Introduction: Lower urinary retention is one of the most common urological emergencies in the hospital setting, primarily affecting elderly men and most often related to prostatic pathologies. This study aimed to describe the therapeutic modalities and outcomes of lower urinary retention managed at the Yalgado Ouedraogo University Hospital Center (CHU-YO). Methodology: This was a prospective, descriptive, longitudinal study conducted from August 1, 2023, to January 31, 2024, in the urological emergency department of CHU-YO. All patients admitted for urinary retention were included, except those already catheterized or non-consenting. Epidemiological, clinical, paraclinical, and therapeutic data were collected via Kobo Toolbox and analyzed with SPSS 20. Results: Out of 333 urological emergencies, 198 cases of urinary retention were identified (59.46%). After exclusions, 181 patients were analyzed. The mean age was 65.8 years, with a marked male predominance (92.8%). Retention was complete in 87.3% of cases and of sudden onset in 91.2%. Prostatic pathologies were the main etiology in men, followed by urethral strictures. Obstructive renal failure was present in 34.8% of patients prior to drainage. Transurethral bladder catheterization was the primary drainage method, with a failure rate of 10.9%. Post-drainage complications were dominated by decompression hematuria (5.0%) and post-obstructive diuresis syndrome (4.4%). The mean hospital stay was 3.7 days. Conclusion: Lower urinary retention remains a frequent emergency at CHU-YO, primarily affecting elderly men and dominated by prostatic pathologies. Late diagnosis exposes patients to a high risk of renal complications, underscoring the need for early screening of voiding disorders and strengthening of management capacities at the peripheral level.
| Published in | International Journal of Clinical Urology (Volume 10, Issue 1) |
| DOI | 10.11648/j.ijcu.20261001.15 |
| Page(s) | 19-27 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Urinary Retention, Urological Emergencies, Prostate, Bladder Drainage
Sociodemographic characteristics | Frequency (n=181) | Percentage (%) |
|---|---|---|
Age | ||
< 25 | 6 | 3.31 |
[25-50] | 14 | 7.73 |
[50-75] | 82 | 45.54 |
≥ 75 | 79 | 43.42 |
Gender | ||
Male | 168 | 92.82 |
Female | 13 | 7.18 |
Origin | ||
Urban area | 118 | 65.19 |
Rural area | 63 | 34.81 |
Occupation | ||
Farmer | 88 | 48.62 |
Salaried employee | 36 | 19.89 |
Merchant | 20 | 11.05 |
Housewife | 11 | 6.08 |
Retired | 9 | 4.97 |
Other * | 17 | 9.39 |
Literacy | ||
Non-literate | 121 | 66.85 |
Literate | 60 | 33.15 |
Marital status | ||
Married | 132 | 75.00 |
Widowed | 34 | 19.32 |
Single | 10 | 5.68 |
Anamnestic Data | Frequency | Percentage (%) |
|---|---|---|
Mode of admission | ||
Referral | 96 | 53.04 |
Direct admission | 78 | 43.09 |
Transfer | 7 | 3.87 |
Reason for admission | ||
Complete retention | 158 | 87.30 |
Incomplete retention | 23 | 12.70 |
Circumstances of onset | ||
Sudden | 165 | 91.16 |
Progressive | 7 | 3.87 |
Trauma | 4 | 2.21 |
Post-anesthetic | 3 | 1.66 |
Travel | 1 | 0.55 |
Hematuria | 1 | 0.55 |
Medical History | ||
Hypertension | 68 | 37.57 |
Diabetes | 13 | 7.18 |
Stroke | 8 | 4.42 |
Neuroleptic use | 5 | 2.76 |
Urological History | ||
Urinary schistosomiasis | 41 | 22.65 |
Urinary catheterization | 36 | 19.89 |
Repeated urethritis | 22 | 12.15 |
Prostate surgery | 7 | 3.87 |
Urethroplasty | 3 | 1.65 |
Urinary lithiasis | 2 | 1.10 |
Functional Symptoms | Frequency (n=181) | Percentage (%) |
|---|---|---|
Filling Phase | ||
Nocturia | 147 | 81.22 |
Urgency | 144 | 79.56 |
Frequency | 142 | 78.45 |
Voiding Phase | ||
Dysuria | 145 | 80.11 |
Burning on micturition | 45 | 24.86 |
Post-voiding Phase | ||
Sensation of incomplete voiding | 121 | 66.85 |
Double voiding | 13 | 7.18 |
Physical Signs | Frequency | Percentage (%) |
|---|---|---|
General condition according to WHO | ||
Preserved (Stage 1, Stage 2) | 160 | 88.40 |
Impaired (Stage 3, Stage 4) | 21 | 11.60 |
Hypogastrium | ||
Bladder globe | 164 | 91.71 |
Mass | 3 | 1.66 |
Digital Rectal Examination of Prostate *(n = 168)* | ||
Increased volume | 150 | 82.87 |
Prostate suggestive of benign origin | 118 | 78.6 |
Prostate suggestive of malignancy | 32 | 22.11 |
Flat prostatic fossa | 6 | 3.31 |
Presence of a gynecological mass, *(n= 13)* | ||
3 | 1.65 | |
External Genitalia | ||
Normal urethral meatus | 168 | 92.88 |
Periurethral induration | 22 | 12.15 |
Blood Tests | Frequency | Percentage (%) |
|---|---|---|
Complete Blood Count | ||
Normal hemoglobin level | 80 | 61.54 |
Moderate anemia [7-12 g/dl] | 40 | 30.77 |
Severe anemia ≤ 6 g/dl | 10 | 7.69 |
Normal leukocyte count | 90 | 69.23 |
Hyperleukocytosis | 34 | 26.15 |
Leukopenia | 6 | 4.62 |
Serum Creatinine | ||
Normal | 115 | 63.54 |
Elevated | 66 | 36.46 |
Uremia | ||
Normal | 134 | 74.03 |
Elevated | 47 | 25.97 |
Blood Glucose | ||
Normal | 142 | 78.45 |
Elevated | 33 | 18.23 |
Low | 6 | 3.32 |
Elevated | 3 | 1.66 |
Ultrasound Findings | Frequency | Percentage (%) |
|---|---|---|
Kidneys and Upper Excretory Tract | ||
Ureterohydronephrosis | 23 | 15.23 |
Renal impairment | 9 | 5.96 |
Prostate | ||
Normal | 55 | 36.42 |
Homogeneous prostate hypertrophy | 59 | 39.07 |
Heterogeneous prostate hypertrophy | 31 | 20.53 |
Bladder | ||
Intravesical tissue mass | 6 | 3.97 |
Thick-walled bladder | 6 | 3.97 |
Bladder lithiasis | 5 | 3.31 |
Post-void Residual (ml) | ||
< 100 | 12 | 7.95 |
[100-300] | 16 | 10.60 |
≥300 | 2 | 1.32 |
AUA | American Urological Association |
AUR | Acute Urinary Retention |
BPH | Benign Prostatic Hyperplasia |
CHU-YO | Yalgado Ouedraogo University Hospital Center |
M/F | Male/Female |
PVR | Post-Void Residual |
RMUC | Retrograde Micturating Urethrocystography |
UR | Urinary Retention |
WHO | World Health Organization |
| [1] | Mevcha A, Drake MJ. Etiology and management of urinary retention in women. Indian Journal of Urology. June 2010; 26(2): 230. |
| [2] | Descazeaud A, Robert G, de La Taille A. Management of lower urinary tract obstruction related to BPH in patients with particular conditions and/or complications. Progrès en Urologie. Nov 1 2018; 28(15): 868-74. |
| [3] | Stoffel JT, Peterson AC, Sandhu JS, Suskind AM, Wei JT, Lightner DJ. AUA White Paper on Nonneurogenic Chronic Urinary Retention: Consensus Definition, Treatment Algorithm, and Outcome End Points. The Journal of Urology. July 1 2017; 198(1): 153-60. |
| [4] | Diallo TO, Diabate I, Barry M, Bah OR. The profile of urological emergencies in a regional hospital in Senegal: a 20-month retrospective study. Pan African Medical Journal. 2022; 42(1). |
| [5] | Vadandi V, Mahamat A, Minguemadji A, Temga OM, Vounouzia B, Abdelmamoud C, et al. Management of Urine Retention in the Emergency Department of the Abeche University Teaching Hospital. Health sciences and disease. Nov 24 2023; 24(12). |
| [6] | Nonoa B, Sikpa KH, Sade SR, Agbedey MS, Botcho G, Padja E, et al. Acute urinary retention in adults at the teaching hospital of Kara: initial management and etiological diagnosis: Acute urinary retention in adults at the teaching hospital of Kara: initial management and etiological diagnosis. Journal of Scientific Research of the University of Lome Dec 20 2023; 25(3): 135-41. |
| [7] | Gas J. Management of chronic urinary retention in 2019. Progrès en Urologie - FMC. Dec 1 2019; 29(4): F91-4. |
| [8] | Diabaté I, Ondo CZ, Sow I, Ba A, MBoup C. Urological emergencies at the Louga hospital center, Senegal: epidemiological aspects and evaluation of management. African journal of urology. Sept 1 2015; 21(3): 181-6. |
| [9] | Botcho G, Tengué K, Kpatcha TM, Sewa EV, Leloua E, Sikpa HK, et al. Management of acute urinary retention at the CHU Sylvanus Olympio in Lome. Journal of Scientific Research of the University of Lome. Nov 22 2016; 18(3): 181-8. |
| [10] | Bouhours AC, Bigot P, Orsat M, Hoarau N, Descamps P, Fournié A, et al. Postpartum bladder retention. Progrès en urologie. Jan 1 2011; 21(1): 11-7. |
| [11] | Horgan AF, Prasad B, Waldron DJ, O'sullivan DC. Acute Urinary Retention. Comparison of Suprapubic and Urethral Catheterisation. British Journal of Urology. 1992; 70(2): 149-51. |
| [12] | Tengue K, Kpatcha TM, Sewa E, Adabra K, Amavi AK, Sikpa K, et al. Management of urological emergencies in Togo. Uro-Andro. 2017 Mar 2; 1(7): 331-4. |
| [13] | Pinar U, Gas J, Sarrazin C, Anract J, Chevrot A, Fassi-Fehri H, et al. Management of acute urinary retention in men in the context of benign prostatic hyperplasia: literature review and good practice recommendations from the Male Voiding Disorders Committee (CTMH). Progrès en Urologie - FMC. Nov 1 2025; 35(7): 288-99. |
APA Style
Ouattara, A., Kirakoya, B., Sawadogo, H., Lingani, N., Traore, Y. J. R. P., et al. (2026). Management of Lower Urinary Retention at the Yalgado Ouedraogo University Hospital Center. International Journal of Clinical Urology, 10(1), 19-27. https://doi.org/10.11648/j.ijcu.20261001.15
ACS Style
Ouattara, A.; Kirakoya, B.; Sawadogo, H.; Lingani, N.; Traore, Y. J. R. P., et al. Management of Lower Urinary Retention at the Yalgado Ouedraogo University Hospital Center. Int. J. Clin. Urol. 2026, 10(1), 19-27. doi: 10.11648/j.ijcu.20261001.15
@article{10.11648/j.ijcu.20261001.15,
author = {Abdoul-Karim Ouattara and Brahima Kirakoya and Hassami Sawadogo and Neimatou Lingani and Yannick Jean Rodrigue Pingdwende Traore and Fatao Ouedraogo and Clotaire Alexis Marie Kiemdiba Donega Yameogo and Abdoul-Karim Pare and Adama Ouattara and Fasnewinde Aristide Kabore},
title = {Management of Lower Urinary Retention at the Yalgado Ouedraogo University Hospital Center},
journal = {International Journal of Clinical Urology},
volume = {10},
number = {1},
pages = {19-27},
doi = {10.11648/j.ijcu.20261001.15},
url = {https://doi.org/10.11648/j.ijcu.20261001.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20261001.15},
abstract = {Introduction: Lower urinary retention is one of the most common urological emergencies in the hospital setting, primarily affecting elderly men and most often related to prostatic pathologies. This study aimed to describe the therapeutic modalities and outcomes of lower urinary retention managed at the Yalgado Ouedraogo University Hospital Center (CHU-YO). Methodology: This was a prospective, descriptive, longitudinal study conducted from August 1, 2023, to January 31, 2024, in the urological emergency department of CHU-YO. All patients admitted for urinary retention were included, except those already catheterized or non-consenting. Epidemiological, clinical, paraclinical, and therapeutic data were collected via Kobo Toolbox and analyzed with SPSS 20. Results: Out of 333 urological emergencies, 198 cases of urinary retention were identified (59.46%). After exclusions, 181 patients were analyzed. The mean age was 65.8 years, with a marked male predominance (92.8%). Retention was complete in 87.3% of cases and of sudden onset in 91.2%. Prostatic pathologies were the main etiology in men, followed by urethral strictures. Obstructive renal failure was present in 34.8% of patients prior to drainage. Transurethral bladder catheterization was the primary drainage method, with a failure rate of 10.9%. Post-drainage complications were dominated by decompression hematuria (5.0%) and post-obstructive diuresis syndrome (4.4%). The mean hospital stay was 3.7 days. Conclusion: Lower urinary retention remains a frequent emergency at CHU-YO, primarily affecting elderly men and dominated by prostatic pathologies. Late diagnosis exposes patients to a high risk of renal complications, underscoring the need for early screening of voiding disorders and strengthening of management capacities at the peripheral level.},
year = {2026}
}
TY - JOUR T1 - Management of Lower Urinary Retention at the Yalgado Ouedraogo University Hospital Center AU - Abdoul-Karim Ouattara AU - Brahima Kirakoya AU - Hassami Sawadogo AU - Neimatou Lingani AU - Yannick Jean Rodrigue Pingdwende Traore AU - Fatao Ouedraogo AU - Clotaire Alexis Marie Kiemdiba Donega Yameogo AU - Abdoul-Karim Pare AU - Adama Ouattara AU - Fasnewinde Aristide Kabore Y1 - 2026/02/25 PY - 2026 N1 - https://doi.org/10.11648/j.ijcu.20261001.15 DO - 10.11648/j.ijcu.20261001.15 T2 - International Journal of Clinical Urology JF - International Journal of Clinical Urology JO - International Journal of Clinical Urology SP - 19 EP - 27 PB - Science Publishing Group SN - 2640-1355 UR - https://doi.org/10.11648/j.ijcu.20261001.15 AB - Introduction: Lower urinary retention is one of the most common urological emergencies in the hospital setting, primarily affecting elderly men and most often related to prostatic pathologies. This study aimed to describe the therapeutic modalities and outcomes of lower urinary retention managed at the Yalgado Ouedraogo University Hospital Center (CHU-YO). Methodology: This was a prospective, descriptive, longitudinal study conducted from August 1, 2023, to January 31, 2024, in the urological emergency department of CHU-YO. All patients admitted for urinary retention were included, except those already catheterized or non-consenting. Epidemiological, clinical, paraclinical, and therapeutic data were collected via Kobo Toolbox and analyzed with SPSS 20. Results: Out of 333 urological emergencies, 198 cases of urinary retention were identified (59.46%). After exclusions, 181 patients were analyzed. The mean age was 65.8 years, with a marked male predominance (92.8%). Retention was complete in 87.3% of cases and of sudden onset in 91.2%. Prostatic pathologies were the main etiology in men, followed by urethral strictures. Obstructive renal failure was present in 34.8% of patients prior to drainage. Transurethral bladder catheterization was the primary drainage method, with a failure rate of 10.9%. Post-drainage complications were dominated by decompression hematuria (5.0%) and post-obstructive diuresis syndrome (4.4%). The mean hospital stay was 3.7 days. Conclusion: Lower urinary retention remains a frequent emergency at CHU-YO, primarily affecting elderly men and dominated by prostatic pathologies. Late diagnosis exposes patients to a high risk of renal complications, underscoring the need for early screening of voiding disorders and strengthening of management capacities at the peripheral level. VL - 10 IS - 1 ER -
Department of Urology, Manga Regional Hospital, Manga, Burkina Faso
Department of Urology, Yalgado Ouedraogo University Teaching Hospital, Ouagadougou, Burkina Faso
Department of Urology, Yalgado Ouedraogo University Teaching Hospital, Ouagadougou, Burkina Faso
Department of Urology, Yalgado Ouedraogo University Teaching Hospital, Ouagadougou, Burkina Faso
Department of Urology, Yalgado Ouedraogo University Teaching Hospital, Ouagadougou, Burkina Faso
Department of Urology, Yalgado Ouedraogo University Teaching Hospital, Ouagadougou, Burkina Faso
Division of Urology, Souro Sanou University Teaching Hospital, Bobo-Dioulasso, Burkina Faso
Division of Urology, Souro Sanou University Teaching Hospital, Bobo-Dioulasso, Burkina Faso
Department of Urology, Yalgado Ouedraogo University Teaching Hospital, Ouagadougou, Burkina Faso
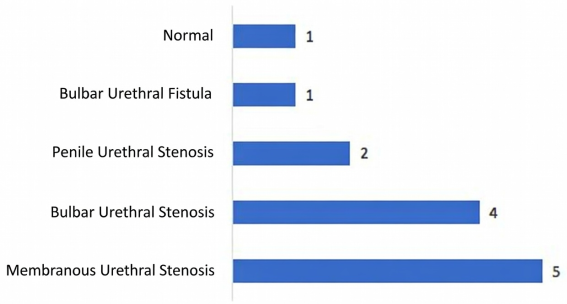
Figure 1. Distribution of patients according to the results of retrograde micturating urethrocystography.
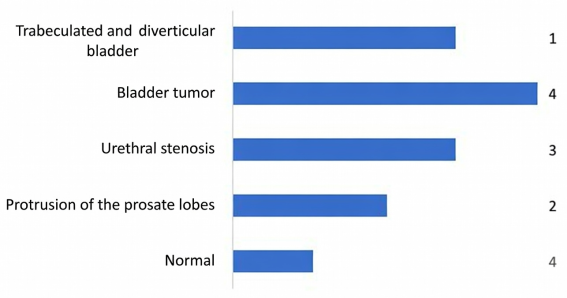
Figure 2. Distribution of patients according to the results of urethrocystoscopy.
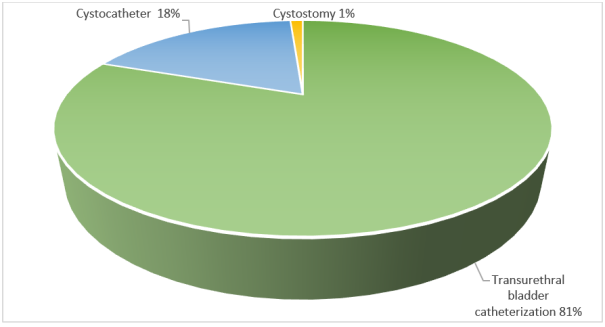
Figure 3. Distribution of patients according to the type of bladder drainage.
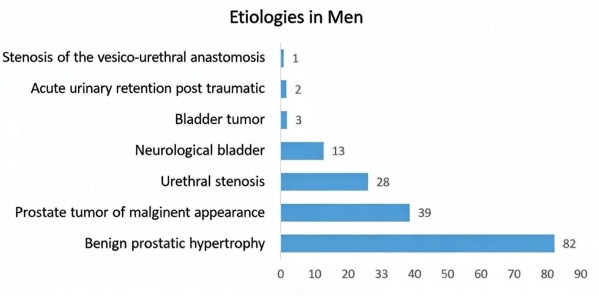
Figure 4. Distribution of male patients according to the etiological diagnosis.
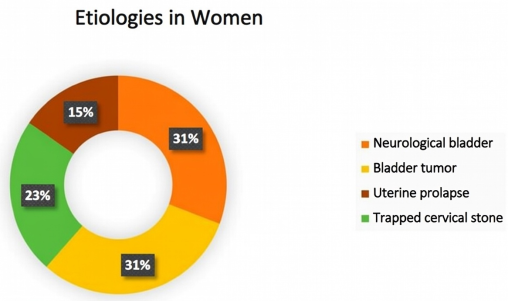
Figure 5. Distribution of patients according to the established etiological diagnosis in women.
Information

