Introduction: The management of posterior urethral valves is challenging in the absence of early diagnosis and optimal technical facilities. Once performed, endoscopic resection of the valves does not guarantee complete healing. The aim of our study was to investigate the outcome of patients treated for posterior urethral valves by endoscopic resection in two hospitals in the city of Yaounde. Materials and methods: This was a 5 years retrospective cross-sectional study conducted in two hospitals in the city of Yaounde from 2019 to 2024. All patients included had been treated for posterior urethral valves by endoscopic resection. Socio-demographic, diagnostic, therapeutic and prognostic variables were investigated. Results: A total of 35 patients were treated over the five-year period, with an admission rate of 6 cases per year. The median age at presentation was 02 years, and 29 participants (82.8%) presented late. Dysuria and recurrent urinary tract infections were the main reasons for consultation. Endoscopic valve ablation relieved obstruction in all participants except 5 (14.3%) who had residual valves. Creatinine levels and glomerular filtration rate before and after resection were measured in 15 participants; among them, 9 (47.5%) had renal insufficiency with a GFR < 60 ml/min/1.73 m2, which did not improve after valve resection. Uroflowmetry showed abnormalities in three patients with a Qmax < 15 ml/s. The mortality rate was 2.9%. Conclusion: Endoscopic resection of posterior urethral valves significantly improves micturition. Follow-up is necessary to prevent complications.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Posterior urethral valves (PUVs) are a congenital obstruction of the posterior urethra
[1]
Hodges SJ, Patel B, McLorie G, Atala A. Posterior Urethral Valves. Sci World J. 2009; 9: 1119‑26.
[1]
. This disorder was first described by Morgagni in 1717 and then by Langenbeck in 1802 and occurs mainly in males
[2]
Krishnan A, De Souza A, Konijeti R, Baskin LS. The Anatomy and Embryology of Posterior Urethral Valves. J Urol. April 2006; 175(4): 1214‑20.
[2]
. They manifest early in gestation, exposing the bladder and upper urinary tract to high pressure, leading to significant alterations in bladder function and kidney damage
[1]
Hodges SJ, Patel B, McLorie G, Atala A. Posterior Urethral Valves. Sci World J. 2009; 9: 1119‑26.
[1]
.
Despite the rarity of posterior urethral valves, they are the most common cause of urological obstruction in male foetuses, with an estimated incidence of 1 infant in every 5,000 to 8,000 live births worldwide
[3]
Avni F, Coulon C, Lérisson H, Priso RH, Manucci-Lahoche A. Avni F, Coulon C, Lérisson H, Priso RH, Manucci-Lahoche A Imaging and valves of the posterior urethra: From fetus to child, or "what happens to them?" Perinatology. June 2020; 12(2): 70‑9.
[4]
Malin G, Tonks A, Morris R, Gardosi J, Kilby M. Congenital lower urinary tract obstruction: a population‐based epidemiological study. BJOG Int J Obstet Gynaecol. nov 2012; 119(12): 1455‑64.
[3, 4]
. Between 1950 and 1969, 38% of children with PUV died between the third hour and the eighth year of life, with an average of 10 months
[4]
Malin G, Tonks A, Morris R, Gardosi J, Kilby M. Congenital lower urinary tract obstruction: a population‐based epidemiological study. BJOG Int J Obstet Gynaecol. nov 2012; 119(12): 1455‑64.
[4]
. The mortality rate for newborns with severe neonatal distress syndrome with septicaemia and renal failure was previously around 50%. According to a 30-year study conducted in Canada by Jeff Warren et al. in 2004, he found that 11% of cases progressed to end-stage renal failure with a mortality rate of 6.6%
[5]
Warren J, Pike J, Leonard M. Warren J, Pike J, Leonard M. Posterior urethral valves in eastern Ontario over 30 years. Can J Urol. 2004 ; 11(2): 2210-5.
[5]
. In Cameroon, in 2018, Tambo et al. reported a low complication rate after endoscopic resection of valves with urethral stenosis in 11.2% of cases. Mortality in the same study was 5.6%, while in Nigeria, Uba et al. reported 4.9% deaths
Tambo FFM, Tolefac PN, Ngowe MN, Minkande JZ, Mbouche L, Guemkam G, et al. Posterior urethral valves: 10 years audit of epidemiologic, diagnostic and therapeutic aspects in Yaounde gynaeco-obstetric and paediatric hospital. BMC Urol. dec 2018; 18(1): 46.
[6, 7]
.
The management of neonatal surgical conditions is problematic in developing countries due to the rarity of antenatal diagnosis, resulting in high intraoperative morbidity and mortality
[8]
Uba AF, Chirdan LB, Ihezue CH, Ramyil VL, Dakum NK. Posterior urethral valves in children: presentation and outcome of initial treatment in Ile-Ife, Nigeria. African Journal Urology. 2007; 13 : 124-131. Moussa ZS, Cherlyn B, Massara KS, Astrid ON, Bénilde T, Madina NA, et al.
[8]
. These diagnostic shortcomings have led to many children with fever being treated incorrectly for malaria or recurrent urinary tract infections before being transferred to the appropriate department
[8]
Uba AF, Chirdan LB, Ihezue CH, Ramyil VL, Dakum NK. Posterior urethral valves in children: presentation and outcome of initial treatment in Ile-Ife, Nigeria. African Journal Urology. 2007; 13 : 124-131. Moussa ZS, Cherlyn B, Massara KS, Astrid ON, Bénilde T, Madina NA, et al.
[8]
. The miniaturisation of endoscopes in paediatric settings has minimised urethral trauma, operating time and bladder irrigation, and has also significantly reduced the rate of post-operative infectious complications
[1]
Hodges SJ, Patel B, McLorie G, Atala A. Posterior Urethral Valves. Sci World J. 2009; 9: 1119‑26.
[9]
Contribution of retrograde urethro-cystography in the diagnostic assessment of posterior urethral valves at the Charles De Gaulle University Pediatric Hospital. J Afr Imag Med 202; 13(2): 80-84.
[1, 9]
. However, relief of the obstruction may not guarantee a good renal and urinary prognosis due to the long-term consequences of the obstruction that may be felt after removal
[3]
Avni F, Coulon C, Lérisson H, Priso RH, Manucci-Lahoche A. Avni F, Coulon C, Lérisson H, Priso RH, Manucci-Lahoche A Imaging and valves of the posterior urethra: From fetus to child, or "what happens to them?" Perinatology. June 2020; 12(2): 70‑9.
[3]
. In Cameroon, in specialist hospitals where valve ablation is performed, most patients do not attend follow-up visits due to a mistaken belief that they will be completely cured once the obstruction has been removed
. The aim of this study was to investigate the outcome of patients treated for PUVS by endoscopic resection in two hospitals in the city of Yaounde.
2. Materials and Methods
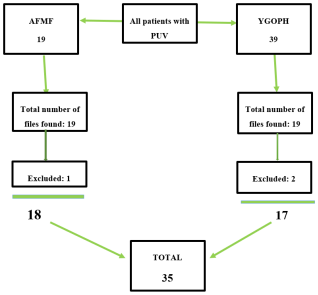
This was a retrospective cross-sectional study conducted in two specialist hospitals in the city of Yaounde: The Yaounde Gynaeco-Obstetrics and Paediatrics Hospital (YGOPH) and the Andre Fouda Medical Foundation (AFMF). Both hospitals have the necessary equipment for the medical and surgical management of posterior urethral valves. The study covered a period of five years from 1st January 2019 to 3rd January 2024. All patients who underwent endoscopic resection of PUVs were included. The study was approved by the Institutional Ethics and Research Committee (Ref 619/CIERSH/DM/2024). Socio-demographic variables included age, place of residence and method of recruitment. Clinical and paraclinical characteristics included the reason for consultation, length of hospitalisation, uroflowmetry, quality of urinary stream, glomerular filtration rate using the Schwartz formula, creatinine, urea, serum electrolytes, and imaging. The therapeutic and prognostic variables investigated were surgical history, date of endoscopic resection, short-, medium term outcomes, post-operative complications, and urine flow measurement after resection. The data collected were entered using CS Pro (Census and Survey Processing) software version 7.5 and analysed using SPSS 20 (Statistical Package for Social Sciences). Quantitative variables were expressed as mean ± standard deviation or median and interquartile range after verification of distribution by normality tests.
3. Results
We recruited a total of 35 cases that met the inclusion criteria and were treated over the five-year period (Figure 1).
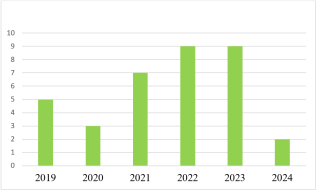
Figure 2. Distribution of posterior urethral valves over time.
The median age of patients on admission was 2 [0.33–4] years, with extremes of 1 day and 17 years. Among them, 6 had an antenatal diagnosis (17.1%); 29 (82.8%) presented after the age of 1 month and 24 after the age of 1 year (67.9%). The majority were less than 1 year old at admission (31.4%). (Table 1)
Table 1. Population distribution by age group.
Variables
Frequency (n)
Percentage (%)
Age range (years)
< 1 month
11
31.4
1-2
9
25.7
3-5
7
20.0
6-9
1
2.9
≥ 10
7
20.0
In our study population, only 06 (17.1%) received an antenatal diagnosis, compared to 29 (82.9%) who received a postnatal diagnosis. All patients presented with dysuria upon admission, and 42.9% had a history of recurrent urinary tract infections (Table 2).
Table 2. Distribution of the population according to the reason for consultation.
Variables
Frequency (n)
Percentage (%)
Reasons for consultation
Dysuria
35
100
Recurrent urinary tract infections
15
42.9
Abnormal urinary stream
13
37.1
Painful urination
13
37.1
Lower abdominal swelling
12
34.3
Incomplete urination
8
22.9
Favourable obstetric ultrasound scan
6
17.1
Fever
6
17.1
Anuria
5
14.3
Urinary incontinence
3
8.6
Oliguria
3
8.6
Haematuria
1
2.9
Oedema of the lower limbs
1
2.9
Ascites
1
2.9
Voiding urethrocystography was the investigation of choice for all participants treated in the postnatal period. Bilateral hydronephrosis was present in 13 patients (37.1%) and unilateral hydronephrosis in 3 participants (8.6%). Vesicoureteral reflux (VUR) was present in 8 (22.9%) others, 6 (17.1%) patients had chronic kidney disease, and 2 patients had growth retardation (2.9%). Vesicostomy was performed in 25.7% (n=9) of cases as the first surgical procedure. The median length of hospitalisation was 4 [2-6] days, with extremes ranging from 2 to 16 days. The median duration of transurethral catheterisation was 4 days, with extremes ranging from 1 to 20 days.
At the end of the first month after valve resection, we observed a significant improvement in urinary function in 88.6% of cases, marked in 97.1% of cases by normal urinary flow, complete bladder emptying in 88.6% of cases, and normal urine stream strength (8.6%). Complications were present in 45.7% of cases, predominantly urinary tract infections in 31.4% of cases.
Valve recurrence during the first month of follow-up was observed in 5 patients, or 14.3% of cases. Six months after valve resection, urine flow was normal in 94.3% of cases, with complete bladder emptying in 85.7% of cases and normal urine stream force in 85.7% of cases. Complications were common in 14.3% of cases, predominantly renal failure in 14.3% of cases. (Table 3).
Prior to surgical treatment, baseline creatinine levels were known in 27 participants (77.1%), ranging from 25.6 μmol/l to 136.1 μmol/l, with a mean of 64.5 μmol/l ± 31.2 μmol/l. Glomerular filtration rate (GFR) could be determined in 19 participants (54.30%). This showed an average GFR of 65.60 ± 27.06 ml/min/1.73 m² with a range of 27.06 to 106.80 ml/min/1.73 m², and most participants had a GFR between 30 and 89 ml/min/1.73 m2. An average GFR of 65.60 ± 27.06 ml/min/1.73 m2 with a range of 11 to 132 ml/min/1.73 m2, and most participants had a GFR between ≥ 90 ml/min/1.73 m2.
Table 3. Patient characteristics at 6 months post-operation.
Variables
Frequency (n)
Percentage (%)
Urinary flow
Normal
33
94,3
Abnormal
1
2,9
Undetermined
1
2,9
Bladder emptying
Complete
30
85,7
Incomplete
4
11,4
Undetermined
1
2,9
Urine Stream strength
Strong
31
88,6
Weak
3
8,6
Undetermined
1
2,9
Complications
No complications
29
82,9
Incontinence
4
11,4
Chronic renal failure
1
2,9
Residual valves
1
2,9
Stenosis
1
2,9
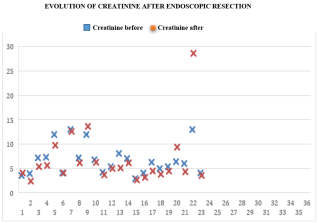
In the post-operative phase, creatinine levels were known for 23 participants (65.7%), ranging from 21.22 μmol/l to 253 μmol/l, with an average of 59.3 μmol/l ± 49.6 μmol/l. Figure 3 shows the trend in serum creatinine levels before and after resection.
Figure 3. Changes in creatinine levels after Endoscopic valve resection.
Postoperative GFR assessment was done in 15 patients. After resection, a significant improvement was noted in 4 patients (26.6%). Seven participants had a GFR ≥ 90 ml/min/1.73 m2 (58.3%) and two participants had a GFR between 60-89 ml/min/1.73 m2. A regression was noted in 2 participants (16.6%), one of whom had an GFR < 15 ml/min/1.73 m2 (6.6%) and the other a GFR between 15-29 ml/min/1.73 m2, and unchanged GFR in 2 participants, both of whom had a GFR between 30-59 ml/min/1.73 m2 (16.6%).
Urine flow measurement was performed in 05 patients (14.3%), two of whom complained of incontinence and the others had no complaints at the time of the examination. It showed abnormalities in three patients with a Qmax < 15 ml/s.
We recorded 1 (2.9%) death.
4. Discussion
We recorded 35 cases over the entire study period, with an annual incidence of 06 cases per years, which is comparable to that of previous studies conducted in Cameroon by Tambo et al.
, in which it varies between 2 and 4 cases per year. Similarly, studies conducted in Nigeria by Jaja et al.
[12]
A Chiabi, F Angwafo, MT Obama, V Takou,, J Kanyi Zoung,. Posterior urethral valves in children: A review of 28 cases in Yaounde, Cameroon. 1996; Clin Mother and Child Health Vol. 1(2) 2004: 89-96.
[12]
and Ajao et al.
[13]
Jaja T, Anochie IC, Eke FU. Posterior urethral valve in childhood in Port Harcourt, Nigeria. Port Harcourt Med J. 2012; 6(1): 10-6.
[13]
found 7 and 8 cases, respectively. The low prevalence in our environment may be linked to early perinatal and neonatal deaths as a result of severe obstruction, superimposed infection, acute renal failure and pulmonary hypoplasia, which never reach hospital and have therefore never been diagnosed
[7]
Tambo FFM, Tolefac PN, Ngowe MN, Minkande JZ, Mbouche L, Guemkam G, et al. Posterior urethral valves: 10 years audit of epidemiologic, diagnostic and therapeutic aspects in Yaounde gynaeco-obstetric and paediatric hospital. BMC Urol. dec 2018; 18(1): 46.
[14]
Ajao EA, Abiola OO, Alao AM, Adeniran JO Posterior urethral valve: a retrospective review of cases and challenges of management in a low-resource center. Res. J. of Health Sci. 2018 ; 6(3): 113-120.
[7, 14]
.
In total, 82.8% presented after the age of 1 month, compared to 17.1% before 1 month with antenatal diagnosis. This suggests that the vast majority of patients in our population presented late. This is similar to studies previously conducted in Cameroon in 2018 by Tambo et al.
Tolefac PN, Tamambang RF, Yeika E, Mbwagbaw LT, Egbe TO. Ten years analysis of stillbirths in a tertiary hospital in sub-Saharan Africa: a case-control study. Notes de BMC Res. 2017; 10(1): 447.
[15]
, where 72.2% and 73.3% of the study population presented late, respectively. Among the factors that may have contributed to this late presentation are the lack of awareness or poor understanding of this malformation
[16]
Sanjay K, Ramanandan P, Shirish SPosterior urethral valves; Analysis of results after endoscopic valve ablation. AJHS. 2022: 2: 435-439.
[16]
, as well as the high cost of radiological examinations and the absence of a universal health insurance system
[16]
Sanjay K, Ramanandan P, Shirish SPosterior urethral valves; Analysis of results after endoscopic valve ablation. AJHS. 2022: 2: 435-439.
[16]
.
The clinical manifestations were dominated by dysuria and recurrent urinary tract infections. This result is similar to those of Trellu et al.
[17]
Odetunde OI, Odetunde OA, Ademuyiwa AO, Okafor HU, Ekwochi U, Azubuike JC et al. Outcome of late presentation of posterior urethral valves in a resource-limited economy: management challenges. Int J Nephrol. 2012 ; 2012 : E345298.
[17]
in France and Gargah et al.
[18]
Trellu M, Adra AL, Mouba JF, Lopez C, Averous M, Gali_fer RB, Dalla-Vale F, Ichay L, Morin D. Posterior Urethra Valves. Current status in Languedoc-Roussillon from 1998 to 2007: antenatal, neonatal data, medium-term outcomes. Archives of Pediatrics 2009; 16(5): 417-425.
[18]
in Tunisia, who reported clinical symptoms dominated by urinary signs and, above all, recurrent urinary tract infections in 43 and 44 cases, respectively. Indeed, the urethral obstruction prevents proper urine drainage and promotes reflux, resulting in urinary disorders and urinary tract infections as the main warning signs.
On admission, voiding cystourethrography was performed on all patients. We found vesico-ureteral reflux (VUR) in 22.9% of cases. These results are consistent with those of Schober et al.
[19]
Gargah T, Gharbi Y, Ben Moussa M, Kaabar N, Lakhoua M. Posterior urethral valves: a report of 44 cases. Tun Med 2010 ; 88(8): 557-562. 2010.
[19]
in the United Kingdom, where VUR was found in 16% of cases, but are inconsistent with those found in Cameroon
, but this could be explained by the lesser severity of the VUR. Vesicostomy as a temporary treatment was performed in 09 patients (25.7%). Although for some it should only be reserved for newborns whose weight or resuscitation conditions do not allow endoscopic surgery, for others it is a safety valve for the upper urinary tract
Khemakhem R, Ben Ahmed Y, Mefteh S, Jlidi S, Charieg A, Louati H, et al. Posterior urethral valves: a report of 38 cases. J Pediatrics and Childcare. oct 2012; 25(5): 242‑8.
[22]
Tachdjian G, Brisset S, Courtout A-M et al. Human embryology and histology. Elsevier Masson. 2016.
After resection, we observed 31.4% urinary tract infections, 11.4% incontinence, persistent VUR in 5.7%, stenosis in 2.9%, and progression to end-stage renal failure in 2.9% of cases. This is similar to the studies by Sanjay et al.
[15]
Tolefac PN, Tamambang RF, Yeika E, Mbwagbaw LT, Egbe TO. Ten years analysis of stillbirths in a tertiary hospital in sub-Saharan Africa: a case-control study. Notes de BMC Res. 2017; 10(1): 447.
, which reported that the main post-resection complications were urinary tract infection, stenosis, and persistent VUR.
The results revealed impaired renal function prior to endoscopic resection, with a glomerular filtration rate < 60 ml/min/1.73 m2 in 47.4% of cases (09 patients). These results are comparable to those of Talabi et al.
[24]
Sagna A, Ndoye M, Mbaye Pa, Ngoy M, Ngom G. Postnatal endoscopic resection of the posterior urethral valves in boys: a preliminary study of 23 cases. Urology Andrology, 2018: 1(9): 409-414.
, who reported 40.5% in 2015 and 55.6% in 2018, respectively. The assessment after resection revealed an eGFR < 60 ml/min/1.73 m2, which is consistent with the current literature on the fact that high serum creatinine levels are associated with a poor prognosis in patients with PUV, and this may not be reversed even with the removal of the obstruction
Talabi AO, Sowande OA, Etonyeaku AC, Salako AA, Adejuyigbe O Posterior urethral valves in children: presentation and outcome of initial treatment at Ile-Ife, Nigeria. Niger J Surg Off Publ Niger Surg Res Soc. 2015 ; 21(2): 151-6. 2015.
[26]
Heikkilä J, Holmberg C, Kyllönen L, Rintala R, Taskinen S. Long-Term Risk of End Stage Renal Disease in Patients With Posterior Urethral Valves. J Urol. dec 2011; 186(6): 2392‑6.
[27]
Denes ED, Barthold JS et Gonzalez R : Early prognostic value of serum creatinine levels in children with posterior urethral valves. J Urol, 1997 ; 157 : 1441.
[6, 25-27]
.
Post-resection urinary flow rate measurement was performed in only five patients, undoubtedly due to parents' reluctance to continue hospital visits when urine flow was satisfactory after the obstruction had been relieved, but also due to a lack of financial resources. Among these patients, two had continence problems and three had no complaints. Uroflowmetry showed abnormalities in three patients with a Qmax < 15 ml/s, one of whom had reported no complaints and was satisfied with the resection. Even after surgical treatment, the consequences of obstruction related to the antenatal presence of VUPs can continue in the long term, including into adulthood
[22]
Tachdjian G, Brisset S, Courtout A-M et al. Human embryology and histology. Elsevier Masson. 2016.
[22]
.
With regard to deaths, 1 (2.9%) case was recorded. This is comparable to the 4.9% reported in Nigeria by Uba et al in 2007
[7]
Tambo FFM, Tolefac PN, Ngowe MN, Minkande JZ, Mbouche L, Guemkam G, et al. Posterior urethral valves: 10 years audit of epidemiologic, diagnostic and therapeutic aspects in Yaounde gynaeco-obstetric and paediatric hospital. BMC Urol. dec 2018; 18(1): 46.
[7]
and the 5.6% reported in Cameroon in 2018 by Tambo et al
. The modernisation of endoscopy tools and the strengthening of the local team in Cameroon could explain the relatively low mortality rate in our series.
Half of the patients were lost to follow-up from the third month post-operatively. This could be due to parents' reluctance to continue hospital visits in the presence of satisfactory urine flow after relief of the obstruction, combined with the long distances required to travel to the hospital, but also to a lack of financial resources. It is therefore necessary to educate parents and guardians about the importance of long-term follow-up and the risks of continued renal and bladder deterioration even after improvement in urination.
Limitations of the study
Although our study described significant clinical and biological results following PUV ablation in the city of Yaounde, its applicability may be limited by:
1) A significant number of participants not residing in the city of Yaounde;
2) Incomplete and missing information on many parameters;
3) Reluctance of some patients to participate in the study, possibly due to their ignorance of the long-term consequences of this malformation, even with satisfactory urinary flow and output after removal of the obstruction.
5. Conclusion
In Yaounde, endoscopic resection of the posterior urethral valves improves urination in the majority of children. Short- and medium-term follow-up reveals persistent renal function impairment, but with low mortality.
Abbreviations
PUV
Posterior Urethral Valve
GFR
Glomerular Filtration Rate
VUR
Vesico-ureteral Reflux
Qmax
Maximum Flow Rate
YGOPH
Yaounde Gynaeco-Obstetrics and Paediatrics Hospital
Hodges SJ, Patel B, McLorie G, Atala A. Posterior Urethral Valves. Sci World J. 2009; 9: 1119‑26.
[2]
Krishnan A, De Souza A, Konijeti R, Baskin LS. The Anatomy and Embryology of Posterior Urethral Valves. J Urol. April 2006; 175(4): 1214‑20.
[3]
Avni F, Coulon C, Lérisson H, Priso RH, Manucci-Lahoche A. Avni F, Coulon C, Lérisson H, Priso RH, Manucci-Lahoche A Imaging and valves of the posterior urethra: From fetus to child, or "what happens to them?" Perinatology. June 2020; 12(2): 70‑9.
[4]
Malin G, Tonks A, Morris R, Gardosi J, Kilby M. Congenital lower urinary tract obstruction: a population‐based epidemiological study. BJOG Int J Obstet Gynaecol. nov 2012; 119(12): 1455‑64.
[5]
Warren J, Pike J, Leonard M. Warren J, Pike J, Leonard M. Posterior urethral valves in eastern Ontario over 30 years. Can J Urol. 2004 ; 11(2): 2210-5.
Tambo FFM, Tolefac PN, Ngowe MN, Minkande JZ, Mbouche L, Guemkam G, et al. Posterior urethral valves: 10 years audit of epidemiologic, diagnostic and therapeutic aspects in Yaounde gynaeco-obstetric and paediatric hospital. BMC Urol. dec 2018; 18(1): 46.
[8]
Uba AF, Chirdan LB, Ihezue CH, Ramyil VL, Dakum NK. Posterior urethral valves in children: presentation and outcome of initial treatment in Ile-Ife, Nigeria. African Journal Urology. 2007; 13 : 124-131. Moussa ZS, Cherlyn B, Massara KS, Astrid ON, Bénilde T, Madina NA, et al.
[9]
Contribution of retrograde urethro-cystography in the diagnostic assessment of posterior urethral valves at the Charles De Gaulle University Pediatric Hospital. J Afr Imag Med 202; 13(2): 80-84.
A Chiabi, F Angwafo, MT Obama, V Takou,, J Kanyi Zoung,. Posterior urethral valves in children: A review of 28 cases in Yaounde, Cameroon. 1996; Clin Mother and Child Health Vol. 1(2) 2004: 89-96.
[13]
Jaja T, Anochie IC, Eke FU. Posterior urethral valve in childhood in Port Harcourt, Nigeria. Port Harcourt Med J. 2012; 6(1): 10-6.
[14]
Ajao EA, Abiola OO, Alao AM, Adeniran JO Posterior urethral valve: a retrospective review of cases and challenges of management in a low-resource center. Res. J. of Health Sci. 2018 ; 6(3): 113-120.
[15]
Tolefac PN, Tamambang RF, Yeika E, Mbwagbaw LT, Egbe TO. Ten years analysis of stillbirths in a tertiary hospital in sub-Saharan Africa: a case-control study. Notes de BMC Res. 2017; 10(1): 447.
[16]
Sanjay K, Ramanandan P, Shirish SPosterior urethral valves; Analysis of results after endoscopic valve ablation. AJHS. 2022: 2: 435-439.
[17]
Odetunde OI, Odetunde OA, Ademuyiwa AO, Okafor HU, Ekwochi U, Azubuike JC et al. Outcome of late presentation of posterior urethral valves in a resource-limited economy: management challenges. Int J Nephrol. 2012 ; 2012 : E345298.
[18]
Trellu M, Adra AL, Mouba JF, Lopez C, Averous M, Gali_fer RB, Dalla-Vale F, Ichay L, Morin D. Posterior Urethra Valves. Current status in Languedoc-Roussillon from 1998 to 2007: antenatal, neonatal data, medium-term outcomes. Archives of Pediatrics 2009; 16(5): 417-425.
[19]
Gargah T, Gharbi Y, Ben Moussa M, Kaabar N, Lakhoua M. Posterior urethral valves: a report of 44 cases. Tun Med 2010 ; 88(8): 557-562. 2010.
Khemakhem R, Ben Ahmed Y, Mefteh S, Jlidi S, Charieg A, Louati H, et al. Posterior urethral valves: a report of 38 cases. J Pediatrics and Childcare. oct 2012; 25(5): 242‑8.
[22]
Tachdjian G, Brisset S, Courtout A-M et al. Human embryology and histology. Elsevier Masson. 2016.
Sagna A, Ndoye M, Mbaye Pa, Ngoy M, Ngom G. Postnatal endoscopic resection of the posterior urethral valves in boys: a preliminary study of 23 cases. Urology Andrology, 2018: 1(9): 409-414.
[25]
Talabi AO, Sowande OA, Etonyeaku AC, Salako AA, Adejuyigbe O Posterior urethral valves in children: presentation and outcome of initial treatment at Ile-Ife, Nigeria. Niger J Surg Off Publ Niger Surg Res Soc. 2015 ; 21(2): 151-6. 2015.
[26]
Heikkilä J, Holmberg C, Kyllönen L, Rintala R, Taskinen S. Long-Term Risk of End Stage Renal Disease in Patients With Posterior Urethral Valves. J Urol. dec 2011; 186(6): 2392‑6.
[27]
Denes ED, Barthold JS et Gonzalez R : Early prognostic value of serum creatinine levels in children with posterior urethral valves. J Urol, 1997 ; 157 : 1441.
Mbouche, L. O., Mbassi, A. A., Ngalle, F. G. E., Kouna, I. N. T., Dikongue, E. C., et al. (2026). Outcomes of Endoscopic Ablation of Posterior Urethral Valves in Children: A Retrospective Review. International Journal of Clinical Urology, 10(1), 35-41. https://doi.org/10.11648/j.ijcu.20261001.17
Mbouche, L. O.; Mbassi, A. A.; Ngalle, F. G. E.; Kouna, I. N. T.; Dikongue, E. C., et al. Outcomes of Endoscopic Ablation of Posterior Urethral Valves in Children: A Retrospective Review. Int. J. Clin. Urol.2026, 10(1), 35-41. doi: 10.11648/j.ijcu.20261001.17
@article{10.11648/j.ijcu.20261001.17,
author = {Landry Oriole Mbouche and Achille Aurele Mbassi and Frantz Guy Epoupa Ngalle and Irene Nadine Tsala Kouna and Eugenie Caroline Dikongue and Bright Che Awondo and Rick Tristan Nguetsop and Justin Kamga and Faustin Tambo Mouafo and Forbuzshi Fru Angwafo III},
title = {Outcomes of Endoscopic Ablation of Posterior Urethral Valves in Children: A Retrospective Review},
journal = {International Journal of Clinical Urology},
volume = {10},
number = {1},
pages = {35-41},
doi = {10.11648/j.ijcu.20261001.17},
url = {https://doi.org/10.11648/j.ijcu.20261001.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20261001.17},
abstract = {Introduction: The management of posterior urethral valves is challenging in the absence of early diagnosis and optimal technical facilities. Once performed, endoscopic resection of the valves does not guarantee complete healing. The aim of our study was to investigate the outcome of patients treated for posterior urethral valves by endoscopic resection in two hospitals in the city of Yaounde. Materials and methods: This was a 5 years retrospective cross-sectional study conducted in two hospitals in the city of Yaounde from 2019 to 2024. All patients included had been treated for posterior urethral valves by endoscopic resection. Socio-demographic, diagnostic, therapeutic and prognostic variables were investigated. Results: A total of 35 patients were treated over the five-year period, with an admission rate of 6 cases per year. The median age at presentation was 02 years, and 29 participants (82.8%) presented late. Dysuria and recurrent urinary tract infections were the main reasons for consultation. Endoscopic valve ablation relieved obstruction in all participants except 5 (14.3%) who had residual valves. Creatinine levels and glomerular filtration rate before and after resection were measured in 15 participants; among them, 9 (47.5%) had renal insufficiency with a GFR 2, which did not improve after valve resection. Uroflowmetry showed abnormalities in three patients with a Qmax Conclusion: Endoscopic resection of posterior urethral valves significantly improves micturition. Follow-up is necessary to prevent complications.},
year = {2026}
}
TY - JOUR
T1 - Outcomes of Endoscopic Ablation of Posterior Urethral Valves in Children: A Retrospective Review
AU - Landry Oriole Mbouche
AU - Achille Aurele Mbassi
AU - Frantz Guy Epoupa Ngalle
AU - Irene Nadine Tsala Kouna
AU - Eugenie Caroline Dikongue
AU - Bright Che Awondo
AU - Rick Tristan Nguetsop
AU - Justin Kamga
AU - Faustin Tambo Mouafo
AU - Forbuzshi Fru Angwafo III
Y1 - 2026/03/17
PY - 2026
N1 - https://doi.org/10.11648/j.ijcu.20261001.17
DO - 10.11648/j.ijcu.20261001.17
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 35
EP - 41
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20261001.17
AB - Introduction: The management of posterior urethral valves is challenging in the absence of early diagnosis and optimal technical facilities. Once performed, endoscopic resection of the valves does not guarantee complete healing. The aim of our study was to investigate the outcome of patients treated for posterior urethral valves by endoscopic resection in two hospitals in the city of Yaounde. Materials and methods: This was a 5 years retrospective cross-sectional study conducted in two hospitals in the city of Yaounde from 2019 to 2024. All patients included had been treated for posterior urethral valves by endoscopic resection. Socio-demographic, diagnostic, therapeutic and prognostic variables were investigated. Results: A total of 35 patients were treated over the five-year period, with an admission rate of 6 cases per year. The median age at presentation was 02 years, and 29 participants (82.8%) presented late. Dysuria and recurrent urinary tract infections were the main reasons for consultation. Endoscopic valve ablation relieved obstruction in all participants except 5 (14.3%) who had residual valves. Creatinine levels and glomerular filtration rate before and after resection were measured in 15 participants; among them, 9 (47.5%) had renal insufficiency with a GFR 2, which did not improve after valve resection. Uroflowmetry showed abnormalities in three patients with a Qmax Conclusion: Endoscopic resection of posterior urethral valves significantly improves micturition. Follow-up is necessary to prevent complications.
VL - 10
IS - 1
ER -
Surgical Department, Yaounde Gynaeco-Obstretrics and Paediatrics Hospital, Yaoundé, Cameroon;Faculty of Medicine and Biomedical Sciences, University of Yaounde I, Yaoundé, Cameroon
Surgical Department, Yaounde Gynaeco-Obstretrics and Paediatrics Hospital, Yaoundé, Cameroon;Faculty of Medicine and Biomedical Sciences, University of Yaounde I, Yaoundé, Cameroon
Eugenie Caroline Dikongue
Surgical Department, Yaounde Gynaeco-Obstretrics and Paediatrics Hospital, Yaoundé, Cameroon
Bright Che Awondo
Faculty of Medicine and Biomedical Sciences, University of Yaounde I, Yaoundé, Cameroon
Rick Tristan Nguetsop
Higher Institute of Health Sciences Bangangte, Bangangte, Cameroon
Justin Kamga
Andre Fouda Medical Foundation, Yaounde, Cameroon
Faustin Tambo Mouafo
Surgical Department, Yaounde Gynaeco-Obstretrics and Paediatrics Hospital, Yaoundé, Cameroon;Faculty of Medicine and Biomedical Sciences, University of Yaounde I, Yaoundé, Cameroon
Forbuzshi Fru Angwafo III
Faculty of Medicine and Biomedical Sciences, University of Yaounde I, Yaoundé, Cameroon
Mbouche, L. O., Mbassi, A. A., Ngalle, F. G. E., Kouna, I. N. T., Dikongue, E. C., et al. (2026). Outcomes of Endoscopic Ablation of Posterior Urethral Valves in Children: A Retrospective Review. International Journal of Clinical Urology, 10(1), 35-41. https://doi.org/10.11648/j.ijcu.20261001.17
Mbouche, L. O.; Mbassi, A. A.; Ngalle, F. G. E.; Kouna, I. N. T.; Dikongue, E. C., et al. Outcomes of Endoscopic Ablation of Posterior Urethral Valves in Children: A Retrospective Review. Int. J. Clin. Urol.2026, 10(1), 35-41. doi: 10.11648/j.ijcu.20261001.17
@article{10.11648/j.ijcu.20261001.17,
author = {Landry Oriole Mbouche and Achille Aurele Mbassi and Frantz Guy Epoupa Ngalle and Irene Nadine Tsala Kouna and Eugenie Caroline Dikongue and Bright Che Awondo and Rick Tristan Nguetsop and Justin Kamga and Faustin Tambo Mouafo and Forbuzshi Fru Angwafo III},
title = {Outcomes of Endoscopic Ablation of Posterior Urethral Valves in Children: A Retrospective Review},
journal = {International Journal of Clinical Urology},
volume = {10},
number = {1},
pages = {35-41},
doi = {10.11648/j.ijcu.20261001.17},
url = {https://doi.org/10.11648/j.ijcu.20261001.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20261001.17},
abstract = {Introduction: The management of posterior urethral valves is challenging in the absence of early diagnosis and optimal technical facilities. Once performed, endoscopic resection of the valves does not guarantee complete healing. The aim of our study was to investigate the outcome of patients treated for posterior urethral valves by endoscopic resection in two hospitals in the city of Yaounde. Materials and methods: This was a 5 years retrospective cross-sectional study conducted in two hospitals in the city of Yaounde from 2019 to 2024. All patients included had been treated for posterior urethral valves by endoscopic resection. Socio-demographic, diagnostic, therapeutic and prognostic variables were investigated. Results: A total of 35 patients were treated over the five-year period, with an admission rate of 6 cases per year. The median age at presentation was 02 years, and 29 participants (82.8%) presented late. Dysuria and recurrent urinary tract infections were the main reasons for consultation. Endoscopic valve ablation relieved obstruction in all participants except 5 (14.3%) who had residual valves. Creatinine levels and glomerular filtration rate before and after resection were measured in 15 participants; among them, 9 (47.5%) had renal insufficiency with a GFR 2, which did not improve after valve resection. Uroflowmetry showed abnormalities in three patients with a Qmax Conclusion: Endoscopic resection of posterior urethral valves significantly improves micturition. Follow-up is necessary to prevent complications.},
year = {2026}
}
TY - JOUR
T1 - Outcomes of Endoscopic Ablation of Posterior Urethral Valves in Children: A Retrospective Review
AU - Landry Oriole Mbouche
AU - Achille Aurele Mbassi
AU - Frantz Guy Epoupa Ngalle
AU - Irene Nadine Tsala Kouna
AU - Eugenie Caroline Dikongue
AU - Bright Che Awondo
AU - Rick Tristan Nguetsop
AU - Justin Kamga
AU - Faustin Tambo Mouafo
AU - Forbuzshi Fru Angwafo III
Y1 - 2026/03/17
PY - 2026
N1 - https://doi.org/10.11648/j.ijcu.20261001.17
DO - 10.11648/j.ijcu.20261001.17
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 35
EP - 41
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20261001.17
AB - Introduction: The management of posterior urethral valves is challenging in the absence of early diagnosis and optimal technical facilities. Once performed, endoscopic resection of the valves does not guarantee complete healing. The aim of our study was to investigate the outcome of patients treated for posterior urethral valves by endoscopic resection in two hospitals in the city of Yaounde. Materials and methods: This was a 5 years retrospective cross-sectional study conducted in two hospitals in the city of Yaounde from 2019 to 2024. All patients included had been treated for posterior urethral valves by endoscopic resection. Socio-demographic, diagnostic, therapeutic and prognostic variables were investigated. Results: A total of 35 patients were treated over the five-year period, with an admission rate of 6 cases per year. The median age at presentation was 02 years, and 29 participants (82.8%) presented late. Dysuria and recurrent urinary tract infections were the main reasons for consultation. Endoscopic valve ablation relieved obstruction in all participants except 5 (14.3%) who had residual valves. Creatinine levels and glomerular filtration rate before and after resection were measured in 15 participants; among them, 9 (47.5%) had renal insufficiency with a GFR 2, which did not improve after valve resection. Uroflowmetry showed abnormalities in three patients with a Qmax Conclusion: Endoscopic resection of posterior urethral valves significantly improves micturition. Follow-up is necessary to prevent complications.
VL - 10
IS - 1
ER -