Introduction: In Benin, where out-of-pocket payment constitutes the primary healthcare financing mechanism, the fee-setting practices of First Contact Health Facilities (FCHFs) directly condition financial access to care for the population. This study aims to document the regulatory framework and pricing practices in Beninese FCHFs and to analyse their relationships with the socio-economic characteristics of health districts. Methods: A descriptive and analytical cross-sectional study was conducted in 2025 using fee schedules from 28 of the 34 health districts. Four categories of services were analysed: clinical and technical procedures (n=59), biological laboratory investigations (n=74), medical imaging examinations (n=4), and specialist procedures (n=17, Cotonou only). Tariffs were stratified by area type (urban/rural) and triangulated with departmental poverty rates, FCHF attendance rates, and the share of community-based financing. A Pearson correlation coefficient was calculated between poverty and fee levels. Results: No legal instrument governed FCHF fee-setting. Childbirth exhibited the highest dispersion (CV=94.46%; range: 885–15,000 FCFA). The mean fee for a medical consultation was 1,571 ± 535 FCFA in urban areas versus 1,118 ± 402 FCFA in rural areas, a differential of 40.5%. Certain highly impoverished rural districts maintained fees above the national average. A moderate but statistically significant negative correlation was observed between the departmental poverty rate and the medical consultation fee (r=−0.651; p=0.001). Own revenues of FCHFs accounted for 97.4% of their resources. Conclusion: Fee-setting in Beninese FCHFs relies on informal mechanisms that generate inequities in access to care. The ongoing reforms in the health sector represent an opportunity to establish equitable fee schedules, grounded in the socio-economic realities of the population, the principles of primary health care, and coupled with social protection mechanisms for vulnerable households.
| Published in | International Journal of Health Economics and Policy (Volume 11, Issue 2) |
| DOI | 10.11648/j.hep.20261102.14 |
| Page(s) | 96-110 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Healthcare Pricing, FCHF, Health Equity, Health District, Benin, Community-based Financing, Universal Health Coverage
Category of service | Procedures (n) | Min. (FCFA) | Max. (FCFA) | Median [Q1; Q3] (FCFA) | Mean ± SD (FCFA) |
|---|---|---|---|---|---|
Clinical and technical procedures | 59 | 0 | 15,000 | 800 [300; 1,900] | 1,450 ± 1,868 |
Biological laboratory investigations | 74 | 0 | 15,000 | 2,000 [1,500; 3,000] | 2,343 ± 1,494 |
Medical imaging examinations | 4 | 4,000 | 12,000 | 5,000 [5,000; 7,000] | 6,177 ± 2,389 |
TOTAL | 154 | 0 | 15,000 | 1,800 [900; 2,500] | 2,000 ± 1,950 |
Department | Area type | Monetary poverty rate (%) [EHCVM 2022] | FCHF attendance rate (%) [HSY 2024] | Share of community-based financing (%) [HSY 2024] |
|---|---|---|---|---|
Littoral | Urban | 18.3 | 67.6 | 90.8 |
Atlantique | Rural | 23.9 | 50.7 | 98.4 |
Ouémé | Urban | 16.0 | 35.1 | 97.2 |
Mono | Rural | 45.1 | 47.7 | 97.8 |
Couffo | Rural | 54.1 | 40.6 | 97.8 |
Plateau | Rural | 34.1 | 28.6 | 95.6 |
Collines | Rural | 22.1 | 42.6 | 97.2 |
Zou | Rural | 41.4 | 43.1 | 98.1 |
Borgou | Rural | 47.7 | 79.1 | 98.2 |
Donga | Rural | 48.4 | 56.5 | 96.3 |
Atacora | Rural | 53.1 | 71.9 | 97.1 |
Alibori | Rural | 44.7 | 61.8 | 98.0 |
Benin (national) | – | 36.2 | 59.3 | 97.4 |
ARCH | Assurance Pour le Renforcement du Capital Humain |
CNERS | National Ethics Committee for Health Research |
CV | Coefficient of Variation |
DHMT | District Health Management Team |
DHIS2 | District Health Information Software 2 |
EHCVM | Harmonised Survey on Living Conditions of Households |
FCHF | First Contact Health Facility |
FCFA | Franc of Financial Community of Africa (1 USD ≈ 600 FCFA) |
HSY | Health Statistics Yearbook |
INStaD | National Institute of Statistics and Demography |
PUSS | Health Service User Platform |
SDG | Sustainable Development Goal |
SIGL | Logistics Management Information System |
SNIGS | National Health Information System |
UHC | Universal Health Coverage |
No. | Procedure Description | Category |
|---|---|---|
1 | Medical consultation | Clinical and technical procedures (n=59) |
2 | Specialist consultation | |
3 | Nursing consultation | |
4 | Curative midwife consultation | |
5 | Follow-up curative consultation | |
6 | New antenatal care consultation (midwife) | |
7 | Follow-up antenatal care consultation (midwife) | |
8 | Postnatal consultation | |
9 | Childbirth (delivery) | |
10 | Ventouse (vacuum extraction) | |
11 | Episiotomy | |
12 | Manual removal of placenta / home delivery | |
13 | Repair of soft-tissue lacerations without episiotomy | |
14 | Manual vacuum aspiration (MVA) / curettage | |
15 | Internal version manoeuvre | |
16 | Manual removal of placenta + uterine revision (DA+RU) | |
17 | Post-abortion care | |
18 | Ward hospitalisation (per day) | |
19 | Admission for observation | |
20 | Care and intravenous injections | |
21 | Care and intramuscular injections | |
22 | Outpatient care (injection) | |
23 | Insertion of intravenous line | |
24 | Catheter placement | |
25 | Transfusion procedure (accredited centre) | |
26 | Blood pressure measurement | |
27 | Weight measurement | |
28 | Wound dressing | |
29 | Post-road traffic accident dressing | |
30 | Post-caesarean section dressing | |
31 | Packing dressing (mèche) | |
32 | Perineal suture | |
33 | Suture of traumatic lesion (per stitch) | |
34 | Suture of traumatic lesion (more than five stitches) | |
35 | Circumcision | |
36 | Incision and drainage of abscess | |
37 | Wound debridement / non-extensive soft-tissue trauma | |
38 | Wound debridement / extensive soft-tissue trauma | |
39 | Burns debridement dressing | |
40 | Nasogastric tube insertion | |
41 | Urinary catheter insertion | |
42 | Removal of indwelling catheter | |
43 | Oxygen therapy per hour (adult) | |
44 | Oxygen therapy per hour (neonate) | |
45 | Neonatal resuscitation | |
46 | TIUB insertion | |
47 | Family planning device insertion (IUD or implant) | |
48 | Jadelle removal | |
49 | IUD removal | |
50 | Foreign body removal | |
51 | Fluid aspiration (paracentesis) | |
52 | Suprapubic aspiration | |
53 | Ear irrigation | |
54 | Nasal irrigation | |
55 | Evacuant enema | |
56 | Nebulisation (aerosol therapy) per session | |
57 | Frenectomy (frenotomy) | |
58 | Ear piercing | |
59 | Miscellaneous outpatient care (including catch-up vaccination) | |
1 | ABO blood group – Rhesus factor (ABO-Rh) | Biological laboratory investigations (n=74) |
2 | Haemoglobin level | |
3 | Haematocrit / Haemoglobin and haematocrit | |
4 | White blood cell count | |
5 | Full blood count (FBC) | |
6 | FBC + platelets | |
7 | Reticulocyte count | |
8 | FBC + platelets + reticulocytes | |
9 | Blood ionogram (serum electrolytes) | |
10 | Urine ionogram | |
11–13 | Na+, K+, Cl− (selective electrolytes) | |
14 | Glycated haemoglobin (HbA1c) | |
15–18 | Blood glucose, urine dipstick (3 parameters), glucosuria, capillary blood glucose | |
19–21 | Serum creatinine, urea, uric acid | |
22–26 | Triglycerides, total cholesterol, HDL, serum calcium, serum magnesium | |
27–32 | AST (SGOT), ALT (SGPT), GGT, total protein, Emmel test, Hb electrophoresis | |
33–39 | Thick blood film/differential, SDW, TPHA, VDRL, standard MCUS, MCUS + sensitivity, CSF culture | |
40–44 | Pus culture, ascitic fluid culture, CSF glucose, CSF biochemistry, CRP | |
45–50 | ESR, bleeding time, clotting time, stool examination (AKOP/coprology), HBs Ag, anti-HCV | |
51–58 | HIV, AFB smear, semen analysis, thyroglobulin (serum/urine), ASLO, total/direct bilirubin, PSA | |
59–65 | H. pylori Ag, total protein, bilharzial ova, bile salts, bile pigments, tuberculin skin test (TST/IDR), microfilaria | |
66–72 | Vaginal swab, TSH, LH, T3, T4, toxoplasmosis serology, rubella serology | |
1 | Obstetric ultrasound | Medical imaging examinations (n=4) |
2 | Pelvic ultrasound | |
3 | Abdomino-pelvic ultrasound | |
4 | Dental radiograph | |
1–11 | Fundoscopy, dental extraction (wisdom tooth, incisor/canine, premolar/molar), stomatology consultation, scaling, obturation (amalgam, simple), pulpectomy (incisor, molar, premolar) | Specialist procedures* (n=17, Cotonou only) |
| [1] | World Health Organisation, World Bank Group. Tracking Universal Health Coverage: 2023 Global Monitoring Report. Geneva: WHO/World Bank Group; 2023. |
| [2] | Institut National de la Statistique et de la Démographie (INStaD). Note on Poverty in 2022 – Results of the Harmonised Survey on Living Conditions of Households (EHCVM) 2021–2022. Cotonou: INStaD; 2023. |
| [3] | Paul E, Sambiéni NE, Wangbe J-P, Fecher F, Bourgeois M. Budgeting challenges on the path towards universal health coverage: the case of Benin. Health Econ Rev. 2020, 10(1), 28. |
| [4] | Ministry of Health of Benin. Report of the Survey on the Availability and Operational Capacity of Health Services (SARA/HHFA) in Benin 2022. Cotonou: Ministry of Health; 2023. |
| [5] | World Health Organisation. Trends in maternal mortality 2000 to 2020: estimates by WHO, UNICEF, UNFPA, World Bank Group and UNDESA/Population Division. Geneva: WHO; 2023. |
| [6] | Gilson L. The lessons of user fee experience in Africa. Health Policy Plan. 1997, 12(3), 273–285. |
| [7] | Houngbeme DJ-L. In Benin, living conditions are deteriorating despite slight economic growth. Dispatch No. 575. Abidjan: Afrobarometer; 2022. |
| [8] | Africa Evidence Network. Poverty dynamics and the Figures of those left behind in Atacora and Donga (Northwest Benin). Johannesburg: Africa Evidence Network; 2023. |
| [9] | Ministry of Health of Benin. Roadmap: Revision of Health Service Fees in Benin. Service Note No. 0537-2025/MS/DC/SGM/SP. Cotonou: Ministry of Health; 2025. |
| [10] | World Bank. Benin Overview: Development Data [Internet]. Washington, DC: World Bank; 2024 [cited 12 April 2026]. Available from: |
| [11] | Houeninvo HG, Bello K, Hounkpatin H, Dossou J-P. Developing and implementing National Health Insurance: learnings from the first try in Benin. BMJ Glob Health. 2022, 7(11), e009027. |
| [12] | ACTwatch Group, Zinsou C, Cherifath AB. The malaria testing and treatment landscape in Benin. Malar J. 2017, 16(1), 174. |
| [13] | Dossou J-P, De Brouwere V, Van Belle S, Marchal B. Opening the 'implementation black-box' of the user fee exemption policy for caesarean section in Benin: a realist evaluation. Health Policy Plan. 2020, 35(2), 153–166. |
| [14] | Grossman M. On the concept of health capital and the demand for health. J Polit Econ. 1972, 80(2), 223–255. |
| [15] | Lagarde M, Palmer N. The impact of user fees on health service utilization in low- and middle-income countries: how strong is the evidence? Bull World Health Organ. 2008, 86(11), 839–848. |
| [16] | Institut National de la Statistique et de la Démographie (INStaD). Demographic Projections from 2014 to 2063 and Perspectives on Social Demand from 2014 to 2030 in Benin. Cotonou: INStaD; 2022. |
| [17] | Ministry of Health of Benin. Health Statistics Yearbook 2024. Cotonou: SNIGS-MS; 2025. |
| [18] | Republic of Benin. Law No. 90-32 of 11 December 1990 on the Constitution of the Republic of Benin. Cotonou; 1990. |
| [19] | Republic of Benin. Law No. 97-020 of 17 June 1997 on the Organisation of Health Care in the Republic of Benin. Cotonou: Government of Benin; 1997. |
| [20] | Republic of Benin. Law No. 2020-37 of 3 February 2021 on the Protection of Persons' Health in the Republic of Benin. Cotonou; 2021. |
| [21] | Republic of Benin. Decree No. 88-444 of 18 November 1988 on the Introduction of Medicine Sales in Public Health Facilities and Confessional or Associative Private Health Centres. Cotonou: Government of Benin; 1988. |
| [22] | Republic of Benin. Law No. 2021-03 of 1 February 2021 on the Organisation of Pharmaceutical Activities in the Republic of Benin. Cotonou: National Assembly; 2021. |
| [23] | Republic of Benin. Decree No. 96-25 of 23 January 1996 on the Method of Determining Public Prices for Medicines and Pharmaceutical Specialities in the Republic of Benin. Cotonou; 1996. |
| [24] | Republic of Benin. Decree No. 97-321 of 17 July 1997 on the Regulation of Social Assistance in the Republic of Benin. Cotonou; 1997. |
| [25] | Institut National de la Statistique et de la Démographie (INStaD). Harmonised Survey on Living Conditions of Households (EHCVM) 2019. Cotonou: INStaD; 2020. |
| [26] | Olago A, Suharlim C, Hussein S, Njuguna D, Macharia S, Muñoz R, et al. The costs and financing needs of delivering Kenya's primary health care service package. Front Public Health. 2023, 11, 1226163. |
| [27] | Jacobs B, Hui K, Lo V, Thiede M, Appelt B, Flessa S. Costing for universal health coverage: insight into essential economic data from three provinces in Cambodia. Health Econ Rev. 2019, 9(1), 29. |
| [28] | Wagstaff A, Van Doorslaer E. Equity in health care finance and delivery. In: Culyer AJ, Newhouse JP. Handbook of Health Economics. Elsevier; 2000. pp. 1803–1862. |
| [29] | O'Donnell O, Van Doorslaer E, Wagstaff A, Lindelow M. Analysing Health Equity Using Household Survey Data. Washington, DC: World Bank; 2008. |
| [30] | Ndayishimiye C, Sowada C, Dubas-Jakóbczyk K, Flessa S. Costing primary health care services in Burundi: evidence for universal health coverage planning. Front Public Health. 2024, 13, 1446497. |
| [31] | Koduah A, Baatiema L, Cronin de Chavez A, Danso-Appiah A, Kretchy IA, Agyepong IA, et al. Implementation of medicines pricing policies in sub-Saharan Africa: systematic review. Syst Rev. 2022, 11, 214. |
| [32] | Palmer S, Torgerson DJ. Definitions of efficiency. BMJ. 1999, 318(7191), 1136. |
| [33] | Kruk ME, Goldmann E, Galea S. Borrowing and selling to pay for health care in low- and middle-income countries. Health Aff. 2009, 28(4), 1056–1066. |
| [34] | Knaul FM, González-Pier E, Gómez-Dantés O, García-Junco D, Arreola-Ornelas H, Barraza-Lloréns M, et al. The quest for universal health coverage: achieving social protection for all in Mexico. Lancet. 2012, 380(9849), 1259–1279. |
| [35] | Dzakpasu S, Powell-Jackson T, Campbell OMR. Impact of user fees on maternal health service utilisation and related health outcomes: a systematic review. Health Policy Plan. 2014, 29(2), 137–150. |
| [36] | Witter S, Dieng T, Mbengue D, Moreira I, De Brouwere V. The national free delivery and caesarean policy in Senegal: evaluating process and outcomes. Health Policy Plan. 2010, 25(5), 384–392. |
| [37] | Xu K, Evans DB, Kawabata K, Zeramdini R, Klavus J, Murray CJ. Household catastrophic health expenditure: a multicountry analysis. Lancet. 2003, 362(9378), 111–117. |
| [38] | Blanchet NJ, Fink G, Osei-Akoto I. The effect of Ghana's National Health Insurance Scheme on health care utilisation. Ghana Med J. 2012, 46(2), 76–84. |
APA Style
Salami, L., Mongbo, V., Kpozehouen, A., Makin, Y. M. U., Kohoun, R., et al. (2026). Fee Variability and Equity in Primary Health Care Facilities in Benin, 2025. International Journal of Health Economics and Policy, 11(2), 96-110. https://doi.org/10.11648/j.hep.20261102.14
ACS Style
Salami, L.; Mongbo, V.; Kpozehouen, A.; Makin, Y. M. U.; Kohoun, R., et al. Fee Variability and Equity in Primary Health Care Facilities in Benin, 2025. Int. J. Health Econ. Policy 2026, 11(2), 96-110. doi: 10.11648/j.hep.20261102.14
@article{10.11648/j.hep.20261102.14,
author = {Lamidhi Salami and Virginie Mongbo and Alphonse Kpozehouen and Yafou Mauricette Ursule Makin and Rodrigue Kohoun and Ali Imorou Bah Chabi and Ghislain Emmanuel Sopoh},
title = {Fee Variability and Equity in Primary Health Care Facilities in Benin, 2025},
journal = {International Journal of Health Economics and Policy},
volume = {11},
number = {2},
pages = {96-110},
doi = {10.11648/j.hep.20261102.14},
url = {https://doi.org/10.11648/j.hep.20261102.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.hep.20261102.14},
abstract = {Introduction: In Benin, where out-of-pocket payment constitutes the primary healthcare financing mechanism, the fee-setting practices of First Contact Health Facilities (FCHFs) directly condition financial access to care for the population. This study aims to document the regulatory framework and pricing practices in Beninese FCHFs and to analyse their relationships with the socio-economic characteristics of health districts. Methods: A descriptive and analytical cross-sectional study was conducted in 2025 using fee schedules from 28 of the 34 health districts. Four categories of services were analysed: clinical and technical procedures (n=59), biological laboratory investigations (n=74), medical imaging examinations (n=4), and specialist procedures (n=17, Cotonou only). Tariffs were stratified by area type (urban/rural) and triangulated with departmental poverty rates, FCHF attendance rates, and the share of community-based financing. A Pearson correlation coefficient was calculated between poverty and fee levels. Results: No legal instrument governed FCHF fee-setting. Childbirth exhibited the highest dispersion (CV=94.46%; range: 885–15,000 FCFA). The mean fee for a medical consultation was 1,571 ± 535 FCFA in urban areas versus 1,118 ± 402 FCFA in rural areas, a differential of 40.5%. Certain highly impoverished rural districts maintained fees above the national average. A moderate but statistically significant negative correlation was observed between the departmental poverty rate and the medical consultation fee (r=−0.651; p=0.001). Own revenues of FCHFs accounted for 97.4% of their resources. Conclusion: Fee-setting in Beninese FCHFs relies on informal mechanisms that generate inequities in access to care. The ongoing reforms in the health sector represent an opportunity to establish equitable fee schedules, grounded in the socio-economic realities of the population, the principles of primary health care, and coupled with social protection mechanisms for vulnerable households.},
year = {2026}
}
TY - JOUR T1 - Fee Variability and Equity in Primary Health Care Facilities in Benin, 2025 AU - Lamidhi Salami AU - Virginie Mongbo AU - Alphonse Kpozehouen AU - Yafou Mauricette Ursule Makin AU - Rodrigue Kohoun AU - Ali Imorou Bah Chabi AU - Ghislain Emmanuel Sopoh Y1 - 2026/05/21 PY - 2026 N1 - https://doi.org/10.11648/j.hep.20261102.14 DO - 10.11648/j.hep.20261102.14 T2 - International Journal of Health Economics and Policy JF - International Journal of Health Economics and Policy JO - International Journal of Health Economics and Policy SP - 96 EP - 110 PB - Science Publishing Group SN - 2578-9309 UR - https://doi.org/10.11648/j.hep.20261102.14 AB - Introduction: In Benin, where out-of-pocket payment constitutes the primary healthcare financing mechanism, the fee-setting practices of First Contact Health Facilities (FCHFs) directly condition financial access to care for the population. This study aims to document the regulatory framework and pricing practices in Beninese FCHFs and to analyse their relationships with the socio-economic characteristics of health districts. Methods: A descriptive and analytical cross-sectional study was conducted in 2025 using fee schedules from 28 of the 34 health districts. Four categories of services were analysed: clinical and technical procedures (n=59), biological laboratory investigations (n=74), medical imaging examinations (n=4), and specialist procedures (n=17, Cotonou only). Tariffs were stratified by area type (urban/rural) and triangulated with departmental poverty rates, FCHF attendance rates, and the share of community-based financing. A Pearson correlation coefficient was calculated between poverty and fee levels. Results: No legal instrument governed FCHF fee-setting. Childbirth exhibited the highest dispersion (CV=94.46%; range: 885–15,000 FCFA). The mean fee for a medical consultation was 1,571 ± 535 FCFA in urban areas versus 1,118 ± 402 FCFA in rural areas, a differential of 40.5%. Certain highly impoverished rural districts maintained fees above the national average. A moderate but statistically significant negative correlation was observed between the departmental poverty rate and the medical consultation fee (r=−0.651; p=0.001). Own revenues of FCHFs accounted for 97.4% of their resources. Conclusion: Fee-setting in Beninese FCHFs relies on informal mechanisms that generate inequities in access to care. The ongoing reforms in the health sector represent an opportunity to establish equitable fee schedules, grounded in the socio-economic realities of the population, the principles of primary health care, and coupled with social protection mechanisms for vulnerable households. VL - 11 IS - 2 ER -
Regional Institute of Public Health (IRSP), University of Abomey-Calavi, Ouidah, Benin
Regional Institute of Public Health (IRSP), University of Abomey-Calavi, Ouidah, Benin
Regional Institute of Public Health (IRSP), University of Abomey-Calavi, Ouidah, Benin
Regional Institute of Public Health (IRSP), University of Abomey-Calavi, Ouidah, Benin
General Secretary, Ministry of Health, Cotonou, Benin
Regional Institute of Public Health (IRSP), University of Abomey-Calavi, Ouidah, Benin
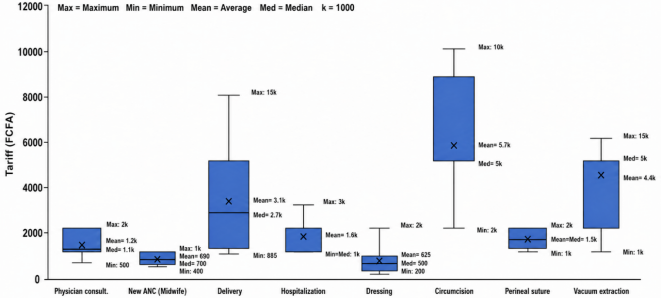
Figure 1. Central tendency and dispersion indicators of care fees in FCHFs in Benin, 2025.
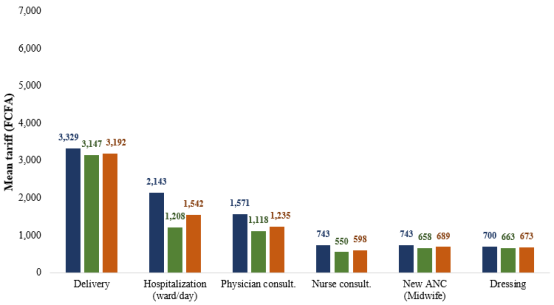
Figure 2. Distribution of fees by geographical area type in FCHFs in Benin, 2025.
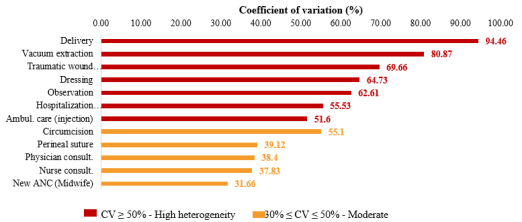
Figure 3. Coefficient of variation of fees for key clinical procedures in FCHFs in Benin, 2025.
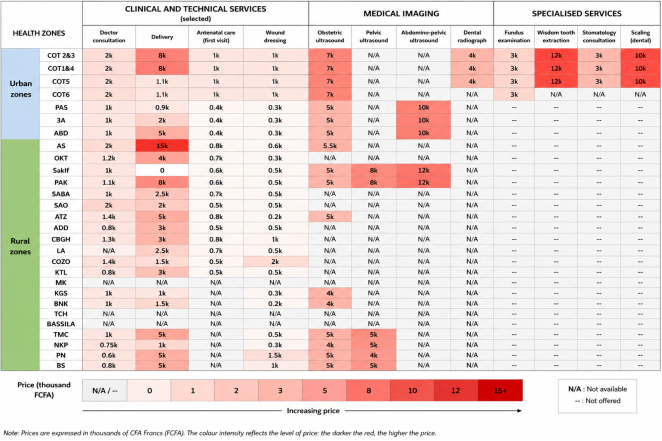
Figure 4. Mapping of fees applied by health district and by procedure in FCHFs in Benin, 2025.
Information

