Background: Pain is one of the most common symptoms in cancer patients. We can understand it as a multifactorial phenomenon. Breast cancer surgical treatment generates real damage to the structures and activates nociception which can generate persistent pain. Current anesthetic management is based on the use of opioids, which generate a large number of complications that can severely affect this group of patients, increasing morbidity and mortality. Opioid-free techniques have been shown to reduce complications and generate optimal anesthetic-analgesic management as well as decrease postoperative misuse. The purpose of this research is to compare both approaches and evaluate their impact on this population group. Methods: Simple, prospective, randomized, controlled blind clinical trial in 30 patients undergoing oncological mammary quadrantectomy a. The patients were divided into two groups study, the first (group A) received balanced general anesthesia with opioids as an analgesic strategy, the other group (group B) received general anesthesia balanced opioid-free supplemented with a PECs II regional block and/or Serratus (BRILMA) according to the patient's sonoanatomy, and ketamine-lidocaine as adjuvant drugs. Analgesia was assessed using the numerical pain scale at 2, 4, and 6 o'clock. The severity and impact of pain on the daily performance of patients were measured using the Brief Pain Inventory (BPI) short form in combination with clinical examination, the presence of postoperative complications, the length of stay in hours and the need for rescue with opioids. Results: 35% of the patients in group A required analgesic rescue with Tramadol to improve pain postoperative, while in group B only 10% needed it. 33% of the patients in group A completed their postoperative period with nausea and vomiting, while in the opioid-free group the percentage was only 1%. Referring to the length of hospital stay from surgery to discharge, group A was hospitalized for a period of 25 hours (SD=21.2), while group B was there for 15.2 hours (SD=8.7). Conclusions:. Use of opioid-free anesthesia along with adjuvant strategies (drugs and nerve blocks) represent a safe and effective anesthetic strategy related with a lower incidence of complications from the use of opioids in the postoperative period, a lower consumption of analgesic rescues, a decrease in the length of hospitalization and a greater degree of comfort for the patient. This protocol represents an alternative when it comes to providing good intra and postoperative conditions for such a susceptible group of patients.
| Published in | International Journal of Anesthesia and Clinical Medicine (Volume 12, Issue 2) |
| DOI | 10.11648/j.ijacm.20241202.12 |
| Page(s) | 73-80 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Opioid Free Anesthesia, Cancer, Pain, Opioid Crisis Prevention, Opioid Misuse, Perioperative Pain Management, ERAS
Variables | Group | Mean | D.E. | Min | Max | p-value |
|---|---|---|---|---|---|---|
Length stay (horas) | Grupo A (n=15) | 25,0 | 21,2 | 10 | 37 | 0,025 |
Grupo B (n=15) | 15,2 | 8,7 | 6 | 24 | ||
satisfaction level at discharge | Grupo A (n=15) | 7,0 | 1,3 | 5 | 9 | 0,047 |
Grupo B (n=15) | 8,2 | 1,1 | 6 | 10 |
BMI | Body Mass Index |
NMDA | N-Methyl-D-aspartate |
MAC | Minimum Alveolar Concentration |
SD | Standard Deviation |
PVB | (Paravertebral Block). |
PEC | Pectoral Nerve Block |
GABA | Gamma-aminobutyric Acid |
5-HT | 5-hydroxytryptamine |
BPI | Brief Pain Inventory |
BRILMA | Block of the Lateral Branches of the Intercostal Nerves in the Middle Axillary Line |
PONV | Postoperative Nausea and Vomiting |
OFA | Opioid Free Anesthesia |
ERAS | Enhanced Recovery After Surgery |
| [1] |
Clark CW, Ferrer-Brechner T, Janal MN, Carroll DJ, Yang JC. The dimensions of pain: a multidimensional scaling comparison of cancer patients and healthy volunteers. Pain. 1989 Apr; 37(1): 23–32.
https://doi.org/10.1016/0304-3959(89)90149-8 PMID: 2726275. |
| [2] | Carles de Marque B. Valoración del dolor por cáncer. En: Bruera E, De Lima L. Cuidados Paliativos: Guías para el manejo clínico Washington: OPS-OMS; 2004; 27-30. |
| [3] | Schug SA, Palmer GM, Scott DA, Halliwell R, Trinca J. Acute pain management: scientific evidence, fourth edition, 2015. Med J Aust 204(8): 315–317. |
| [4] | Kehlet H, Jensen T, Wool C. Persistent postsurgical pain: risk factors and prevention. The Lancet, Vol 367, Issue 9522; 2006; 18-1625, ISSN 0140-6736, |
| [5] | Yuksel S, Chappell A, Jackson B, Wescott A, Ellis M. “Post Mastectomy Pain Syndrome: A Systematic Review of Prevention Modalities”, JPRAS Open, Vol 31; 2022; 32-49, ISSN 2352-5878, |
| [6] | Sancho JF, López G, Sancho A, Ávila C, Grande ML, Cavallo L, et al. Tratamiento del dolor oncológico [Treatment of cancer pain]. Psicooncologia (Pozuelo Alarcon). 2006; 3(1): 121–38. |
| [7] | Ramírez-Villagomez. Jaime Alberto. Efecto de la técnica anestésica y el uso de opioides en la función inmune del paciente quirúrgico oncológico [Effect of the anesthetic technique and the use of opioids on the immune function of the oncological surgical patient]. Anest. Méx. [online]; 2018, Vol. 30, n. 1 [cited 2021-09-06], 35-40. Disponible en: ISSN 2448-8771. |
| [8] | Sacerdote P, Franchi S, Panerai AE. Non-analgesic effects of opioids: mechanisms and potential clinical relevance of opioidinduced immu-nodepression. Curr Pharm; 2012; 18(37): 6034–42. PMID: 22747543 |
| [9] |
Lee LA, Caplan RA, Stephens LS, Posner KL, Terman GW, Voepel-Lewis T, et al. Postoperative opioid-induced respiratory depression: a closed claims analysis. Anesthesiology. 2015 Mar; 122(3): 659–65.
https://doi.org/10.1097/ALN.0000000000000564 PMID: 25536092. |
| [10] |
Kumar K, Goyal R, Mudgal A, Mohan A, Pasha S. YFa and analogs: investigation of opioid receptors in smooth muscle contraction. World J Gastroenterol. 2011 Oct; 17(40): 4523–31.
https://doi.org/10.3748/wjg.v17.i40.4523 PMID: 22110284. |
| [11] |
Steyaert A, Lavand’homme P. Postoperative opioids: let us take responsibility for the possible consequences. Eur J Anaesthesiol. 2013 Feb; 30(2): 50–2.
https://doi.org/10.1097/EJA.0b013e32835b9db2 PMID: 23303242. |
| [12] | Offermanns S, Rosenthal W. Encyclopedia of molecular pharmacology. Volume 1. 2nd ed. New York: Springer; 2010. pp. 25–36. |
| [13] | Boysen PG, Pappas MM, Evans B. An evidence-based opioid-free anesthetic technique to manage perioperative and periprocedural pain. Ochsner J. 2018; 18(2): 121–5. 17.0072 PMID: 30258291 |
| [14] | Samuels D, Abou-samra A, Dalvi P, et al. Journal of clini- 803 Artículo Original cal anesthesia and opioid-free anesthesia results in reduced post-operative opioid consumption. J Clin Anesth Pain Med. 2017; 1: 2–4. |
| [15] |
Morioka H, Kamiya Y, Yoshida T, Baba H. Pectoral nerve block combined with general anesthesia for breast cancer surgery: a retrospective comparison [Internet]. JA Clin Rep. 2015; 1(1): 15.
https://doi.org/10.1186/s40981-015-0018-1 PMID: 29497647. |
| [16] |
Bashandy GM, Abbas DN. Pectoral nerves I and II blocks in multimodal analgesia for breast cancer surgery: a randomized clinical trial. Reg Anesth Pain Med. 2015; 40(1): 68–74.
https://doi.org/10.1097/AAP.0000000000000163 PMID: 25376971. |
| [17] |
Blanco R, Fajardo M, Maldonado TP. Revista Española de Anestesiología y Reanimación Ultrasound description of Pecs II (modified Pecs I): A novel. Rev Esp Anestesiol Reanim [Internet]. Sociedad Española de Anestesiología. Reanimación y Terapéutica del Dolor. 2012; 59(9): 470–5.
https://doi.org/10.1016/j.redar.2012.07.003 PMID: 22939099. |
| [18] | Yusheng Y, Junyu L, Huanghui H, Ting X, Yanqing C. Ultrasoundguided serratus plane block enhances pain relief and quality of recovery after breast cancer surgery: A randomised controlled trial. European Journal of Anaesthesiology; 2019; Vol 36, Issue 6, p 436-441. |
| [19] |
Peltoniemi MA, Hagelberg NM, Olkkola KT, Saari TI. Ketamine: A Review of clinical pharmacokinetics and pharmacodynamics in anesthesia and pain therapy. Clin Pharmacokinet. 2016 Sep; 55(9): 1059–77.
https://doi.org/10.1007/s40262-016-0383-6 PMID: 27028535. |
| [20] |
Brinck EC, Tiippana E, Heesen M, Bell RF, Straube S, Moore RA, et al. Perioperative intravenous ketamine for acute postoperative pain in adults. Cochrane Database Syst Rev. 2018 Dec; 12(12): CD012033.
https://doi.org/10.1002/14651858.CD012033.pub4 PMID: 30570761. |
| [21] |
Frauenknecht J, Kirkham KR, Jacot-Guillarmod A, Albrecht E. Analgesic impact of intra-operative opioids vs. opioid-free anaesthesia: a systematic review and meta-analysis. Anaesthesia. 2019 May; 74(5): 651–62.
https://doi.org/10.1111/anae.14582 PMID: 30802933. |
| [22] |
Sultana A, Torres D, Schumann R. Special indications for Opioid Free Anaesthesia and Analgesia, patient and procedure related: including obesity, sleep apnoea, chronic obstructive pulmonary disease, complex regional pain syndromes, opioid addiction and cancer surgery. Best Pract Res Clin Anaesthesiol. 2017 Dec; 31(4): 547–60.
https://doi.org/10.1016/j.bpa.2017.11.002 PMID: 29739543. |
| [23] | López García O, et al. Ventajas de la anestesia intravenosa libre de opioides en cirugía ambulatoria oncológica de mama [Advantages of opioid-free intravenous anesthesia in outpatient breast oncology surgery]. Rev Ciencias Médicas [online]; 2020; Vol. 24, n. 5 [citado 2021-09- 05], e4648. Epub 25-Nov-2020. ISSN 1561-3194. |
| [24] |
Tripathy S, Rath S, Agrawal S, Rao PB, Panda A, Mishra TS, et al. Opioid-free anesthesia for breast cancer surgery: an observational study. J Anaesthesiol Clin Pharmacol. 2018; 34(1): 35–40.
https://doi.org/10.4103/joacp.JOACP_143_17 PMID: 29643620. |
| [25] |
Mulier JP. Is opioid-free general anesthesia for breast and gynecological surgery a viable option? Curr Opin Anaesthesiol. 2019 Jun; 32(3): 257–62.
https://doi.org/10.1097/ACO.0000000000000716 PMID: 31045633. |
| [26] |
De Oliveira GS Jr, Chang R, Khan SA, Hansen NM, Khan JH, McCarthy RJ, et al. Factors associated with the development of chronic pain after surgery for breast cancer: a prospective cohort from a tertiary center in the United States. Breast J. 2014; 20(1): 9–14.
https://doi.org/10.1111/tbj.12207 PMID: 24224885. |
| [27] |
Jogerst K, Thomas O, Kosiorek HE, Gray R, Cronin P, Casey W 3rd, et al. Same-Day Discharge After Mastectomy: Breast Cancer Surgery in the Era of ERAS®. Ann Surg Oncol. 2020 Sep; 27(9): 3436–45.
https://doi.org/10.1245/s10434-020-08386-w PMID: 32221736. |
APA Style
Heit, R. S. P. (2024). Opioid-Free Anesthesia and Analgesic Quality During the Postoperative Period of Oncological Breast Surgery. International Journal of Anesthesia and Clinical Medicine, 12(2), 73-80. https://doi.org/10.11648/j.ijacm.20241202.12
ACS Style
Heit, R. S. P. Opioid-Free Anesthesia and Analgesic Quality During the Postoperative Period of Oncological Breast Surgery. Int. J. Anesth. Clin. Med. 2024, 12(2), 73-80. doi: 10.11648/j.ijacm.20241202.12
AMA Style
Heit RSP. Opioid-Free Anesthesia and Analgesic Quality During the Postoperative Period of Oncological Breast Surgery. Int J Anesth Clin Med. 2024;12(2):73-80. doi: 10.11648/j.ijacm.20241202.12
@article{10.11648/j.ijacm.20241202.12,
author = {Rodrigo Sebastian Parada Heit},
title = {Opioid-Free Anesthesia and Analgesic Quality During the Postoperative Period of Oncological Breast Surgery
},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {12},
number = {2},
pages = {73-80},
doi = {10.11648/j.ijacm.20241202.12},
url = {https://doi.org/10.11648/j.ijacm.20241202.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20241202.12},
abstract = {Background: Pain is one of the most common symptoms in cancer patients. We can understand it as a multifactorial phenomenon. Breast cancer surgical treatment generates real damage to the structures and activates nociception which can generate persistent pain. Current anesthetic management is based on the use of opioids, which generate a large number of complications that can severely affect this group of patients, increasing morbidity and mortality. Opioid-free techniques have been shown to reduce complications and generate optimal anesthetic-analgesic management as well as decrease postoperative misuse. The purpose of this research is to compare both approaches and evaluate their impact on this population group. Methods: Simple, prospective, randomized, controlled blind clinical trial in 30 patients undergoing oncological mammary quadrantectomy a. The patients were divided into two groups study, the first (group A) received balanced general anesthesia with opioids as an analgesic strategy, the other group (group B) received general anesthesia balanced opioid-free supplemented with a PECs II regional block and/or Serratus (BRILMA) according to the patient's sonoanatomy, and ketamine-lidocaine as adjuvant drugs. Analgesia was assessed using the numerical pain scale at 2, 4, and 6 o'clock. The severity and impact of pain on the daily performance of patients were measured using the Brief Pain Inventory (BPI) short form in combination with clinical examination, the presence of postoperative complications, the length of stay in hours and the need for rescue with opioids. Results: 35% of the patients in group A required analgesic rescue with Tramadol to improve pain postoperative, while in group B only 10% needed it. 33% of the patients in group A completed their postoperative period with nausea and vomiting, while in the opioid-free group the percentage was only 1%. Referring to the length of hospital stay from surgery to discharge, group A was hospitalized for a period of 25 hours (SD=21.2), while group B was there for 15.2 hours (SD=8.7). Conclusions:. Use of opioid-free anesthesia along with adjuvant strategies (drugs and nerve blocks) represent a safe and effective anesthetic strategy related with a lower incidence of complications from the use of opioids in the postoperative period, a lower consumption of analgesic rescues, a decrease in the length of hospitalization and a greater degree of comfort for the patient. This protocol represents an alternative when it comes to providing good intra and postoperative conditions for such a susceptible group of patients.
},
year = {2024}
}
TY - JOUR T1 - Opioid-Free Anesthesia and Analgesic Quality During the Postoperative Period of Oncological Breast Surgery AU - Rodrigo Sebastian Parada Heit Y1 - 2024/07/29 PY - 2024 N1 - https://doi.org/10.11648/j.ijacm.20241202.12 DO - 10.11648/j.ijacm.20241202.12 T2 - International Journal of Anesthesia and Clinical Medicine JF - International Journal of Anesthesia and Clinical Medicine JO - International Journal of Anesthesia and Clinical Medicine SP - 73 EP - 80 PB - Science Publishing Group SN - 2997-2698 UR - https://doi.org/10.11648/j.ijacm.20241202.12 AB - Background: Pain is one of the most common symptoms in cancer patients. We can understand it as a multifactorial phenomenon. Breast cancer surgical treatment generates real damage to the structures and activates nociception which can generate persistent pain. Current anesthetic management is based on the use of opioids, which generate a large number of complications that can severely affect this group of patients, increasing morbidity and mortality. Opioid-free techniques have been shown to reduce complications and generate optimal anesthetic-analgesic management as well as decrease postoperative misuse. The purpose of this research is to compare both approaches and evaluate their impact on this population group. Methods: Simple, prospective, randomized, controlled blind clinical trial in 30 patients undergoing oncological mammary quadrantectomy a. The patients were divided into two groups study, the first (group A) received balanced general anesthesia with opioids as an analgesic strategy, the other group (group B) received general anesthesia balanced opioid-free supplemented with a PECs II regional block and/or Serratus (BRILMA) according to the patient's sonoanatomy, and ketamine-lidocaine as adjuvant drugs. Analgesia was assessed using the numerical pain scale at 2, 4, and 6 o'clock. The severity and impact of pain on the daily performance of patients were measured using the Brief Pain Inventory (BPI) short form in combination with clinical examination, the presence of postoperative complications, the length of stay in hours and the need for rescue with opioids. Results: 35% of the patients in group A required analgesic rescue with Tramadol to improve pain postoperative, while in group B only 10% needed it. 33% of the patients in group A completed their postoperative period with nausea and vomiting, while in the opioid-free group the percentage was only 1%. Referring to the length of hospital stay from surgery to discharge, group A was hospitalized for a period of 25 hours (SD=21.2), while group B was there for 15.2 hours (SD=8.7). Conclusions:. Use of opioid-free anesthesia along with adjuvant strategies (drugs and nerve blocks) represent a safe and effective anesthetic strategy related with a lower incidence of complications from the use of opioids in the postoperative period, a lower consumption of analgesic rescues, a decrease in the length of hospitalization and a greater degree of comfort for the patient. This protocol represents an alternative when it comes to providing good intra and postoperative conditions for such a susceptible group of patients. VL - 12 IS - 2 ER -
Anesthesiology Department, Sanatorium Allende, Córdoba, Argentina
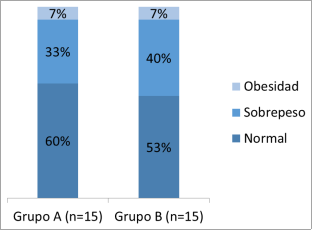
Figure 1. Distribution of BMI according to group (p = 0.731).
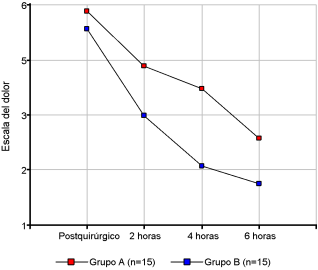
Figure 2. Graph of pain profiles according to group and moment of measurement.
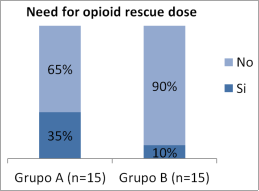
Figure 3. Need for rescue according to group (p = 0.235).
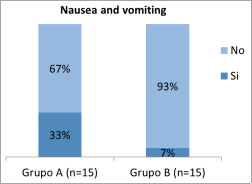
Figure 4. Presence of nausea and vomiting according to group (p = 0.043).
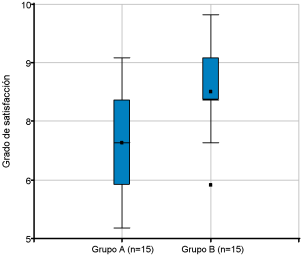
Figure 5. Box plots of the degree of comfort at discharge according to group.
Information

