Abstract
Cutaneous precancerous lesions represent a heterogeneous group of pathological conditions associated with an increased risk of progression to non-melanoma skin cancers, most commonly cutaneous squamous cell carcinoma (cSCC). They reflect a dynamic process of skin carcinogenesis, characterized by a biological continuum ranging from actinic keratosis (AK) through squamous cell carcinoma in situ to invasive carcinoma. This review summarizes the key clinical features, etiological factors, diagnostic approaches, and current therapeutic strategies for cutaneous precancerous lesions. Chronic ultraviolet (UV) exposure plays a central etiological role, along with genetic predisposition, viral infections, and states of immunosuppression. Actinic keratosis is the most common form and represents an early clinical manifestation within the spectrum of squamous cell carcinogenesis. Diagnosis is primarily based on clinical and dermoscopic evaluation, with histopathological confirmation recommended for suspicious or atypical lesions; however, diagnostic accuracy may be limited by interobserver variability and the absence of reliable biomarkers for predicting lesion progression. Contemporary therapeutic approaches include both lesion-directed and field-directed strategies, reflecting the concept of field cancerization, although the lack of standardized treatment algorithms and limited comparative evidence from large-scale studies remain important challenges. Treatment modalities encompass cryotherapy, topical pharmacological agents, photodynamic therapy, laser ablation, and surgical excision, yet recurrence rates and long-term outcomes vary considerably across modalities. Early diagnosis, individualized treatment, and effective photoprotection are essential for reducing the risk of progression to invasive carcinoma and decreasing the overall burden of non-melanoma skin cancers. Future research should focus on improving risk stratification through the identification of molecular and imaging biomarkers, advancing non-invasive diagnostic technologies, and conducting well-designed prospective trials to establish evidence-based treatment strategies. Additionally, the development of targeted and immunomodulatory therapies, along with strengthened preventive measures, may further optimize patient outcomes.
Keywords
Cutaneous Precancerous Lesions, Actinic Keratosis, Cutaneous Squamous Cell Carcinoma, Field Cancerization, Photocarcinogenesis, Photodynamic Therapy
1. Introduction
Cutaneous precancerous lesions represent a heterogeneous group of pathological conditions associated with an increased risk of developing malignant skin neoplasms, most commonly cutaneous squamous cell carcinoma (cSCC)
. They are considered an intermediate stage in skin carcinogenesis and constitute an important focus of contemporary dermatological and oncological practice
| [3] | Stockfleth E, Peris K, Guillen C, et al. Actinic keratosis and field cancerization. Eur J Dermatol. 2015; 25(4): 293–302. https://doi.org/10.1684/ejd.2015.2599 |
| [4] | Slaughter DP, Southwick HW, Smejkal W. Field cancerization in oral stratified squamous epithelium. Cancer. 1953; 6(5): 963–968.
https://doi.org/10.1002/1097-0142(195309)6:5<963::AID-CNCR2820060515>3.0.CO;2-Q |
| [5] | Braakhuis BJ, Tabor MP, Kummer JA, et al. A genetic explanation of field cancerization. Cancer Res. 2003; 63(8): 1727–1730. |
| [6] | Curtius K, Wright NA, Graham TA. An evolutionary perspective on field cancerization. Nat Rev Cancer. 2018; 18(1): 19–32. https://doi.org/10.1038/nrc.2017.102 |
| [7] | Stockfleth E. Field cancerization: concept and treatment implications. J Eur Acad Dermatol Venereol. 2011; 25(Suppl 1): 2–8.
https://doi.org/10.1111/j.1468-3083.2010.03964.x |
[3, 4-7]
.
In recent decades, the incidence of non-melanoma skin cancers has increased significantly, mainly due to chronic ultraviolet (UV) radiation exposure, population aging, and the rising number of immunosuppressed patients
. In this context, cutaneous precancers are of particular clinical importance, as early recognition and timely treatment can effectively prevent progression to invasive carcinoma
| [1] | Eisen DB, Asgari MM, Bennett DD, et al. Guidelines of care for the management of actinic keratosis. J Am Acad Dermatol. 2021; 85(2): e209–e233.
https://doi.org/10.1016/j.jaad.2021.02.031 |
| [13] | Werner RN, Stockfleth E, Connolly SM, et al. Evidence- and consensus-based (S3) guidelines for the treatment of actinic keratosis. J Eur Acad Dermatol Venereol. 2015; 29(11): 2069–2079. https://doi.org/10.1111/jdv.13180 |
[1, 13]
.
Actinic keratosis (AK) is the most common form of cutaneous precancer and is regarded as an early clinical manifestation within the spectrum of squamous cell carcinogenesis
. Other conditions classified as cutaneous precancers include Bowen’s disease, erythroplasia of Queyrat, chronic radiodermatitis, and chemically induced keratoses
.
Modern diagnostic methods, including dermoscopy and histopathological examination, have significantly improved the early detection of precancerous lesions
| [19] | Lallas A, Zalaudek I, Argenziano G. Dermoscopy in general dermatology. Dermatol Clin. 2013; 31(4): 679–694.
https://doi.org/10.1016/j.det.2013.06.005 |
| [20] | Zalaudek I, Giacomel J, Argenziano G, et al. Dermoscopy of facial nonpigmented actinic keratosis. Br J Dermatol. 2006; 155(5): 951–956.
https://doi.org/10.1111/j.1365-2133.2006.07483.x |
| [21] | Lallas A, Apalla Z, Ioannides D, et al. Dermoscopic patterns of actinic keratosis. J Eur Acad Dermatol Venereol. 2015; 29(9): 1729–1734. https://doi.org/10.1111/jdv.13019 |
| [22] | Bolognia JL, Schaffer JV, Cerroni L. Dermatology. 4th ed. Philadelphia: Elsevier; 2018. |
| [23] | Weedon D. Weedon’s Skin Pathology. 4th ed. London: Elsevier; 2016. |
[19-23]
. In parallel, the development of novel therapeutic approaches, such as photodynamic therapy and topical immunomodulators, has expanded the options for effective treatment and disease control
| [24] | Morton CA, Szeimies RM, Basset-Seguin N, et al. European Dermatology Forum guidelines on topical photodynamic therapy. J Eur Acad Dermatol Venereol. 2019; 33(12): 2225–2238. https://doi.org/10.1111/jdv.15881 |
| [25] | Gupta AK, Paquet M, Villanueva E, et al. Interventions for actinic keratoses. Cochrane Database Syst Rev. 2012; (12): CD004415. https://doi.org/10.1002/14651858.CD004415.pub2 |
| [26] | Jansen MHE, Kessels JPHM, Nelemans PJ, et al. Randomized trial of four treatment approaches for actinic keratosis. N Engl J Med. 2019; 380(10): 935–946.
https://doi.org/10.1056/NEJMoa1811850 |
[24-26]
.
The aim of this review is to summarize current data on the etiology, pathogenesis, clinical manifestations, diagnostic methods, and therapeutic approaches to cutaneous precancers, as well as their role in the prevention of non-melanoma skin cancers.
2. Methods
A narrative literature review was conducted using electronic databases including PubMed, Scopus, and Web of Science. Relevant articles published in English were identified using combinations of keywords such as “cutaneous precancerous lesions,” “actinic keratosis,” “Bowen’s disease,” “squamous cell carcinoma in situ,” “field cancerization,” and “non-melanoma skin cancer.” Additional sources were identified through manual screening of reference lists of selected articles. Priority was given to recent publications, review articles, clinical studies, and established guidelines. Articles were selected based on their relevance to the etiology, pathogenesis, diagnosis, and management of cutaneous precancers.
3. Epidemiology of Cutaneous Precancers
Cutaneous precancers comprise a diverse group of lesions with the potential to progress to non-melanoma skin cancers, most commonly cSCC
. Their prevalence varies considerably depending on geographic latitude, UV intensity, population age structure, skin phototype, and occupational sun exposure
.
AK is the most common form of cutaneous precancer. It occurs significantly more frequently in elderly individuals and in those with chronic sun exposure
. Epidemiological studies indicate that its prevalence in Europe ranges from 11% to 25% among individuals over 60 years of age, with even higher rates reported in specific high-risk groups
| [27] | Schaefer I, Augustin M, Spehr C, et al. Prevalence and risk factors of actinic keratoses in Germany. Br J Dermatol. 2014; 171(2): 389–396. https://doi.org/10.1111/bjd.12933 |
[27]
.
The condition is more commonly observed in individuals with fair skin phototypes (Fitzpatrick types I–II), blond or red hair, and light-colored eyes, which is associated with lower melanin content and reduced photoprotective capacity of the skin
. Chronic immunosuppression represents an additional major risk factor, particularly in organ transplant recipients, in whom the risk of development and progression of precancerous lesions and cSCC is markedly increased
.
Geographic variation also plays an important role. In regions with high levels of solar radiation, such as Australia and the southern United States, the prevalence of AK may reach 40–60% among the adult population
. This highlights the central role of ultraviolet radiation as a key etiological factor in the development of cutaneous precancers
.
4. Etiology of Cutaneous Precancers
The etiology of cutaneous precancers is multifactorial and involves a complex interplay between exogenous carcinogenic factors, genetic predisposition, and immunological mechanisms
. The main risk factors for the development of these lesions include prolonged ultraviolet (UV) exposure, fair skin phototype (Fitzpatrick types I–II), advanced age, occupational sun exposure, immunosuppression, and genetic defects in DNA repair mechanisms
. However, increasing evidence suggests that these factors do not act uniformly, contributing instead to a biologically heterogeneous spectrum of lesions with variable malignant potential.
The most significant etiological factor is chronic UV exposure, particularly within the UVB spectrum (280–320 nm), which induces direct DNA damage in epidermal keratinocytes
. This results in the formation of pyrimidine dimers and characteristic UV-signature mutations affecting key tumor suppressor genes, most notably
TP53, which plays a central role in cell cycle regulation and apoptosis
. In addition to
TP53, recent genomic studies have identified recurrent alterations in genes such as
NOTCH1/2,
CDKN2A, and components of the MAPK and PI3K pathways, supporting a model of early clonal expansion of mutated keratinocytes within sun-damaged skin (recent genomic analyses, 2025–2026)
| [30] | Wang Z, Wang X, Shi Y, Wu S, Ding Y, Yao G, Chen J. Advancements in elucidating the pathogenesis of actinic keratosis: present state and future prospects. Front Med (Lausanne) 9; 11: 1330491.
https://doi.org/10.3389/fmed.2024.1330491 |
| [31] | Li Z, Lu F, Zhou F, Song D, Chang L, Liu W, Yan G and Zhang G (2025) From actinic keratosis to cutaneous squamous cell carcinoma: the key pathogenesis and treatments. Front. Immunol. 16: 1518633.
https://doi.org/10.3389/fimmu.2025.1518633 |
| [32] | De Francesco MA, Salvi M, Gerami R, Alberti M, Cesanelli F, Scarvaglieri I, Tiecco G, Quiros-Roldan E. Actinic Keratosis and Human Papillomaviruses: may their relationship constitute a new approach for actinic keratosis management? Tumour Virus Res. 2025 Dec; 20: 200330. https://doi.org/10.1016/j.tvr.2025.200330 |
[30-32]
. The accumulation of such mutations leads to impaired cellular differentiation and the development of keratinocyte dysplasia, the morphological basis of precancerous changes
| [33] | Pickering CR, Zhou JH, Lee JJ, et al. Mutational landscape of cutaneous squamous cell carcinoma. Nat Genet. 2014; 46(10): 1062–1066. https://doi.org/10.1038/ng.3081 |
| [34] | South AP, Purdie KJ, Watt SA, et al. NOTCH1 mutations occur early during cutaneous squamous cell carcinogenesis. J Invest Dermatol. 2014; 134(10): 2630–2638.
https://doi.org/10.1038/jid.2014.154 |
[33, 34]
.
The concept of field cancerization, first described by D. P. Slaughter et al.
, refers to the presence of genetically altered keratinocytes within clinically normal-appearing skin chronically exposed to UV radiation
. Contemporary molecular data further refine this concept, demonstrating that sun-exposed skin contains multiple competing mutant clones with distinct evolutionary trajectories. Importantly, only a subset of these clones progresses to clinically apparent lesions, highlighting the stochastic and heterogeneous nature of carcinogenesis.
Actinic keratosis (AK), traditionally considered a precursor lesion, is now increasingly viewed within a biological continuum that includes squamous cell carcinoma in situ and invasive cSCC
. However, this linear progression model remains debated. Emerging evidence suggests that some AK lesions may represent early invasive disease ab initio, while others may remain stable or even regress. The risk of malignant transformation is therefore highly variable and lesion-specific, influenced by factors such as lesion thickness, molecular profile, local immune response, and cumulative mutational burden. Recent longitudinal and molecular studies (2025–2026) emphasize that progression risk cannot be reliably predicted based solely on clinical or histopathological features, underscoring significant diagnostic uncertainty.
Fair skin phototype represents an important risk factor, as reduced melanin content is associated with decreased photoprotective capacity against UV radiation
. With advancing age, cumulative UV-induced mutations increase, explaining the higher prevalence of cutaneous precancers in patients over 50–60 years of age
| [27] | Schaefer I, Augustin M, Spehr C, et al. Prevalence and risk factors of actinic keratoses in Germany. Br J Dermatol. 2014; 171(2): 389–396. https://doi.org/10.1111/bjd.12933 |
[27]
. Age-related decline in immune surveillance and the accumulation of senescent cells further contribute to carcinogenic susceptibility, as highlighted in recent immuno-oncological studies.
A particularly high risk is observed in immunosuppressed individuals, including organ transplant recipients. In this population, the incidence of precancerous lesions and cSCC is markedly increased, and lesions are often multiple and demonstrate more rapid progression to invasive neoplasia due to impaired immune surveillance of atypical cells
. Recent data also suggest qualitative differences in tumor biology in these patients, including higher mutational burden and distinct viral–host interactions.
Additional etiological factors include exposure to chemical carcinogens, such as arsenic compounds, which cause direct DNA damage and are associated with the development of arsenical keratoses
. Chronic inflammatory and cicatricial processes (e.g., chronic ulcers, radiation dermatitis, and longstanding scars) also promote sustained cellular regeneration, epigenetic alterations, and mutational accumulation
. Epigenetic dysregulation, including DNA methylation changes and histone modification patterns, has recently been recognized as a key contributor to early keratinocyte transformation (emerging data, 2025).
The role of human papillomavirus (HPV) has also been implicated in the pathogenesis of certain precancerous lesions, particularly in anogenital forms and Bowen’s disease
| [32] | De Francesco MA, Salvi M, Gerami R, Alberti M, Cesanelli F, Scarvaglieri I, Tiecco G, Quiros-Roldan E. Actinic Keratosis and Human Papillomaviruses: may their relationship constitute a new approach for actinic keratosis management? Tumour Virus Res. 2025 Dec; 20: 200330. https://doi.org/10.1016/j.tvr.2025.200330 |
| [37] | Warnakulasuriya S. Actinic cheilitis. Oral Dis. 2009; 15(5): 357–363. https://doi.org/10.1111/j.1601-0825.2009.01548.x |
| [38] | Yu RC, Pryce DW, Macfarlane AW, et al. Cutaneous horns. Br J Dermatol. 1991; 124(5): 449–452.
https://doi.org/10.1111/j.1365-2133.1991.tb00630.x |
[32, 37, 38]
. Oncogenic HPV types induce cellular transformation through the expression of viral oncoproteins that inactivate tumor suppressor proteins p53 and Rb
. Recent studies further suggest a modulatory rather than purely causal role of HPV in cutaneous carcinogenesis, interacting with UV-induced mutagenesis and host immune status.
Genetic defects in DNA repair mechanisms are also of clinical significance. A classic example is xeroderma pigmentosum, in which defects in nucleotide excision repair lead to extreme UV sensitivity and a markedly increased risk of developing precancerous and malignant skin neoplasms
| [22] | Bolognia JL, Schaffer JV, Cerroni L. Dermatology. 4th ed. Philadelphia: Elsevier; 2018. |
[22]
. More broadly, subtle polymorphisms in DNA repair genes and genome stability pathways are increasingly recognized as modifiers of individual susceptibility.
The prolonged action of these factors leads to the development of epidermal keratinocyte dysplasia, characterized by impaired cellular differentiation, nuclear atypia, and increased mitotic activity
| [33] | Pickering CR, Zhou JH, Lee JJ, et al. Mutational landscape of cutaneous squamous cell carcinoma. Nat Genet. 2014; 46(10): 1062–1066. https://doi.org/10.1038/ng.3081 |
| [34] | South AP, Purdie KJ, Watt SA, et al. NOTCH1 mutations occur early during cutaneous squamous cell carcinogenesis. J Invest Dermatol. 2014; 134(10): 2630–2638.
https://doi.org/10.1038/jid.2014.154 |
[33, 34]
. These changes represent the main histopathological substrate of cutaneous precancers and may progressively evolve into squamous cell carcinoma in situ and subsequently into invasive carcinoma
. Nevertheless, the transition from dysplasia to invasive malignancy is neither uniform nor inevitable, reflecting underlying biological heterogeneity and highlighting the need for improved molecular risk stratification.
The key risk factors for the development of cutaneous precancers are summarized in
Table 1.
Table 1. Key risk factors for cutaneous precancers.
Factor / Mechanism | Pathogenetic Role | Molecular / Cellular Effects | Clinical Implications |
Chronic UV Radiation (UVB 280–320 nm) | Principal carcinogenic factor | Induces pyrimidine dimers, DNA photoproducts, and UV-signature mutations (C→T transitions); mutations in TP53, NOTCH1/2, CDKN2A | Initiates keratinocyte dysplasia; drives field cancerization; major risk for AK and cSCC |
Field Cancerization | Clonal expansion of mutated keratinocytes in sun-exposed skin | Multiple genetically distinct clones with variable mutational burden and evolutionary potential | Explains multifocal lesions, recurrence, and variable progression risk |
Genetic Alterations | Early driver events in carcinogenesis | Mutations in tumor suppressor genes (TP53, CDKN2A) and signaling pathways (MAPK, PI3K); genomic instability | Contributes to heterogeneity of lesions and unpredictable malignant transformation |
Epigenetic Dysregulation | Modulates gene expression without DNA sequence changes | DNA methylation changes, histone modification, altered chromatin structure | Influences progression potential and may serve as future biomarkers |
Actinic Keratosis (AK) – Biological Continuum Debate | Intermediate or early malignant lesion | Variable dysplasia; may represent early invasive clones or stable/regressive lesions | Challenges linear progression model; supports lesion heterogeneity and diagnostic uncertainty |
Immunosuppression | Impaired immune surveillance of atypical cells | Reduced T-cell–mediated tumor control; increased viral persistence (e.g., HPV) | Higher incidence, multiplicity, and faster progression to invasive cSCC |
Fair Skin Phototype (Fitzpatrick I–II) | Reduced natural photoprotection | Low melanin → decreased UV absorption and increased DNA damage | Increased susceptibility to UV-induced mutations and precancer formation |
Aging | Cumulative exposure and biological decline | Accumulation of DNA damage, cellular senescence, reduced immune function | Higher prevalence of precancers; increased transformation risk |
Chemical Carcinogens (e.g., arsenic) | Direct genotoxic effects | DNA damage, oxidative stress, altered keratinocyte proliferation | Development of arsenical keratoses and increased malignancy risk |
Chronic Inflammation / Scarring | Sustained regenerative stimulus | Continuous cell turnover, oxidative stress, accumulation of mutations | Promotes malignant transformation in chronic wounds and scars |
Human Papillomavirus (HPV) | Cofactor in carcinogenesis (especially anogenital lesions) | Viral oncoproteins (E6, E7) inhibit p53 and Rb pathways | Enhances carcinogenesis in combination with UV and immunosuppression |
DNA Repair Defects (e.g., xeroderma pigmentosum) | Failure to correct UV-induced DNA damage | Defective nucleotide excision repair → accumulation of mutations | Extremely high risk of early and multiple precancerous and malignant lesions |
Clonal Evolution and Heterogeneity | Non-linear carcinogenesis model | Competing keratinocyte clones with distinct genetic profiles | Explains why only some lesions progress while others regress or remain stable |
5. Pathogenesis of Cutaneous Precancers
Current evidence indicates that the development of cutaneous precancers results from complex molecular and cellular processes involving interactions between genetic mutations, epigenetic alterations, chronic inflammation, and immunological mechanisms
| [6] | Curtius K, Wright NA, Graham TA. An evolutionary perspective on field cancerization. Nat Rev Cancer. 2018; 18(1): 19–32. https://doi.org/10.1038/nrc.2017.102 |
| [29] | Ziegler A, Jonason AS, Leffell DJ, et al. Sunburn and p53 mutations in skin cancer. Nature. 1994; 372(6508): 773–776. https://doi.org/10.1038/372773a0 |
| [30] | Wang Z, Wang X, Shi Y, Wu S, Ding Y, Yao G, Chen J. Advancements in elucidating the pathogenesis of actinic keratosis: present state and future prospects. Front Med (Lausanne) 9; 11: 1330491.
https://doi.org/10.3389/fmed.2024.1330491 |
| [31] | Li Z, Lu F, Zhou F, Song D, Chang L, Liu W, Yan G and Zhang G (2025) From actinic keratosis to cutaneous squamous cell carcinoma: the key pathogenesis and treatments. Front. Immunol. 16: 1518633.
https://doi.org/10.3389/fimmu.2025.1518633 |
[6, 29-31]
.
5.1. Molecular and Genetic Mechanisms
One of the most frequently affected genes in actinic keratosis and other precancerous lesions is
TP53, which encodes the tumor suppressor protein p53
. This protein plays a central role in maintaining genomic stability by regulating the cell cycle, DNA repair, and apoptosis. UV-induced mutations in
TP53 lead to impaired apoptosis and the accumulation of genetically damaged keratinocytes
| [5] | Braakhuis BJ, Tabor MP, Kummer JA, et al. A genetic explanation of field cancerization. Cancer Res. 2003; 63(8): 1727–1730. |
| [28] | Brash DE. UV signature mutations. Photochem Photobiol. 2015; 91(1): 15–26. https://doi.org/10.1111/php.12377 |
| [29] | Ziegler A, Jonason AS, Leffell DJ, et al. Sunburn and p53 mutations in skin cancer. Nature. 1994; 372(6508): 773–776. https://doi.org/10.1038/372773a0 |
[5, 28, 29]
.
In addition to
TP53, mutations have been identified in other genes involved in the regulation of cell proliferation and differentiation, including
NOTCH1,
CDKN2A, as well as genes associated with the RAS/RAF/MAPK signaling pathways
| [30] | Wang Z, Wang X, Shi Y, Wu S, Ding Y, Yao G, Chen J. Advancements in elucidating the pathogenesis of actinic keratosis: present state and future prospects. Front Med (Lausanne) 9; 11: 1330491.
https://doi.org/10.3389/fmed.2024.1330491 |
| [31] | Li Z, Lu F, Zhou F, Song D, Chang L, Liu W, Yan G and Zhang G (2025) From actinic keratosis to cutaneous squamous cell carcinoma: the key pathogenesis and treatments. Front. Immunol. 16: 1518633.
https://doi.org/10.3389/fimmu.2025.1518633 |
[30, 31]
. These molecular alterations contribute to the development of dysplastic changes in the epidermis
| [30] | Wang Z, Wang X, Shi Y, Wu S, Ding Y, Yao G, Chen J. Advancements in elucidating the pathogenesis of actinic keratosis: present state and future prospects. Front Med (Lausanne) 9; 11: 1330491.
https://doi.org/10.3389/fmed.2024.1330491 |
[30]
.
5.2. Role of Chronic UV-Induced Inflammation
Chronic UV-induced inflammation plays a key role in the pathogenesis of cutaneous precancers
. UV radiation stimulates the production of pro-inflammatory mediators, including IL-1, IL-6, TNF-α, and COX-2, which promote cellular proliferation and create a microenvironment conducive to carcinogenesis
.
Persistent inflammation leads to oxidative stress, generation of reactive oxygen species, and additional DNA damage in keratinocytes
| [30] | Wang Z, Wang X, Shi Y, Wu S, Ding Y, Yao G, Chen J. Advancements in elucidating the pathogenesis of actinic keratosis: present state and future prospects. Front Med (Lausanne) 9; 11: 1330491.
https://doi.org/10.3389/fmed.2024.1330491 |
[30]
.
5.3. Immunological Mechanisms
The immune system plays a critical role in controlling transformed keratinocytes
. UV radiation induces local immunosuppression, including a reduction in the number and function of Langerhans cells, thereby impairing immune recognition and elimination of atypical cells
.
In patients with chronic systemic immunosuppression (e.g., organ transplant recipients), this effect is more pronounced, resulting in a markedly increased incidence of actinic keratosis and accelerated progression to cSCC
.
5.4. Epigenetic Alterations
Increasing evidence highlights the role of epigenetic mechanisms in the development of precancerous skin lesions
| [31] | Li Z, Lu F, Zhou F, Song D, Chang L, Liu W, Yan G and Zhang G (2025) From actinic keratosis to cutaneous squamous cell carcinoma: the key pathogenesis and treatments. Front. Immunol. 16: 1518633.
https://doi.org/10.3389/fimmu.2025.1518633 |
[31]
. These include changes in DNA methylation, histone modifications, and dysregulation of microRNA expression, which modulate gene expression without altering the DNA sequence
| [31] | Li Z, Lu F, Zhou F, Song D, Chang L, Liu W, Yan G and Zhang G (2025) From actinic keratosis to cutaneous squamous cell carcinoma: the key pathogenesis and treatments. Front. Immunol. 16: 1518633.
https://doi.org/10.3389/fimmu.2025.1518633 |
[31]
.
These processes contribute to clonal selection and progression of precancerous lesions toward invasive neoplasia.
5.5. Clonal Evolution and Therapeutic Implications
A growing body of evidence supports the concept of clonal evolution in cutaneous precancers, whereby the accumulation of sequential genetic and epigenetic alterations leads to the selection and expansion of cell clones with increased malignant potential
| [6] | Curtius K, Wright NA, Graham TA. An evolutionary perspective on field cancerization. Nat Rev Cancer. 2018; 18(1): 19–32. https://doi.org/10.1038/nrc.2017.102 |
| [30] | Wang Z, Wang X, Shi Y, Wu S, Ding Y, Yao G, Chen J. Advancements in elucidating the pathogenesis of actinic keratosis: present state and future prospects. Front Med (Lausanne) 9; 11: 1330491.
https://doi.org/10.3389/fmed.2024.1330491 |
[6, 30]
. This process underlies the heterogeneity of lesions within the same field of damaged skin and the variable risk of progression to invasive squamous cell carcinoma.
Understanding these mechanisms has direct clinical implications and underlies the use of field-directed therapy, which targets not only clinically visible lesions but also subclinical changes in areas of field cancerization
| [4] | Slaughter DP, Southwick HW, Smejkal W. Field cancerization in oral stratified squamous epithelium. Cancer. 1953; 6(5): 963–968.
https://doi.org/10.1002/1097-0142(195309)6:5<963::AID-CNCR2820060515>3.0.CO;2-Q |
| [24] | Morton CA, Szeimies RM, Basset-Seguin N, et al. European Dermatology Forum guidelines on topical photodynamic therapy. J Eur Acad Dermatol Venereol. 2019; 33(12): 2225–2238. https://doi.org/10.1111/jdv.15881 |
| [25] | Gupta AK, Paquet M, Villanueva E, et al. Interventions for actinic keratoses. Cochrane Database Syst Rev. 2012; (12): CD004415. https://doi.org/10.1002/14651858.CD004415.pub2 |
| [26] | Jansen MHE, Kessels JPHM, Nelemans PJ, et al. Randomized trial of four treatment approaches for actinic keratosis. N Engl J Med. 2019; 380(10): 935–946.
https://doi.org/10.1056/NEJMoa1811850 |
[4, 24-26]
. This approach forms the basis for therapies such as photodynamic therapy and topical immunomodulators, which target broader areas of affected epidermis and reduce the risk of developing new precancerous and malignant lesions
| [24] | Morton CA, Szeimies RM, Basset-Seguin N, et al. European Dermatology Forum guidelines on topical photodynamic therapy. J Eur Acad Dermatol Venereol. 2019; 33(12): 2225–2238. https://doi.org/10.1111/jdv.15881 |
| [25] | Gupta AK, Paquet M, Villanueva E, et al. Interventions for actinic keratoses. Cochrane Database Syst Rev. 2012; (12): CD004415. https://doi.org/10.1002/14651858.CD004415.pub2 |
| [26] | Jansen MHE, Kessels JPHM, Nelemans PJ, et al. Randomized trial of four treatment approaches for actinic keratosis. N Engl J Med. 2019; 380(10): 935–946.
https://doi.org/10.1056/NEJMoa1811850 |
[24-26]
.
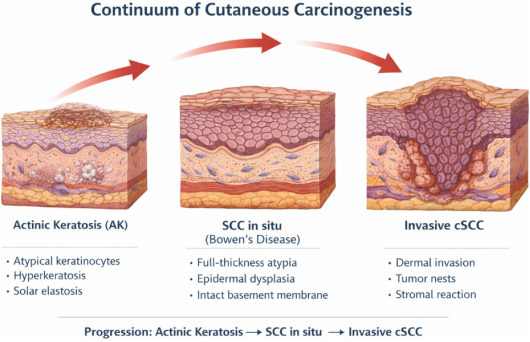
The biological continuum of keratinocyte carcinogenesis, from actinic keratosis to invasive cSCC, is illustrated in
Figure 1.
Figure 1. Biological continuum of keratinocyte carcinogenesis, illustrating the progression from actinic keratosis (AK) to squamous cell carcinoma in situ (Bowen’s disease) and invasive cutaneous squamous cell carcinoma (cSCC).
6. Classification of Cutaneous Precancers
Cutaneous precancers represent a heterogeneous group of lesions associated with an increased risk of developing malignant skin neoplasms, most commonly cSCC
. Traditionally, they are classified into obligate and facultative precancers based on the risk of malignant transformation
| [1] | Eisen DB, Asgari MM, Bennett DD, et al. Guidelines of care for the management of actinic keratosis. J Am Acad Dermatol. 2021; 85(2): e209–e233.
https://doi.org/10.1016/j.jaad.2021.02.031 |
| [13] | Werner RN, Stockfleth E, Connolly SM, et al. Evidence- and consensus-based (S3) guidelines for the treatment of actinic keratosis. J Eur Acad Dermatol Venereol. 2015; 29(11): 2069–2079. https://doi.org/10.1111/jdv.13180 |
[1, 13]
.
This classification is of significant clinical relevance, as it allows estimation of the likelihood of progression to invasive carcinoma and supports the selection of appropriate diagnostic and therapeutic strategies
| [13] | Werner RN, Stockfleth E, Connolly SM, et al. Evidence- and consensus-based (S3) guidelines for the treatment of actinic keratosis. J Eur Acad Dermatol Venereol. 2015; 29(11): 2069–2079. https://doi.org/10.1111/jdv.13180 |
[13]
.
6.1. Obligate Precancers
Obligate precancers are conditions associated with a high risk of malignant transformation and, if left untreated, frequently progress to invasive carcinoma
.
6.1.1. Bowen’s Disease
Bowen’s disease represents an intraepidermal squamous cell carcinoma (squamous cell carcinoma in situ, SCC in situ). Clinically, it presents as well-demarcated erythematous scaly plaques with a slow, progressive course
. Lesions are most commonly located on chronically sun-exposed areas but may also occur on covered skin
.
Histologically, full-thickness epidermal dysplasia is observed without evidence of dermal invasion
.
6.1.2. Erythroplasia of Queyrat
Erythroplasia of Queyrat is a mucocutaneous variant of Bowen’s disease. It is most commonly localized on the glans penis and the inner prepuce
| [23] | Weedon D. Weedon’s Skin Pathology. 4th ed. London: Elsevier; 2016. |
[23]
. Clinically, it appears as a well-demarcated, bright red, velvety plaque.
The condition is associated with infection by oncogenic HPV types and carries a significant risk of progression to invasive squamous cell carcinoma
| [22] | Bolognia JL, Schaffer JV, Cerroni L. Dermatology. 4th ed. Philadelphia: Elsevier; 2018. |
| [23] | Weedon D. Weedon’s Skin Pathology. 4th ed. London: Elsevier; 2016. |
[22, 23]
.
6.1.3. Xeroderma Pigmentosum
Xeroderma pigmentosum is a rare autosomal recessive disorder characterized by defects in nucleotide excision repair of UV-induced DNA damage
| [22] | Bolognia JL, Schaffer JV, Cerroni L. Dermatology. 4th ed. Philadelphia: Elsevier; 2018. |
| [23] | Weedon D. Weedon’s Skin Pathology. 4th ed. London: Elsevier; 2016. |
[22, 23]
.
Affected individuals exhibit marked photosensitivity and have an extremely high risk of developing multiple precancerous and malignant skin neoplasms at an early age.
6.2. Facultative Precancers
Facultative precancers are associated with an increased, but not obligatory, risk of malignant transformation. The likelihood of progression depends on multiple factors, including lesion duration, the patient’s immune status, and the degree of UV exposure
.
6.2.1. Actinic (Solar) Keratosis
AK is the most common form of cutaneous precancer and results from chronic UV-induced damage to keratinocytes
. Clinically, it presents as hyperkeratotic papules or plaques with a rough surface, typically located on chronically sun-exposed areas such as the face, scalp, ears, and dorsal hands
.
AK is considered an early lesion within the spectrum of squamous cell carcinogenesis and may progress to invasive carcinoma
. Current evidence suggests that the boundary between AK and SCC in situ is not sharply defined but rather represents a continuum of keratinocyte carcinogenesis, reflecting the gradual accumulation of genetic and morphological alterations
| [15] | Werner RN, Sammain A, Erdmann R, et al. The natural history of actinic keratosis. Br J Dermatol. 2013; 169(3): 502–518. https://doi.org/10.1111/bjd.12436 |
| [16] | Glogau RG. The risk of progression to invasive disease. J Am Acad Dermatol. 2000; 42(1 Pt 2): 23–24.
https://doi.org/10.1016/S0190-9622(00)90006-6 |
| [30] | Wang Z, Wang X, Shi Y, Wu S, Ding Y, Yao G, Chen J. Advancements in elucidating the pathogenesis of actinic keratosis: present state and future prospects. Front Med (Lausanne) 9; 11: 1330491.
https://doi.org/10.3389/fmed.2024.1330491 |
| [31] | Li Z, Lu F, Zhou F, Song D, Chang L, Liu W, Yan G and Zhang G (2025) From actinic keratosis to cutaneous squamous cell carcinoma: the key pathogenesis and treatments. Front. Immunol. 16: 1518633.
https://doi.org/10.3389/fimmu.2025.1518633 |
[15, 16, 30, 31]
.
6.2.2. Cutaneous Horn
A cutaneous horn is a conical hyperkeratotic projection composed of compact keratin layers
| [22] | Bolognia JL, Schaffer JV, Cerroni L. Dermatology. 4th ed. Philadelphia: Elsevier; 2018. |
| [35] | Ulrich M, Maltusch A, Rius-Diaz F, et al. Reflectance confocal microscopy for actinic keratosis. J Invest Dermatol. 2008; 128(2): 370–377. https://doi.org/10.1038/sj.jid.5701017 |
[22, 35]
. The underlying lesion may vary and includes benign, precancerous, or malignant conditions
| [33] | Pickering CR, Zhou JH, Lee JJ, et al. Mutational landscape of cutaneous squamous cell carcinoma. Nat Genet. 2014; 46(10): 1062–1066. https://doi.org/10.1038/ng.3081 |
[33]
.
In approximately 20–25% of cases, the underlying pathology is precancerous or malignant, which necessitates histopathological examination following excision
| [23] | Weedon D. Weedon’s Skin Pathology. 4th ed. London: Elsevier; 2016. |
[23]
.
6.2.3. Chronic Scars and Ulcers
Chronic scars and ulcers, particularly those resulting from burns, chronic infections, or trauma, may undergo malignant transformation and lead to the development of Marjolin’s ulcer, an aggressive form of cSCC
.
Persistent inflammation, tissue hypoxia, and ongoing cellular regeneration are considered key pathogenic mechanisms in this process
.
The classification and risk of malignant transformation of cutaneous precancers are summarized in
Table 2.
Table 2. Classification and risk of malignant transformation of cutaneous precancers.
Group | Condition | Characteristics | Risk of malignant transformation |
Obligate precancers | Bowen’s disease | Intraepidermal squamous cell carcinoma (SCC in situ) | High |
| Erythroplasia of Queyrat | Mucocutaneous variant of Bowen’s disease associated with HPV | High |
| Xeroderma pigmentosum | Genetic defect in DNA repair (nucleotide excision repair) | Very high |
Facultative precancers | Actinic keratosis | Most common precancer associated with chronic UV exposure | Low to moderate* |
| Cutaneous horn | Hyperkeratotic lesion with variable underlying pathology | Variable |
| Chronic scars and ulcers (Marjolin’s ulcer) | Post-traumatic or post-burn lesions with chronic inflammation | Moderate |
7. Clinical Presentation
The clinical presentation of cutaneous precancers is variable and depends on the type of lesion, its duration, and individual patient characteristics
. The most common findings include hyperkeratotic papules and plaques, erythematous scaly lesions, as well as areas of chronic hyperkeratosis and skin atrophy, typically located on sun-exposed sites
.
AK is the predominant form of cutaneous precancer and is regarded as an early lesion within the spectrum of squamous cell carcinogenesis, including SCC in situ
. Clinically, AK presents as rough, scaly lesions that are often better appreciated by palpation than visual inspection and are frequently described by patients as having a “sandpaper-like” texture (sandpaper sign)
.
AK may occur as solitary lesions or as part of field cancerization, representing areas of chronically photodamaged skin. These fields contain clonally altered keratinocytes with accumulated genetic changes and an increased risk of developing multiple clinical and subclinical precancerous and neoplastic lesions
.
Common anatomical sites include the face, scalp (particularly in patients with androgenetic alopecia), auricles, dorsal hands, forearms, and the lower lip (actinic cheilitis)
. These areas are particularly susceptible to chronic UV exposure and photoaging
.
Several clinical variants of AK have been described, differing in morphology, clinical presentation, and potential for progression to cSCC
.
The main clinical forms of AK are summarized in
Table 3.
Table 3. Clinical variants of actinic keratosis.
Clinical variant | Clinical characteristics | Diagnostic features |
Atrophic | Thin erythematous macules or plaques with minimal hyperkeratosis | Often detected by palpation (sandpaper sign) |
Hyperkeratotic | Thick, rough hyperkeratotic papules or plaques | May resemble early cSCC |
Pigmented | Brown to dark brown macules or plaques | Requires differential diagnosis with lentigo and melanoma |
Lichenoid | Erythematous, infiltrated plaques with inflammatory component | Often associated with pruritus |
Bowenoid | Erythematous scaly plaques resembling Bowen’s disease | Histologically marked atypia |
Actinic cheilitis | Predominantly affects the lower lip | Dryness, scaling, erosions; increased risk of cSCC |
Cutaneous horn | Conical hyperkeratotic projection | Requires histopathological evaluation of the underlying lesion |
8. Dermoscopy of Cutaneous Precancers
Dermoscopy is a key non-invasive diagnostic method that significantly improves the early detection of precancerous and malignant skin lesions
. In AK, it enables visualization of characteristic vascular and keratotic structures that are not visible to the naked eye
.
One of the most characteristic dermoscopic features of facial AK is the so-called
strawberry pattern, which is defined by an erythematous pseudonetwork, follicular openings filled with keratin, and fine linear or coiled vessels
.
Dermoscopy also plays an important role in the differential diagnosis between AK, Bowen’s disease, and early cSCC
.
The dermoscopic features of the main cutaneous precancers are summarized in
Table 4.
Table 4. Dermoscopic features of cutaneous precancers.
Condition | Main dermoscopic features | Diagnostic relevance |
Actinic keratosis | Strawberry pattern; erythematous background; follicular openings with keratin; fine linear/coiled vessels | Typical dermoscopic pattern, especially on the face |
Hyperkeratotic actinic keratosis | Thick keratotic structures; yellowish-white scales | Limited visualization of vascular structures |
Pigmented actinic keratosis | Gray dots; pseudonetwork; irregular pigmentation | May mimic melanoma |
Bowen’s disease | Glomerular vessels clustered on an erythematous background; scales | High diagnostic value for SCC in situ |
Actinic cheilitis | White lines; erosions; irregular vascular structures | Supports early diagnosis of lip lesions |
Cutaneous horn | Compact keratotic masses | Evaluation of the base is critical for diagnosis |
9. Histopathology of Cutaneous Precancers
Histopathological examination represents the gold standard for the definitive diagnosis of cutaneous precancers and is essential for distinguishing them from invasive malignant neoplasms
.
The main histological feature of precancerous lesions is keratinocyte dysplasia, characterized by varying degrees of cellular atypia, disordered differentiation, and increased mitotic activity within the epidermis
.
In AK, partial epidermal dysplasia is observed, predominantly involving the basal and suprabasal layers
. Histological findings include hyperkeratosis, parakeratosis, irregular acanthosis, and atypical keratinocytes. A characteristic feature is solar elastosis in the dermis, reflecting chronic UV-induced damage
. The presence of so-called “skip areas” of dysplasia may also be observed, supporting the concept of field cancerization.
Bowen’s disease is characterized by full-thickness epidermal dysplasia, with atypical keratinocytes involving the entire thickness of the epidermis without invasion through the basement membrane
. Marked cellular pleomorphism, dyskeratosis, and numerous mitotic figures are typically present.
Actinic cheilitis represents a localized form of AK affecting the lip, with histological features including hyperkeratosis, parakeratosis, epidermal dysplasia, and pronounced solar elastosis
| [23] | Weedon D. Weedon’s Skin Pathology. 4th ed. London: Elsevier; 2016. |
| [34] | South AP, Purdie KJ, Watt SA, et al. NOTCH1 mutations occur early during cutaneous squamous cell carcinogenesis. J Invest Dermatol. 2014; 134(10): 2630–2638.
https://doi.org/10.1038/jid.2014.154 |
[23, 34]
.
In cutaneous horn, the histopathological findings depend on the underlying lesion, which may be benign, precancerous, or malignant
. Therefore, histopathological examination of the base of the lesion is mandatory
| [23] | Weedon D. Weedon’s Skin Pathology. 4th ed. London: Elsevier; 2016. |
[23]
.
Chronic scars and ulcers that may give rise to Marjolin’s ulcer demonstrate features of chronic inflammation, fibrosis, and progressive development of squamous cell neoplasia, often with invasive growth and more aggressive clinical behavior
| [23] | Weedon D. Weedon’s Skin Pathology. 4th ed. London: Elsevier; 2016. |
| [36] | Boone M, Suppa M, Dhaenens F, et al. Optical coherence tomography in dermatology. J Biophotonics. 2016; 9(4): 343–352. https://doi.org/10.1002/jbio.201500094 |
[23, 36]
.
Immunohistochemical studies complement histopathological evaluation and aid in distinguishing between different degrees of keratinocyte dysplasia. Aberrant p53 expression is frequently observed and is associated with UV-induced mutations
.
The proliferation marker Ki-67 shows increased expression in dysplastic areas, with its distribution correlating with the degree of dysplasia—restricted to basal layers in AK and more diffuse in Bowen’s disease
.
These markers provide additional diagnostic value, particularly in borderline cases between AK and SCC in situ.
Comparative features of clinical presentation, dermoscopy, and histopathology are summarized in
Table 5.
Table 5. Clinicopathological features of cutaneous precancers.
Condition | Clinical presentation | Dermoscopy | Histopathology |
Actinic keratosis | Rough hyperkeratotic papules on sun-exposed skin | Strawberry pattern; follicular openings with keratin; linear vessels | Partial epidermal dysplasia; parakeratosis; solar elastosis; possible “skip areas” |
Bowen’s disease | Erythematous scaly plaques | Glomerular vessels; scales | Full-thickness epidermal dysplasia without invasion |
Actinic cheilitis | Dryness, scaling, and erosions of the lower lip | White lines; erosions; vascular structures | Epidermal dysplasia and solar elastosis |
Cutaneous horn | Conical hyperkeratotic projection | Dense keratotic masses | Marked hyperkeratosis; findings depend on the underlying lesion (often AK or cSCC) |
Marjolin’s ulcer | Chronic ulcer on a scar | Non-specific vascular structures | Invasive cSCC, often with aggressive behavior |
10. Diagnosis of Cutaneous Precancers
The diagnosis of cutaneous precancers is based on an integrated approach combining clinical examination, dermoscopy, and histopathological evaluation
. This approach enables early detection of precancerous lesions and their differentiation from invasive skin neoplasms
.
10.1. Clinical Examination
Clinical examination represents the first and fundamental step in the diagnostic process. Assessment includes lesion morphology, size and borders, degree of hyperkeratosis, localization on sun-exposed areas, and the presence of multiple lesions in the context of field cancerization
.
Particular attention should be paid to lesions exhibiting rapid growth, ulceration, infiltration, or bleeding, as these features may indicate progression to invasive cSCC
.
10.2. Dermoscopy
Dermoscopy significantly increases diagnostic accuracy in precancerous and early malignant skin lesions
. It allows visualization of structures not visible to the naked eye.
In AK, characteristic findings include the
strawberry pattern, follicular openings filled with keratin, fine linear or coiled vessels, and white or yellowish scales
.
In Bowen’s disease, glomerular vessels clustered on an erythematous background are typically observed, often accompanied by scaling
.
Dermoscopy plays a key role in the differential diagnosis between AK, Bowen’s disease, cSCC, basal cell carcinoma, and melanoma
.
10.3. Biopsy and Histopathological Examination
Histopathological evaluation remains the gold standard for definitive diagnosis
. Biopsy is recommended in the following situations:
1) atypical or rapidly progressive lesions
2) suspicion of invasive carcinoma
3) treatment-resistant lesions
4) clinical or dermoscopic uncertainty
Histological findings include keratinocyte atypia, hyperkeratosis, parakeratosis, disordered epidermal architecture, and solar elastosis as a marker of chronic UV-induced damage
.
10.4. Immunohistochemical Markers
Immunohistochemistry supports diagnosis and provides information on the biological behavior of lesions
. The most commonly used markers include:
1) p53 – indicator of UV-induced mutations
2) Ki-67 – marker of cellular proliferation
3) CK5/6 – marker of squamous differentiation
4) p16 – used in suspected HPV-associated lesions
Increased Ki-67 expression and abnormal p53 expression correlate with the degree of dysplasia and the risk of progression to invasive squamous cell carcinoma
.
10.5. Advanced Non-Invasive Diagnostic Methods
Modern non-invasive techniques enable in vivo visualization of skin structures and are increasingly used in clinical practice
| [32] | De Francesco MA, Salvi M, Gerami R, Alberti M, Cesanelli F, Scarvaglieri I, Tiecco G, Quiros-Roldan E. Actinic Keratosis and Human Papillomaviruses: may their relationship constitute a new approach for actinic keratosis management? Tumour Virus Res. 2025 Dec; 20: 200330. https://doi.org/10.1016/j.tvr.2025.200330 |
| [33] | Pickering CR, Zhou JH, Lee JJ, et al. Mutational landscape of cutaneous squamous cell carcinoma. Nat Genet. 2014; 46(10): 1062–1066. https://doi.org/10.1038/ng.3081 |
[32, 33]
.
10.5.1. Reflectance Confocal Microscopy (RCM)
This method allows near-histological resolution imaging of the epidermis and superficial dermis. In AK, findings include atypical keratinocytes, architectural disorganization, and enlarged nuclei
| [32] | De Francesco MA, Salvi M, Gerami R, Alberti M, Cesanelli F, Scarvaglieri I, Tiecco G, Quiros-Roldan E. Actinic Keratosis and Human Papillomaviruses: may their relationship constitute a new approach for actinic keratosis management? Tumour Virus Res. 2025 Dec; 20: 200330. https://doi.org/10.1016/j.tvr.2025.200330 |
[32]
.
10.5.2. Optical Coherence Tomography (OCT)
OCT provides non-invasive cross-sectional imaging of the skin and facilitates differentiation between precancerous and invasive lesions
| [33] | Pickering CR, Zhou JH, Lee JJ, et al. Mutational landscape of cutaneous squamous cell carcinoma. Nat Genet. 2014; 46(10): 1062–1066. https://doi.org/10.1038/ng.3081 |
[33]
.
These methods are particularly useful for monitoring therapeutic response and detecting subclinical lesions within areas of field cancerization
.
10.5.3. Artificial Intelligence in Dermatology
Artificial intelligence (AI), particularly machine learning and deep learning algorithms, has rapidly emerged as a transformative tool in dermatology, especially in the diagnosis of skin cancers. Recent systematic reviews and meta-analyses demonstrate that convolutional neural network (CNN)-based models can achieve diagnostic accuracy comparable to or exceeding that of non-expert clinicians, with reported sensitivities approaching or exceeding 90% for melanoma detection
| [42] | Salinas, M. P., Sepúlveda, J., Hidalgo, L. et al. A systematic review and meta-analysis of artificial intelligence versus clinicians for skin cancer diagnosis. npj Digit. Med. 7, 125 (2024). https://doi.org/10.1038/s41746-024-01103-x |
[42]
. AI-assisted dermoscopy and total body photography have further enhanced early detection and diagnostic consistency, supporting clinicians in differentiating between benign and malignant lesions
| [43] | Ertürk Zararsız G, Yerlitaş Taştan SI, Çelik Gürbulak E, Erakcaoğlu A, Yılmaz Işıkhan S, Demirbaş A, Ertaş R, Eroğlu İ, Korkmaz S, Elmas ÖF, Zararsız G. Diagnosis melanoma with artificial intelligence systems: A meta-analysis study and systematic review. J Eur Acad Dermatol Venereol. 2025 Nov; 39(11): 1912-1922. https://doi.org/10.1111/jdv.20781 |
[43]
. Moreover, newer AI systems incorporating multimodal data and clinically informed preprocessing show improved performance in distinguishing actinic keratosis from invasive cSCC, addressing a key area of diagnostic uncertainty. However, despite these advances, significant limitations remain, including dataset bias, lack of model interpretability, and challenges in real-world clinical integration, emphasizing that AI should currently be regarded as an adjunct rather than a replacement for clinical expertise.
10.5.4. Molecular Diagnostics in Cutaneous Precancers
Advances in molecular diagnostics have significantly improved the understanding of cutaneous precancerous lesions, revealing a complex genomic landscape characterized by early and heterogeneous mutations. High-throughput sequencing studies have identified recurrent alterations in genes such as
TP53,
NOTCH1/2, and
CDKN2A, as well as dysregulation of key signaling pathways including MAPK and PI3K, supporting the concept of early clonal evolution within sun-damaged skin
| [30] | Wang Z, Wang X, Shi Y, Wu S, Ding Y, Yao G, Chen J. Advancements in elucidating the pathogenesis of actinic keratosis: present state and future prospects. Front Med (Lausanne) 9; 11: 1330491.
https://doi.org/10.3389/fmed.2024.1330491 |
[30]
. Importantly, recent evidence indicates that actinic keratosis represents a biologically heterogeneous entity, with some lesions harboring molecular features similar to invasive cSCC, challenging the traditional linear progression model. Emerging molecular tools, including transcriptomic profiling and epigenetic analysis, offer potential for improved risk stratification and identification of high-risk lesions. Furthermore, the integration of molecular biomarkers with non-invasive imaging techniques may enhance diagnostic precision and guide personalized therapeutic strategies
| [32] | De Francesco MA, Salvi M, Gerami R, Alberti M, Cesanelli F, Scarvaglieri I, Tiecco G, Quiros-Roldan E. Actinic Keratosis and Human Papillomaviruses: may their relationship constitute a new approach for actinic keratosis management? Tumour Virus Res. 2025 Dec; 20: 200330. https://doi.org/10.1016/j.tvr.2025.200330 |
| [40] | Blauvelt A, Kempers S, Lain E, et al. Phase 3 trials of tirbanibulin ointment for actinic keratosis. N Engl J Med. 2021; 384(6): 512–520. https://doi.org/10.1056/NEJMoa2024040 |
[32, 40]
. Despite these advances, the clinical implementation of molecular diagnostics remains limited, and further research is needed to validate biomarkers and standardize their application in routine practice.
11. Differential Diagnosis of Cutaneous Precancers
The differential diagnosis of cutaneous precancers is an essential component of the diagnostic process, as a variety of benign, inflammatory, and malignant skin conditions may mimic their clinical presentation
. In most cases, it is discussed in the context of AK, which is the most common form and a well-established precursor of cSCC
.
Differentiation is based on an integrated assessment of clinical features, dermoscopic findings, and histopathological examination, which remains the gold standard for definitive diagnosis
. The differential diagnostic spectrum includes benign keratoses, inflammatory dermatoses, and malignant skin neoplasms, including melanoma, particularly in pigmented lesions
.
The main conditions included in the differential diagnosis are summarized in
Table 6.
Table 6. Differential diagnosis of cutaneous precancers.
Condition | Clinical characteristics | Distinguishing features |
Seborrheic keratosis | Brownish papules or plaques with a “stuck-on” appearance | Milia-like cysts; comedo-like openings; absence of coarse hyperkeratosis |
Psoriasis | Erythematous scaly plaques | Symmetrical distribution; silvery-white scales |
Discoid lupus erythematosus | Erythematous plaques with atrophy | Follicular hyperkeratosis; scarring |
Porokeratosis | Keratotic plaques with central atrophy | Peripheral keratotic ridge (cornoid lamella) |
Lichen planus | Violaceous, flat-topped papules | Wickham’s striae; intense pruritus |
Basal cell carcinoma | Papule or nodule with pearly border | Telangiectasias; central ulceration; arborizing vessels (dermoscopy) |
Squamous cell carcinoma | Hyperkeratotic, infiltrated plaque or nodule | Rapid growth; infiltration; ulceration |
Bowen’s disease | Erythematous scaly plaque with well-defined borders | Intraepidermal SCC (carcinoma in situ) |
Melanoma (lentigo maligna) | Pigmented lesion with asymmetry | ABCDE criteria; atypical pigment network; rhomboidal structures |
Melanoma in the Differential Diagnosis
Melanoma, particularly lentigo maligna and lentigo maligna melanoma, represents a key differential diagnosis for lesions located on chronically sun-exposed skin, most commonly on the face and scalp
. These lesions may clinically and dermoscopically resemble pigmented AK or Bowen’s disease.
Dermoscopically, melanoma is characterized by asymmetric pigmentation, an atypical pigment network, irregular dots and globules, as well as specific features such as rhomboidal structures and atypical follicular openings
.
In cases of suspected melanoma, biopsy followed by histopathological examination is mandatory, allowing definitive diagnosis and differentiation from precancerous lesions
| [22] | Bolognia JL, Schaffer JV, Cerroni L. Dermatology. 4th ed. Philadelphia: Elsevier; 2018. |
| [23] | Weedon D. Weedon’s Skin Pathology. 4th ed. London: Elsevier; 2016. |
[22, 23]
.
Comparative features of actinic keratosis, Bowen’s disease, cSCC, and melanoma are summarized in
Table 7.
Table 7. Comparative features of cutaneous precancers and malignant skin tumors.
Feature | Actinic keratosis | Bowen’s disease | Squamous cell carcinoma (cSCC) | Melanoma (lentigo maligna) |
Clinical presentation | Rough hyperkeratotic papules/plaques | Erythematous scaly plaque with well-defined borders | Infiltrated plaque or nodule, often ulcerated | Pigmented, asymmetric lesion |
Typical location | Sun-exposed areas (face, scalp, ears, hands) | Trunk and extremities | Sun-exposed areas; chronic wounds | Face (lentigo maligna); trunk |
Growth pattern | Slow | Slow, progressive | Faster, infiltrative | Progressive |
Dermoscopy | Strawberry pattern; follicular openings; fine vessels | Glomerular vessels; scales | Polymorphous vessels; keratotic structures | Atypical pigment network; irregular dots and globules |
Histopathology | Partial epidermal dysplasia; solar elastosis | Full-thickness dysplasia (SCC in situ) | Invasion of atypical keratinocytes into the dermis | Atypical melanocytes with dermal invasion |
Risk of malignancy | Low, cumulative (→ cSCC) | High | Already invasive tumor | High metastatic potential |
Diagnostic standard | Clinical examination + dermoscopy | Biopsy | Biopsy | Biopsy |
The overlap in clinical and dermoscopic features of lesions on chronically sun-exposed skin necessitates careful evaluation and a low threshold for biopsy when malignancy is suspected. The modern diagnostic approach is multimodal, combining clinical assessment, dermoscopy, and histopathological confirmation, which remains decisive for the final diagnosis
.
12. Treatment of Cutaneous Precancers
The therapeutic approach to cutaneous precancers aims to eliminate lesions, limit disease progression, and prevent malignant transformation to invasive cSCC
. Contemporary strategies are based on the concept of field cancerization, in which, in addition to clinically visible lesions, subclinical atypical changes are present in the surrounding photodamaged skin.
In this context, two main therapeutic approaches are distinguished:
1)
lesion-directed therapy – targeting individual clinically visible lesions
| [1] | Eisen DB, Asgari MM, Bennett DD, et al. Guidelines of care for the management of actinic keratosis. J Am Acad Dermatol. 2021; 85(2): e209–e233.
https://doi.org/10.1016/j.jaad.2021.02.031 |
| [13] | Werner RN, Stockfleth E, Connolly SM, et al. Evidence- and consensus-based (S3) guidelines for the treatment of actinic keratosis. J Eur Acad Dermatol Venereol. 2015; 29(11): 2069–2079. https://doi.org/10.1111/jdv.13180 |
| [22] | Bolognia JL, Schaffer JV, Cerroni L. Dermatology. 4th ed. Philadelphia: Elsevier; 2018. |
[1, 13, 22]
;
2)
field-directed therapy – targeting the entire cancerized field to eliminate subclinical changes and reduce the risk of recurrence
.
The choice of therapy depends on the number, location, and characteristics of lesions, as well as the patient’s age, immune status, and overall oncological risk
| [4] | Slaughter DP, Southwick HW, Smejkal W. Field cancerization in oral stratified squamous epithelium. Cancer. 1953; 6(5): 963–968.
https://doi.org/10.1002/1097-0142(195309)6:5<963::AID-CNCR2820060515>3.0.CO;2-Q |
| [16] | Glogau RG. The risk of progression to invasive disease. J Am Acad Dermatol. 2000; 42(1 Pt 2): 23–24.
https://doi.org/10.1016/S0190-9622(00)90006-6 |
| [24] | Morton CA, Szeimies RM, Basset-Seguin N, et al. European Dermatology Forum guidelines on topical photodynamic therapy. J Eur Acad Dermatol Venereol. 2019; 33(12): 2225–2238. https://doi.org/10.1111/jdv.15881 |
| [25] | Gupta AK, Paquet M, Villanueva E, et al. Interventions for actinic keratoses. Cochrane Database Syst Rev. 2012; (12): CD004415. https://doi.org/10.1002/14651858.CD004415.pub2 |
| [26] | Jansen MHE, Kessels JPHM, Nelemans PJ, et al. Randomized trial of four treatment approaches for actinic keratosis. N Engl J Med. 2019; 380(10): 935–946.
https://doi.org/10.1056/NEJMoa1811850 |
[4, 16, 24-26]
.
The main therapeutic modalities are summarized in
Table 8.
Table 8. Therapeutic modalities for cutaneous precancers.
Method | Mechanism of action | Main indications |
Cryotherapy | Tissue destruction by liquid nitrogen freezing | Solitary or limited lesions |
5-fluorouracil (5-FU) | Antimetabolite; inhibits DNA synthesis | Multiple AK; extensive field cancerization |
Imiquimod | TLR-7 agonist → immunomodulation | AK; Bowen’s disease; field therapy |
Tirbanibulin | Inhibits microtubule polymerization and Src kinases → antiproliferative and pro-apoptotic effects | Small treatment fields; short-course therapy |
Photodynamic therapy (PDT) | Photoactivated selective cytotoxicity | Multiple lesions; cosmetically sensitive areas |
Laser therapy | Ablation of superficial skin layers | Superficial precancers |
Surgical excision | Complete removal with histological verification | Suspicion of invasive carcinoma |
Tirbanibulin (tirbanibulin 1% ointment) is a recently introduced therapeutic agent for actinic keratosis that inhibits microtubule polymerization and Src kinase signaling, leading to suppression of cellular proliferation and induction of apoptosis
. Its short treatment course (5 days) is associated with improved patient adherence and a lower incidence of local skin reactions compared to 5-fluorouracil (5-FU) and imiquimod.
5-FU remains one of the most effective therapies for extensive field cancerization, whereas imiquimod has the advantage of inducing a local immune response against atypical keratinocytes
| [1] | Eisen DB, Asgari MM, Bennett DD, et al. Guidelines of care for the management of actinic keratosis. J Am Acad Dermatol. 2021; 85(2): e209–e233.
https://doi.org/10.1016/j.jaad.2021.02.031 |
| [13] | Werner RN, Stockfleth E, Connolly SM, et al. Evidence- and consensus-based (S3) guidelines for the treatment of actinic keratosis. J Eur Acad Dermatol Venereol. 2015; 29(11): 2069–2079. https://doi.org/10.1111/jdv.13180 |
| [26] | Jansen MHE, Kessels JPHM, Nelemans PJ, et al. Randomized trial of four treatment approaches for actinic keratosis. N Engl J Med. 2019; 380(10): 935–946.
https://doi.org/10.1056/NEJMoa1811850 |
[1, 13, 26]
.
Photodynamic therapy (PDT) using 5-aminolevulinic acid (ALA) or methyl aminolevulinate (MAL) is a highly effective modality, particularly for multiple lesions and lesions located in cosmetically sensitive areas, providing excellent cosmetic outcomes
| [1] | Eisen DB, Asgari MM, Bennett DD, et al. Guidelines of care for the management of actinic keratosis. J Am Acad Dermatol. 2021; 85(2): e209–e233.
https://doi.org/10.1016/j.jaad.2021.02.031 |
| [13] | Werner RN, Stockfleth E, Connolly SM, et al. Evidence- and consensus-based (S3) guidelines for the treatment of actinic keratosis. J Eur Acad Dermatol Venereol. 2015; 29(11): 2069–2079. https://doi.org/10.1111/jdv.13180 |
| [22] | Bolognia JL, Schaffer JV, Cerroni L. Dermatology. 4th ed. Philadelphia: Elsevier; 2018. |
| [24] | Morton CA, Szeimies RM, Basset-Seguin N, et al. European Dermatology Forum guidelines on topical photodynamic therapy. J Eur Acad Dermatol Venereol. 2019; 33(12): 2225–2238. https://doi.org/10.1111/jdv.15881 |
[1, 13, 22, 24]
.
The therapeutic approach should always be individualized according to the clinical context.
Recent advances in the understanding of molecular and immunological mechanisms underlying cutaneous precancers have led to the development of novel therapeutic strategies beyond conventional lesion- and field-directed treatments. Immunotherapy, particularly immune checkpoint inhibitors targeting the PD-1/PD-L1 axis (e.g., cemiplimab, pembrolizumab), has demonstrated significant efficacy in advanced cutaneous squamous cell carcinoma and is increasingly being explored for earlier disease stages and even chemopreventive applications in high-risk populations
| [43] | Ertürk Zararsız G, Yerlitaş Taştan SI, Çelik Gürbulak E, Erakcaoğlu A, Yılmaz Işıkhan S, Demirbaş A, Ertaş R, Eroğlu İ, Korkmaz S, Elmas ÖF, Zararsız G. Diagnosis melanoma with artificial intelligence systems: A meta-analysis study and systematic review. J Eur Acad Dermatol Venereol. 2025 Nov; 39(11): 1912-1922. https://doi.org/10.1111/jdv.20781 |
[43]
.
Targeted molecular therapies are also emerging, focusing on key pathways involved in keratinocyte carcinogenesis. Recent studies have identified potential targets such as the
OVOL1/OVOL2–ZEB1 axis, which regulates epithelial–mesenchymal transition, and mutations in genes like
KNSTRN, opening perspectives for gene-targeted interventions and precision medicine approaches. In parallel, advances in nanotechnology-based drug delivery systems, including lipid nanoparticles and nanoformulations, aim to enhance topical drug penetration, increase therapeutic efficacy, and reduce systemic toxicity
| [44] | Persson C, Gupta A. Emerging Combination Therapies Involving Photodynamic Therapy for Basal and Squamous Cell Carcinomas. J Biomed Res Environ Sci. 2025 Jun 16; 6(6): 715-728. https://doi.org/10.37871/jbres2125= |
[44]
.
Additionally, combination therapies—such as topical agents combined with photodynamic therapy or immunomodulators—are being actively investigated to improve clearance rates and address the concept of field cancerization more effectively. Emerging research also highlights the potential role of epigenetic therapies and RNA-based approaches targeting non-coding RNAs and tumor microenvironment interactions, although these remain largely experimental.
Collectively, these innovations reflect a shift toward mechanism-based, personalized treatment strategies, although their routine clinical implementation requires further validation through well-designed prospective studies.
13. Therapeutic Algorithm
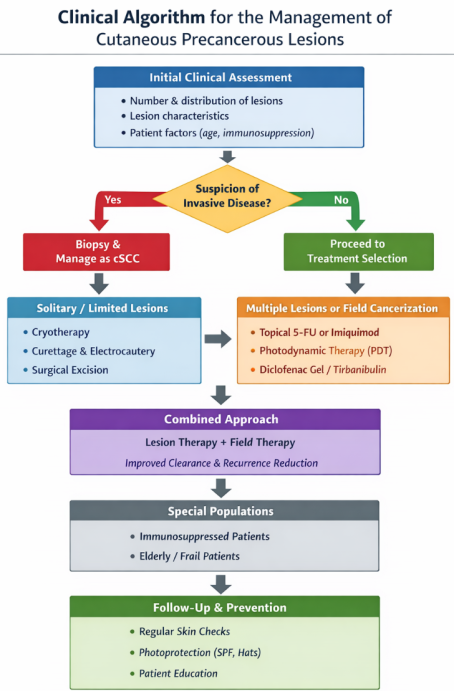
The therapeutic approach to cutaneous precancerous lesions is guided by clinical assessment, particularly lesion number, distribution, and the presence of field cancerization
. For solitary or limited lesions, lesion-directed therapies are preferred. These include cryotherapy, curettage with electrocautery, and surgical excision, all of which aim to achieve complete removal of clinically visible lesions. In contrast, in cases of multiple lesions or when field cancerization is present, field-directed therapies are recommended. These approaches target both clinically apparent and subclinical lesions and include topical agents such as 5-fluorouracil (5-FU) and imiquimod, as well as photodynamic therapy and combination regimens
.
Increasing evidence supports the use of combined treatment strategies, integrating both lesion-directed and field-directed modalities. This approach has demonstrated improved efficacy in reducing subclinical disease burden and lowering recurrence rates compared to monotherapy
.
Figure 2 summarizies a clinical approach for th management of precancerous lesions.
Figure 2. Therapeutic Algorithm.
14. Follow-up and Prevention
Follow-up is an essential component of therapeutic management. Dermatological examinations are recommended at intervals of 3 to 12 months, particularly in patients with multiple lesions or immunosuppression
.
Preventive measures include:
1) strict photoprotection (SPF ≥ 50);
2) limitation of UV exposure;
3) early detection and treatment of new lesions;
4) control of modifiable risk factors
.
15. Prevention and Screening
Prevention of cutaneous precancers can be categorized into primary (reduction of UV exposure), secondary (early detection), and tertiary prevention (monitoring of high-risk patients)
.
15.1. Photoprotection
Photoprotection is a cornerstone of primary prevention. It includes avoidance of direct sun exposure, use of broad-spectrum sunscreens (SPF ≥ 30–50), protective clothing, and avoidance of tanning beds. Regular use has been shown to reduce the incidence of actinic keratosis and the risk of developing cSCC
.
15.2. Early Detection
Screening is based on clinical examination and dermoscopy, which enable early identification of precancerous changes. In suspicious lesions, biopsy followed by histopathological examination is recommended.
15.3. Monitoring of High-Risk Groups
Regular follow-up is necessary for patients with chronic UV exposure, fair skin phototypes (Fitzpatrick I–II), immunosuppression, a history of skin cancer, or multiple actinic keratoses. Recommended follow-up intervals are 6–12 months, with more frequent monitoring in high-risk individuals
.
16. Prognosis and Risk of Malignant Transformation
Cutaneous precancers represent a dynamic spectrum of lesions with the potential to progress to invasive cSCC. AK is regarded as an early intraepidermal neoplasia arising as a result of chronic UV exposure
| [8] | Rogers HW, Weinstock MA, Feldman SR, et al. Incidence estimate of nonmelanoma skin cancer in the United States. JAMA Dermatol. 2015; 151(10): 1081–1086.
https://doi.org/10.1001/jamadermatol.2015.1187 |
| [13] | Werner RN, Stockfleth E, Connolly SM, et al. Evidence- and consensus-based (S3) guidelines for the treatment of actinic keratosis. J Eur Acad Dermatol Venereol. 2015; 29(11): 2069–2079. https://doi.org/10.1111/jdv.13180 |
[8, 13]
.
Current evidence supports the concept of a biological continuum between AK, Bowen’s disease (SCC in situ), and invasive cSCC, driven by the progressive accumulation of genetic and epigenetic alterations
.
The risk of malignant transformation of an individual AK lesion is low but highly variable, ranging from 0.025% to 16% per lesion per year. However, in patients with multiple lesions, the cumulative risk increases substantially, with the incidence of cSCC reaching up to 10–15% over a 10-year period
| [8] | Rogers HW, Weinstock MA, Feldman SR, et al. Incidence estimate of nonmelanoma skin cancer in the United States. JAMA Dermatol. 2015; 151(10): 1081–1086.
https://doi.org/10.1001/jamadermatol.2015.1187 |
| [13] | Werner RN, Stockfleth E, Connolly SM, et al. Evidence- and consensus-based (S3) guidelines for the treatment of actinic keratosis. J Eur Acad Dermatol Venereol. 2015; 29(11): 2069–2079. https://doi.org/10.1111/jdv.13180 |
| [40] | Blauvelt A, Kempers S, Lain E, et al. Phase 3 trials of tirbanibulin ointment for actinic keratosis. N Engl J Med. 2021; 384(6): 512–520. https://doi.org/10.1056/NEJMoa2024040 |
[8, 13, 40]
.
A key role is played by the concept of field cancerization, in which large areas of photodamaged skin harbor genetically altered keratinocytes with increased neoplastic potential. In this context, AK should be considered a clinical marker of increased risk for the development of cSCC.
Major risk factors for malignant transformation include chronic UV exposure, advanced age, fair skin phototype, immunosuppression, a history of skin cancer, the presence of multiple lesions, and localization on severely photodamaged areas
| [8] | Rogers HW, Weinstock MA, Feldman SR, et al. Incidence estimate of nonmelanoma skin cancer in the United States. JAMA Dermatol. 2015; 151(10): 1081–1086.
https://doi.org/10.1001/jamadermatol.2015.1187 |
| [13] | Werner RN, Stockfleth E, Connolly SM, et al. Evidence- and consensus-based (S3) guidelines for the treatment of actinic keratosis. J Eur Acad Dermatol Venereol. 2015; 29(11): 2069–2079. https://doi.org/10.1111/jdv.13180 |
| [16] | Glogau RG. The risk of progression to invasive disease. J Am Acad Dermatol. 2000; 42(1 Pt 2): 23–24.
https://doi.org/10.1016/S0190-9622(00)90006-6 |
| [40] | Blauvelt A, Kempers S, Lain E, et al. Phase 3 trials of tirbanibulin ointment for actinic keratosis. N Engl J Med. 2021; 384(6): 512–520. https://doi.org/10.1056/NEJMoa2024040 |
| [41] | Flohil SC, van der Leest RJ, Arends LR, et al. Risk of subsequent cutaneous malignancy in patients with actinic keratosis. Br J Dermatol. 2013; 168(4): 873–880.
https://doi.org/10.1111/bjd.12245 |
[8, 13, 16, 40, 41]
.
Early diagnosis, appropriate treatment, and regular follow-up are essential for reducing the risk of progression and improving long-term outcomes.
Despite advances in diagnostic and therapeutic approaches, cutaneous precancers remain a significant clinical challenge, underscoring the need for ongoing research aimed at optimizing treatment strategies and improving preventive measures.
17. Conclusion
Cutaneous precancers represent a critical stage in skin carcinogenesis and a significant clinical challenge due to their potential to progress to non-melanoma skin cancers, most commonly cSCC. They reflect a dynamic biological continuum—from actinic keratosis through SCC in situ to invasive carcinoma—driven by the cumulative accumulation of genetic and epigenetic alterations.
Early diagnosis, based on clinical examination, dermoscopy, and histopathology, is essential for timely therapeutic intervention and prevention of malignant transformation. Contemporary therapeutic strategies, grounded in the concept of field cancerization, enable the simultaneous treatment of both clinically visible and subclinical lesions, thereby reducing the risk of recurrence and progression.
Prevention and follow-up play a central role in the long-term management of these patients. Effective photoprotection, active dermatological screening, and an individualized approach in high-risk populations are fundamental for reducing the incidence of cSCC.
An integrated approach—combining early diagnosis, modern therapeutic strategies, and systematic prevention—is crucial for optimal disease control and for reducing the overall burden of non-melanoma skin cancers.
18. Key Points
1) Cutaneous precancers represent a biological continuum from actinic keratosis to invasive cutaneous squamous cell carcinoma (cSCC).
2) Chronic ultraviolet (UV) exposure is the primary etiological factor, driving cumulative genetic and epigenetic alterations in keratinocytes.
3) Early diagnosis based on clinical examination, dermoscopy, and histopathology is essential for preventing malignant transformation.
4) Field cancerization underlies the development of multiple clinical and subclinical lesions, necessitating field-directed therapeutic strategies.
5) An individualized, multimodal approach—combining lesion- and field-directed therapies, photoprotection, and regular follow-up—is critical for optimal disease control and prevention of cSCC.
Abbreviations
cSCC | Cutaneous Squamous Cell Carcinoma |
UV | Ultraviolet Radiation |
AK | Actinic Keratosis |
SCC in situ | Squamous Cell Carcinoma in situ |
HPV | Human Papillomavirus |
PDT | Photodynamic Therapy |
ALA | 5-aminolevulinic Acid |
MAL | Methyl Aminolevulinate |
RCM | Reflectance Confocal Microscopy |
OCT | Optical Coherence Tomography |
CK5/6 | Cytokeratin 5/6 |
Author Contributions
Valentina Broshtilova: Conceptualization, Supervision, Writing – review & editing
Ivan Vasilevski: Data curation, Methodology
Yoanna Velevska: Data curation, Investigation
Irina Yungareva: Data curation, Resources
Yoanna Petkova: Data curation, Validation
Sonya Marina: Supervision, Writing – original draft
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Eisen DB, Asgari MM, Bennett DD, et al. Guidelines of care for the management of actinic keratosis. J Am Acad Dermatol. 2021; 85(2): e209–e233.
https://doi.org/10.1016/j.jaad.2021.02.031
|
| [2] |
Green AC, Olsen CM. Cutaneous squamous cell carcinoma: an epidemiological review. Br J Dermatol. 2017; 177(2): 373–381.
https://doi.org/10.1111/bjd.15324
|
| [3] |
Stockfleth E, Peris K, Guillen C, et al. Actinic keratosis and field cancerization. Eur J Dermatol. 2015; 25(4): 293–302.
https://doi.org/10.1684/ejd.2015.2599
|
| [4] |
Slaughter DP, Southwick HW, Smejkal W. Field cancerization in oral stratified squamous epithelium. Cancer. 1953; 6(5): 963–968.
https://doi.org/10.1002/1097-0142(195309)6:5<963::AID-CNCR2820060515>3.0.CO;2-Q
|
| [5] |
Braakhuis BJ, Tabor MP, Kummer JA, et al. A genetic explanation of field cancerization. Cancer Res. 2003; 63(8): 1727–1730.
|
| [6] |
Curtius K, Wright NA, Graham TA. An evolutionary perspective on field cancerization. Nat Rev Cancer. 2018; 18(1): 19–32.
https://doi.org/10.1038/nrc.2017.102
|
| [7] |
Stockfleth E. Field cancerization: concept and treatment implications. J Eur Acad Dermatol Venereol. 2011; 25(Suppl 1): 2–8.
https://doi.org/10.1111/j.1468-3083.2010.03964.x
|
| [8] |
Rogers HW, Weinstock MA, Feldman SR, et al. Incidence estimate of nonmelanoma skin cancer in the United States. JAMA Dermatol. 2015; 151(10): 1081–1086.
https://doi.org/10.1001/jamadermatol.2015.1187
|
| [9] |
Leiter U, Garbe C. Epidemiology of skin cancer. Adv Exp Med Biol. 2014; 810: 120–140.
https://doi.org/10.1007/978-1-4939-0437-2_7
|
| [10] |
Euvrard S, Kanitakis J, Claudy A. Skin cancers after organ transplantation. N Engl J Med. 2003; 348(17): 1681–1691.
https://doi.org/10.1056/NEJMra022137
|
| [11] |
Narayanan DL, Saladi RN, Fox JL. Ultraviolet radiation and skin cancer. Int J Dermatol. 2010; 49(9): 978–986.
https://doi.org/10.1111/j.1365-4632.2010.04474.x
|
| [12] |
Schmitt JV, Miot HA. Actinic keratosis: a clinical and epidemiological revision. An Bras Dermatol. 2012; 87(3): 425–434.
https://doi.org/10.1590/S0365-05962012000300009
|
| [13] |
Werner RN, Stockfleth E, Connolly SM, et al. Evidence- and consensus-based (S3) guidelines for the treatment of actinic keratosis. J Eur Acad Dermatol Venereol. 2015; 29(11): 2069–2079.
https://doi.org/10.1111/jdv.13180
|
| [14] |
Siegel JA, Korgavkar K, Weinstock MA. Current perspective on actinic keratosis. Br J Dermatol. 2017; 177(2): 350–358.
https://doi.org/10.1111/bjd.14852
|
| [15] |
Werner RN, Sammain A, Erdmann R, et al. The natural history of actinic keratosis. Br J Dermatol. 2013; 169(3): 502–518.
https://doi.org/10.1111/bjd.12436
|
| [16] |
Glogau RG. The risk of progression to invasive disease. J Am Acad Dermatol. 2000; 42(1 Pt 2): 23–24.
https://doi.org/10.1016/S0190-9622(00)90006-6
|
| [17] |
Cox NH, Eedy DJ, Morton CA. Guidelines for management of Bowen's disease. Br J Dermatol. 2007; 156(1): 11–21.
https://doi.org/10.1111/j.1365-2133.2006.07566.x
|
| [18] |
Kossard S, Rosen R. Cutaneous Bowen disease. J Am Acad Dermatol. 1992; 27(3): 406–410.
https://doi.org/10.1016/0190-9622(92)70216-O
|
| [19] |
Lallas A, Zalaudek I, Argenziano G. Dermoscopy in general dermatology. Dermatol Clin. 2013; 31(4): 679–694.
https://doi.org/10.1016/j.det.2013.06.005
|
| [20] |
Zalaudek I, Giacomel J, Argenziano G, et al. Dermoscopy of facial nonpigmented actinic keratosis. Br J Dermatol. 2006; 155(5): 951–956.
https://doi.org/10.1111/j.1365-2133.2006.07483.x
|
| [21] |
Lallas A, Apalla Z, Ioannides D, et al. Dermoscopic patterns of actinic keratosis. J Eur Acad Dermatol Venereol. 2015; 29(9): 1729–1734.
https://doi.org/10.1111/jdv.13019
|
| [22] |
Bolognia JL, Schaffer JV, Cerroni L. Dermatology. 4th ed. Philadelphia: Elsevier; 2018.
|
| [23] |
Weedon D. Weedon’s Skin Pathology. 4th ed. London: Elsevier; 2016.
|
| [24] |
Morton CA, Szeimies RM, Basset-Seguin N, et al. European Dermatology Forum guidelines on topical photodynamic therapy. J Eur Acad Dermatol Venereol. 2019; 33(12): 2225–2238.
https://doi.org/10.1111/jdv.15881
|
| [25] |
Gupta AK, Paquet M, Villanueva E, et al. Interventions for actinic keratoses. Cochrane Database Syst Rev. 2012; (12): CD004415.
https://doi.org/10.1002/14651858.CD004415.pub2
|
| [26] |
Jansen MHE, Kessels JPHM, Nelemans PJ, et al. Randomized trial of four treatment approaches for actinic keratosis. N Engl J Med. 2019; 380(10): 935–946.
https://doi.org/10.1056/NEJMoa1811850
|
| [27] |
Schaefer I, Augustin M, Spehr C, et al. Prevalence and risk factors of actinic keratoses in Germany. Br J Dermatol. 2014; 171(2): 389–396.
https://doi.org/10.1111/bjd.12933
|
| [28] |
Brash DE. UV signature mutations. Photochem Photobiol. 2015; 91(1): 15–26.
https://doi.org/10.1111/php.12377
|
| [29] |
Ziegler A, Jonason AS, Leffell DJ, et al. Sunburn and p53 mutations in skin cancer. Nature. 1994; 372(6508): 773–776.
https://doi.org/10.1038/372773a0
|
| [30] |
Wang Z, Wang X, Shi Y, Wu S, Ding Y, Yao G, Chen J. Advancements in elucidating the pathogenesis of actinic keratosis: present state and future prospects. Front Med (Lausanne) 9; 11: 1330491.
https://doi.org/10.3389/fmed.2024.1330491
|
| [31] |
Li Z, Lu F, Zhou F, Song D, Chang L, Liu W, Yan G and Zhang G (2025) From actinic keratosis to cutaneous squamous cell carcinoma: the key pathogenesis and treatments. Front. Immunol. 16: 1518633.
https://doi.org/10.3389/fimmu.2025.1518633
|
| [32] |
De Francesco MA, Salvi M, Gerami R, Alberti M, Cesanelli F, Scarvaglieri I, Tiecco G, Quiros-Roldan E. Actinic Keratosis and Human Papillomaviruses: may their relationship constitute a new approach for actinic keratosis management? Tumour Virus Res. 2025 Dec; 20: 200330.
https://doi.org/10.1016/j.tvr.2025.200330
|
| [33] |
Pickering CR, Zhou JH, Lee JJ, et al. Mutational landscape of cutaneous squamous cell carcinoma. Nat Genet. 2014; 46(10): 1062–1066.
https://doi.org/10.1038/ng.3081
|
| [34] |
South AP, Purdie KJ, Watt SA, et al. NOTCH1 mutations occur early during cutaneous squamous cell carcinogenesis. J Invest Dermatol. 2014; 134(10): 2630–2638.
https://doi.org/10.1038/jid.2014.154
|
| [35] |
Ulrich M, Maltusch A, Rius-Diaz F, et al. Reflectance confocal microscopy for actinic keratosis. J Invest Dermatol. 2008; 128(2): 370–377.
https://doi.org/10.1038/sj.jid.5701017
|
| [36] |
Boone M, Suppa M, Dhaenens F, et al. Optical coherence tomography in dermatology. J Biophotonics. 2016; 9(4): 343–352.
https://doi.org/10.1002/jbio.201500094
|
| [37] |
Warnakulasuriya S. Actinic cheilitis. Oral Dis. 2009; 15(5): 357–363.
https://doi.org/10.1111/j.1601-0825.2009.01548.x
|
| [38] |
Yu RC, Pryce DW, Macfarlane AW, et al. Cutaneous horns. Br J Dermatol. 1991; 124(5): 449–452.
https://doi.org/10.1111/j.1365-2133.1991.tb00630.x
|
| [39] |
Kerr-Valentic MA, Samimi K, Rohlen BH, et al. Marjolin’s ulcer. Plast Reconstr Surg. 2009; 123(1): 184–191.
https://doi.org/10.1097/PRS.0b013e3181904d86
|
| [40] |
Blauvelt A, Kempers S, Lain E, et al. Phase 3 trials of tirbanibulin ointment for actinic keratosis. N Engl J Med. 2021; 384(6): 512–520.
https://doi.org/10.1056/NEJMoa2024040
|
| [41] |
Flohil SC, van der Leest RJ, Arends LR, et al. Risk of subsequent cutaneous malignancy in patients with actinic keratosis. Br J Dermatol. 2013; 168(4): 873–880.
https://doi.org/10.1111/bjd.12245
|
| [42] |
Salinas, M. P., Sepúlveda, J., Hidalgo, L. et al. A systematic review and meta-analysis of artificial intelligence versus clinicians for skin cancer diagnosis. npj Digit. Med. 7, 125 (2024).
https://doi.org/10.1038/s41746-024-01103-x
|
| [43] |
Ertürk Zararsız G, Yerlitaş Taştan SI, Çelik Gürbulak E, Erakcaoğlu A, Yılmaz Işıkhan S, Demirbaş A, Ertaş R, Eroğlu İ, Korkmaz S, Elmas ÖF, Zararsız G. Diagnosis melanoma with artificial intelligence systems: A meta-analysis study and systematic review. J Eur Acad Dermatol Venereol. 2025 Nov; 39(11): 1912-1922.
https://doi.org/10.1111/jdv.20781
|
| [44] |
Persson C, Gupta A. Emerging Combination Therapies Involving Photodynamic Therapy for Basal and Squamous Cell Carcinomas. J Biomed Res Environ Sci. 2025 Jun 16; 6(6): 715-728.
https://doi.org/10.37871/jbres2125=
|
Cite This Article
-
APA Style
Broshtilova, V., Vasilevski, I., Velevska, Y., Yungareva, I., Petkova, Y., et al. (2026). Cutaneous Precancers: Current Concepts in Etiology, Pathogenesis, Diagnosis, and Management. International Journal of Clinical Dermatology, 9(1), 76-91. https://doi.org/10.11648/j.ijcd.20260901.20
 Copy
|
Copy
|
 Download
Download
ACS Style
Broshtilova, V.; Vasilevski, I.; Velevska, Y.; Yungareva, I.; Petkova, Y., et al. Cutaneous Precancers: Current Concepts in Etiology, Pathogenesis, Diagnosis, and Management. Int. J. Clin. Dermatol. 2026, 9(1), 76-91. doi: 10.11648/j.ijcd.20260901.20
Copy
|
Download
AMA Style
Broshtilova V, Vasilevski I, Velevska Y, Yungareva I, Petkova Y, et al. Cutaneous Precancers: Current Concepts in Etiology, Pathogenesis, Diagnosis, and Management. Int J Clin Dermatol. 2026;9(1):76-91. doi: 10.11648/j.ijcd.20260901.20
Copy
|
Download
-
@article{10.11648/j.ijcd.20260901.20,
author = {Valentina Broshtilova and Ivan Vasilevski and Yoanna Velevska and Irina Yungareva and Yoanna Petkova and Sonya Marina},
title = {Cutaneous Precancers: Current Concepts in Etiology, Pathogenesis, Diagnosis, and Management},
journal = {International Journal of Clinical Dermatology},
volume = {9},
number = {1},
pages = {76-91},
doi = {10.11648/j.ijcd.20260901.20},
url = {https://doi.org/10.11648/j.ijcd.20260901.20},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcd.20260901.20},
abstract = {Cutaneous precancerous lesions represent a heterogeneous group of pathological conditions associated with an increased risk of progression to non-melanoma skin cancers, most commonly cutaneous squamous cell carcinoma (cSCC). They reflect a dynamic process of skin carcinogenesis, characterized by a biological continuum ranging from actinic keratosis (AK) through squamous cell carcinoma in situ to invasive carcinoma. This review summarizes the key clinical features, etiological factors, diagnostic approaches, and current therapeutic strategies for cutaneous precancerous lesions. Chronic ultraviolet (UV) exposure plays a central etiological role, along with genetic predisposition, viral infections, and states of immunosuppression. Actinic keratosis is the most common form and represents an early clinical manifestation within the spectrum of squamous cell carcinogenesis. Diagnosis is primarily based on clinical and dermoscopic evaluation, with histopathological confirmation recommended for suspicious or atypical lesions; however, diagnostic accuracy may be limited by interobserver variability and the absence of reliable biomarkers for predicting lesion progression. Contemporary therapeutic approaches include both lesion-directed and field-directed strategies, reflecting the concept of field cancerization, although the lack of standardized treatment algorithms and limited comparative evidence from large-scale studies remain important challenges. Treatment modalities encompass cryotherapy, topical pharmacological agents, photodynamic therapy, laser ablation, and surgical excision, yet recurrence rates and long-term outcomes vary considerably across modalities. Early diagnosis, individualized treatment, and effective photoprotection are essential for reducing the risk of progression to invasive carcinoma and decreasing the overall burden of non-melanoma skin cancers. Future research should focus on improving risk stratification through the identification of molecular and imaging biomarkers, advancing non-invasive diagnostic technologies, and conducting well-designed prospective trials to establish evidence-based treatment strategies. Additionally, the development of targeted and immunomodulatory therapies, along with strengthened preventive measures, may further optimize patient outcomes.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Cutaneous Precancers: Current Concepts in Etiology, Pathogenesis, Diagnosis, and Management
AU - Valentina Broshtilova
AU - Ivan Vasilevski
AU - Yoanna Velevska
AU - Irina Yungareva
AU - Yoanna Petkova
AU - Sonya Marina
Y1 - 2026/04/25
PY - 2026
N1 - https://doi.org/10.11648/j.ijcd.20260901.20
DO - 10.11648/j.ijcd.20260901.20
T2 - International Journal of Clinical Dermatology
JF - International Journal of Clinical Dermatology
JO - International Journal of Clinical Dermatology
SP - 76
EP - 91
PB - Science Publishing Group
SN - 2995-1305
UR - https://doi.org/10.11648/j.ijcd.20260901.20
AB - Cutaneous precancerous lesions represent a heterogeneous group of pathological conditions associated with an increased risk of progression to non-melanoma skin cancers, most commonly cutaneous squamous cell carcinoma (cSCC). They reflect a dynamic process of skin carcinogenesis, characterized by a biological continuum ranging from actinic keratosis (AK) through squamous cell carcinoma in situ to invasive carcinoma. This review summarizes the key clinical features, etiological factors, diagnostic approaches, and current therapeutic strategies for cutaneous precancerous lesions. Chronic ultraviolet (UV) exposure plays a central etiological role, along with genetic predisposition, viral infections, and states of immunosuppression. Actinic keratosis is the most common form and represents an early clinical manifestation within the spectrum of squamous cell carcinogenesis. Diagnosis is primarily based on clinical and dermoscopic evaluation, with histopathological confirmation recommended for suspicious or atypical lesions; however, diagnostic accuracy may be limited by interobserver variability and the absence of reliable biomarkers for predicting lesion progression. Contemporary therapeutic approaches include both lesion-directed and field-directed strategies, reflecting the concept of field cancerization, although the lack of standardized treatment algorithms and limited comparative evidence from large-scale studies remain important challenges. Treatment modalities encompass cryotherapy, topical pharmacological agents, photodynamic therapy, laser ablation, and surgical excision, yet recurrence rates and long-term outcomes vary considerably across modalities. Early diagnosis, individualized treatment, and effective photoprotection are essential for reducing the risk of progression to invasive carcinoma and decreasing the overall burden of non-melanoma skin cancers. Future research should focus on improving risk stratification through the identification of molecular and imaging biomarkers, advancing non-invasive diagnostic technologies, and conducting well-designed prospective trials to establish evidence-based treatment strategies. Additionally, the development of targeted and immunomodulatory therapies, along with strengthened preventive measures, may further optimize patient outcomes.
VL - 9
IS - 1
ER -
Copy
|
Download