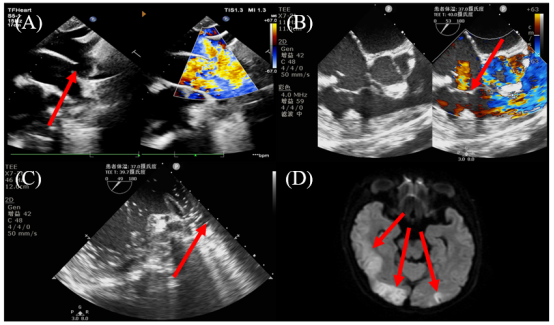
Background: There is a risk of significant complications due to paradoxical gas embolism during tricuspid annuloplasty under non-stop extracorporeal circulation without aortic block. Intraoperative real-time transesophageal echocardiography (TEE) is the most sensitive indicator for the detection of gas embolism. Case: This case present a patent ductus arteriosus (PDA) patient with pulmonary hypertension and severe tricuspid regurgitation scheduled for PDA closure and tricuspid annuloplasty. Intraoperative real-time TEE also showed a large number of small bubbles appearing in the left atrium near the orifice of the pulmonary vein. This case demonstrates that the amount of bubbles from the right heart may have exceeded the gas exchange capacity of the lung and entered the left atrium through the pulmonary vein. The patient delayed awakening after surgery and developed convulsive symptoms, decreased muscle strength of the left extremity, and head MRI suggested the possibility of acute cerebral embolism. Lessons: As a relatively simple tricuspid annuloplasty under non-stop extracorporeal circulation without aortic block, surgical may have catastrophic arterial embolism complications.
| Published in | International Journal of Anesthesia and Clinical Medicine (Volume 12, Issue 2) |
| DOI | 10.11648/j.ijacm.20241202.14 |
| Page(s) | 85-88 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Paradoxical Gas Embolism, Cerebral Infarction, Transesophageal Echocardiography, Non-Stop Extracorporeal Circulation
TEE | Transesophageal Echocardiography |
PDA | Patent Ductus Arteriosus |
CPB | Cardiopulmonary Bypass |
PFO | Patent Foramen Ovale |
TEE | Transesophageal Echocardiography |
ICU | Intensive Care Unit |
MRI | Magnetic Resonance Imaging |
| [1] | Chen, Z., Ke, Y., Xie, X., et al. Beating-Heart Totally Endoscopic Tricuspid Valvuloplasty in Reoperative Cardiac Surgery. The Annals of thoracic surgery. 2019, 107(1), e79-e82. |
| [2] | Niyibizi, E., Kembi, G. E., Lae, C., et al. Delayed hyperbaric oxygen therapy for air emboli after open heart surgery: case report and review of a success story. Journal of cardiothoracic surgery. 2016, 11(1), 167. |
| [3] | Oka, Y., Tsuzaki, K., Kamei, M., et al. Postoperative cerebral air embolism with delayed abnormal brain MRI findings. eNeurologicalSci. 2021, 22, 100305. |
| [4] | Wei, S., Cao, Y. R., Liu, D. X., et al. Cerebral infarction after cardiac surgery. Ibrain. 2022, 8(2), 190-198. |
| [5] | Brown, B., Frasco, P. E., Stoker, A. D. Intrapulmonary Shunting and Paradoxical Air Embolism in Liver Transplantation: A Case Report. The American journal of case reports. 2024, 25, e943042. |
| [6] | Sherlock, S. Paradoxical gas embolism during hysteroscopy. British journal of anaesthesia. 2008, 101(5), 742; author reply 742-743. |
| [7] | Hou, W., Zhong, J., Pan, B., et al. Paradoxical carbon dioxide embolism during laparoscopic surgery without intracardiac right-to-left shunt: two case reports and a brief review of the literature. The Journal of international medical research. 2020, 48(8), 300060520933816. |
| [8] | Jeon, S., Hong, J. M., Lee, H. J., et al. Paradoxical carbon dioxide embolism during laparoscopic hepatectomy without intracardiac shunt: A case report. World journal of clinical cases. 2022, 10(9), 2908-2915. |
| [9] | Nishant, A. R., Maddali, M. M. Intraoperative Transesophageal Echocardiography: A Sensitive and Reliable Tool for Detecting Air Embolism in Real Time. Journal of cardiothoracic and vascular anesthesia. 2019, 33(3), 878-880. |
| [10] | Kawahara, T., Hagiwara, M., Takahashi, H., et al. Cerebral Infarction by Paradoxical Gas Embolism During Laparoscopic Liver Resection with Injury of the Hepatic Vessels in a Patient without a Right-to-Left Systemic Shunt. The American journal of case reports. 2017, 18, 687-691. |
| [11] | Shimizu, K., Usuda, M., Kakizaki, Y., et al. Cerebral infarction by paradoxical gas embolism detected after laparoscopic partial hepatectomy with an insufflation management system: a case report. Surgical case reports. 2023, 9(1), 34. |
| [12] | Glenski, J. A., Cucchiara, R. F., Michenfelder, J. D. Transesophageal echocardiography and transcutaneous O2 and CO2 monitoring for detection of venous air embolism. Anesthesiology. 1986, 64(5), 541-545. |
| [13] | Butler, B. D., Hills, B. A. Transpulmonary passage of venous air emboli. Journal of applied physiology (Bethesda, Md: 1985). 1985, 59(2), 543-547. |
| [14] | Harlan, N. P., Davies, L. H., Weaver, L. K., et al. Spontaneous cerebral gas embolism and pulmonary arteriovenous malformation: a case report. Undersea & hyperbaric medicine: journal of the Undersea and Hyperbaric Medical Society, Inc. 2015, 42(5), 425-428. |
| [15] | Lee, H. N., Hyun, D. Pulmonary Arteriovenous Malformation and Its Vascular Mimickers. Korean journal of radiology. 2022, 23(2), 202-217. |
APA Style
Zhang, G., Yang, J., Li, X. (2024). Cerebral Infarction by Paradoxical Gas Embolism Detected Non-Stop Extracorporeal Circulation Tricuspid Annuloplasty Surgery with Real-Time TEE: A Case Report. International Journal of Anesthesia and Clinical Medicine, 12(2), 85-88. https://doi.org/10.11648/j.ijacm.20241202.14
ACS Style
Zhang, G.; Yang, J.; Li, X. Cerebral Infarction by Paradoxical Gas Embolism Detected Non-Stop Extracorporeal Circulation Tricuspid Annuloplasty Surgery with Real-Time TEE: A Case Report. Int. J. Anesth. Clin. Med. 2024, 12(2), 85-88. doi: 10.11648/j.ijacm.20241202.14
AMA Style
Zhang G, Yang J, Li X. Cerebral Infarction by Paradoxical Gas Embolism Detected Non-Stop Extracorporeal Circulation Tricuspid Annuloplasty Surgery with Real-Time TEE: A Case Report. Int J Anesth Clin Med. 2024;12(2):85-88. doi: 10.11648/j.ijacm.20241202.14
@article{10.11648/j.ijacm.20241202.14,
author = {Guangchao Zhang and Jiaqi Yang and Xuejie Li},
title = {Cerebral Infarction by Paradoxical Gas Embolism Detected Non-Stop Extracorporeal Circulation Tricuspid Annuloplasty Surgery with Real-Time TEE: A Case Report
},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {12},
number = {2},
pages = {85-88},
doi = {10.11648/j.ijacm.20241202.14},
url = {https://doi.org/10.11648/j.ijacm.20241202.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20241202.14},
abstract = {Background: There is a risk of significant complications due to paradoxical gas embolism during tricuspid annuloplasty under non-stop extracorporeal circulation without aortic block. Intraoperative real-time transesophageal echocardiography (TEE) is the most sensitive indicator for the detection of gas embolism. Case: This case present a patent ductus arteriosus (PDA) patient with pulmonary hypertension and severe tricuspid regurgitation scheduled for PDA closure and tricuspid annuloplasty. Intraoperative real-time TEE also showed a large number of small bubbles appearing in the left atrium near the orifice of the pulmonary vein. This case demonstrates that the amount of bubbles from the right heart may have exceeded the gas exchange capacity of the lung and entered the left atrium through the pulmonary vein. The patient delayed awakening after surgery and developed convulsive symptoms, decreased muscle strength of the left extremity, and head MRI suggested the possibility of acute cerebral embolism. Lessons: As a relatively simple tricuspid annuloplasty under non-stop extracorporeal circulation without aortic block, surgical may have catastrophic arterial embolism complications.
},
year = {2024}
}
TY - JOUR T1 - Cerebral Infarction by Paradoxical Gas Embolism Detected Non-Stop Extracorporeal Circulation Tricuspid Annuloplasty Surgery with Real-Time TEE: A Case Report AU - Guangchao Zhang AU - Jiaqi Yang AU - Xuejie Li Y1 - 2024/07/31 PY - 2024 N1 - https://doi.org/10.11648/j.ijacm.20241202.14 DO - 10.11648/j.ijacm.20241202.14 T2 - International Journal of Anesthesia and Clinical Medicine JF - International Journal of Anesthesia and Clinical Medicine JO - International Journal of Anesthesia and Clinical Medicine SP - 85 EP - 88 PB - Science Publishing Group SN - 2997-2698 UR - https://doi.org/10.11648/j.ijacm.20241202.14 AB - Background: There is a risk of significant complications due to paradoxical gas embolism during tricuspid annuloplasty under non-stop extracorporeal circulation without aortic block. Intraoperative real-time transesophageal echocardiography (TEE) is the most sensitive indicator for the detection of gas embolism. Case: This case present a patent ductus arteriosus (PDA) patient with pulmonary hypertension and severe tricuspid regurgitation scheduled for PDA closure and tricuspid annuloplasty. Intraoperative real-time TEE also showed a large number of small bubbles appearing in the left atrium near the orifice of the pulmonary vein. This case demonstrates that the amount of bubbles from the right heart may have exceeded the gas exchange capacity of the lung and entered the left atrium through the pulmonary vein. The patient delayed awakening after surgery and developed convulsive symptoms, decreased muscle strength of the left extremity, and head MRI suggested the possibility of acute cerebral embolism. Lessons: As a relatively simple tricuspid annuloplasty under non-stop extracorporeal circulation without aortic block, surgical may have catastrophic arterial embolism complications. VL - 12 IS - 2 ER -
Department of Anesthesiology, West China Hospital, Sichuan University and The Research Units of West China (2018RU012), Chinese Academy of Medical Sciences, Chengdu, China
Department of Anesthesiology, West China Hospital, Sichuan University and The Research Units of West China (2018RU012), Chinese Academy of Medical Sciences, Chengdu, China
Department of Anesthesiology, West China Hospital, Sichuan University and The Research Units of West China (2018RU012), Chinese Academy of Medical Sciences, Chengdu, China
Information