Intracranial aneurysm is a very common disease, which is an abnormal bulge on the wall of intracranial artery. It is the first cause of subarachnoid hemorrhage. With the development of imaging, the disease is easily diagnosed. A 60-year-old man was diagnosed with anterior communicating artery aneurysm and underwent aneurysm clipping. During routine induction of anesthesia, a nasopharyngolaryngeal hemangioma was visualized under a video laryngoscope. This poses a serious challenge for tracheal intubation. With the assistance of a video laryngoscope and local anesthesia with lidocaine, a 6.5# reinforced endotracheal tube was inserted. Nasopharyngolaryngeal hemangioma is a congenital vascular anomaly characterized by proliferation of endothelial cells. The incidence of infantile and childhood hemangiomas is low, and most spontaneously resolve by the age of 4 to 6 years. Adult nasopharyngolaryngeal hemangioma are extremely rare and are residual lesions from infancy and childhood. Although nasopharyngolaryngeal hemangioma does not clearly affect the quality of life of patients, intracranial hemangioma has caused blurred vision and decreased vision. Therefore, surgery for intracranial aneurysm was necessary for this patient. This case emphasizes the management of unplanned difficult airway of pharyngeal hemangioma and the emergency plan for hemangioma rupture and bleeding. Provide guidance and risk management procedures for nasopharyngotracheal intubation.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
. The incidence of hemangiomas in infancy and childhood is about 4% to 5%. 85% to 90% of infantile hemangiomas resolve spontaneously by the age of 4 to 6 years
[2]
Luque-Luna M, Ivars M, et al. PIK3CA-related congenital haemangioma. J Eur Acad Dermatol Venereol. 2023; Epub ahead of print.
. Although adult hemangioma does not regress naturally, it is characterized by a relatively slow progression. Adult nasopharyngeal hemangioma (ANPLH) is extremely rare, deep and hidden. Previous studies have shown that ANPLH is a residual disease in infancy and childhood
[3]
Shpitzer T, Noyek AM, Witterick I, et al. Noncutaneous cavernous hemangiomas of the head and neck. Am J Otolaryngol 1997; 18: 367–374.
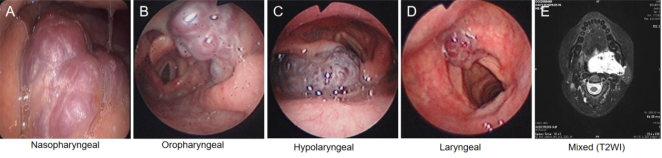
. ANPLH has been classified into four major categories: (1) nasopharyngeal (2) oropharyngeal (3) hypopharyngeal (4) laryngeal (5) mixed (hemangioma invading multiple anatomical sites) (Figure 1)
[4]
Shen Z, Zhang D, Li G, Huang D, Qiu Y, Xie C, Zhang X, Wang X, Liu Y. Clinical Characteristics, Classification, and Management of Adult Nasopharyngolaryngeal Hemangioma. Laryngoscope. 2021 Dec; 131 (12): 2724-2728.
. The case reports the airway management of a patient with intracranial aneurysm and laryngeal hemangioma. To our knowledge, this case has not been previously reported. This case describes the staging of nasopharyngeal haemangiomas, as well as giving advice on airway management of this disease. Written informed consent was obtained from the patient for the publication of this case report.
Figure 1. Different clinical types of laryngoscope pictures: A, nasopharyngeal; B, oropharyngeal; C, hypolaryngeal; D, laryngeal; E, magnetic resonance imaging of mixed (T2WI).
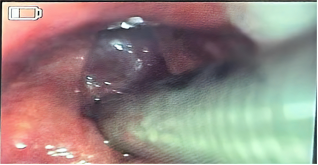
Figure 3. Visual laryngoscopic visualisation of the vocal folds after intubation.
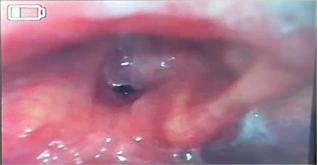
A 60-year-old male patient presented with double vision, blurred vision, decreased visual acuity, right-sided cranial distension, and generalised fatigue without any obvious cause. After admission, the patient underwent a complete examination, and CTA (Computed tomography angiography) suggested a nodular protrusion of the anterior communicating artery, with a diameter of about 0.3 cm, and the possibility of an aneurysm. The diagnosis was: 1. visual impairment: intracranial aneurysm? Other; 2. Hypertension grade 3 Very high risk; 3. Hyperlipidaemia; 4. Diabetes mellitus? The patient was proposed for anterior communicating artery aneurysm clamping. On admission to the operating theatre, induction of anaesthesia was performed after completion of routine monitoring. He was given 2 mg midazolam, 15ug sufentanil, 13 mg cis-atracurium, and 120 mg propofol followed by mask-assisted ventilation. Mask-assisted ventilation showed no obvious abnormality. After waiting for the drugs to take effect, visual laryngoscopy was performed to expose the vocal folds (Figure 2). Under visual laryngoscopy, there was a high suspicion that the supraglottic mass was a haemangioma. Immediately, 2% lidocaine surface anaesthesia was applied to the vocal folds and the area around the mass, and mask ventilation in PCV (Pressure-Controlled Ventilation) mode was applied until the surface anaesthesia took effect. The glottis was fully exposed under visual laryngoscopy again, and a 6.5# reinforced tracheal tube was gently rotated into the glottis, and the tracheal tube was fixed properly (Figure 3).
After completing the procedure, the tracheal tube was sent to PACU (Post anesthesia care unit) for extubation. Before extubation, he communicated with the otolaryngologist, neurosurgeon and the patient's family about the supraglottic tumour, surgical resection of the supraglottic haemangioma as well as tracheotomy if necessary. Considering the dual factors that intracranial aneurysm surgery does not affect respiratory awareness and that extubation may cause rupture and bleeding of the supraglottic aneurysm, deep anaesthesia was proposed for extubation. Depth of anaesthesia was maintained with 1% sevoflurane, 2% lidocaine was sprayed endotracheally, 1 mg/kg of 2% lidocaine was given intravenously, and adequate suctioning was performed. Lung resuscitation strategies prevented the patient from developing hypoxia after extubation due to pulmonary atelectasis, and PEEP support was also necessary. After the patient developed spontaneous respiration, the ventilator was switched to manual mode to assist spontaneous respiration and minimise confrontation with spontaneous respiration. When the patient's tidal volume was 6-8 ml/kg and the respiratory rate was 12-20 breaths, a 7.5# nasopharyngeal airway was placed, sevoflurane was turned off, and the endotracheal tube was gently withdrawn. The patient's thoracic respiratory motility was closely observed. The patient awoke with no obvious blood between the mouth and did not complain of any special discomfort.
3. Discussion
Hemangioma is a congenital vascular anomaly characterised by endothelial cell proliferation. ANPLH in adults is usually a residual lesion from infancy and childhood, and due to its rarity, there are only sporadic case reports and no large systematic studies are available
[5]
Rafie A, Jolly K, Darr A, Thompson S. Adult cavernous haemangioma of the vocal cords with a unique presentation of acute respiratory distress: a case report. Ann R Coll Surg Engl 2020; 102: e152–e154.
Jin M, Wang CY, Da YX, Zhu W, Jiang H. Surgical resection of a large hypopharyngeal hemangioma in an adult using neodymium-doped yttrium aluminum garnet laser: a case report. World J Clin Cases 2020; 8: 932–938.
. A review of previous cases summarised five types of nasopharyngeal hemangiomas, which are 1. isolated nasopharyngeal type; 2. oropharyngeal type; 3. hypopharyngeal type; 4. laryngeal type; and 5. mixed type (Figure 1). Our patient had laryngeal type hemangioma. For surgical treatment, all patients were resected via non-open surgery under general anaesthesia through the natural cavity (oral or nasal). Intraoperatively, high-frequency electric knife, bipolar electrocoagulation, CO2 laser, and low-temperature plasma radiofrequency ablation (LTPRA) were used alone or in combination. In patients with deep invasion of surrounding tissues, a single non-open surgery cannot ensure complete resection of the lesion, and sclerosing agents need to be injected around the wide and deep lesion to avoid postoperative recurrence
[8]
Jia J, Zhang J, Xiao S. Clinical effects of radiofrequency coblation for adult laryngopharyngeal vascular lesions. Laryngoscope 2021; 131: 566–570.
Shim HK, Kim MR. Potassium-titanyl-phosphate (KTP) laser photocoagulation combined with resection using an ultrasonic scalpel for pharyngolaryngeal hemangioma via a transoral approach: case report and literature review. Am J Case Rep 2021; 22: e931042.
In this case, the patient presented with an unplanned difficult airway and an urgent need for intracranial aneurysm surgery. Therefore, the management of the difficult airway in this case was of particular importance. Previous studies have shown that an anterior cervical airway approach can be used when there is a high risk of oxygenation failure when airway management is performed after induction of general anaesthesia or when there is a high risk of failure when tracheal intubation is performed while the patient is awake (e. g., in patients with large tumours in the supraglottic region)
[11]
Law JA, Heidegger T. Structured planning of airway management. In: Cook T, Kristensen MS, eds. Core topics in airway management. 3rd ed. Cambridge, England: Cambridge University Press, 2021: 38-49.
[12]
Popat M, Mitchell V, Dravid R, Patel A, Swampillai C, Higgs A. Difficult Airway Society guidelines for the management of tracheal extubation. Anaesthesia 2012; 67: 318.
. However, in the present case, an anterior carotid airway approach would have resulted in delayed recovery in a patient with an intracranial aneurysm, increased the risk of pulmonary infection, and should only be used as an emergency precaution. Under visual laryngoscopy, a laryngeal-type haemangioma was observed, which was extensive, covering approximately 1/2 of the vocal folds, but was soft and of low tension. These factors prompted an attempt at tracheal intubation. After evaluation and under the safeguard of an ENT, a 6.5# tracheal tube was gently inserted.
Removal of the tracheal tube in this case was also a difficult task. Previous studies have recommended that delayed extubation or tracheotomy be considered for extubation where there is a significant risk of extubation. A tracheal exchange catheter is recommended for high-risk patients who may have difficulty with reintubation. In the event that extubation fails, the physician can immediately reintubate the patient via a tracheal exchange catheter
[13]
Mort TC, Braffett BH. Conventional versus video laryngoscopy for tracheal tube exchange: glottic visualization, success rates, complications, and rescue alternatives in the high-risk difficult airway patient. Anesth Analg 2015; 121: 440-8.
. Prior to extubation, an appropriately sized catheter is placed and secured over the rongeur. These catheters usually do not cause problems and can be left in place until it is determined that the patient is unlikely to require reintubation
[14]
Heidegger T. Management of the Difficult Airway. N Engl J Med. 2021 May 13; 384 (19): 1836-1847.
. However, this method needs to be used with caution and may cause irreversible damage. For this reason, a mask or high-flow nasal cannula should be used to assist with oxygenation
[15]
Duggan LV, Law JA, Murphy MF. Supplementing oxygen through an airway exchange catheter: efficacy, complications, and recommendations. Can J Anaesth 2011; 58: 560-8.
. For our patient, the main risk of reintubation was rupture and bleeding of the laryngeal hemangioma. Therefore, the deep anaesthesia extubation method was used to reduce coughing, stress reaction and stimulation of the laryngeal hemangioma by the tracheal tube. However, the risk of this method lies in the patency of the airway after extubation and whether spontaneous breathing meets the oxygenation requirements.
For unplanned findings of nasopharyngeal haemangiomas that severely interfere with tracheal intubation, the case recommend that the urgency of the procedure be considered in combination with the urgency of the procedure to consider whether the non-nasopharyngeal haemangioma procedure should be performed first, and whether the proposed procedure can be postponed. If there is an urgent need for the proposed surgery, tracheal intubation may be attempted depending on the circumstances, provided that the anaesthesiologist and otolaryngologist are present and that the necessary tools for tracheotomy and angioma surgery are available. During extubation, extubation under deep anaesthesia can be considered under adequate surface anaesthesia and if the proposed surgery does not affect the patient's breathing and consciousness. Of course, adequate suctioning, nasopharyngeal airway, and pulmonary reexpansion strategies are essential before extubation.
4. Conclusion
This case gives some advice on the management of unplanned difficult airway due to combined nasopharyngolaryngeal hemangioma. Tracheal intubation can be attempted with adequate assessment of the vocal folds, team security, and equipment. During extubation, extubation under deep anaesthesia may be attempted. Also, secondary intubation needs to be avoided as much as possible.
Abbreviations
ANPLH
Adult Nasopharyngeal Hemangioma
CTA
Computed Tomography Angiography
PCV
Pressure-Controlled Ventilation
PACU
Post Anesthesia Care Unit
LTPRA
Low-Temperature Plasma Radiofrequency Ablation
Author Contributions
Guowei Wu: Writing - original draft, Visualization
Hongwei Xu: Writing - review & editing
Ethics Approval and Consent to Participate
All clinical practices were conducted by the principles of the Declaration of Helsinki.
Funding
This case report was not funded by any funding.
Data Availability Statement
No relevant data are available in this paper.
Conflicts of Interest
The authors declared that they have no competing interests.
References
[1]
Chen ZY, Wang QN, Zhu YH, et al. Progress in the treatment of infantile hemangioma. Ann Transl Med 2019; 7: 692.
Shen Z, Zhang D, Li G, Huang D, Qiu Y, Xie C, Zhang X, Wang X, Liu Y. Clinical Characteristics, Classification, and Management of Adult Nasopharyngolaryngeal Hemangioma. Laryngoscope. 2021 Dec; 131 (12): 2724-2728.
Rafie A, Jolly K, Darr A, Thompson S. Adult cavernous haemangioma of the vocal cords with a unique presentation of acute respiratory distress: a case report. Ann R Coll Surg Engl 2020; 102: e152–e154.
Jin M, Wang CY, Da YX, Zhu W, Jiang H. Surgical resection of a large hypopharyngeal hemangioma in an adult using neodymium-doped yttrium aluminum garnet laser: a case report. World J Clin Cases 2020; 8: 932–938.
Shim HK, Kim MR. Potassium-titanyl-phosphate (KTP) laser photocoagulation combined with resection using an ultrasonic scalpel for pharyngolaryngeal hemangioma via a transoral approach: case report and literature review. Am J Case Rep 2021; 22: e931042.
Law JA, Heidegger T. Structured planning of airway management. In: Cook T, Kristensen MS, eds. Core topics in airway management. 3rd ed. Cambridge, England: Cambridge University Press, 2021: 38-49.
[12]
Popat M, Mitchell V, Dravid R, Patel A, Swampillai C, Higgs A. Difficult Airway Society guidelines for the management of tracheal extubation. Anaesthesia 2012; 67: 318.
Mort TC, Braffett BH. Conventional versus video laryngoscopy for tracheal tube exchange: glottic visualization, success rates, complications, and rescue alternatives in the high-risk difficult airway patient. Anesth Analg 2015; 121: 440-8.
Duggan LV, Law JA, Murphy MF. Supplementing oxygen through an airway exchange catheter: efficacy, complications, and recommendations. Can J Anaesth 2011; 58: 560-8.
Wu, G., Xu, H. (2024). Airway Management of Intracranial Aneurysms Associated with Nasopharyngolaryngeal Hemangioma: A Case Report. International Journal of Anesthesia and Clinical Medicine, 12(1), 53-56. https://doi.org/10.11648/j.ijacm.20241201.20
Wu, G.; Xu, H. Airway Management of Intracranial Aneurysms Associated with Nasopharyngolaryngeal Hemangioma: A Case Report. Int. J. Anesth. Clin. Med.2024, 12(1), 53-56. doi: 10.11648/j.ijacm.20241201.20
Wu G, Xu H. Airway Management of Intracranial Aneurysms Associated with Nasopharyngolaryngeal Hemangioma: A Case Report. Int J Anesth Clin Med. 2024;12(1):53-56. doi: 10.11648/j.ijacm.20241201.20
@article{10.11648/j.ijacm.20241201.20,
author = {Guowei Wu and Hongwei Xu},
title = {Airway Management of Intracranial Aneurysms Associated with Nasopharyngolaryngeal Hemangioma: A Case Report
},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {12},
number = {1},
pages = {53-56},
doi = {10.11648/j.ijacm.20241201.20},
url = {https://doi.org/10.11648/j.ijacm.20241201.20},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20241201.20},
abstract = {Intracranial aneurysm is a very common disease, which is an abnormal bulge on the wall of intracranial artery. It is the first cause of subarachnoid hemorrhage. With the development of imaging, the disease is easily diagnosed. A 60-year-old man was diagnosed with anterior communicating artery aneurysm and underwent aneurysm clipping. During routine induction of anesthesia, a nasopharyngolaryngeal hemangioma was visualized under a video laryngoscope. This poses a serious challenge for tracheal intubation. With the assistance of a video laryngoscope and local anesthesia with lidocaine, a 6.5# reinforced endotracheal tube was inserted. Nasopharyngolaryngeal hemangioma is a congenital vascular anomaly characterized by proliferation of endothelial cells. The incidence of infantile and childhood hemangiomas is low, and most spontaneously resolve by the age of 4 to 6 years. Adult nasopharyngolaryngeal hemangioma are extremely rare and are residual lesions from infancy and childhood. Although nasopharyngolaryngeal hemangioma does not clearly affect the quality of life of patients, intracranial hemangioma has caused blurred vision and decreased vision. Therefore, surgery for intracranial aneurysm was necessary for this patient. This case emphasizes the management of unplanned difficult airway of pharyngeal hemangioma and the emergency plan for hemangioma rupture and bleeding. Provide guidance and risk management procedures for nasopharyngotracheal intubation.
},
year = {2024}
}
TY - JOUR
T1 - Airway Management of Intracranial Aneurysms Associated with Nasopharyngolaryngeal Hemangioma: A Case Report
AU - Guowei Wu
AU - Hongwei Xu
Y1 - 2024/06/19
PY - 2024
N1 - https://doi.org/10.11648/j.ijacm.20241201.20
DO - 10.11648/j.ijacm.20241201.20
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 53
EP - 56
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20241201.20
AB - Intracranial aneurysm is a very common disease, which is an abnormal bulge on the wall of intracranial artery. It is the first cause of subarachnoid hemorrhage. With the development of imaging, the disease is easily diagnosed. A 60-year-old man was diagnosed with anterior communicating artery aneurysm and underwent aneurysm clipping. During routine induction of anesthesia, a nasopharyngolaryngeal hemangioma was visualized under a video laryngoscope. This poses a serious challenge for tracheal intubation. With the assistance of a video laryngoscope and local anesthesia with lidocaine, a 6.5# reinforced endotracheal tube was inserted. Nasopharyngolaryngeal hemangioma is a congenital vascular anomaly characterized by proliferation of endothelial cells. The incidence of infantile and childhood hemangiomas is low, and most spontaneously resolve by the age of 4 to 6 years. Adult nasopharyngolaryngeal hemangioma are extremely rare and are residual lesions from infancy and childhood. Although nasopharyngolaryngeal hemangioma does not clearly affect the quality of life of patients, intracranial hemangioma has caused blurred vision and decreased vision. Therefore, surgery for intracranial aneurysm was necessary for this patient. This case emphasizes the management of unplanned difficult airway of pharyngeal hemangioma and the emergency plan for hemangioma rupture and bleeding. Provide guidance and risk management procedures for nasopharyngotracheal intubation.
VL - 12
IS - 1
ER -
Wu, G., Xu, H. (2024). Airway Management of Intracranial Aneurysms Associated with Nasopharyngolaryngeal Hemangioma: A Case Report. International Journal of Anesthesia and Clinical Medicine, 12(1), 53-56. https://doi.org/10.11648/j.ijacm.20241201.20
Wu, G.; Xu, H. Airway Management of Intracranial Aneurysms Associated with Nasopharyngolaryngeal Hemangioma: A Case Report. Int. J. Anesth. Clin. Med.2024, 12(1), 53-56. doi: 10.11648/j.ijacm.20241201.20
Wu G, Xu H. Airway Management of Intracranial Aneurysms Associated with Nasopharyngolaryngeal Hemangioma: A Case Report. Int J Anesth Clin Med. 2024;12(1):53-56. doi: 10.11648/j.ijacm.20241201.20
@article{10.11648/j.ijacm.20241201.20,
author = {Guowei Wu and Hongwei Xu},
title = {Airway Management of Intracranial Aneurysms Associated with Nasopharyngolaryngeal Hemangioma: A Case Report
},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {12},
number = {1},
pages = {53-56},
doi = {10.11648/j.ijacm.20241201.20},
url = {https://doi.org/10.11648/j.ijacm.20241201.20},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20241201.20},
abstract = {Intracranial aneurysm is a very common disease, which is an abnormal bulge on the wall of intracranial artery. It is the first cause of subarachnoid hemorrhage. With the development of imaging, the disease is easily diagnosed. A 60-year-old man was diagnosed with anterior communicating artery aneurysm and underwent aneurysm clipping. During routine induction of anesthesia, a nasopharyngolaryngeal hemangioma was visualized under a video laryngoscope. This poses a serious challenge for tracheal intubation. With the assistance of a video laryngoscope and local anesthesia with lidocaine, a 6.5# reinforced endotracheal tube was inserted. Nasopharyngolaryngeal hemangioma is a congenital vascular anomaly characterized by proliferation of endothelial cells. The incidence of infantile and childhood hemangiomas is low, and most spontaneously resolve by the age of 4 to 6 years. Adult nasopharyngolaryngeal hemangioma are extremely rare and are residual lesions from infancy and childhood. Although nasopharyngolaryngeal hemangioma does not clearly affect the quality of life of patients, intracranial hemangioma has caused blurred vision and decreased vision. Therefore, surgery for intracranial aneurysm was necessary for this patient. This case emphasizes the management of unplanned difficult airway of pharyngeal hemangioma and the emergency plan for hemangioma rupture and bleeding. Provide guidance and risk management procedures for nasopharyngotracheal intubation.
},
year = {2024}
}
TY - JOUR
T1 - Airway Management of Intracranial Aneurysms Associated with Nasopharyngolaryngeal Hemangioma: A Case Report
AU - Guowei Wu
AU - Hongwei Xu
Y1 - 2024/06/19
PY - 2024
N1 - https://doi.org/10.11648/j.ijacm.20241201.20
DO - 10.11648/j.ijacm.20241201.20
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 53
EP - 56
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20241201.20
AB - Intracranial aneurysm is a very common disease, which is an abnormal bulge on the wall of intracranial artery. It is the first cause of subarachnoid hemorrhage. With the development of imaging, the disease is easily diagnosed. A 60-year-old man was diagnosed with anterior communicating artery aneurysm and underwent aneurysm clipping. During routine induction of anesthesia, a nasopharyngolaryngeal hemangioma was visualized under a video laryngoscope. This poses a serious challenge for tracheal intubation. With the assistance of a video laryngoscope and local anesthesia with lidocaine, a 6.5# reinforced endotracheal tube was inserted. Nasopharyngolaryngeal hemangioma is a congenital vascular anomaly characterized by proliferation of endothelial cells. The incidence of infantile and childhood hemangiomas is low, and most spontaneously resolve by the age of 4 to 6 years. Adult nasopharyngolaryngeal hemangioma are extremely rare and are residual lesions from infancy and childhood. Although nasopharyngolaryngeal hemangioma does not clearly affect the quality of life of patients, intracranial hemangioma has caused blurred vision and decreased vision. Therefore, surgery for intracranial aneurysm was necessary for this patient. This case emphasizes the management of unplanned difficult airway of pharyngeal hemangioma and the emergency plan for hemangioma rupture and bleeding. Provide guidance and risk management procedures for nasopharyngotracheal intubation.
VL - 12
IS - 1
ER -