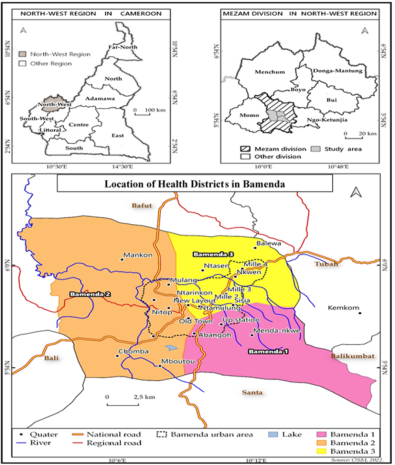
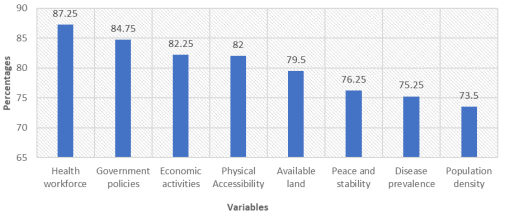
Accessibility of healthcare infrastructure are growing globally in a sustained manner and approximately 7.3 billion people around the world are unable to access essential health infrastructures embedded with well-deserved services needed for the treatment of health-related challenges. Health infrastructures accessibility remains a major cause of disease burden in Bamenda, couple with spatial distribution, insufficient resources, inadequate infrastructures and poor access to health services impact disease outcomes. This study seeks to analyze the spatial distribution of health infrastructure in Bamenda in the context of disease management. To obtained relative data for this study, both qualitative and quantitative data tools were employed. A total of 400 questionnaires were administered and analyzed using a spatial correlation and was presented in tables, Figures and maps. Findings reveals that health infrastructures in Bamenda include; hospitals, clinics, health centers and pharmacies. These health facilities are unevenly distributed with a strong concentration in Bamenda II, followed by Bamenda III, and very limited facilities in Bamenda I. This clustering patterns is observed particularly in commercial zones such as Commercial Avenue, Azire, and Nkwen. It was further observed that this spatial distribution of health infrastructure is greatly influence by government policies. Government planning and regulation are foundational to where health infrastructure is located. Policies often establish formal plans or health system frameworks that directly guide the siting of health facilities to meet population needs. Governments and private investors are more likely to locate facilities in areas where staffing needs can be met. Findings further revealed that the availability of skilled health workforce is the most important driver influencing the distribution of health facilities in Bamenda with. Investments in workforce training, deployment, and retention can stimulate more balanced spatial distribution of health infrastructure, improving equity and population health outcomes.
| Published in | International Journal of Health Economics and Policy (Volume 11, Issue 2) |
| DOI | 10.11648/j.hep.20261102.16 |
| Page(s) | 121-130 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Health, Infrastructure, Accessibility, Diseases, Management, Bamenda
WHO | World Health Organization |
COPD | Chronic Obstructive Pulmonary Diseases |
SPSS | Statistical Package for Social Sciences |
IHC | Integrated Health Centers |
NGOs | Non-Governmental Organizations |
TB | Tuberculosis |
HIV/AIDS | Human Immune Virus/Acquired Immune Deficiency Syndrome |
| [1] |
World Health Organization, (2018). Primary health care and health emergencies. World Health Organization.
https://www.who.int/docs/defaut-source/documents/primary-health-care-and-health-emergencies.pdf |
| [2] | World Health Organization [WHO] & Bank. (2013). Tracking Universal Health Coverage: 2017 global monitoring report. World Health Organization. |
| [3] | Kanuganti, S., Sarkar, A. K., Singh, A. P., & Arkatkar, S. S. (2015). Quantification of accessibility to health facilities in rural areas. Case Studies on Transport Policy, 3(3), 311–320. |
| [4] | Makanga, P. T., Schuurman, N., Sacoor, C., Boene, H. E., Vilanculo, F., Vidler, M., Magee, L., von Dadelszen, P., Sevene, E., Munguambe, K., & Firoz, T. (2017). Seasonal variation in geographical access to maternal health services in regions of southern Mozambique. International Journal of Health Geographics, 16(1), 1. |
| [5] | Tanou, M., Kishida, T., & Kamiya, Y. (2021). The effects of geographical accessibility to health facilities on antenatal care and delivery services utilization in Benin: A cross-sectional study. Reproductive Health, 18(1), 205. |
| [6] | Mboera LE, Mfinanga SG, Karimuribo ED, Rumisha SF, Sindato C. The changing landscape of public health in sub-Saharan Africa: control and prevention of communicable diseases needs rethinking. Onderstepoort J Vet Res. 2014; 81(2): E1–6. Epub 2014/07/10. |
| [7] | Gouda HN, Charlson F, Sorsdahl K, Ahmadzada S, Ferrari AJ, Erskine H, et al. Burden of non-communicable diseases in sub-Saharan Africa, 1990–2017: results from the Global Burden of Disease Study 2017. The Lancet Global Health. 2019; 7(10): e1375–e87. |
| [8] | Delamater PL, Messina JP, Shortridge AM, Grady SC. Measuring geographic access to health care: raster and network-based methods. International journal of health geographics. 2012; 11(1): 15. |
| [9] | Ajala, O. A., Sanni, L., Adeyinka, S. A. (2005). Accessibility to health care facilities: A panacea for sustainable rural development in Osun State south-western Nigeria. J Hum Ecol, 18(2): 121-128. |
| [10] | World Meteorological Organization. (2023). Extreme weather caused two million deaths and $4 trillion in losses over 50 years. United Nations Office at Geneva. |
| [11] | World Health Organization (WHO). (2010). Equitable access to essential medicines: A framework for collective action. Geneva: WHO. |
| [12] | Tikkanen, R. S., & Eric C. Schneider. (2020). Social spending to improve population health—Does the United States spend as wisely as other countries? The New England Journal of Medicine, 382(10), 885–887. |
| [13] | CDP. (2012). Bamenda city council development plan. Yaounde: MINDDEVEL. |
| [14] |
Centers for Disease Control and Prevention. (2020, February 14). Health equity considerations and racial and ethnic minority groups.
https://www.cdc.gov/coronavirus/2019-ncov/community/health-equity/race-ethnicity.html |
| [15] | United Nations. (2006). Convention on the rights of persons with disabilities. |
| [16] | World Health Organization. (2020). Primary health care on the road to universal health coverage: 2019 monitoring report. |
| [17] | SOP SOP Maturin Désiré, Abossolo Samuel Aimé, Nuebissi simo joseph Landry, Mbarga Manga J. M. V, Batha Romain Armand Soleil (2015). The influence of climate change/variability on the prevalence of respiratory diseases: The case of asthma in Bamenda. WWJMRD 2015; 1(4): 40-53. |
| [18] |
World Health Organization. (2022). Universal health coverage (UHC).
https://ww.who.int/news-room/fact-sheets/detail/universal-health-coverage-(uhc) |
APA Style
Akwanwi, N. B., Kometa, S. S., Temgoua, N. Y. (2026). Health Infrastructures Accessibility and Diseases Management in Bamenda North West Region, Cameroon. International Journal of Health Economics and Policy, 11(2), 121-130. https://doi.org/10.11648/j.hep.20261102.16
ACS Style
Akwanwi, N. B.; Kometa, S. S.; Temgoua, N. Y. Health Infrastructures Accessibility and Diseases Management in Bamenda North West Region, Cameroon. Int. J. Health Econ. Policy 2026, 11(2), 121-130. doi: 10.11648/j.hep.20261102.16
@article{10.11648/j.hep.20261102.16,
author = {Ngyia Benis Akwanwi and Sunday Shende Kometa and Nadine Yemelong Temgoua},
title = {Health Infrastructures Accessibility and Diseases Management in Bamenda North West Region, Cameroon},
journal = {International Journal of Health Economics and Policy},
volume = {11},
number = {2},
pages = {121-130},
doi = {10.11648/j.hep.20261102.16},
url = {https://doi.org/10.11648/j.hep.20261102.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.hep.20261102.16},
abstract = {Accessibility of healthcare infrastructure are growing globally in a sustained manner and approximately 7.3 billion people around the world are unable to access essential health infrastructures embedded with well-deserved services needed for the treatment of health-related challenges. Health infrastructures accessibility remains a major cause of disease burden in Bamenda, couple with spatial distribution, insufficient resources, inadequate infrastructures and poor access to health services impact disease outcomes. This study seeks to analyze the spatial distribution of health infrastructure in Bamenda in the context of disease management. To obtained relative data for this study, both qualitative and quantitative data tools were employed. A total of 400 questionnaires were administered and analyzed using a spatial correlation and was presented in tables, Figures and maps. Findings reveals that health infrastructures in Bamenda include; hospitals, clinics, health centers and pharmacies. These health facilities are unevenly distributed with a strong concentration in Bamenda II, followed by Bamenda III, and very limited facilities in Bamenda I. This clustering patterns is observed particularly in commercial zones such as Commercial Avenue, Azire, and Nkwen. It was further observed that this spatial distribution of health infrastructure is greatly influence by government policies. Government planning and regulation are foundational to where health infrastructure is located. Policies often establish formal plans or health system frameworks that directly guide the siting of health facilities to meet population needs. Governments and private investors are more likely to locate facilities in areas where staffing needs can be met. Findings further revealed that the availability of skilled health workforce is the most important driver influencing the distribution of health facilities in Bamenda with. Investments in workforce training, deployment, and retention can stimulate more balanced spatial distribution of health infrastructure, improving equity and population health outcomes.},
year = {2026}
}
TY - JOUR T1 - Health Infrastructures Accessibility and Diseases Management in Bamenda North West Region, Cameroon AU - Ngyia Benis Akwanwi AU - Sunday Shende Kometa AU - Nadine Yemelong Temgoua Y1 - 2026/06/10 PY - 2026 N1 - https://doi.org/10.11648/j.hep.20261102.16 DO - 10.11648/j.hep.20261102.16 T2 - International Journal of Health Economics and Policy JF - International Journal of Health Economics and Policy JO - International Journal of Health Economics and Policy SP - 121 EP - 130 PB - Science Publishing Group SN - 2578-9309 UR - https://doi.org/10.11648/j.hep.20261102.16 AB - Accessibility of healthcare infrastructure are growing globally in a sustained manner and approximately 7.3 billion people around the world are unable to access essential health infrastructures embedded with well-deserved services needed for the treatment of health-related challenges. Health infrastructures accessibility remains a major cause of disease burden in Bamenda, couple with spatial distribution, insufficient resources, inadequate infrastructures and poor access to health services impact disease outcomes. This study seeks to analyze the spatial distribution of health infrastructure in Bamenda in the context of disease management. To obtained relative data for this study, both qualitative and quantitative data tools were employed. A total of 400 questionnaires were administered and analyzed using a spatial correlation and was presented in tables, Figures and maps. Findings reveals that health infrastructures in Bamenda include; hospitals, clinics, health centers and pharmacies. These health facilities are unevenly distributed with a strong concentration in Bamenda II, followed by Bamenda III, and very limited facilities in Bamenda I. This clustering patterns is observed particularly in commercial zones such as Commercial Avenue, Azire, and Nkwen. It was further observed that this spatial distribution of health infrastructure is greatly influence by government policies. Government planning and regulation are foundational to where health infrastructure is located. Policies often establish formal plans or health system frameworks that directly guide the siting of health facilities to meet population needs. Governments and private investors are more likely to locate facilities in areas where staffing needs can be met. Findings further revealed that the availability of skilled health workforce is the most important driver influencing the distribution of health facilities in Bamenda with. Investments in workforce training, deployment, and retention can stimulate more balanced spatial distribution of health infrastructure, improving equity and population health outcomes. VL - 11 IS - 2 ER -
Department of Geography and Planning, University of Bamenda, Bamenda, Cameroon
Department of Geography and Planning, University of Bamenda, Bamenda, Cameroon
Department of Customs, University of Bamenda, Bamenda, Cameroon
Information