. N., Quarshie, L. S., Allison, M., & Bello, M. A. (2022). Marburg virus amidst COVID-19 pandemic in Guinea: Fighting within the looming cases. In International Journal of Health Planning and Management (Vol. 37, Issue 1).
https://doi.org/10.1002/hpm.3332
|
| [2] |
Ajelli, M., & Merler, S. (2012). Transmission Potential and Design of Adequate Control Measures for Marburg Hemorrhagic Fever. PLoS ONE, 7(12).
https://doi.org/10.1371/journal.pone.0050948
|
| [3] |
Amman, B. R., Carroll, S. A., Reed, Z. D., Sealy, T. K., Balinandi, S., Swanepoel, R., Kemp, A., Erickson, B. R., Comer, J. A., Campbell, S., Cannon, D. L., Khristova, M. L., Atimnedi, P., Paddock, C. D., Kent Crockett, R. J., Flietstra, T. D., Warfield, K. L., Unfer, R., Katongole-Mbidde, E., … Towner, J. S. (2012). Seasonal Pulses of Marburg Virus Circulation in Juvenile Rousettus aegyptiacus Bats Coincide with Periods of Increased Risk of Human Infection. PLoS Pathogens, 8(10).
https://doi.org/10.1371/journal.ppat.1002877
|
| [4] |
Balibouse, D. (Reuters/Aljazeera). (n.d.). Child infected with Marburg virus dies in Ghana World Health Organization News Al Jazeera.
|
| [5] |
Bausch, D. G., Borchert, M., Grein, T., Roth, C., Swanepoel, R., Libande, M. L., Talarmin, A., Bertherat, E., Muyembe-Tamfum, J. J., Tugume, B., Colebunders, R., Kondé, K. M., Pirard, P., Olinda, L. L., Rodier, G. R., Campbell, P., Tomori, O., Ksiazek, T. G., & Rollin, P. E. (2003). Risk Factors for Marburg Hemorrhagic Fever, Democratic Republic of the Congo. In Emerging Infectious Diseases (Vol. 9, Issue 12).
https://doi.org/10.3201/eid0912.030355
|
| [6] |
CDC. (1967). factsheet-Marburg Hemorrhagic Fever.
https://www.cdc.gov/vhf/marburg/pdf/factsheet.pdf
|
| [7] |
Kika, T. (n.d.). First Infant Dies From Marburg Outbreak, Virus Related to Ebola.
|
| [8] |
Kortepeter, M. G., Dierberg, K., Shenoy, E. S., & Cieslak, T. J. (2020). Marburg virus disease: A summary for clinicians. International Journal of Infectious Diseases, 99.
https://doi.org/10.1016/j.ijid.2020.07.042
|
| [9] |
Martini, G. A. (1969). Marburg agent disease: In man. Transactions of the Royal Society of Tropical Medicine and Hygiene, 63(3), 295–302.
https://doi.org/10.1016/0035-9203(69)90001-7
|
| [10] |
Nyakarahuka, L., Shoemaker, T. R., Balinandi, S., Chemos, G., Kwesiga, B., Mulei, S., Kyondo, J., Tumusiime, A., Kofman, A., Masiira, B., Whitmer, S., Brown, S., Cannon, D., Chiang, C. F., Graziano, J., Morales-Betoulle, M., Patel, K., Zufan, S., Komakech, I., … Lutwama, J. J. (2018). Marburg virus disease outbreak in Kween District Uganda, 2017: Epidemiological and laboratory findings. PLoS Neglected Tropical Diseases, 13(3).
https://doi.org/10.1371/journal.pntd.0007257
|
| [11] |
Trappler, B., Clausen, L., Meyers, A. M., Kew, M. C., Bothwell, T. H., Sher, R., Miller, G. B., Schneider, J., & Gear, J. H. S. (1975). Outbreak of Marburg virus disease in Johannesburg. British Medical Journal, 4(5995), 489–493.
https://doi.org/10.1136/bmj.4.5995.489
|
| [12] |
WHO. (1977). Marburg virus disease. In Update (Vol. 14, Issue 2, pp. 125–138).
https://doi.org/10.47583/ijpsrr.2022.v72i02.010
|
| [13] |
WHO. (2022). Marburg virus disease - Ghana.
https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON402
|
Cite This Article
-
APA Style
Asiamah, D. Y., Boakye, S., Owusu, P., Sackey, P. A., Adu, D. A., et al. (2026). Marburg Viral Disease Outbreak in the Adansi North of Ashanti Region, Ghana: A Case Report. International Journal of Infectious Diseases and Therapy, 11(2), 30-37. https://doi.org/10.11648/j.ijidt.20261102.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Asiamah, D. Y.; Boakye, S.; Owusu, P.; Sackey, P. A.; Adu, D. A., et al. Marburg Viral Disease Outbreak in the Adansi North of Ashanti Region, Ghana: A Case Report. Int. J. Infect. Dis. Ther. 2026, 11(2), 30-37. doi: 10.11648/j.ijidt.20261102.13
Copy
|
Download
AMA Style
Asiamah DY, Boakye S, Owusu P, Sackey PA, Adu DA, et al. Marburg Viral Disease Outbreak in the Adansi North of Ashanti Region, Ghana: A Case Report. Int J Infect Dis Ther. 2026;11(2):30-37. doi: 10.11648/j.ijidt.20261102.13
Copy
|
Download
-
@article{10.11648/j.ijidt.20261102.13,
author = {Daniel Yeboah Asiamah and Solomon Boakye and Patrick Owusu and Portia Anna Sackey and Daniel Amankwaa Adu and Georgina Frimpong Siraa},
title = {Marburg Viral Disease Outbreak in the Adansi North of Ashanti Region, Ghana: A Case Report},
journal = {International Journal of Infectious Diseases and Therapy},
volume = {11},
number = {2},
pages = {30-37},
doi = {10.11648/j.ijidt.20261102.13},
url = {https://doi.org/10.11648/j.ijidt.20261102.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijidt.20261102.13},
abstract = {On July 7, 2022, a blood sample from a resident of Adansi North District, Ashanti region of Ghana, tested positive for Marburg virus disease. Within 24 hours of confirmation, a rapid outbreak response was initiated. This report presents results of response activities conducted to adequately response to the outbreak. A regional rapid response team was activated consisting of specialized teams to conduct case finding, case management and isolation, contact listing and follow up, sample collection and testing, and community engagement. Support from the National Surveillance Department and WHO were provided. An investigation was also carried out to identify the potential source of infection. Laboratory virus isolation and sequencing were performed by the NMIMR and corroborated by the Institute Pasteur in Dakar to identify the strain of Marburg virus. One hundred and ninety-eight closed contacts were epidemiologically investigated, with blood samples of sixteen (16) randomly selected tested for MVD. Standard case definition of MVD was used to screen all. No case was suspected based on the case definition used. Two closed contacts were confirmed as MVD after the follow- up. Of the three confirmed MVD cases, two died, yielding a case fatality rate of 67.0%. All three cases form a single nuclear family and 50% (2/3) of the MVD cases were male. The cases had clinical symptoms of fever, chills, general malaise, and bleeding from the nose and mouth. Genetic sequencing results indicated that the Marburg virus genomes were related to the sequence from the 2021 outbreak and overall, group with sequences obtained from bats in Sierra Leone and an outbreak that occurred in Angola in 2004-2005. This outbreak of MVD occurred as a family cluster with no additional transmission outside of the three related cases. Rapid case detection, prompt laboratory testing at the NMIMR and presence of pre-trained, well-prepared national and district rapid response teams facilitated the containment and control of this outbreak.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Marburg Viral Disease Outbreak in the Adansi North of Ashanti Region, Ghana: A Case Report
AU - Daniel Yeboah Asiamah
AU - Solomon Boakye
AU - Patrick Owusu
AU - Portia Anna Sackey
AU - Daniel Amankwaa Adu
AU - Georgina Frimpong Siraa
Y1 - 2026/06/30
PY - 2026
N1 - https://doi.org/10.11648/j.ijidt.20261102.13
DO - 10.11648/j.ijidt.20261102.13
T2 - International Journal of Infectious Diseases and Therapy
JF - International Journal of Infectious Diseases and Therapy
JO - International Journal of Infectious Diseases and Therapy
SP - 30
EP - 37
PB - Science Publishing Group
SN - 2578-966X
UR - https://doi.org/10.11648/j.ijidt.20261102.13
AB - On July 7, 2022, a blood sample from a resident of Adansi North District, Ashanti region of Ghana, tested positive for Marburg virus disease. Within 24 hours of confirmation, a rapid outbreak response was initiated. This report presents results of response activities conducted to adequately response to the outbreak. A regional rapid response team was activated consisting of specialized teams to conduct case finding, case management and isolation, contact listing and follow up, sample collection and testing, and community engagement. Support from the National Surveillance Department and WHO were provided. An investigation was also carried out to identify the potential source of infection. Laboratory virus isolation and sequencing were performed by the NMIMR and corroborated by the Institute Pasteur in Dakar to identify the strain of Marburg virus. One hundred and ninety-eight closed contacts were epidemiologically investigated, with blood samples of sixteen (16) randomly selected tested for MVD. Standard case definition of MVD was used to screen all. No case was suspected based on the case definition used. Two closed contacts were confirmed as MVD after the follow- up. Of the three confirmed MVD cases, two died, yielding a case fatality rate of 67.0%. All three cases form a single nuclear family and 50% (2/3) of the MVD cases were male. The cases had clinical symptoms of fever, chills, general malaise, and bleeding from the nose and mouth. Genetic sequencing results indicated that the Marburg virus genomes were related to the sequence from the 2021 outbreak and overall, group with sequences obtained from bats in Sierra Leone and an outbreak that occurred in Angola in 2004-2005. This outbreak of MVD occurred as a family cluster with no additional transmission outside of the three related cases. Rapid case detection, prompt laboratory testing at the NMIMR and presence of pre-trained, well-prepared national and district rapid response teams facilitated the containment and control of this outbreak.
VL - 11
IS - 2
ER -
Copy
|
Download