Abstract
Background: Constrictive pericarditis has a variety of etiologies which leads to severe symptoms and heart failure which affects the quality of life. So far the main modality of treatment is pericardiectomy. Objective: The aim of this research was to know pericardiectomy outcomes and determinants among constrictive pericarditis patients who were operated at Tikur Anbessa Specialized Hospital from 2014 - 2022. Methods: A retrospective study was done among 65 patients. Data was presented using frequencies with percentages, mean (±standard deviation) and/ or median (interquartile range) as required. Perioperative mortality and complications were summarized using incidence density with 95% confidence interval (CI). Result: Most patients were in their 20s (53.8%) and where male are (84.6%). The commonest presenting symptom was shortness of breath (100%), fatiguability (96.9%), and coughs (66.2%). The median time of presentation was 12.3 months (IQR, 7.0-25.5). There were also cases with clinical symptoms of tuberculosis (13.8%). The etiology of constrictive pericarditis was infectious in 83.1% of cases. The mean length of surgery was 3.3 ± 0.6 hours. The median duration of hospital stay is 9.0 days (IQR, 7.0-12.0). The incidence rate (IR) of perioperative death was 7.9 per 1000 person-days (PD) of observation (94% CI = 3.3 – 19.2) and the incidence rate of complication was 4.8 per 1000 PD (95% CI = 1.5 -14.9). Conclusion: Pericardiectomy is the best treatment for patients with constrictive pericarditis. The majority of patients had a good outcome, with an improvement in symptoms and functional status. The mortality rate was low, and the complication rate was acceptable. However, this study is based on relatively small sample size, and it is a retrospective study from a single center. Hence, further prospective studies are needed to confirm the findings of this study.
Keywords
Pericardiectomy, Constrictive Pericarditis, Out Come
1. Introduction
1.1. Background
In patients with constrictive pericarditis (CP), a chronic inflammatory condition marked by fibrotic lesions and serous effusions, adherent parietal and visceral pericardium limits ventricular filling and impedes ventricular output. Ventricular compression is brought on by pericardial thickening, adhesions, and sporadic calcifications
| [1] | Faiza Z, Prakash A, Namburi N, Johnson B, Timsina L, Lee LS. Fifteen-year experience with pericardiectomy at a tertiary referral center. J Cardiothorac Surg. 2021 Jun 22; 16(1): 180. https://doi.org/10.1186/s13019-021-01561-4 |
| [2] | George, T. J., Arnaoutakis, G. J., Beaty, C. A., Kilic, A., Baumgartner, W. A., & Conte, J. V. (2012). Contemporary etiologies, risk factors, and outcomes after pericardiectomy. The Annals of thoracic surgery, 94(2), 445–451. https://doi.org/10.1016/j.athoracsur.2012.03.079 |
| [3] | Gillaspie EA, Stulak JM, Daly RC, Greason KL, Joyce LD, Oh J, Schaff HV, Dearani JA. A 20-year experience with isolated pericardiectomy: Analysis of indications and outcomes. J Thorac Cardiovasc Surg. 2016 Aug; 152(2): 448-58. https://doi.org/10.1016/j.jtcvs.2016.03.098 |
| [4] | DeValeria PA, Baumgartner WA, Casale AS, Greene PS, Cameron DE, Gardner TJ, Gott VL, Watkins L Jr, Reitz BA. Current indications, risks, and outcome after pericardiectomy. Ann Thorac Surg. 1991 Aug; 52(2): 219-24. https://doi.org/10.1016/0003-4975(91)91339-w |
| [5] | Vistarini N, Chen C, Mazine A, Bouchard D, Hebert Y, Carrier M, Cartier R, Demers P, Pellerin M, Perrault LP. Pericardiectomy for Constrictive Pericarditis: 20 Years of Experience at the Montreal Heart Institute. Ann Thorac Surg. 2015 Jul; 100(1): 107-13. https://doi.org/10.1016/j.athoracsur.2015.02.054 |
| [13] | Kumawat M, Lahiri TK, Agarwal D. Constrictive pericarditis: retrospective study of 109 patients. Asian Cardiovasc Thorac Ann. 2018 Jun; 26(5): 347-352. https://doi.org/10.1177/0218492318771490 |
[1-5, 13]
, resulting to restrictive heart failure in the end
| [10] | Szabó G, Schmack B, Bulut C, Soós P, Weymann A, Stadtfeld S, Karck M. Constrictive pericarditis: risks, aetiologies, and outcomes after total pericardiectomy: 24 years of experience. Eur J Cardiothorac Surg. 2013 Dec; 44(6): 1023-8; discussion 1028. https://doi.org/10.1093/ejcts/ezt138 |
[10]
, which may be life-threatening for the patient
| [1] | Faiza Z, Prakash A, Namburi N, Johnson B, Timsina L, Lee LS. Fifteen-year experience with pericardiectomy at a tertiary referral center. J Cardiothorac Surg. 2021 Jun 22; 16(1): 180. https://doi.org/10.1186/s13019-021-01561-4 |
| [2] | George, T. J., Arnaoutakis, G. J., Beaty, C. A., Kilic, A., Baumgartner, W. A., & Conte, J. V. (2012). Contemporary etiologies, risk factors, and outcomes after pericardiectomy. The Annals of thoracic surgery, 94(2), 445–451. https://doi.org/10.1016/j.athoracsur.2012.03.079 |
| [3] | Gillaspie EA, Stulak JM, Daly RC, Greason KL, Joyce LD, Oh J, Schaff HV, Dearani JA. A 20-year experience with isolated pericardiectomy: Analysis of indications and outcomes. J Thorac Cardiovasc Surg. 2016 Aug; 152(2): 448-58. https://doi.org/10.1016/j.jtcvs.2016.03.098 |
| [4] | DeValeria PA, Baumgartner WA, Casale AS, Greene PS, Cameron DE, Gardner TJ, Gott VL, Watkins L Jr, Reitz BA. Current indications, risks, and outcome after pericardiectomy. Ann Thorac Surg. 1991 Aug; 52(2): 219-24. https://doi.org/10.1016/0003-4975(91)91339-w |
| [5] | Vistarini N, Chen C, Mazine A, Bouchard D, Hebert Y, Carrier M, Cartier R, Demers P, Pellerin M, Perrault LP. Pericardiectomy for Constrictive Pericarditis: 20 Years of Experience at the Montreal Heart Institute. Ann Thorac Surg. 2015 Jul; 100(1): 107-13. https://doi.org/10.1016/j.athoracsur.2015.02.054 |
| [6] | Murashita T, Schaff HV, Daly RC, Oh JK, Dearani JA, Stulak JM, King KS, Greason KL. Experience With Pericardiectomy for Constrictive Pericarditis Over Eight Decades. Ann Thorac Surg. 2017 Sep; 104(3): 742-750. https://doi.org/10.1016/j.athoracsur.2017.05.063 |
[1-6]
.
Constriction has an intricate pathophysiology
| [10] | Szabó G, Schmack B, Bulut C, Soós P, Weymann A, Stadtfeld S, Karck M. Constrictive pericarditis: risks, aetiologies, and outcomes after total pericardiectomy: 24 years of experience. Eur J Cardiothorac Surg. 2013 Dec; 44(6): 1023-8; discussion 1028. https://doi.org/10.1093/ejcts/ezt138 |
[10]
. It is characterized by a reduce in stroke volume and an increase in ventricular diastolic pressures because of the pericardial thickness
| [6] | Murashita T, Schaff HV, Daly RC, Oh JK, Dearani JA, Stulak JM, King KS, Greason KL. Experience With Pericardiectomy for Constrictive Pericarditis Over Eight Decades. Ann Thorac Surg. 2017 Sep; 104(3): 742-750. https://doi.org/10.1016/j.athoracsur.2017.05.063 |
[6]
. It causes the intrathoracic and intracardiac pressures to diverge and increases the dependency of the ventricles. Since the right heart is the circuit with the lowest pressure, it is the one that is most restricted. The mean central venous pressure increases, a and v waves become more pronounced, and the x and y-descents become steeper due to the rigidity of the pericardium. Systemic venous congestion is the initial cause of several clinical features such as pedal edema, hepatomegaly, and ascites. Periodically, recurrent, inexplicable pleural effusions may be the first sign to appear. Afterwards, evidence of decreased cardiac output occur
| [14] | Gatti G, Fiore A, Ternacle J, Porcari A, Fiorica I, Poletti A, Ecarnot F, Bussani R, Pappalardo A, Chocron S, Folliguet T, Perrotti A. Pericardiectomy for constrictive pericarditis: a risk factor analysis for early and late failure. Heart Vessels. 2020 Jan; 35(1): 92-103. https://doi.org/10.1007/s00380-019-01464-4 |
[14]
.
The diagnosis of constrictive pericarditis is established using typical clinical presentation, which includes abnormal ECG readings and symptoms like pulsus paradoxus, jugular venous pulse, pericardial knock (sometimes called a fast filling sound), and pericardial rub. Echocardiography is the main diagnostic method used to detect constriction, effusion, or effusion with constriction, and to confirm the diagnosis. It also displays floating flakes in the pericardial sac and provides information about vein flow in the liver and inferior vena cava (IVC). Additionally, echocardiography assesses the ejection fraction and eliminates other associated issues. In the modern era, heart CT and MRI have become the standard for diagnosis. Chronic constrictive pericarditis may be more likely to be diagnosed if there are observable clinical signs and calcification in the cardio-pericardial area on imaging. The presence of a normal pericardial picture rules out constrictive pericarditis, while calcification of the pericardium rules out restrictive cardiomyopathy. Computed tomography and magnetic resonance imaging are considered more effective in evaluating pericardial anatomy. Invasive cardiac catheterization and pressure measurements can reveal predominant ventricular filling in the first third of diastole. During mid- and late diastole, when the pericardial sac becomes fixed and stiff, it can no longer stretch, causing the abrupt cessation of heart chamber filling. This restriction equalizes the pressures in the right atrium, right ventricle, and pulmonary wedge pressure during diastole, with the pulmonary wedge pressure reflecting the left heart's diastolic pressure. A pericardium thickness of 7 mm or more is a strong indicator of constrictive features, but a thickness exceeding 4 mm does not necessarily indicate constriction
| [10] | Szabó G, Schmack B, Bulut C, Soós P, Weymann A, Stadtfeld S, Karck M. Constrictive pericarditis: risks, aetiologies, and outcomes after total pericardiectomy: 24 years of experience. Eur J Cardiothorac Surg. 2013 Dec; 44(6): 1023-8; discussion 1028. https://doi.org/10.1093/ejcts/ezt138 |
| [13] | Kumawat M, Lahiri TK, Agarwal D. Constrictive pericarditis: retrospective study of 109 patients. Asian Cardiovasc Thorac Ann. 2018 Jun; 26(5): 347-352. https://doi.org/10.1177/0218492318771490 |
[10, 13]
.
Previously, tuberculosis (TB) played a significant role, but nowadays, the majority of cases are of unknown origin or stem from past radiation therapy or surgery. Nonetheless, TB remains a significant cause of pericarditis in many developing countries, particularly in regions like sub-Saharan Africa where HIV infection has become widespread
| [24] | Adem Ali, H. Biluts, A. Bekele. Thoracic surgical unit, Tikur Anbessa Hospital, Department of Surgery, Medical Faculty, Addis Ababa University, Addis Ababa, Ethiopia Vol. 12 No. 1 (2007). |
[24]
. The natural progression of this condition is not well understood. Typically, without undergoing surgery, CP leads to worsening symptoms and often premature death, as indicated by observational studies and case studies. Furthermore, most patients who have undergone surgery experience an enhancement in their functional abilities and overall quality of life. As a result, the recommended treatment for symptomatic CP is almost always pericardiectomy
| [9] | Bertog SC, Thambidorai SK, Parakh K, Schoenhagen P, Ozduran V, Houghtaling PL, Lytle BW, Blackstone EH, Lauer MS, Klein AL. Constrictive pericarditis: etiology and cause-specific survival after pericardiectomy. J Am Coll Cardiol. 2004 Apr 21; 43(8): 1445-52. https://doi.org/10.1016/j.jacc.2003.11.048 |
[9]
. In the majority of instances, pericardiectomy proves to be a beneficial intervention. After the diagnosis has been established, the most effective treatment for symptomatic CP remains pericardiectomy, which should be performed promptly
| [5] | Vistarini N, Chen C, Mazine A, Bouchard D, Hebert Y, Carrier M, Cartier R, Demers P, Pellerin M, Perrault LP. Pericardiectomy for Constrictive Pericarditis: 20 Years of Experience at the Montreal Heart Institute. Ann Thorac Surg. 2015 Jul; 100(1): 107-13. https://doi.org/10.1016/j.athoracsur.2015.02.054 |
| [6] | Murashita T, Schaff HV, Daly RC, Oh JK, Dearani JA, Stulak JM, King KS, Greason KL. Experience With Pericardiectomy for Constrictive Pericarditis Over Eight Decades. Ann Thorac Surg. 2017 Sep; 104(3): 742-750. https://doi.org/10.1016/j.athoracsur.2017.05.063 |
[5, 6]
.
Various surgical methods, including left anterior thoracotomy, bilateral thoracotomies, and median sternotomies, have been employed. Typically, the latter provides the most comprehensive exposure. Pericardiectomy is generally coupled with early hemodynamic stabilization
| [13] | Kumawat M, Lahiri TK, Agarwal D. Constrictive pericarditis: retrospective study of 109 patients. Asian Cardiovasc Thorac Ann. 2018 Jun; 26(5): 347-352. https://doi.org/10.1177/0218492318771490 |
| [24] | Adem Ali, H. Biluts, A. Bekele. Thoracic surgical unit, Tikur Anbessa Hospital, Department of Surgery, Medical Faculty, Addis Ababa University, Addis Ababa, Ethiopia Vol. 12 No. 1 (2007). |
[13, 24]
.
1.2. Statement of the Problem
In the general population the true incidence of constrictive pericarditis is not well understood due to its potentially subtle and painless nature, making detection challenging. However, traditional estimates indicate that around 6% of autopsies indicate signs of pericarditis, which represents approximately 1/1000 of patients admitted to hospital
| [3] | Gillaspie EA, Stulak JM, Daly RC, Greason KL, Joyce LD, Oh J, Schaff HV, Dearani JA. A 20-year experience with isolated pericardiectomy: Analysis of indications and outcomes. J Thorac Cardiovasc Surg. 2016 Aug; 152(2): 448-58. https://doi.org/10.1016/j.jtcvs.2016.03.098 |
[3]
. Up to 5% of individuals experiencing chest pain are diagnosed with this condition, where only a small percentage develops chronic symptoms. It is believed that 20% of individuals diagnosed with pericarditis may eventually require pericardiectomy. While a history of viral infections, previous heart surgeries, and mediastinal radiation are considered underlying factors in developed countries, the precise cause of pericarditis remains unknown
| [1] | Faiza Z, Prakash A, Namburi N, Johnson B, Timsina L, Lee LS. Fifteen-year experience with pericardiectomy at a tertiary referral center. J Cardiothorac Surg. 2021 Jun 22; 16(1): 180. https://doi.org/10.1186/s13019-021-01561-4 |
[1]
. Between 0.2% and 0.4% of heart surgical procedures lead to CP within the initial two years. TB is the primary cause of pericarditis in underdeveloped countries, often occurring alongside HIV infection and accounting for 22% to 91% of cases
| [1] | Faiza Z, Prakash A, Namburi N, Johnson B, Timsina L, Lee LS. Fifteen-year experience with pericardiectomy at a tertiary referral center. J Cardiothorac Surg. 2021 Jun 22; 16(1): 180. https://doi.org/10.1186/s13019-021-01561-4 |
[1]
. In developed nations, idiopathic factors account for 46.4% of CP cases, while post-cardiac surgery contributes to 19.6%, post-mediastinal radiation to 9.3%, and other causes (such as autoimmune, TB, rheumatic, or mixed) make up the remaining 24.7% of cases
| [2] | George, T. J., Arnaoutakis, G. J., Beaty, C. A., Kilic, A., Baumgartner, W. A., & Conte, J. V. (2012). Contemporary etiologies, risk factors, and outcomes after pericardiectomy. The Annals of thoracic surgery, 94(2), 445–451. https://doi.org/10.1016/j.athoracsur.2012.03.079 |
[2]
.
Treatment for constrictive pericarditis involves medical therapy and surgical procedures. Drugs like diuretics are useful for individuals with mild or no symptoms to avoid the risks of surgery. However, surgical pericardiectomy is the recommended approach for all other cases and provides relief from symptoms. Nevertheless, the operational risk and long-term mortality can vary depending on different factors, with a range of 5 to 10% and 15 to 70%, respectively
| [10] | Szabó G, Schmack B, Bulut C, Soós P, Weymann A, Stadtfeld S, Karck M. Constrictive pericarditis: risks, aetiologies, and outcomes after total pericardiectomy: 24 years of experience. Eur J Cardiothorac Surg. 2013 Dec; 44(6): 1023-8; discussion 1028. https://doi.org/10.1093/ejcts/ezt138 |
[10]
. In the United States, 21% of hospitalized individuals with constrictive pericarditis finally will undergo surgery
| [1] | Faiza Z, Prakash A, Namburi N, Johnson B, Timsina L, Lee LS. Fifteen-year experience with pericardiectomy at a tertiary referral center. J Cardiothorac Surg. 2021 Jun 22; 16(1): 180. https://doi.org/10.1186/s13019-021-01561-4 |
[1]
. The perioperative mortality rates for Pericardiectomy have varied, resulting in 2 to 15%
| [1] | Faiza Z, Prakash A, Namburi N, Johnson B, Timsina L, Lee LS. Fifteen-year experience with pericardiectomy at a tertiary referral center. J Cardiothorac Surg. 2021 Jun 22; 16(1): 180. https://doi.org/10.1186/s13019-021-01561-4 |
| [2] | George, T. J., Arnaoutakis, G. J., Beaty, C. A., Kilic, A., Baumgartner, W. A., & Conte, J. V. (2012). Contemporary etiologies, risk factors, and outcomes after pericardiectomy. The Annals of thoracic surgery, 94(2), 445–451. https://doi.org/10.1016/j.athoracsur.2012.03.079 |
[1, 2]
, with different long-term outcomes. Surgical mortality rates for pericardial effusion and constriction were 4.2% and 5.6%, respectively
| [4] | DeValeria PA, Baumgartner WA, Casale AS, Greene PS, Cameron DE, Gardner TJ, Gott VL, Watkins L Jr, Reitz BA. Current indications, risks, and outcome after pericardiectomy. Ann Thorac Surg. 1991 Aug; 52(2): 219-24. https://doi.org/10.1016/0003-4975(91)91339-w |
[4]
. Many patients undergoing surgery have also associated comorbidities, making it difficult to interpret the findings. Only a few studies have identified the risk factors for unsuccessful outcomes after constrictive pericarditis surgery. Investigations frequently recognize end-organ dysfunction, especially in the liver, kidney, and lungs, as a separate risk factor for death
| [11] | Busch C, Penov K, Amorim PA, Garbade J, Davierwala P, Schuler GC, Rastan AJ, Mohr FW. Risk factors for mortality after pericardiectomy for chronic constrictive pericarditis in a large single-centre cohort. Eur J Cardiothorac Surg. 2015 Dec; 48(6): e110-6. https://doi.org/10.1093/ejcts/ezv322 |
[11]
.
1.3. Significant of the Study
The result found from this research may contribute to the scientific findings on pericardiectomy outcome especially in resource limited set up.
2. Literature Review
Surgical removal of the pericardium is an effective treatment for pericarditis that does not respond to standard treatments, although it is relatively rare. Despite improving symptoms and the NYHA Class, a successful pericardiectomy carries a moderate to high risk of intermediate and long-term mortality, especially in patients with significant underlying medical conditions
| [1] | Faiza Z, Prakash A, Namburi N, Johnson B, Timsina L, Lee LS. Fifteen-year experience with pericardiectomy at a tertiary referral center. J Cardiothorac Surg. 2021 Jun 22; 16(1): 180. https://doi.org/10.1186/s13019-021-01561-4 |
[1]
. The high risk of death during surgery remains a characteristic of the outcomes of pericardiectomy for constrictive pericarditis. However, surgical intervention can elevate the functional class for most patients who survive long-term. Undergoing surgery early seems to be the most favorable choice. Preoperative clinical factors and concurrent health conditions are crucial in determining the risk of mortality. If a valvular procedure is performed concurrently, the optimal surgical approach is still to be determined
| [4] | DeValeria PA, Baumgartner WA, Casale AS, Greene PS, Cameron DE, Gardner TJ, Gott VL, Watkins L Jr, Reitz BA. Current indications, risks, and outcome after pericardiectomy. Ann Thorac Surg. 1991 Aug; 52(2): 219-24. https://doi.org/10.1016/0003-4975(91)91339-w |
| [5] | Vistarini N, Chen C, Mazine A, Bouchard D, Hebert Y, Carrier M, Cartier R, Demers P, Pellerin M, Perrault LP. Pericardiectomy for Constrictive Pericarditis: 20 Years of Experience at the Montreal Heart Institute. Ann Thorac Surg. 2015 Jul; 100(1): 107-13. https://doi.org/10.1016/j.athoracsur.2015.02.054 |
| [15] | Biçer M, Özdemir B, Kan İ, Yüksel A, Tok M, Şenkaya I. Long-term outcomes of pericardiectomy for constrictive pericarditis. J Cardiothorac Surg. 2015 Nov 27; 10: 177. https://doi.org/10.1186/s13019-015-0385-8 |
[4, 5, 15]
.
The mainstay of managing constrictive pericarditis remains pericardiectomy. An analysis of current retrospective data shows that most patients who undergo total pericardiectomy see a significant improvement in survival, symptoms, quality of life, hemodynamics, and cardiac function. Following pericardiectomy for constrictive pericarditis, long-term survival is influenced by the original cause, left ventricular systolic function, renal function, serum sodium levels, and pulmonary artery pressure. The safety of pericardiectomy in this group is demonstrated by the relatively high survival rate in idiopathic constrictive pericarditis cases
| [7] | Avgerinos D, Rabitnokov Y, Worku B, Neragi-Miandoab S, Girardi LN. Fifteen-year experience and outcomes of pericardiectomy for constrictive pericarditis. J Card Surg. 2014 Jul; 29(4): 434-8. https://doi.org/10.1111/jocs.12344 |
| [9] | Bertog SC, Thambidorai SK, Parakh K, Schoenhagen P, Ozduran V, Houghtaling PL, Lytle BW, Blackstone EH, Lauer MS, Klein AL. Constrictive pericarditis: etiology and cause-specific survival after pericardiectomy. J Am Coll Cardiol. 2004 Apr 21; 43(8): 1445-52. https://doi.org/10.1016/j.jacc.2003.11.048 |
| [10] | Szabó G, Schmack B, Bulut C, Soós P, Weymann A, Stadtfeld S, Karck M. Constrictive pericarditis: risks, aetiologies, and outcomes after total pericardiectomy: 24 years of experience. Eur J Cardiothorac Surg. 2013 Dec; 44(6): 1023-8; discussion 1028. https://doi.org/10.1093/ejcts/ezt138 |
[7, 9, 10]
.
In summary, pericardiectomy remains a safe option for constrictive pericarditis, even though survival rates vary significantly depending on the cause. Hypoalbuminemia, hyperbilirubinemia, and post-radiation pericarditis are important risk factors for decreased long-term survival. Lastly, despite changes in the etiologic spectrum over time, outcomes have not been altered. The spectrum has changed over time, but the outcomes have remained consistent. Compared to sub-total pericardiectomy, radical pericardiectomy has shown improved clinical performance and 10-year survival rates in patients with chronic constrictive pericarditis
| [2] | George, T. J., Arnaoutakis, G. J., Beaty, C. A., Kilic, A., Baumgartner, W. A., & Conte, J. V. (2012). Contemporary etiologies, risk factors, and outcomes after pericardiectomy. The Annals of thoracic surgery, 94(2), 445–451. https://doi.org/10.1016/j.athoracsur.2012.03.079 |
| [17] | Nishimura S, Izumi C, Amano M, Imamura S, Onishi N, Tamaki Y, Enomoto S, Miyake M, Tamura T, Kondo H, Kaitani K, Yamanaka K, Nakagawa Y. Long-Term Clinical Outcomes and Prognostic Factors After Pericardiectomy for Constrictive Pericarditis in a Japanese Population. Circ J. 2017 Jan 25; 81(2): 206-212. https://doi.org/10.1253/circj.CJ-16-0633 |
[2, 17]
.
Long-term clinical outcomes following pericardiectomy in a Japanese population were found to be associated with the underlying cause and the patient's preoperative clinical status. A study conducted in China at a single center indicated that total pericardiectomy is associated with reduced postoperative and late mortality. The extent of pericardial resection should be determined based on the specific circumstances of the patient. Proper preoperative care and complete relaxation of the left ventricle's thickened pericardium can help avoid postoperative issues. The Korean population experienced greater improvement in right ventricular systolic pressure and reduced tricuspid regurgitation over time with radical pericardiectomy compared to the traditional technique
| [17] | Nishimura S, Izumi C, Amano M, Imamura S, Onishi N, Tamaki Y, Enomoto S, Miyake M, Tamura T, Kondo H, Kaitani K, Yamanaka K, Nakagawa Y. Long-Term Clinical Outcomes and Prognostic Factors After Pericardiectomy for Constrictive Pericarditis in a Japanese Population. Circ J. 2017 Jan 25; 81(2): 206-212. https://doi.org/10.1253/circj.CJ-16-0633 |
| [18] | Zhu P, Mai M, Wu R, Lu C, Fan R, Zheng S. Pericardiectomy for constrictive pericarditis: single-center experience in China. J Cardiothorac Surg. 2015 Mar 19; 10: 34. https://doi.org/10.1186/s13019-015-0237-6 |
| [19] | Choi MS, Jeong DS, Oh JK, Chang SA, Park SJ, Chung S. Long-term results of radical pericardiectomy for constrictive pericarditis in Korean population. J Cardiothorac Surg. 2019 Feb 6; 14(1): 32. https://doi.org/10.1186/s13019-019-0845-7 |
[17-19]
.
For individuals with chronic constrictive pericarditis, poor outcomes after pericardiectomy were associated with preoperative high early diastolic mitral input velocity and diabetes mellitus
| [20] | Kang SH, Song JM, Kim M, Choo SJ, Chung CH, Kang DH, Song JK. Prognostic predictors in pericardiectomy for chronic constrictive pericarditis. J Thorac Cardiovasc Surg. 2014 Feb; 147(2): 598-605. https://doi.org/10.1016/j.jtcvs.2013.01.022 |
[20]
. This suggests that preoperative Doppler echocardiographic examination may help predict prognosis after pericardiectomy, in addition to diagnosing constrictive pericarditis. Chronic constrictive pericarditis can be surgically addressed to treat diastolic heart failure. This disease is most prevalent in nations where tuberculosis is endemic, such as Nepal. For individuals with tuberculous constrictive pericarditis, undergoing complete pericardiectomy was associated with a heightened risk of postoperative complications. Research has shown that elevated preoperative CVP and a lower preoperative NYHA functional class can forecast the outcome
| [22] | Jaiswal LS, Pandit N, Sah B. Surgical treatment of tuberculous chronic constrictive pericarditis: A retrospective observational study from tertiary hospital of eastern Nepal. Indian J Tuberc. 2021 Apr; 68(2): 174-178. https://doi.org/10.1016/j.ijtb.2020.08.002 |
| [23] | Fang L, Yu G, Huang J, Zhao W, Ye B. Predictors of postoperative complication and prolonged intensive care unit stay after complete pericardiectomy in tuberculous constrictive pericarditis. J Cardiothorac Surg. 2020 Jun 19; 15(1): 148. https://doi.org/10.1186/s13019-020-01198-9 |
[22, 23]
. Based on previous cases at Tikur Anbessa Hospital, pericardiectomy can be performed without the use of CPB and with minimal mortality, ultimately enhancing the functional ability of most patients
| [24] | Adem Ali, H. Biluts, A. Bekele. Thoracic surgical unit, Tikur Anbessa Hospital, Department of Surgery, Medical Faculty, Addis Ababa University, Addis Ababa, Ethiopia Vol. 12 No. 1 (2007). |
[24]
.
3. Objectives
3.1. General Objective
To evaluate pericardiectomy outcomes and its determinants among patients who were operated at TASH from 2014 to 2022.
3.2. Specific Objective
1) To determine pericardiectomy outcomes among patients who were operated at Tikur Anbessa specialized Hospital.
2) To identify determinants of pericardiectomy outcomes among patients who were operated at Tikur Anbessa specialized Hospital.
4. Methods
4.1. Study Setting and Period
The study was conducted from February 15/2023 to March 30/ 2023 at Tikur Anbessa specialized Hospital (TASH), a tertiary teaching hospital in Addis Ababa, Ethiopia. The hospital was established in 1972 as the teaching hospital of Addis Ababa University, College of Health Sciences. It is the largest referral hospital in the country with 700 in-patient beds. The Cardiothoracic surgery unit has a total of 15-20 in-patient beds and performs with an average of 288 cases annually.
4.2. Study Design
A retrospective study design employed among constrictive pericarditis patients that were operated in the hospital from 2014 to 2022.
4.3. Eligibility Criteria
4.3.1. Inclusion Criteria
All Patients who underwent pericardiectomy in the hospital during the study period were included.
4.3.2. Exclusion Criteria
Patients with incomplete data on the outcome or major exposure variables on their records were excluded.
4.4. Sampling Technique
A total of 69 cases were operated during the study period. All who fulfill the eligibility criteria were found to be 65 and all of them included.
4.5. Study Variables
4.5.1. Outcome Variable
1) NYHA clinical Improvement
2) Post-operative outcome
3) Recovery
4) complication
5) Death
a. mortality (at 30days)
b. mortality (at 1 year)
4.5.2. Exposure Variables
1) Age
2) sex,
3) place of residence
4) educational status …
5) Baseline clinical characteristics
a. Presenting symptom
b. Physical examination findings
6) Laboratory parameters
7) Radiologic findings
8) Intraoperative monitoring
9) Operative status
10) types of pericardiectomy
11) Duration of surgery
12) Rhythm
13) Etiologic causes
14) Prolonged intubation
15) Postop hemorrhage
16) Post-op follow-up duration
17) Rhythm status
18) Complications
19) Postop NYHA class functional status
20) Etiologic evidence of pericarditis
4.6. Operational Definitions
1) Pericardiectomy types
a. Total: the removal of all anterior pericardium between the phrenic nerve and from the great vessels superiorly down to and includes the diaphragm surface
| [2] | George, T. J., Arnaoutakis, G. J., Beaty, C. A., Kilic, A., Baumgartner, W. A., & Conte, J. V. (2012). Contemporary etiologies, risk factors, and outcomes after pericardiectomy. The Annals of thoracic surgery, 94(2), 445–451. https://doi.org/10.1016/j.athoracsur.2012.03.079 |
[2]
b. Subtotal: removal of less than the total
| [2] | George, T. J., Arnaoutakis, G. J., Beaty, C. A., Kilic, A., Baumgartner, W. A., & Conte, J. V. (2012). Contemporary etiologies, risk factors, and outcomes after pericardiectomy. The Annals of thoracic surgery, 94(2), 445–451. https://doi.org/10.1016/j.athoracsur.2012.03.079 |
[2]
c. Completion: completion of the incomplete pericardiectomy for recurrent CP
| [2] | George, T. J., Arnaoutakis, G. J., Beaty, C. A., Kilic, A., Baumgartner, W. A., & Conte, J. V. (2012). Contemporary etiologies, risk factors, and outcomes after pericardiectomy. The Annals of thoracic surgery, 94(2), 445–451. https://doi.org/10.1016/j.athoracsur.2012.03.079 |
[2]
2) Delayed extubation: defined as a postoperative mechanical ventilation lasting >48hours
| [2] | George, T. J., Arnaoutakis, G. J., Beaty, C. A., Kilic, A., Baumgartner, W. A., & Conte, J. V. (2012). Contemporary etiologies, risk factors, and outcomes after pericardiectomy. The Annals of thoracic surgery, 94(2), 445–451. https://doi.org/10.1016/j.athoracsur.2012.03.079 |
[2]
3) Perioperative mortality/ Hospital mortality: death during the initial hospitalization or within 30 days following surgery
| [9] | Bertog SC, Thambidorai SK, Parakh K, Schoenhagen P, Ozduran V, Houghtaling PL, Lytle BW, Blackstone EH, Lauer MS, Klein AL. Constrictive pericarditis: etiology and cause-specific survival after pericardiectomy. J Am Coll Cardiol. 2004 Apr 21; 43(8): 1445-52. https://doi.org/10.1016/j.jacc.2003.11.048 |
[9]
.
4.7. Data Collection and Quality Assurance
Data were collected from the patients’ medical record using a data abstraction tool that consists of all the variables. Data on the following variables was recorded; socio-demographic characteristics, preoperative characteristics and intraoperative characteristics that will be retrieved from the medical records (charts and electronic database). The post-operative endpoints will be recorded from follow-up progress notes. A pretest on 5% of randomly selected medical charts was made and the necessary revision on the data collection tool was made based on the test result.
Training on the basics of the data abstraction form and on how to use the form appropriately was given by the principal investigator for four General practitioners and one supervisor for one day. Data was collected from February 15/2023 to March 30/2023. The collected data was checked for its consistency and completeness before any attempt to enter code and analyze it. Data management and analysis were performed suing STATA software V 14.0.
4.8. Data Management and Analysis
Data was summarized using frequencies and percentages for categorical variables. For numerical variables, after testing for the assumption of normality using Kolmogorov Smirnov test of normality where p-value of <0.05 indicates skewed distribution, data was summarized with a mean ± standard deviation (SD) or median with Inter Quartile range (IQR) values for variables with normal or skewed distribution, respectively.
The incidence rate of perioperative mortality and complications were measured using incidence density where person time was calculated using the total number of days of hospital from post-operation to discharge/complication/death for each group and was finally reported as incidence per 1000 person-days (PD) of observation. Furthermore, the 95% CI for the calculated incidence density was reported.
4.9. Ethical Clearance
Ethical clearance was obtained from Department of Surgery Research committee and IRB of the College of Health Sciences, Addis Ababa University Access to the collected information was limited to the principal investigator and confidentiality was maintained throughout the study.
5. Result
From the 65 patients, majority were in their 20s (53.8%) and were male (84.6%). A large proportion of patients were from Oromia (40.0%), Amhara (26.2%), and Addis Ababa (18.5%). The most common presenting symptom was shortness of breath (SOB) (100%), followed by fatiguability (96.9%), and cough (66.2%). The median duration symptom upon admission was 12.3 months (IQR, 7.0-25.5). Clinically active symptoms complex for tuberculosis (TB) were found in 9 (13.8%), and none of the patients has a history of past or current smoking. In terms of etiology, 54 (83.1%) cases were due to infectious conditions and the remaining 11 (16.9%) were idiopathic.
Elevated JVP was present in 38 (58.5%) cases. Pericardial friction rub and pulsus paradoxus were recorded in 6 (9.2%) and 2 (3.1%) patients, respectively. Preoperative cardiac rhythm was normal in all patients. The mean systemic systolic and diastolic blood pressures were 105.8 ± 10.8 mmHg and 69.5 ± 8.7 mmHg, respectively. LVEF and RV function assessments showed a median of 60.0% (IQR=55.0-65.0%) and 19.0 mm (IQR=18.0-20.0), respectively.
The most frequently reported abnormal finding on ECG and CXR were left atrial enlargement in 5 (7.7%) and cardiomegaly in 28 (43.1%) cases, respectively. Echocardiography showed features of effusive and calcified constrictive pericarditis in 7 and 4 patients, respectively and Chest CT scan showed disseminated tuberculosis in 3 patients.
The preoperative functional status of the patients showed that majority of the patients were classified as Class 3 (64.6%) and 100% were Stage C.
During the intraoperative period, invasive monitoring was used in 61 (93.8%) of the patients, and chest surface ECG was used in 100% of patients for non-invasive monitoring. Sternotomy was used in 100% of patients for surgical approach and in all of the cases the surgery was elective. Total pericardiectomy was performed in 64 (98.5%) of the patients, and subtotal pericardiectomy was performed in 1 (1.5%) of the patients. The mean duration of operation was 3.3 ± 0.6 hours. Intraoperative rhythm status was abnormal in only one patient, who had atrial fibrillation. The majority of the patients (83.1%) had etiologic evidence of pericarditis, and 41 patients were treated for tuberculosis. Of these 41 patients, 13 had evidence of TB pericarditis on biopsy.
In 16 (24.6%) patients extubation was delayed. Postoperative abnormal rhythm status was recorded for one patient, who had atrial fibrillation. Postoperative CXR and Echo showed an improvement in the majority of cases, 46 (70.8%) and 60 (92.3%), respectively.
The postoperative functional status of the patients showed that the majority of the patients were classified as Class 1 (47.7%) and 2 (43.1%). In addition, 52 (80.0%) were classified as Stage B. There was no major post-operative bleeding in any of the patients.
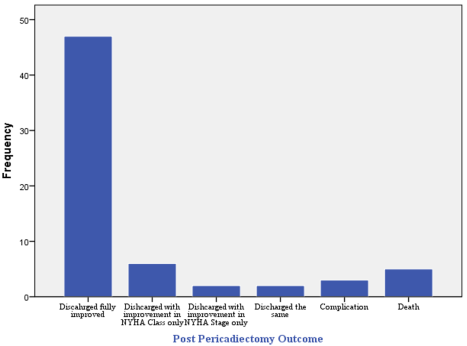
Among the 65 patients, 57 recovered and discharged alive, 3 complicated and 5 died. Of the 57 recovered cases, as compared to their preoperative status, 47 recovered with improvement in both NYHA Class and Stage, 6 recovered with improvement in their NYHA Class only, 2 recovered with improvement in their NYHA stage only, and 2 were discharged in same condition as their preoperative status (with Class 2 and Stage C state). The three complicated cases were due to hypocalcemia, atrial fibrillation, and acute kidney injury. The 5 deaths were mainly due to cardiac and respiratory arrest and intractable cardiac shock. (
Figure 1)
Figure 1. Post-operative outcomes of pericardiectomy among patients with constrictive pericarditis.
Table 1. Sociodemographic and preoperative parameters among constrictive pericardiectomy patients who underwent pericardiectomy (n=65).
Variable | Frequency (%) Median (IQR) Mean ± SD | Variable | Frequency (%) Median (IQR) Mean ± SD |
Age | | Cardiac rhythm status | |
12-19 | 10 (15.4) | Normal | 65 (100.0) |
20-29 | 35 (53.8) | Systemic SBP | 105.8 ± 10.8 |
30-39 | 10 (15.4) | Systemic DBP | 69.5 ± 8.7 |
40-60 | 10 (15.4) | LVEF (in %) | 60.0 (55.0-65.0) |
Sex | | RV function (in mm) | 19.0 (18.0-20.0) |
Male | 55 (84.6) | Laboratory parameters | |
Female | 10 (15.4) | SGOT | 38.0 (29.8-51.5) |
Place of residence | | SGPT | 28.0 (13.0-40.0) |
Addis Ababa | 12 (18.5) | ALP | 150.0 (99.0-223.5) |
Oromia | 25 (40.0) | BUN | 24.0 (16.5-30.0) |
Amhara | 17 (26.2) | Cr | 0.7 (0.5-0.9) |
SNNPR | 9 (13.8) | Serum K | 3.9 (3.5-4.3) |
Tigray | 1 (1.5) | Serum Na | 137.0 (135.0-140.5) |
Presenting symptom | | Serum Cl | 103.0 (99.0-108.0) |
Cough | 43 (66.2) | ECG | |
Chest pain | 13 (20.0) | Sinus rhythm | 47 (72.3) |
SOB | 65 (100.0) | Left atrial enlargement | 5 (7.7) |
Fatigability (body swelling) | 63 (96.9) | Left ventricular hypertrophy | 2 (3.1) |
Weight loss | 16 (24.6) | Atrial fibrillation and abnormal T-waves | 2 (3.1) |
Poor appetite | 8 (12.3) | Sinus tachycardia | 2 (3.1) |
Night sweating | 4 (6.2) | Inverted T-wave | 2 (3.1) |
Palpitation | 2 (3.1) | Right atrial enlargement | 1 (1.5) |
Fever | 1 (1.5) | Prolonged T-wave | 1 (1.5) |
Duration of symptom in months | 12.3 (7.0-25.5) | CXR | |
Etiology | | Normal | 11 (16.9) |
Idiopathic | 11 (16.9) | Cardiomegaly | 28 (43.1) |
Infectious | 54 (83.1) | Others* | 16 (24.6) |
Comorbidities/ TB symptoms | | Echo | |
Clinically active symptoms for TB | 9 (13.8) | Constrictive pericarditis | 54 (83.1) |
DVT | 2 (3.1) | effusive constrictive pericarditis | 7 (10.7) |
T4-RVI | 1 (1.5) | calcified constrictive pericarditis | 4 (6.2) |
AKI, SVC thrombosis | 1 (1.5) | Chest CT | |
Cigarette smoking | | Constrictive pericarditis | 24 (36.9) |
No | 65 (100.0) | Effusive constrictive pericarditis | 6 (9.2) |
JVP (CVP) status | | Calcified constrictive pericarditis | 4 (6.2) |
Normal | 27 (41.5) | Disseminated TB with constrictive physiology | 2 (3.1) |
Elevated | 38 (58.5) | Pre-op NYHA functional status Class | |
Pericardial friction rub | | 2 | 16 (24.6) |
No | 59 (90.8) | 3 | 42 (64.6) |
Yes | 6 (9.2) | 4 | 7 (10.8) |
Pulsus paradoxus | | Pre-op NYHA functional status Stage | |
No | 63 (96.9) | C | 65 (100.0) |
Yes | 2 (3.1) | | |
N.B.: Others* include pulmonary edema, pleural effusion, pericardial calcification and lung fibrosis.
Table 2. Intraoperative and postoperative parameters among constrictive pericardiectomy patients who underwent pericardiectomy (n=65).
Variable | Frequency Mean ± SD | Variable | Frequency |
Type of invasive Intra-op monitoring | | Prolonged intubation | |
Central/peripheral arterial line | 61 (93.8) | No | 49 (75.4) |
Other | 4 (6.2) | Yes | 16 (24.6) |
Type of non-invasive Intra-op monitoring | | Postoperative rhythm status | |
Chest surface ECG | 65 (100.0) | Normal | 64 (98.5) |
Type of surgical approach | | Abnormal (Atrial fibrillation) | 1 (1.5) |
Sternotomy | 65 (100.0) | CXR | |
Operative status | | Normal | 46 (70.8) |
Elective | 65 (100.0) | Pleural effusion | 16 (24.6) |
Type of pericardiectomy | | Right lung fibrosis, right lung opacity, right lower lobe consolidation | 3 (4.6) |
Total | 64 (98.5) | Echo | |
Sub-total | 1 (1.5) | Improved | 60 (92.3) |
Duration of operation (in hours) | 3.3 ± 0.6 | residual constrictive pericarditis | 4 (6.2) |
Rhythm status | | poor systolic function | 1 (1.5) |
Normal | 64 (98.5) | Post-op NYHA functional status Class | |
Abnormal (Atrial fibrillation) | 1 (1.5) | 1 | 31 (47.7) |
Etiologic evidence of pericarditis | | 2 | 28 (43.1) |
No | 11 (16.9) | 3 | 5 (7.7) |
Yes | 54 (83.1) | 4 | 1 (1.5) |
Treated for TB | 41 | Post-op NYHA functional status Stage | |
Biopsy-TB pericarditis | 13 | B | 52 (80.0) |
| | C | 13 (20.0) |
The 65 patients were followed for a median duration/ inpatient follow up/ of 9.0 days (IQR, 7.0-12.0). The incidence rate (IR) of perioperative mortality was 7.9 per 1000 person-days (PD) of observation (94% CI = 3.3 – 19.2). The incidence rate of complication was 4.8 per 1000 PD (95% CI = 1.5-14.9).
6. Discussion
This study investigated the outcomes of pericardiectomy for constrictive pericarditis. The study included 65 patients, with a median age of 27 years and a male predominance (84.6%). The most common presenting symptoms were shortness of breath (100%), fatigue (96.9%), and cough (66.2%). The median duration of symptoms before presentation was 12.3 days. The most common underlying etiology was infectious (83.1%), with tuberculosis being the most common specific diagnosis (13.8%). The presenting pattern in this study is in agreement with what is known so far except for age. The commonest age for constrictive pericarditis is reported in the 60s and there appears to be a male predominance, with some studies reporting a male-to-female ratio of 3:1. The most common presenting symptom is shortness of breath. Other symptoms include fatigue, cough, abdominal pain, and edema. In addition, literatures show that the most common underlying etiology is infectious, accounting for up to 80% of cases. Tuberculosis is the most common specific diagnosis, followed by cancer and autoimmune diseases
| [16] | Nozohoor S, Johansson M, Koul B, Cunha-Goncalves D. Radical pericardiectomy for chronic constrictive pericarditis. J Card Surg. 2018 Jun; 33(6): 301-307. https://doi.org/10.1111/jocs.13715 |
| [17] | Nishimura S, Izumi C, Amano M, Imamura S, Onishi N, Tamaki Y, Enomoto S, Miyake M, Tamura T, Kondo H, Kaitani K, Yamanaka K, Nakagawa Y. Long-Term Clinical Outcomes and Prognostic Factors After Pericardiectomy for Constrictive Pericarditis in a Japanese Population. Circ J. 2017 Jan 25; 81(2): 206-212. https://doi.org/10.1253/circj.CJ-16-0633 |
| [18] | Zhu P, Mai M, Wu R, Lu C, Fan R, Zheng S. Pericardiectomy for constrictive pericarditis: single-center experience in China. J Cardiothorac Surg. 2015 Mar 19; 10: 34. https://doi.org/10.1186/s13019-015-0237-6 |
[16-18]
. There are a number of reasons why pericarditis is more common in young people in developing countries. One reason is that these countries have higher rates of infectious diseases, such as tuberculosis and HIV, which can cause pericarditis. In addition, poor nutrition and exposure to environmental toxins, such as air pollution, can also increase the risk of developing pericarditis. This further is compounded by the lack of access to healthcare, which means that risk factors for pericarditis may not be diagnosed or treated on time to prevent complications
| [15] | Biçer M, Özdemir B, Kan İ, Yüksel A, Tok M, Şenkaya I. Long-term outcomes of pericardiectomy for constrictive pericarditis. J Cardiothorac Surg. 2015 Nov 27; 10: 177. https://doi.org/10.1186/s13019-015-0385-8 |
| [16] | Nozohoor S, Johansson M, Koul B, Cunha-Goncalves D. Radical pericardiectomy for chronic constrictive pericarditis. J Card Surg. 2018 Jun; 33(6): 301-307. https://doi.org/10.1111/jocs.13715 |
| [17] | Nishimura S, Izumi C, Amano M, Imamura S, Onishi N, Tamaki Y, Enomoto S, Miyake M, Tamura T, Kondo H, Kaitani K, Yamanaka K, Nakagawa Y. Long-Term Clinical Outcomes and Prognostic Factors After Pericardiectomy for Constrictive Pericarditis in a Japanese Population. Circ J. 2017 Jan 25; 81(2): 206-212. https://doi.org/10.1253/circj.CJ-16-0633 |
[15-17]
.
In this study, the mean duration of surgery was 3.3 hours. This is in line with other studies conducted so far where a mean duration of pericardiectomy was reported to be around 2.8-3.2 hours (range 1.5-4.5 hours). In addition, the study found that the intraoperative and postoperative rhythm status was abnormal in only one patient (1.5%). The expected intraoperative and postoperative rhythm status during pericardiectomy is usually sinus rhythm. However, some patients may have atrial fibrillation or other arrhythmias. The finding from this study is lower than other studies which reported an intraoperative and postoperative atrial fibrillation in 13-14% of patients had atrial fibrillation and 1-2% of other types of arrhythmias
| [16] | Nozohoor S, Johansson M, Koul B, Cunha-Goncalves D. Radical pericardiectomy for chronic constrictive pericarditis. J Card Surg. 2018 Jun; 33(6): 301-307. https://doi.org/10.1111/jocs.13715 |
| [17] | Nishimura S, Izumi C, Amano M, Imamura S, Onishi N, Tamaki Y, Enomoto S, Miyake M, Tamura T, Kondo H, Kaitani K, Yamanaka K, Nakagawa Y. Long-Term Clinical Outcomes and Prognostic Factors After Pericardiectomy for Constrictive Pericarditis in a Japanese Population. Circ J. 2017 Jan 25; 81(2): 206-212. https://doi.org/10.1253/circj.CJ-16-0633 |
| [18] | Zhu P, Mai M, Wu R, Lu C, Fan R, Zheng S. Pericardiectomy for constrictive pericarditis: single-center experience in China. J Cardiothorac Surg. 2015 Mar 19; 10: 34. https://doi.org/10.1186/s13019-015-0237-6 |
[16-18]
.
Five patients (7.7%) died during the study period. The most common causes of death were cardiac arrest (3 patients) and respiratory arrest (2 patients). There were three complications (4.6%): hypocalcemia (1 patient), atrial fibrillation (1 patient), and acute kidney injury (1 patient). The overall incidence rate of perioperative mortality was 7.9 per 1000 person-days of observation. The overall incidence rate of complications was 4.8 per 1000 person-days of observation. The study found that the majority of patients had a good outcome, with an improvement in symptoms and functional status. The mortality rate was low, and the complication rate was acceptable. These results are consistent with the findings of other studies on pericardiectomy for constrictive pericarditis. Three studies published between 2016 and 2018 which investigated the outcomes of pericardiectomy for constrictive pericarditis showed that pericardiectomy was associated with a low mortality rate (2.5-3.3%) and a moderate complication rate (10.7-13.6%). In the majority of patients, pericardiectomy led to an improvement in symptoms and functional status
| [19] | Choi MS, Jeong DS, Oh JK, Chang SA, Park SJ, Chung S. Long-term results of radical pericardiectomy for constrictive pericarditis in Korean population. J Cardiothorac Surg. 2019 Feb 6; 14(1): 32. https://doi.org/10.1186/s13019-019-0845-7 |
| [20] | Kang SH, Song JM, Kim M, Choo SJ, Chung CH, Kang DH, Song JK. Prognostic predictors in pericardiectomy for chronic constrictive pericarditis. J Thorac Cardiovasc Surg. 2014 Feb; 147(2): 598-605. https://doi.org/10.1016/j.jtcvs.2013.01.022 |
| [21] | Acharya A, Koirala R, Rajbhandari N, Sharma J, Rajbanshi B. Anterior Pericardiectomy for Postinfective Constrictive Pericarditis: Intermediate-Term Outcomes. Ann Thorac Surg. 2018 Oct; 106(4): 1178-1181. https://doi.org/10.1016/j.athoracsur.2018.04.048 |
[19-21]
.
The study's findings are a valuable addition to the existing literature because it addressed a less-studied research question and was conducted in the largest national referral hospital. However, there are some limitations to the study that should be considered when interpreting the findings.
First, because the study was conducted retrospectively and there was insufficient chart recording with limited information on additional exposures, further relevant exposures were not studies. Second, due to the small sample size, further analysis to identify determinants of pericardiectomy outcomes was not possible and thus further generalization of the findings is impossible. Despite these limitations, the study's findings are still valuable and can be used to inform future research on pericardiectomy.
7. Conclusions
These results show that pericardiectomy is a safe and effective treatment for constrictive pericarditis. Most of patients had a good outcome, with an improvement in symptoms and functional status. The mortality rate was low, and the complication rate was acceptable.
However, it is important to note that the study is based on relatively small sample size, and it is a retrospective study from a single center. Hence, further prospective studies are needed to confirm the findings of this study.
Abbreviations
ANOVA | Analysis of Variance |
ALP | Alkaline Phosphates |
ARR | Absolute Relative Risk |
BUN | Blood Urea Nitrogen |
CBP | Cardiopulmonary Bypass |
CVP | Central Venous Pressure |
CXR | Chest x-ray |
COPD | Chronic Obstructive Pulmonary Disease |
CP | Constrictive Pericarditis |
CT | Computed Tomography |
Cr | Creatinine |
CRR | Cumulative Relative Risk |
DM | Diabetes Mellitus |
ECG | Electrocardiogram |
HIV | Human Immunodeficiency Virus |
IRB | Institutional Review Board |
HTN | Hypertension |
MRI | Magnetic Resonance Imaging |
NYHA | New York Heart Association |
Acknowledgments
We would like thank you that assisted in data collection, typing the manuscript and also who advised us on statistical analysis of the result.
Funding
We disclose there is no conflict of interest, no funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Faiza Z, Prakash A, Namburi N, Johnson B, Timsina L, Lee LS. Fifteen-year experience with pericardiectomy at a tertiary referral center. J Cardiothorac Surg. 2021 Jun 22; 16(1): 180.
https://doi.org/10.1186/s13019-021-01561-4
|
| [2] |
George, T. J., Arnaoutakis, G. J., Beaty, C. A., Kilic, A., Baumgartner, W. A., & Conte, J. V. (2012). Contemporary etiologies, risk factors, and outcomes after pericardiectomy. The Annals of thoracic surgery, 94(2), 445–451.
https://doi.org/10.1016/j.athoracsur.2012.03.079
|
| [3] |
Gillaspie EA, Stulak JM, Daly RC, Greason KL, Joyce LD, Oh J, Schaff HV, Dearani JA. A 20-year experience with isolated pericardiectomy: Analysis of indications and outcomes. J Thorac Cardiovasc Surg. 2016 Aug; 152(2): 448-58.
https://doi.org/10.1016/j.jtcvs.2016.03.098
|
| [4] |
DeValeria PA, Baumgartner WA, Casale AS, Greene PS, Cameron DE, Gardner TJ, Gott VL, Watkins L Jr, Reitz BA. Current indications, risks, and outcome after pericardiectomy. Ann Thorac Surg. 1991 Aug; 52(2): 219-24.
https://doi.org/10.1016/0003-4975(91)91339-w
|
| [5] |
Vistarini N, Chen C, Mazine A, Bouchard D, Hebert Y, Carrier M, Cartier R, Demers P, Pellerin M, Perrault LP. Pericardiectomy for Constrictive Pericarditis: 20 Years of Experience at the Montreal Heart Institute. Ann Thorac Surg. 2015 Jul; 100(1): 107-13.
https://doi.org/10.1016/j.athoracsur.2015.02.054
|
| [6] |
Murashita T, Schaff HV, Daly RC, Oh JK, Dearani JA, Stulak JM, King KS, Greason KL. Experience With Pericardiectomy for Constrictive Pericarditis Over Eight Decades. Ann Thorac Surg. 2017 Sep; 104(3): 742-750.
https://doi.org/10.1016/j.athoracsur.2017.05.063
|
| [7] |
Avgerinos D, Rabitnokov Y, Worku B, Neragi-Miandoab S, Girardi LN. Fifteen-year experience and outcomes of pericardiectomy for constrictive pericarditis. J Card Surg. 2014 Jul; 29(4): 434-8.
https://doi.org/10.1111/jocs.12344
|
| [8] |
Miranda WR, Oh JK. Constrictive Pericarditis: A Practical Clinical Approach. Prog Cardiovasc Dis. 2017 Jan-Feb; 59(4): 369-379.
https://doi.org/10.1016/j.pcad.2016.12.008
|
| [9] |
Bertog SC, Thambidorai SK, Parakh K, Schoenhagen P, Ozduran V, Houghtaling PL, Lytle BW, Blackstone EH, Lauer MS, Klein AL. Constrictive pericarditis: etiology and cause-specific survival after pericardiectomy. J Am Coll Cardiol. 2004 Apr 21; 43(8): 1445-52.
https://doi.org/10.1016/j.jacc.2003.11.048
|
| [10] |
Szabó G, Schmack B, Bulut C, Soós P, Weymann A, Stadtfeld S, Karck M. Constrictive pericarditis: risks, aetiologies, and outcomes after total pericardiectomy: 24 years of experience. Eur J Cardiothorac Surg. 2013 Dec; 44(6): 1023-8; discussion 1028.
https://doi.org/10.1093/ejcts/ezt138
|
| [11] |
Busch C, Penov K, Amorim PA, Garbade J, Davierwala P, Schuler GC, Rastan AJ, Mohr FW. Risk factors for mortality after pericardiectomy for chronic constrictive pericarditis in a large single-centre cohort. Eur J Cardiothorac Surg. 2015 Dec; 48(6): e110-6.
https://doi.org/10.1093/ejcts/ezv322
|
| [12] |
Mori M, Mullan CW, Bin Mahmood SU, Yousef S, Pelletier KJ, Mangi AA, Geirsson A. US National Trends in the Management and Outcomes of Constrictive Pericarditis: 2005-2014. Can J Cardiol. 2019 Oct; 35(10): 1394-1399.
https://doi.org/10.1016/j.cjca.2019.05.015
|
| [13] |
Kumawat M, Lahiri TK, Agarwal D. Constrictive pericarditis: retrospective study of 109 patients. Asian Cardiovasc Thorac Ann. 2018 Jun; 26(5): 347-352.
https://doi.org/10.1177/0218492318771490
|
| [14] |
Gatti G, Fiore A, Ternacle J, Porcari A, Fiorica I, Poletti A, Ecarnot F, Bussani R, Pappalardo A, Chocron S, Folliguet T, Perrotti A. Pericardiectomy for constrictive pericarditis: a risk factor analysis for early and late failure. Heart Vessels. 2020 Jan; 35(1): 92-103.
https://doi.org/10.1007/s00380-019-01464-4
|
| [15] |
Biçer M, Özdemir B, Kan İ, Yüksel A, Tok M, Şenkaya I. Long-term outcomes of pericardiectomy for constrictive pericarditis. J Cardiothorac Surg. 2015 Nov 27; 10: 177.
https://doi.org/10.1186/s13019-015-0385-8
|
| [16] |
Nozohoor S, Johansson M, Koul B, Cunha-Goncalves D. Radical pericardiectomy for chronic constrictive pericarditis. J Card Surg. 2018 Jun; 33(6): 301-307.
https://doi.org/10.1111/jocs.13715
|
| [17] |
Nishimura S, Izumi C, Amano M, Imamura S, Onishi N, Tamaki Y, Enomoto S, Miyake M, Tamura T, Kondo H, Kaitani K, Yamanaka K, Nakagawa Y. Long-Term Clinical Outcomes and Prognostic Factors After Pericardiectomy for Constrictive Pericarditis in a Japanese Population. Circ J. 2017 Jan 25; 81(2): 206-212.
https://doi.org/10.1253/circj.CJ-16-0633
|
| [18] |
Zhu P, Mai M, Wu R, Lu C, Fan R, Zheng S. Pericardiectomy for constrictive pericarditis: single-center experience in China. J Cardiothorac Surg. 2015 Mar 19; 10: 34.
https://doi.org/10.1186/s13019-015-0237-6
|
| [19] |
Choi MS, Jeong DS, Oh JK, Chang SA, Park SJ, Chung S. Long-term results of radical pericardiectomy for constrictive pericarditis in Korean population. J Cardiothorac Surg. 2019 Feb 6; 14(1): 32.
https://doi.org/10.1186/s13019-019-0845-7
|
| [20] |
Kang SH, Song JM, Kim M, Choo SJ, Chung CH, Kang DH, Song JK. Prognostic predictors in pericardiectomy for chronic constrictive pericarditis. J Thorac Cardiovasc Surg. 2014 Feb; 147(2): 598-605.
https://doi.org/10.1016/j.jtcvs.2013.01.022
|
| [21] |
Acharya A, Koirala R, Rajbhandari N, Sharma J, Rajbanshi B. Anterior Pericardiectomy for Postinfective Constrictive Pericarditis: Intermediate-Term Outcomes. Ann Thorac Surg. 2018 Oct; 106(4): 1178-1181.
https://doi.org/10.1016/j.athoracsur.2018.04.048
|
| [22] |
Jaiswal LS, Pandit N, Sah B. Surgical treatment of tuberculous chronic constrictive pericarditis: A retrospective observational study from tertiary hospital of eastern Nepal. Indian J Tuberc. 2021 Apr; 68(2): 174-178.
https://doi.org/10.1016/j.ijtb.2020.08.002
|
| [23] |
Fang L, Yu G, Huang J, Zhao W, Ye B. Predictors of postoperative complication and prolonged intensive care unit stay after complete pericardiectomy in tuberculous constrictive pericarditis. J Cardiothorac Surg. 2020 Jun 19; 15(1): 148.
https://doi.org/10.1186/s13019-020-01198-9
|
| [24] |
Adem Ali, H. Biluts, A. Bekele. Thoracic surgical unit, Tikur Anbessa Hospital, Department of Surgery, Medical Faculty, Addis Ababa University, Addis Ababa, Ethiopia Vol. 12 No. 1 (2007).
|
Cite This Article
-
APA Style
F. Senbu, M., Desalegn, A. B., Mideksa, D. T. (2024). Evaluating Pericardiectomy Outcomes and Determinants; an 8-Year Retrospective Study at Tertiary Teaching Hospitals in Ethiopia. International Journal of Cardiovascular and Thoracic Surgery, 10(3), 36-45. https://doi.org/10.11648/j.ijcts.20241003.12
 Copy
|
Copy
|
 Download
Download
ACS Style
F. Senbu, M.; Desalegn, A. B.; Mideksa, D. T. Evaluating Pericardiectomy Outcomes and Determinants; an 8-Year Retrospective Study at Tertiary Teaching Hospitals in Ethiopia. Int. J. Cardiovasc. Thorac. Surg. 2024, 10(3), 36-45. doi: 10.11648/j.ijcts.20241003.12
Copy
|
Download
AMA Style
F. Senbu M, Desalegn AB, Mideksa DT. Evaluating Pericardiectomy Outcomes and Determinants; an 8-Year Retrospective Study at Tertiary Teaching Hospitals in Ethiopia. Int J Cardiovasc Thorac Surg. 2024;10(3):36-45. doi: 10.11648/j.ijcts.20241003.12
Copy
|
Download
-
@article{10.11648/j.ijcts.20241003.12,
author = {Mekonnen F. Senbu and Admikew Bekele Desalegn and Demu Tesfaye Mideksa},
title = {Evaluating Pericardiectomy Outcomes and Determinants; an 8-Year Retrospective Study at Tertiary Teaching Hospitals in Ethiopia
},
journal = {International Journal of Cardiovascular and Thoracic Surgery},
volume = {10},
number = {3},
pages = {36-45},
doi = {10.11648/j.ijcts.20241003.12},
url = {https://doi.org/10.11648/j.ijcts.20241003.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcts.20241003.12},
abstract = {Background: Constrictive pericarditis has a variety of etiologies which leads to severe symptoms and heart failure which affects the quality of life. So far the main modality of treatment is pericardiectomy. Objective: The aim of this research was to know pericardiectomy outcomes and determinants among constrictive pericarditis patients who were operated at Tikur Anbessa Specialized Hospital from 2014 - 2022. Methods: A retrospective study was done among 65 patients. Data was presented using frequencies with percentages, mean (±standard deviation) and/ or median (interquartile range) as required. Perioperative mortality and complications were summarized using incidence density with 95% confidence interval (CI). Result: Most patients were in their 20s (53.8%) and where male are (84.6%). The commonest presenting symptom was shortness of breath (100%), fatiguability (96.9%), and coughs (66.2%). The median time of presentation was 12.3 months (IQR, 7.0-25.5). There were also cases with clinical symptoms of tuberculosis (13.8%). The etiology of constrictive pericarditis was infectious in 83.1% of cases. The mean length of surgery was 3.3 ± 0.6 hours. The median duration of hospital stay is 9.0 days (IQR, 7.0-12.0). The incidence rate (IR) of perioperative death was 7.9 per 1000 person-days (PD) of observation (94% CI = 3.3 – 19.2) and the incidence rate of complication was 4.8 per 1000 PD (95% CI = 1.5 -14.9). Conclusion: Pericardiectomy is the best treatment for patients with constrictive pericarditis. The majority of patients had a good outcome, with an improvement in symptoms and functional status. The mortality rate was low, and the complication rate was acceptable. However, this study is based on relatively small sample size, and it is a retrospective study from a single center. Hence, further prospective studies are needed to confirm the findings of this study.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Evaluating Pericardiectomy Outcomes and Determinants; an 8-Year Retrospective Study at Tertiary Teaching Hospitals in Ethiopia
AU - Mekonnen F. Senbu
AU - Admikew Bekele Desalegn
AU - Demu Tesfaye Mideksa
Y1 - 2024/09/26
PY - 2024
N1 - https://doi.org/10.11648/j.ijcts.20241003.12
DO - 10.11648/j.ijcts.20241003.12
T2 - International Journal of Cardiovascular and Thoracic Surgery
JF - International Journal of Cardiovascular and Thoracic Surgery
JO - International Journal of Cardiovascular and Thoracic Surgery
SP - 36
EP - 45
PB - Science Publishing Group
SN - 2575-4882
UR - https://doi.org/10.11648/j.ijcts.20241003.12
AB - Background: Constrictive pericarditis has a variety of etiologies which leads to severe symptoms and heart failure which affects the quality of life. So far the main modality of treatment is pericardiectomy. Objective: The aim of this research was to know pericardiectomy outcomes and determinants among constrictive pericarditis patients who were operated at Tikur Anbessa Specialized Hospital from 2014 - 2022. Methods: A retrospective study was done among 65 patients. Data was presented using frequencies with percentages, mean (±standard deviation) and/ or median (interquartile range) as required. Perioperative mortality and complications were summarized using incidence density with 95% confidence interval (CI). Result: Most patients were in their 20s (53.8%) and where male are (84.6%). The commonest presenting symptom was shortness of breath (100%), fatiguability (96.9%), and coughs (66.2%). The median time of presentation was 12.3 months (IQR, 7.0-25.5). There were also cases with clinical symptoms of tuberculosis (13.8%). The etiology of constrictive pericarditis was infectious in 83.1% of cases. The mean length of surgery was 3.3 ± 0.6 hours. The median duration of hospital stay is 9.0 days (IQR, 7.0-12.0). The incidence rate (IR) of perioperative death was 7.9 per 1000 person-days (PD) of observation (94% CI = 3.3 – 19.2) and the incidence rate of complication was 4.8 per 1000 PD (95% CI = 1.5 -14.9). Conclusion: Pericardiectomy is the best treatment for patients with constrictive pericarditis. The majority of patients had a good outcome, with an improvement in symptoms and functional status. The mortality rate was low, and the complication rate was acceptable. However, this study is based on relatively small sample size, and it is a retrospective study from a single center. Hence, further prospective studies are needed to confirm the findings of this study.
VL - 10
IS - 3
ER -
Copy
|
Download