Abstract
This prospective randomized double-blind trial compared the efficacy and safety of 0.3 mg/kg versus 0.5 mg/kg esketamine combined with propofol in 120 young and middle-aged patients (ASA I–II, 20–45 years) undergoing combined gastroscopy and colonoscopy. Participants were randomized to 0.3 mg/kg (Esk0.3, n = 60) or 0.5 mg/kg esketamine (Esk0.5, n = 60). The Esk0.5 group required significantly less propofol (126.1 ± 38.5 mg vs. 154.5 ± 25.8 mg, P < 0.001) and shorter induction time (51.5 ± 8.3 s vs. 58.6 ± 9.1 s, P < 0.001) compared to Esk0.3. However, postoperative recovery time (17.6 ± 4.8 min vs. 13.2 ± 5.8 min, P < 0.001) and operating room exit time (28.7 ± 7.6 min vs. 21.5 ± 4.1 min, P < 0.001) were prolonged in the Esk0.5 group. No differences were observed in procedure duration or patient satisfaction. The Esk0.5 group exhibited higher heart rates at gastroscope withdrawal (83.55 ± 5.34 vs. 80.46 ± 7.45 bpm, P = 0.01), alongside increased adverse events including secretions (13.3% vs. 3.3%, P = 0.037) and diplopia (13.3% vs. 3.3%, P = 0.037). Both groups showed high rates of involuntary twitching (28.3% vs. 35.0%). Esketamine 0.5 mg/kg reduces propofol requirements and accelerates induction but prolongs recovery and increases specific adverse events, necessitating individualized dosing and postoperative monitoring to optimize safety.
Keywords
Esketamine, Propofol, Gastroscopy, Colonoscopy
1. Introduction
With the widespread adoption of painless combined gastroscopy and colonoscopy in diagnosing and managing gastrointestinal diseases, optimizing the balance between anesthesia depth and safety has become a central clinical challenge. Propofol, a widely used sedative, provides rapid induction but exhibits limited analgesic efficacy. Its high-dose administration carries risks of complications such as respiratory depression and hemodynamic instability
| [1] | X. Kong, K. Wang, Y. Wei, B. Sun, G. Gao, C. Song, C. Li, Nonintubated spontaneous ventilation versus intubated mechanical ventilation anesthesia for video-assisted thoracic surgery in terms of perioperative complications and practitioners' workload assessments: a pilot randomized control study, Bmc Anesthesiol. 24(1) (2024) 99, https://doi.org/10.1186/s12871-024-02481-1 |
| [2] | S. C. Jansen, M. van Lemmen, E. Olofsen, L. Moss, J. V. J. Pergolizzi, T. Miller, R. D. Colucci, M. van Velzen, P. Kremer, A. Dahan, R. van der Schrier, M. Niesters, Reversal of propofol-induced depression of the hypoxic ventilatory response by bk-channel blocker ena-001: a randomized controlled trial, Anesthesiology 140(6) (2024) 1076-1087, https://doi.org/10.1097/ALN.0000000000004915 |
[1, 2].
In recent years, esketamine—the S-enantiomer of ketamine—has emerged as a valuable adjunct in perioperative multimodal anesthesia due to its potent
N-methyl-D-aspartate (NMDA) receptor antagonism and reduced neuropsychiatric side effects compared to racemic ketamine
| [3] | L. A. Jelen, A. H. Young, J. M. Stone, Ketamine: a tale of two enantiomers, J. Psychopharmacol. 35(2) (2021) 109-123, https://doi.org/10.1177/0269881120959644 |
| [4] | L. Zhou, L. Lv, R. Wu, W. Mang, L. Hu, Improvement in pain by using lidocaine combined with esketamine in elderly patients receiving local anaesthesia for percutaneous kyphoplasty: a randomized controlled study, Bmc Anesthesiol. 24(1) (2024) 384, https://doi.org/10.1186/s12871-024-02768-3 |
[3, 4]
.
Existing evidence demonstrates that subanesthetic doses of esketamine combined with propofol significantly reduce propofol consumption while preserving hemodynamic stability
| [5] | H. Andersen, [Israel-palestine--zionism and democracy are two incompatible entities], Vardfacket 21(5) (1997) 32. |
| [6] | E. F. Verdu, D. Armstrong, L. Sabovcikova, J. P. Idstrom, C. Cederberg, A. L. Blum, P. Bercik, High concentrations of ammonia, but not volatile amines, in gastric juice of subjects with helicobacter pylori infection, Helicobacter 3(2) (1998) 97-102, https://doi.org/10.1046/j.1523-5378.1998.08068.x |
[5, 6]
. However, dose optimization studies targeting young and middle-aged patients—the primary demographic undergoing gastrointestinal endoscopy—remain limited. Although higher esketamine doses (e.g., 0.5 mg/kg) may theoretically align with the enhanced physiological resilience of this population, concerns persist regarding prolonged recovery times and elevated adverse event rates
| [7] | H. Guo, B. Wang, S. Yuan, S. Wu, J. Liu, M. He, J. Wang, Neurological adverse events associated with esketamine: a disproportionality analysis for signal detection leveraging the fda adverse event reporting system, Front. Pharmacol. 13 (2022) 849758, https://doi.org/10.3389/fphar.2022.849758 |
[7]
. These safety margins and clinical trade-offs remain inadequately characterized.
This study aimed to compare two subanesthetic esketamine regimens (0.3 mg/kg vs. 0.5 mg/kg) during combined gastroscopy and colonoscopy in young and middle-aged patients, evaluating their effects on propofol requirements, hemodynamic stability, post-anesthesia recovery, and adverse event profiles. The findings seek to inform evidence-based anesthesia protocols tailored to this population.
2. Materials and Methods
2.1. Study Participants
This prospective study enrolled 120 patients (age range: 20–45 years; American Society of Anesthesiologists [ASA] physical status I–II) scheduled for elective combined gastroscopy and colonoscopy. Exclusion criteria were as follows: (1) severe underlying diseases (e.g., poorly controlled hypertension, severe ischemic heart disease); (2) allergy to esketamine or its excipients; (3) high risk of hypertension or elevated intracranial pressure; (4) severe mental disorders; (5) untreated or inadequately managed hyperthyroidism; (6) elevated intraocular pressure; and (7) history of substance use disorder.
Participants were randomly allocated to two parallel groups using a computer-generated randomization sequence. Allocation concealment was ensured via sequentially numbered, opaque, sealed envelopes. Prior to the procedure, an independent researcher opened the envelopes, prepared the study drugs, and dispensed them to the anesthesiologists. Anesthesiologists, nurses, and endoscopists remained blinded to group assignments and drug identities. All procedures adhered to standardized protocols.
2.2. Study Protocol
Routine preoperative fasting and fluid restriction were implemented. Oxygen was administered via a face mask at 5 L/min, and vital signs were continuously monitored. An experienced anesthesiologist performed anesthesia induction by slow intravenous injection of esketamine (prepared by an independent researcher, 0.3 mg/kg or 0.5 mg/kg), followed by 2 mg/kg propofol administered over 30 seconds. Endoscopic procedures commenced upon loss of the eyelash reflex. Intraoperatively, supplemental propofol (1 mg/kg) was administered if the Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) score exceeded 3 or if coughing/movement occurred. Postoperatively, patients were transferred immediately to the post-anesthesia care unit (PACU). Consciousness was assessed every 2 minutes; awakening time was recorded when patients demonstrated eye-opening and nodding. PACU discharge criteria required a modified Aldrete score ≥9.
Vital signs were recorded at predefined intervals (T0: Preoperative baseline, T1: Post-induction, T2: Gastroscope insertion, T3: Gastroscope withdrawal, T4: Colonoscope insertion, T5: Ileocecal valve reach, T6: Colonoscopy completion, T7: Consciousness recovery). Adverse events that occur during the operation will be dealt with. For respiratory depression (respiratory rate <10 breaths/min or SpO2 <90%), interventions included mandibular support, placement of an oropharyngeal/nasopharyngeal airway, or positive pressure ventilation. Hypotension (mean arterial pressure <65 mmHg or >20% decrease from baseline) was managed with intravenous metaraminol 0.2 mg. Bradycardia (heart rate <50 beats/min) was treated with intravenous atropine 0.3 mg. All respiratory and cardiovascular adverse events were documented and managed per clinical guidelines.
2.3. Outcome Measures
The primary outcome was total propofol consumption. Secondary outcomes comprised induction time (from study drug injection to loss of eyelash reflex), procedure time (gastroscope insertion to colonoscope withdrawal), recovery time (final drug administration to MOAA/S score of 5), room exit time (last drug injection to modified Aldrete score ≥9), patient satisfaction (assessed post-procedure), vital signs at predefined intervals (T0–T7), and adverse events, including propofol injection pain, bradycardia (heart rate <50 beats/min), respiratory depression (respiratory rate <10 breaths/min or SpO2 <90%), hypotension (mean arterial pressure <65 mmHg or >20% decrease from baseline), hypertension (blood pressure increase >30% from baseline or systolic/diastolic ≥140/90 mmHg), nausea/vomiting, dizziness, coughing, body movement, excessive oral secretions, and antipsychotic-like effects.
2.4. Statistical Analysis
Demographic characteristics were summarized using descriptive statistics. Continuous variables are expressed as mean ± standard deviation, and categorical variables as n (%). The normality of continuous variables was assessed using the Kolmogorov-Smirnov test, with comparisons performed via Student’s t-test. Categorical variables were analyzed using the chi-square test or Fisher’s exact test, as appropriate. A P-value <0.05 was considered statistically significant.
3. Results
3.1. Patient Baseline Characteristics
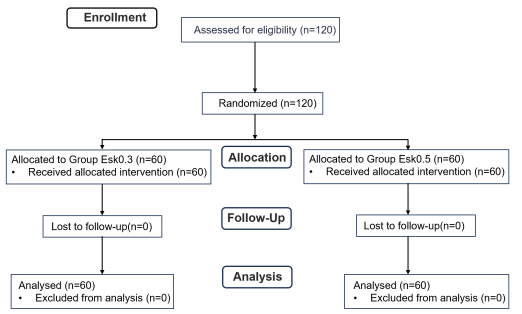
A total of 120 patients meeting the inclusion criteria were randomized into the study groups (
Figure 1). Baseline characteristics of the cohort are summarized in
Table 1. Demographic and clinical parameters, including age, gender, height, weight, body mass index (BMI), ASA classification, and preoperative comorbidities, were comparable between the two groups.
Figure 1. Patient inclusion flow chart.
Table 1. Patient baseline characteristics.
| Group Esk0.3 (n=60) | Group Esk0.5 (n=60) | P value |
Age (year) | 34.51 ± 6.88 | 35.35 ± 7.03 | 0.510 |
Gender (male/female) | 39/21 | 43/17 | 0.432 |
Height (cm) | 165.52 ± 5.77 | 167.48 ± 5.34 | 0.057 |
Weight (kg) | 62.85 ± 4.46 | 64.78 ± 6.29 | 0. 058 |
BMI (kg·m-2) | 22.63 ± 2.45 | 23.39 ± 2.88 | 0.120 |
ASA, I/II | 23/37 | 25/35 | 0.709 |
Hypertension | 10 (16.7%) | 8 (13.3%) | 0.601 |
Diabetes | 3 (5%) | 1 (1.7%) | 0.189 |
Asthma | 0 (0%) | 0 (0%) | 1.000 |
COPD | 0 (0%) | 0 (0%) | 1.000 |
Tachycardia | 5 (8.3%) | 3 (5%) | 0.463 |
Bradycardia | 2 (3.3%) | 1 (1.7%) | 0.576 |
Smoking | 34 (56.7%) | 30 (50%) | 0.467 |
Alcohol Consumption | 20 (33.3%) | 17 (28.3%) | 0.553 |
Motion sickness | 1 (1.7%) | 0 (0%) | 1.000 |
History of surgery | 2 (3.3%) | 1 (1.7%) | 0.576 |
Data are presented as mean ± SD, or number (%).
Abbreviations: BMI, body mass index; ASA, American Society of Anesthesiologists; COPD, chronic obstructive pulmonary disease.
3.2. Propofol Dosage, Perioperative Time Parameters and Patient Satisfaction
Propofol consumption and perioperative time parameters are detailed in
Table 2. The 0.5 mg/kg esketamine group (Esk0.5) demonstrated significantly lower propofol requirements compared to the 0.3 mg/kg group (Esk0.3) (126.1 ± 38.5 mg vs. 154.5 ± 25.8 mg,
P < 0.001) and a shorter induction time (51.5 ± 8.3 s vs. 58.6 ± 9.1 s,
P < 0.001). Conversely, post-anesthesia recovery time (17.6 ± 4.8 min vs. 13.2 ± 5.8 min,
P < 0.001) and operating room discharge time (28.7 ± 7.6 min vs. 21.5 ± 4.1 min,
P < 0.001) were prolonged in the Esk0.5 group. No significant differences were observed in procedure duration (20.3 ± 5.9 min vs. 20.8 ± 4.4 min,
P = 0.599) or patient satisfaction scores (4.2 ± 2.2 vs. 4.7 ± 1.1,
P = 0.118).
Table 2. Propofol dosage, perioperative time parameters and patient satisfaction.
| Group Esk0.3 (n=60) | Group Esk0.5 (n=60) | P value |
Propofol (mg) | 154.5 ± 25.77 | 126.1 ± 38.5 | <0.001 |
Induction time (s) | 58.6 ± 9.1 | 51.5 ± 8.3 | <0.001 |
Procedure time (min) | 20.8 ± 4.4 | 20.3 ± 5.9 | 0.599 |
Recovery time (min) | 13.2 ± 5.8 | 17.6 ± 4.8 | <0.001 |
Room exit time (min) | 21.5 ± 4.1 | 28.7 ± 7.6 | <0.001 |
Patient satisfaction | 4.7 ± 1.1 | 4.2 ± 2.2 | 0.118 |
Data are presented as mean ± SD.
3.3. Vital Signs at Critical Time Points
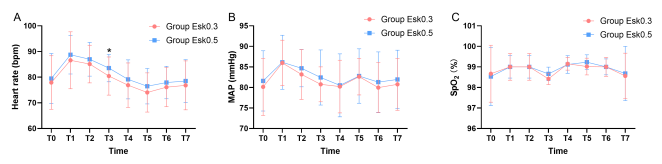
As illustrated in
Figure 2, the group Esk0.5 exhibited a significantly higher heart rate at T3 (80.46 ± 7.45 bpm vs 83.55 ± 5.34 bpm, P = 0.01) compared to the group Esk0.3. No significant intergroup differences in heart rate were observed at other time points (T0, T1, T2, T4, T5, T6, or T7). Similarly, mean arterial pressure (MAP) and SpO
2 remained comparable between groups across all time points (T0–T7).
Two groups are compared: *P<0.05.
Abbreviations: HR, heart rate; MAP, mean arterial pressure; SpO2, oxygen saturation.
3.4. Adverse Events
The group Esk0.5 demonstrated a higher incidence of increased secretions and diplopia compared to the group Esk0.3. However, no significant differences were observed in other adverse events, including injection pain (
Table 3).
Table 3. Adverse events.
| Group Esk0.3 (n=60) | Group Esk0.5 (n=60) | P value |
Injection pain | 13 (21.7%) | 9 (15.0%) | 0.345 |
Bradycardia | 0 (0%) | 0 (0%) | 1.000 |
Hypotension | 3 (5.0%) | 1 (1.7%) | 0.189 |
Hypertension | 0 (0%) | 0 (0%) | 1.000 |
Body movement | 31 (51.7%) | 20 (33.3%) | 0.058 |
Involuntary twitching | 17 (28.3%) | 21 (35.0%) | 0.432 |
Respiratory depressio | 8 (13.3%) | 6 (10.0%) | 0.570 |
Hiccup | 4 (6.7%) | 3 (5.0%) | 0.743 |
Aspiration | 0 (0%) | 0 (0%) | 1.000 |
Nausea and vomiting | 1 (1.7%) | 2 (3.3%) | 0.576 |
Increased secretions | 2 (3.3%) | 8 (13.3%) | 0.037 |
Irritative cough | 9 (15.0%) | 15 (25.0%) | 0.121 |
Diplopia | 2 (3.3%) | 8 (13.3%) | 0.037 |
Agitation | 0 (0%) | 1 (1.7%) | 1.000 |
Lacrimation | 0 (0%) | 0 (0%) | 1.000 |
Nightmare | 0 (0%) | 1 (1.7%) | 1.000 |
Delirium | 0 (0%) | 0 (0%) | 1.000 |
Hallucination | 1 (1.7%) | 1 (1.7%) | 1.000 |
Data are presented as number (%).
4. Discussion
This study represents the first systematic evaluation of the dose-response relationship between 0.3 mg/kg and 0.5 mg/kg esketamine for anesthesia during combined gastroscopy and colonoscopy in young and middle-aged patients. The results indicate that the higher esketamine dose (0.5 mg/kg) significantly reduced propofol requirements by 18.4% and shortened induction time compared to 0.3 mg/kg. However, these benefits were counterbalanced by prolonged post-anesthesia recovery and increased incidence of specific adverse events, underscoring the need for individualized dosing strategies.
The reduced propofol consumption in the 0.5 mg/kg esketamine group (126.1 mg vs. 154.5 mg, P < 0.001) likely stems from esketamine’s synergistic analgesic effects via NMDA receptor antagonism and partial μ-opioid receptor activation. These findings are consistent with previous studies that have demonstrated a reduction in propofol requirements as esketamine doses increase, suggesting a dose-dependent synergistic effect
| [8] | J.M. Miller, Direction of medical care--one physician's view, Md Med J 46(10) (1997) 513. |
| [9] | S. Eberl, L. Koers, J. van Hooft, E. de Jong, J. Hermanides, M.W. Hollmann, B. Preckel, The effectiveness of a low-dose esketamine versus an alfentanil adjunct to propofol sedation during endoscopic retrograde cholangiopancreatography: a randomised controlled multicentre trial, Eur. J. Anaesthesiol. 37(5) (2020) 394-401, https://doi.org/10.1097/EJA.0000000000001134 |
[8, 9]
. Previous studies indicate that esketamine doses below 0.3 mg/kg fail to reduce anesthesia induction time
| [5] | H. Andersen, [Israel-palestine--zionism and democracy are two incompatible entities], Vardfacket 21(5) (1997) 32. |
[5]
. In this trial, the 0.5 mg/kg dose demonstrated a modest reduction in induction time compared to 0.3 mg/kg (51.5 s vs. 58.6 s, P < 0.001). However, the observed 7.1-second difference may lack clinical relevance, suggesting that dose escalation beyond 0.5 mg/kg is unlikely to yield meaningful improvements in this metric. Of concern, the 0.5 mg/kg dose prolonged recovery time (17.6 min vs. 13.2 min, P < 0.001), consistent with observations in broader populations
| [10] | C. Zhang, J. He, Q. Shi, F. Bao, J. Xu, Subanaesthetic dose of esketamine during induction delays anaesthesia recovery a randomized, double-blind clinical trial, Bmc Anesthesiol. 22(1) (2022) 138, https://doi.org/10.1186/s12871-022-01662-0 |
| [11] | H. Yang, Q. Zhao, H. Chen, W. Liu, T. Ding, B. Yang, J. Song, The median effective concentration of propofol with different doses of esketamine during gastrointestinal endoscopy in elderly patients: a randomized controlled trial, Br. J. Clin. Pharmacol. 88(3) (2022) 1279-1287, https://doi.org/10.1111/bcp.15072 |
[10, 11]
. This may reflect accumulation of norketamine—an active metabolite with a >50% longer half-life than esketamine—highlighting the need to consider pharmacokinetic variability at higher doses
| [12] | C. Yang, S. Kobayashi, K. Nakao, C. Dong, M. Han, Y. Qu, Q. Ren, J. Zhang, M. Ma, H. Toki, J. Yamaguchi, S. Chaki, Y. Shirayama, K. Nakazawa, T. Manabe, K. Hashimoto, Ampa receptor activation-independent antidepressant actions of ketamine metabolite (s)-norketamine, Biol. Psychiatry 84(8) (2018) 591-600, https://doi.org/10.1016/j.biopsych.2018.05.007 |
[12]
. While the extended recovery (4.4 min) warrants attention, its clinical relevance requires further evaluation against the benefits of reduced propofol exposure.
Except for a transient elevation in heart rate at T3 in the group Esk0.5, both groups exhibited comparable trends in heart rate, MAP, and SpO
2 across all time points. Perioperative monitoring confirmed the absence of clinically significant bradycardia or hypotension in either group. This hemodynamic stability may arise from esketamine’s dose-dependent sympathomimetic effects—mediated through central vagal inhibition and peripheral catecholamine reuptake blockade—which counteract propofol-induced parasympathetic dominance
| [13] | M. H. Lee, K. Yang, C. S. Lee, H. S. Lee, S. Y. Moon, S. Hwang, J. Song, The effect-site concentration of propofol producing respiratory depression during spinal anesthesia, Korean J. Anesthesiol. 61(2) (2011) 122-126, https://doi.org/10.4097/kjae.2011.61.2.122 |
| [14] | A. F. Schatzberg, Mechanisms of action of ketamine and esketamine, Am. J. Psychiatry. 178(12) (2021) 1130, https://doi.org/10.1176/appi.ajp.2021.21060653 |
[13, 14]
. Furthermore, the synergistic sedative-analgesic properties of esketamine and propofol likely reduced intraoperative propofol rescue doses, thereby mitigating cardiovascular depression
| [15] | L. Zhao, Z. Li, B. Jin, N. Hou, H. Yang, Safety and efficacy of low-dose esketamine in laparoscopic cholecystectomy: a prospective, double-blind randomized controlled trial, Bmc Anesthesiol. 24(1) (2024) 47, https://doi.org/10.1186/s12871-024-02429-5 |
[15]
.
Safety assessments revealed a higher incidence of diplopia and excessive secretions in the the group Esk0.5, consistent with ketamine’s known anticholinergic limitations and transient oculomotor nucleus inhibition. These mechanisms may also contribute to prolonged recovery times observed in this group
| [16] | P. Kawczak, I. Feszak, T. Baczek, Ketamine, esketamine, and arketamine: their mechanisms of action and applications in the treatment of depression and alleviation of depressive symptoms, Biomedicines 12(10) (2024), https://doi.org/10.3390/biomedicines12102283 |
[16]
. Notably, despite dose escalation, esketamine did not increase neuropsychiatric adverse events (e.g., hallucinations or delirium), aligning with prior reports of its favorable psychiatric safety profile at subanesthetic doses
| [11] | H. Yang, Q. Zhao, H. Chen, W. Liu, T. Ding, B. Yang, J. Song, The median effective concentration of propofol with different doses of esketamine during gastrointestinal endoscopy in elderly patients: a randomized controlled trial, Br. J. Clin. Pharmacol. 88(3) (2022) 1279-1287, https://doi.org/10.1111/bcp.15072 |
[11]
.
Notably, we identified a previously unreported adverse event: involuntary twitching occurred in 28.3% and 35.0% of patients in the group Esk0.3 and group Esk0.5, respectively, despite adequate sedation depth (Supplementary Video). These movements, potentially disruptive to endoscopic procedures, may arise from incomplete NMDA receptor antagonism by esketamine, leading to dysregulated neuronal excitability in specific brain regions. Interindividual variability in esketamine metabolism, genetic polymorphisms affecting receptor sensitivity, or preexisting neurological conditions could further predispose patients to such motor phenomena. While mechanistic clarity remains elusive, these observations underscore the need for cautious esketamine use in gastrointestinal endoscopy until the safety implications of involuntary twitching are fully elucidated.
This study has several limitations. First, the exclusion of ASA class III patients or those with severe metabolic syndromes limits generalizability to broader populations. Second, the absence of bispectral index or nociceptive response monitoring precluded objective quantification of anesthesia depth relative to procedural stimuli.
5. Conclusions
0.5 mg/kg esketamine can effectively reduce the dosage of propofol and accelerate induction, but the prolonged recovery period and the risk of adverse reactions need to be weighed. It is recommended to implement individualized dosage strategies based on the patient's physiological characteristics and the requirements of the operation, while strengthening postoperative neurological function monitoring to optimize safety.
Abbreviations
NMDA | N-methyl-D-aspartate |
ASA | American Society of Anesthesiologists |
MOAA/S | Modified Observer’s Assessment of Alertness/Sedation |
PACU | Post-anesthesia Care Unit |
COPD | Chronic Obstructive Pulmonary Disease |
HR | Heart Rate |
MAP | Mean Arterial Pressure |
SpO2 | Oxygen Saturation |
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Deyang People’s Hospital (Approval No. 2022-04-024). Written informed consent was obtained from all participants following a detailed explanation of study procedures and potential risks. Patient confidentiality was maintained through anonymized data management compliant with China’s Personal Information Protection Law.
Author Contributions
Jia Han: Project administration, Funding acquisition
Xian-Jie Zhang: Conceptualization, Methodology
Wen-Hu Zhai: Investigation
Jian-Sheng Luo: Funding acquisition, Writing- review & editing
Yu-Hang Shou: Investigation, Writing-original draft
Funding
This work is supported by Deyang People’s Hospital (Grant No. FHT202402), Deyang City Science and Technology Bureau (Grant No. 2024SZY013), Sichuan Provincial Association of Chinese Medicine Information (Grant No. 20210111), and Sichuan Provincial Association of Chinese Medicine Information (Grant No. 20210107).
Data Availability Statement
The data analyzed during this study can be obtained from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
X. Kong, K. Wang, Y. Wei, B. Sun, G. Gao, C. Song, C. Li, Nonintubated spontaneous ventilation versus intubated mechanical ventilation anesthesia for video-assisted thoracic surgery in terms of perioperative complications and practitioners' workload assessments: a pilot randomized control study, Bmc Anesthesiol. 24(1) (2024) 99,
https://doi.org/10.1186/s12871-024-02481-1
|
| [2] |
S. C. Jansen, M. van Lemmen, E. Olofsen, L. Moss, J. V. J. Pergolizzi, T. Miller, R. D. Colucci, M. van Velzen, P. Kremer, A. Dahan, R. van der Schrier, M. Niesters, Reversal of propofol-induced depression of the hypoxic ventilatory response by bk-channel blocker ena-001: a randomized controlled trial, Anesthesiology 140(6) (2024) 1076-1087,
https://doi.org/10.1097/ALN.0000000000004915
|
| [3] |
L. A. Jelen, A. H. Young, J. M. Stone, Ketamine: a tale of two enantiomers, J. Psychopharmacol. 35(2) (2021) 109-123,
https://doi.org/10.1177/0269881120959644
|
| [4] |
L. Zhou, L. Lv, R. Wu, W. Mang, L. Hu, Improvement in pain by using lidocaine combined with esketamine in elderly patients receiving local anaesthesia for percutaneous kyphoplasty: a randomized controlled study, Bmc Anesthesiol. 24(1) (2024) 384,
https://doi.org/10.1186/s12871-024-02768-3
|
| [5] |
H. Andersen, [Israel-palestine--zionism and democracy are two incompatible entities], Vardfacket 21(5) (1997) 32.
|
| [6] |
E. F. Verdu, D. Armstrong, L. Sabovcikova, J. P. Idstrom, C. Cederberg, A. L. Blum, P. Bercik, High concentrations of ammonia, but not volatile amines, in gastric juice of subjects with helicobacter pylori infection, Helicobacter 3(2) (1998) 97-102,
https://doi.org/10.1046/j.1523-5378.1998.08068.x
|
| [7] |
H. Guo, B. Wang, S. Yuan, S. Wu, J. Liu, M. He, J. Wang, Neurological adverse events associated with esketamine: a disproportionality analysis for signal detection leveraging the fda adverse event reporting system, Front. Pharmacol. 13 (2022) 849758,
https://doi.org/10.3389/fphar.2022.849758
|
| [8] |
J.M. Miller, Direction of medical care--one physician's view, Md Med J 46(10) (1997) 513.
|
| [9] |
S. Eberl, L. Koers, J. van Hooft, E. de Jong, J. Hermanides, M.W. Hollmann, B. Preckel, The effectiveness of a low-dose esketamine versus an alfentanil adjunct to propofol sedation during endoscopic retrograde cholangiopancreatography: a randomised controlled multicentre trial, Eur. J. Anaesthesiol. 37(5) (2020) 394-401,
https://doi.org/10.1097/EJA.0000000000001134
|
| [10] |
C. Zhang, J. He, Q. Shi, F. Bao, J. Xu, Subanaesthetic dose of esketamine during induction delays anaesthesia recovery a randomized, double-blind clinical trial, Bmc Anesthesiol. 22(1) (2022) 138,
https://doi.org/10.1186/s12871-022-01662-0
|
| [11] |
H. Yang, Q. Zhao, H. Chen, W. Liu, T. Ding, B. Yang, J. Song, The median effective concentration of propofol with different doses of esketamine during gastrointestinal endoscopy in elderly patients: a randomized controlled trial, Br. J. Clin. Pharmacol. 88(3) (2022) 1279-1287,
https://doi.org/10.1111/bcp.15072
|
| [12] |
C. Yang, S. Kobayashi, K. Nakao, C. Dong, M. Han, Y. Qu, Q. Ren, J. Zhang, M. Ma, H. Toki, J. Yamaguchi, S. Chaki, Y. Shirayama, K. Nakazawa, T. Manabe, K. Hashimoto, Ampa receptor activation-independent antidepressant actions of ketamine metabolite (s)-norketamine, Biol. Psychiatry 84(8) (2018) 591-600,
https://doi.org/10.1016/j.biopsych.2018.05.007
|
| [13] |
M. H. Lee, K. Yang, C. S. Lee, H. S. Lee, S. Y. Moon, S. Hwang, J. Song, The effect-site concentration of propofol producing respiratory depression during spinal anesthesia, Korean J. Anesthesiol. 61(2) (2011) 122-126,
https://doi.org/10.4097/kjae.2011.61.2.122
|
| [14] |
A. F. Schatzberg, Mechanisms of action of ketamine and esketamine, Am. J. Psychiatry. 178(12) (2021) 1130,
https://doi.org/10.1176/appi.ajp.2021.21060653
|
| [15] |
L. Zhao, Z. Li, B. Jin, N. Hou, H. Yang, Safety and efficacy of low-dose esketamine in laparoscopic cholecystectomy: a prospective, double-blind randomized controlled trial, Bmc Anesthesiol. 24(1) (2024) 47,
https://doi.org/10.1186/s12871-024-02429-5
|
| [16] |
P. Kawczak, I. Feszak, T. Baczek, Ketamine, esketamine, and arketamine: their mechanisms of action and applications in the treatment of depression and alleviation of depressive symptoms, Biomedicines 12(10) (2024),
https://doi.org/10.3390/biomedicines12102283
|
Cite This Article
-
APA Style
Shou, Y., Luo, J., Zhai, W., Zhang, X., Han, J. (2025). Efficacy and Safety of Different Esketamine Doses Combined with Propofol in Gastrointestinal Endoscopy. International Journal of Anesthesia and Clinical Medicine, 13(1), 30-36. https://doi.org/10.11648/j.ijacm.20251301.15
 Copy
|
Copy
|
 Download
Download
ACS Style
Shou, Y.; Luo, J.; Zhai, W.; Zhang, X.; Han, J. Efficacy and Safety of Different Esketamine Doses Combined with Propofol in Gastrointestinal Endoscopy. Int. J. Anesth. Clin. Med. 2025, 13(1), 30-36. doi: 10.11648/j.ijacm.20251301.15
Copy
|
Download
AMA Style
Shou Y, Luo J, Zhai W, Zhang X, Han J. Efficacy and Safety of Different Esketamine Doses Combined with Propofol in Gastrointestinal Endoscopy. Int J Anesth Clin Med. 2025;13(1):30-36. doi: 10.11648/j.ijacm.20251301.15
Copy
|
Download
-
@article{10.11648/j.ijacm.20251301.15,
author = {Yu-Hang Shou and Jian-Sheng Luo and Wen-Hu Zhai and Xian-Jie Zhang and Jia Han},
title = {Efficacy and Safety of Different Esketamine Doses Combined with Propofol in Gastrointestinal Endoscopy
},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {13},
number = {1},
pages = {30-36},
doi = {10.11648/j.ijacm.20251301.15},
url = {https://doi.org/10.11648/j.ijacm.20251301.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20251301.15},
abstract = {This prospective randomized double-blind trial compared the efficacy and safety of 0.3 mg/kg versus 0.5 mg/kg esketamine combined with propofol in 120 young and middle-aged patients (ASA I–II, 20–45 years) undergoing combined gastroscopy and colonoscopy. Participants were randomized to 0.3 mg/kg (Esk0.3, n = 60) or 0.5 mg/kg esketamine (Esk0.5, n = 60). The Esk0.5 group required significantly less propofol (126.1 ± 38.5 mg vs. 154.5 ± 25.8 mg, P P P < 0.001) were prolonged in the Esk0.5 group. No differences were observed in procedure duration or patient satisfaction. The Esk0.5 group exhibited higher heart rates at gastroscope withdrawal (83.55 ± 5.34 vs. 80.46 ± 7.45 bpm, P = 0.01), alongside increased adverse events including secretions (13.3% vs. 3.3%, P = 0.037) and diplopia (13.3% vs. 3.3%, P = 0.037). Both groups showed high rates of involuntary twitching (28.3% vs. 35.0%). Esketamine 0.5 mg/kg reduces propofol requirements and accelerates induction but prolongs recovery and increases specific adverse events, necessitating individualized dosing and postoperative monitoring to optimize safety.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Efficacy and Safety of Different Esketamine Doses Combined with Propofol in Gastrointestinal Endoscopy
AU - Yu-Hang Shou
AU - Jian-Sheng Luo
AU - Wen-Hu Zhai
AU - Xian-Jie Zhang
AU - Jia Han
Y1 - 2025/04/22
PY - 2025
N1 - https://doi.org/10.11648/j.ijacm.20251301.15
DO - 10.11648/j.ijacm.20251301.15
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 30
EP - 36
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20251301.15
AB - This prospective randomized double-blind trial compared the efficacy and safety of 0.3 mg/kg versus 0.5 mg/kg esketamine combined with propofol in 120 young and middle-aged patients (ASA I–II, 20–45 years) undergoing combined gastroscopy and colonoscopy. Participants were randomized to 0.3 mg/kg (Esk0.3, n = 60) or 0.5 mg/kg esketamine (Esk0.5, n = 60). The Esk0.5 group required significantly less propofol (126.1 ± 38.5 mg vs. 154.5 ± 25.8 mg, P P P < 0.001) were prolonged in the Esk0.5 group. No differences were observed in procedure duration or patient satisfaction. The Esk0.5 group exhibited higher heart rates at gastroscope withdrawal (83.55 ± 5.34 vs. 80.46 ± 7.45 bpm, P = 0.01), alongside increased adverse events including secretions (13.3% vs. 3.3%, P = 0.037) and diplopia (13.3% vs. 3.3%, P = 0.037). Both groups showed high rates of involuntary twitching (28.3% vs. 35.0%). Esketamine 0.5 mg/kg reduces propofol requirements and accelerates induction but prolongs recovery and increases specific adverse events, necessitating individualized dosing and postoperative monitoring to optimize safety.
VL - 13
IS - 1
ER -
Copy
|
Download