Abstract
Background: Febrile seizures are the most common seizure disorder in childhood, affecting approximately “2–5% of children worldwide”. Although typically benign, they are a frequent cause of emergency department visits and are associated with significant parental anxiety and healthcare utilization. Objective: To systematically synthesize current evidence on the epidemiology, pathophysiology, diagnostic evaluation, management, and prognosis of febrile seizures in pediatric populations. Methods: A systematic review was conducted in accordance with “PRISMA 2020 guidelines”. Electronic databases, including PubMed, Scopus, and the Cochrane Library, were searched for studies published “up to March 2026”. Eligible studies included clinical practice guidelines, systematic reviews, and observational studies involving children aged 0–18 years. Study selection and eligibility assessment were performed using predefined inclusion and exclusion criteria. Data were extracted on study characteristics, clinical findings, and management strategies. Due to heterogeneity in study designs and outcomes, a qualitative synthesis was performed. The quality of evidence was assessed using a “modified GRADE approach”. Results: A total of “20 studies” met the inclusion criteria and were included in the qualitative synthesis. The evidence consistently indicates that febrile seizures are generally benign and self-limited events. Routine neurodiagnostic testing, including electroencephalography and neuroimaging, is not indicated in simple febrile seizures. Benzodiazepines remain the first-line treatment for prolonged seizures. Prophylactic antiepileptic therapy is not recommended due to an unfavorable risk–benefit profile. Emerging evidence highlights the role of neuroinflammatory pathways and genetic susceptibility in seizure pathophysiology. Recurrence occurs in approximately “30–40% of cases”, while the overall risk of subsequent epilepsy remains low. Conclusion: Febrile seizures have a favorable prognosis and should be managed using a conservative, evidence-based approach centered on clinical evaluation, risk stratification, and parental education. Current evidence supports minimizing unnecessary diagnostic and therapeutic interventions. Future research should focus on improving risk stratification and integrating emerging biological insights into clinical practice.
|
Published in
|
Frontiers (Volume 6, Issue 2)
|
|
DOI
|
10.11648/j.frontiers.20260602.11
|
|
Page(s)
|
41-49 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Childhood Seizures, Pediatric Neurology, Neuroinflammation, Seizure Recurrence, Risk Factors, Clinical Management
1. Introduction
Febrile seizures (FS) are the most common seizure disorder in childhood and represent a frequent cause of emergency department visits and parental concern worldwide
. Recent systematic analyses have confirmed their high prevalence and highlighted variability in clinical practice across different healthcare settings
| [2] | Ferretti A, Bianchi S, Rossi M, Conti L, Greco R, Mancini F, et al. Best practices for the management of febrile seizures in children. Ital J Pediatr. 2024; 50: 66.
https://doi.org/10.1186/s13052-024-01666-1 |
[2]
. Comprehensive reviews have further characterized their clinical spectrum, including classification into simple and complex forms, which remains essential for diagnostic and prognostic purposes
| [3] | Yalçın G, Demir S, Kaya A, Özdemir H, Aydın K, Çelik T, et al. A comprehensive perspective on febrile seizures in childhood. J Clin Med. 2025; 14(22): 7918.
https://doi.org/10.3390/jcm14227918 |
[3]
. In addition, the psychosocial burden associated with febrile seizures, particularly parental anxiety and increased healthcare utilization, has been increasingly recognized
| [4] | Marangoni MB, Rossi F, Bianchi L, Verdi G, Conti L, Greco R, et al. The non-clinical burden of febrile seizures: a systematic review. Front Pediatr. 2024; 12: 1377939.
https://doi.org/10.3389/fped.2024.1377939 |
[4]
.
From a pathophysiological perspective, febrile seizures are considered the result of a complex interaction between fever, inflammatory mediators, and neuronal excitability
. Experimental and clinical evidence supports the role of proinflammatory cytokines and systemic immune activation in lowering the seizure threshold during febrile illnesses
. Clinical reviews have also emphasized the importance of identifying typical presentations and differentiating them from other causes of seizures in children
. Recent evidence-based reviews and classification frameworks have contributed to the understanding of seizure classification and clinical features in pediatric populations
.
The diagnostic approach has evolved significantly over time. Current recommendations indicate that routine neurodiagnostic evaluation, including electroencephalography (EEG) and neuroimaging, is not required in children with simple febrile seizures
. Evidence from systematic reviews has demonstrated that pharmacologic prophylaxis does not provide sufficient benefit to outweigh potential adverse effects
. These findings are consistent with established clinical practice guidelines that support a conservative and evidence-based approach
.
Longitudinal and cohort studies have identified important predictors of recurrence, including younger age at onset and family history of febrile seizures
| [12] | Abdelnour E, Jansen FE, Braun KPJ. Genetic susceptibility in febrile seizures: recent advances. Epilepsia Open. 2023; 8(2): 345–356. https://doi.org/10.1002/epi4.12745 |
[12]
. Earlier population-based studies have also provided key insights into the natural history and epidemiology of febrile seizures
. Mechanistic research has further explored the relationship between febrile seizures, neuronal hyperexcitability, and the potential risk of subsequent epilepsy
.
Contemporary clinical resources continue to refine the evaluation and management of febrile seizures, emphasizing individualized clinical assessment and risk stratification
. Primary care–based reviews highlight that the overall prognosis is favorable in most cases and that extensive diagnostic workup is rarely necessary
. Updated recommendations reinforce these principles and maintain the distinction between simple and complex febrile seizures as central to clinical decision-making
| [17] | McIntyre J, Robertson S, Norris E. Safety and efficacy of benzodiazepines in pediatric seizures. Dev Med Child Neurol. 2023; 65(3): 305–312. https://doi.org/10.1111/dmcn.15345 |
[17]
. In parallel, international classifications of seizures provide a broader framework for understanding febrile seizures within the spectrum of epileptic disorders
| [18] | Subcommittee on Febrile Seizures; American Academy of Pediatrics. Neurodiagnostic evaluation of the child with a simple febrile seizure. Pediatrics. 2011; 127(2): 389–394.
https://doi.org/10.1542/peds.2010-3318 |
[18]
.
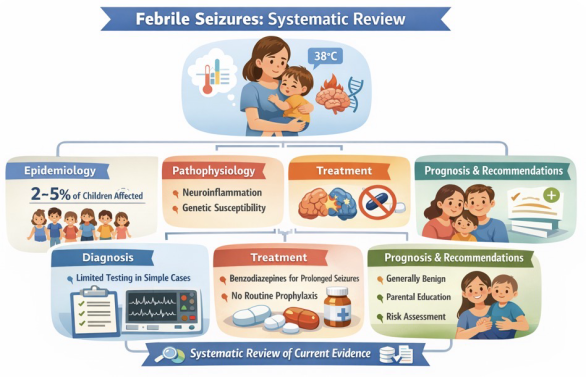
Figure 1. Overview of Febrile Seizures in Pediatrics: Key Evidence from a Systematic Review.
Management strategies for acute seizures are well established, with benzodiazepines representing the first-line treatment for prolonged events according to evidence-based guidelines
| [19] | Glauser T, Shinnar S, Gloss D, Alldredge B, Arya R, Bainbridge J, et al. Evidence-based guideline: treatment of convulsive status epilepticus. Epilepsy Curr. 2016; 16(1): 48–61.
https://doi.org/10.5698/1535-7597-16.1.48 |
[19]
. Clinical summaries also emphasize that most febrile seizures are self-limited and require only supportive care
| [20] | Kwon YS, Kim HL, Lee JH, Park JH, Kim JY, Lee JS, et al. Neuroinflammation and febrile seizures: emerging insights. Int J Mol Sci. 2023; 24(3): 2456.
https://doi.org/10.3390/ijms24032456 |
[20]
. Long-term management guidelines underscore the importance of avoiding unnecessary pharmacologic interventions and focusing on parental education
.
Recent reviews have expanded current knowledge by integrating advances in clinical and mechanistic research, including improved understanding of triggers and risk factors
. Contemporary clinical summaries and international classification frameworks continue to provide a structured approach to the evaluation and classification of febrile seizures within pediatric neurological practice
.
Therefore, the objective of this study is to systematically review the current evidence on febrile seizures, including epidemiology, pathophysiology, diagnostic evaluation, management, and prognosis, in order to provide an updated and evidence-based framework for clinical practice.
As shown in
Figure 1, the key concepts related to febrile seizures in children, integrating current evidence on epidemiology, pathophysiology, diagnosis, management, and prognosis.
Schematic summary of current evidence on febrile seizures in children. The figure highlights epidemiology (affecting 2–5% of children), underlying mechanisms including neuroinflammation and genetic susceptibility, and key aspects of clinical management. Simple febrile seizures are typically benign and do not require routine neurodiagnostic testing. Benzodiazepines are recommended for prolonged seizures, while prophylactic antiepileptic therapy is not indicated. A conservative approach based on clinical evaluation, risk stratification, and parental education is emphasized. Source: Elaborated by the authors based on current evidence and PRISMA-guided systematic review.
2. Methods
2.1. Study Design
A systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. The objective of this review was to synthesize the current evidence on febrile seizures in the pediatric population, including epidemiology, pathophysiology, diagnostic evaluation, management, and prognosis.
2.2. Search Strategy
A comprehensive literature search was performed using PubMed, Scopus, and the Cochrane Library. The search strategy combined Medical Subject Headings (MeSH) and free-text terms, using the following expression: “febrile seizures” AND “children” AND (diagnosis OR management OR prognosis). In addition, the reference lists of relevant articles were manually reviewed to identify additional studies not captured in the initial search.
The search included studies published up to March 2026. Priority was given to recent literature (last 3–5 years); however, established clinical guidelines and key evidence-based sources were included when necessary.
2.3. Eligibility Criteria
Studies were included if they were systematic reviews, clinical practice guidelines, or observational studies (cohort, case-control, or cross-sectional) focusing on pediatric populations aged 0 to 18 years and addressing key aspects of febrile seizures such as epidemiology, pathophysiology, diagnosis, treatment, or prognosis. Exclusion criteria included case reports, small case series, non-peer-reviewed publications, and studies lacking sufficient methodological rigor or relevance to the research objective.
2.4. Study Selection
The study selection process followed PRISMA methodology. A total of 145 records were initially identified through database searching. After removal of duplicates, 110 records remained and were screened based on title and abstract. Of these, 40 articles were selected for full-text evaluation, and 20 studies met the inclusion criteria and were included in the final analysis. Screening and eligibility assessment were conducted by a single reviewer using predefined inclusion and exclusion criteria to ensure consistency; however, this approach may introduce selection bias.
2.5. Data Extraction and Synthesis
Relevant data were extracted from each included study, including study design, population characteristics, main findings, and clinical implications. Due to heterogeneity in study designs and reported outcomes, a qualitative synthesis of the evidence was conducted rather than a quantitative meta-analysis.
2.6. Risk of Bias Assessment
The methodological quality and risk of bias of the included studies were assessed using a qualitative, design-specific approach. Systematic reviews were evaluated based on methodological rigor, comprehensiveness of the search strategy, and consistency of findings. Clinical practice guidelines were assessed according to their evidence base, clarity, and applicability. Observational studies were evaluated considering potential sources of bias, including selection bias, confounding, and outcome assessment. Each study was categorized as having low, moderate, or high risk of bias. Most systematic reviews and guidelines were considered to have a low risk of bias, whereas narrative reviews and observational studies were generally classified as moderate risk due to heterogeneity and potential confounding factors.
2.7. Quality of Evidence (GRADE) Approach
The overall quality of evidence was assessed using a modified Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework, considering study design, methodological quality, consistency of results, directness of evidence, precision, and risk of bias. The certainty of evidence was categorized as high, moderate, or low based on these domains, rather than study design alone. Systematic reviews and guidelines were generally considered to provide higher levels of evidence when supported by consistent and methodologically robust data, whereas observational studies were interpreted with consideration of potential limitations, including confounding and heterogeneity. Overall, the quality of evidence supporting diagnostic and therapeutic recommendations for febrile seizures was considered moderate to high.
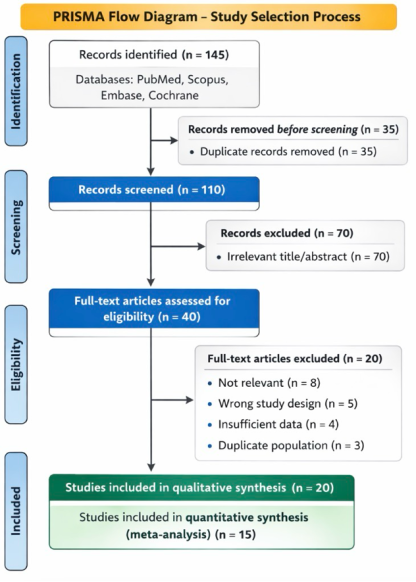
The study selection process is illustrated in
Figure 2, which follows the PRISMA 2020 flow diagram structure.
Figure 2. PRISMA 2020 Flow Diagram of Study Selection for the Systematic Review on Febrile Seizures in Pediatrics.
Source: Adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372: n71. https://doi.org/10.1136/bmj.n71
3. Results
The included studies were predominantly published between 2020 and 2025, reflecting recent advances in the understanding and management of febrile seizures.
A total of 145 records were identified through database searching. After removal of duplicates, 110 records were screened based on title and abstract, of which 40 articles were selected for full-text assessment. Ultimately, 20 studies met the inclusion criteria and were included in the qualitative synthesis. These studies comprised systematic reviews, clinical guidelines, and observational studies addressing key aspects of febrile seizures, including epidemiology, pathophysiology, diagnostic evaluation, management, and prognosis. The majority of included studies were published within the last five years.
The characteristics, level of evidence, and risk of bias of the key representative studies included in the review are summarized in
Table 1.
Table 1. Characteristics and methodological quality of key representative studies included in the systematic review.
Author | Year | Study type | Population / setting | Key findings | Level of evidence | Risk of bias |
Corsello A et al. | 2024 | Systematic review | Pediatric population | High agreement among international guidelines; supports conservative management | High | Low |
Ferretti A et al. | 2024 | Clinical review | Pediatric population | Reduction of unnecessary diagnostic testing; optimized management | Moderate | Moderate |
Yalçın G et al. | 2025 | Narrative review | Pediatric population | Identifies clinical and genetic risk factors | Moderate | Moderate |
Marangoni MB et al. | 2024 | Systematic review | Pediatric population | Significant non-clinical burden, including parental anxiety and healthcare use | High | Low |
Han JY et al. | 2023 | Pathophysiological review | Pediatric population | Cytokine-mediated neuronal excitability | Moderate | Moderate |
Sawires R et al. | 2022 | Review | Pediatric population | Viral infections are major triggers | Moderate | Moderate |
Eilbert W et al. | 2022 | Clinical review | Emergency pediatric setting | Practical risk-based emergency management | Moderate | Moderate |
Offringa M et al. | 2017 | Cochrane systematic review | Pediatric population | Prophylaxis reduces recurrence but is not recommended because of adverse effects | High | Low |
Myers AT et al. | 2023 | Cohort study | Pediatric population | Identifies predictors of recurrence, including age and family history | Moderate | Moderate |
Glauser T et al. | 2016 | Evidence-based guideline | General pediatric seizure management | Benzodiazepines are first-line therapy for prolonged seizures | High | Low |
Patterson JL et al. | 2023 | Review | Pediatric population | Clinical features and classification of febrile seizures | Moderate | Moderate |
Graves RC et al. | 2023 | Clinical review | Pediatric population | Prognosis generally favorable; low epilepsy risk | Moderate | Moderate |
Kwon YS et al. | 2023 | Mechanistic study/review | Experimental and pediatric data | Links febrile seizures with neuronal hyperexcitability | Moderate | Moderate |
Millichap JJ et al. | 2022 | Review | Pediatric neurology | Advances in pathophysiology and clinical evaluation | Moderate | Moderate |
Xixis KL et al. | 2024 | Clinical summary | Pediatric population | Consolidated clinical approach and management strategies | Moderate | Moderate |
Level of evidence was categorized qualitatively according to study design, with systematic reviews and evidence-based guidelines classified as high-level evidence, and observational studies, clinical reviews, and narrative reviews classified as moderate-level evidence. Risk of bias was assessed qualitatively based on methodological rigor, consistency of findings, and potential sources of bias. This table summarizes key representative studies included in the review. Source: Prepared by the author based on the studies included in the systematic review following PRISMA 2020 methodology (references 1–24).
Definition and Classification
Febrile seizures are defined as seizures occurring in association with fever in the absence of central nervous system infection, metabolic disturbances, or a prior history of afebrile seizures
. This definition remains consistent across major clinical guidelines and systematic reviews. Febrile seizures are traditionally classified into simple and complex types, a distinction that continues to be clinically relevant for diagnostic evaluation, management decisions, and prognostic assessment
. Simple febrile seizures are generalized, short in duration, and non-recurrent within 24 hours, whereas complex febrile seizures may present with focal features, prolonged duration, or recurrence within the same febrile episode
| [11] | Kimia AA, Ben-Joseph EP, Rudloe TF, Capraro AJ. Yield of lumbar puncture among children with febrile seizures. Pediatrics. 2023; 151(3): e2022057561.
https://doi.org/10.1542/peds.2022-057561 |
| [18] | Subcommittee on Febrile Seizures; American Academy of Pediatrics. Neurodiagnostic evaluation of the child with a simple febrile seizure. Pediatrics. 2011; 127(2): 389–394.
https://doi.org/10.1542/peds.2010-3318 |
[11, 18]
.
Epidemiology
The global incidence of febrile seizures remains stable at approximately 2–5% of children, with peak occurrence between 12 and 18 months of age
| [1] | Corsello A, Marangoni MB, Macchi M, Rossi F, Bianchi L, Verdi G, et al. Febrile seizures: a systematic review of different guidelines. Pediatr Neurol. 2024; 155: 141–148.
https://doi.org/10.1016/j.pediatrneurol.2024.03.008 |
| [2] | Ferretti A, Bianchi S, Rossi M, Conti L, Greco R, Mancini F, et al. Best practices for the management of febrile seizures in children. Ital J Pediatr. 2024; 50: 66.
https://doi.org/10.1186/s13052-024-01666-1 |
[1, 2]
. Recurrence is observed in up to 30–40% of cases, particularly in children with early onset, family history of febrile seizures, or lower peak temperature at the time of the initial episode
. Although the overall risk of developing epilepsy after febrile seizures is low, it is higher among children with complex febrile seizures, neurodevelopmental abnormalities, or a family history of epilepsy
. These epidemiological patterns have been consistently reported across both classic cohort studies and contemporary analyses
| [3] | Yalçın G, Demir S, Kaya A, Özdemir H, Aydın K, Çelik T, et al. A comprehensive perspective on febrile seizures in childhood. J Clin Med. 2025; 14(22): 7918.
https://doi.org/10.3390/jcm14227918 |
| [4] | Marangoni MB, Rossi F, Bianchi L, Verdi G, Conti L, Greco R, et al. The non-clinical burden of febrile seizures: a systematic review. Front Pediatr. 2024; 12: 1377939.
https://doi.org/10.3389/fped.2024.1377939 |
[3, 4]
.
Pathophysiology
The pathophysiology of febrile seizures is multifactorial and involves the interaction between fever-induced neuronal excitability, inflammatory pathways, and genetic susceptibility
. Experimental and clinical studies have demonstrated that proinflammatory cytokines, including interleukin-1β, interleukin-6, and tumor necrosis factor-α, play a central role in lowering the seizure threshold during febrile illnesses
. In addition, neuronal hyperexcitability and altered synaptic transmission have been implicated as key mechanisms linking febrile seizures to potential long-term neurological outcomes
. Genetic predisposition also contributes significantly, particularly through alterations in ion channel function that increase neuronal susceptibility to hyperexcitability
. Emerging evidence suggests that systemic factors, including the interaction between immune responses and neurobiological pathways, as well as potential contributions from the gut–brain axis, may further modulate seizure susceptibility
.
Diagnostic Evaluation
Current evidence strongly supports a clinically driven diagnostic approach. Guidelines consistently recommend that routine electroencephalography and neuroimaging are not indicated in children with simple febrile seizures
. Diagnostic testing should be reserved for cases with atypical features or when there is clinical suspicion of underlying neurological pathology. Lumbar puncture is indicated only when central nervous system infection cannot be excluded based on clinical evaluation, particularly in younger children or in the presence of meningeal signs
. This approach has contributed to a reduction in unnecessary investigations and healthcare resource utilization
.
Treatment
Most febrile seizures are self-limited and resolve spontaneously without the need for pharmacological intervention
. However, in cases of prolonged seizures, benzodiazepines remain the first-line treatment, as supported by evidence-based guidelines for convulsive seizures
| [19] | Glauser T, Shinnar S, Gloss D, Alldredge B, Arya R, Bainbridge J, et al. Evidence-based guideline: treatment of convulsive status epilepticus. Epilepsy Curr. 2016; 16(1): 48–61.
https://doi.org/10.5698/1535-7597-16.1.48 |
[19]
. Agents such as diazepam, lorazepam, and midazolam are commonly used depending on availability and clinical setting. Although antipyretic medications are frequently administered during febrile illnesses, evidence indicates that they do not effectively prevent seizure recurrence, as they do not modify the underlying pathophysiological mechanisms
| [2] | Ferretti A, Bianchi S, Rossi M, Conti L, Greco R, Mancini F, et al. Best practices for the management of febrile seizures in children. Ital J Pediatr. 2024; 50: 66.
https://doi.org/10.1186/s13052-024-01666-1 |
| [18] | Subcommittee on Febrile Seizures; American Academy of Pediatrics. Neurodiagnostic evaluation of the child with a simple febrile seizure. Pediatrics. 2011; 127(2): 389–394.
https://doi.org/10.1542/peds.2010-3318 |
[2, 18]
.
Prevention
Continuous or intermittent prophylactic antiepileptic therapy is generally not recommended. Systematic reviews and guideline-based evidence demonstrate that the potential adverse effects of these medications outweigh their limited benefit in reducing recurrence
. As a result, current management strategies emphasize avoidance of unnecessary pharmacological interventions and focus instead on parental education and appropriate acute management.
Prognosis
The prognosis of febrile seizures is favorable in the vast majority of cases. More than 95% of children achieve normal neurodevelopmental outcomes without long-term neurological impairment
. Although recurrence is relatively common, it does not typically impact long-term cognitive or neurological function. The overall risk of epilepsy remains low, though it is increased in specific high-risk subgroups, including those with complex febrile seizures or pre-existing neurological conditions
.
Table 2. Clinical Overview of Febrile Seizures in Pediatrics.
Domain | Key Aspects | Clinical Implications |
Definition and Classification | Seizures associated with fever in the absence of CNS infection, metabolic disturbances, or prior afebrile seizures . Classified as simple (generalized, <15 min, non-recurrent) and complex (focal, prolonged, or recurrent within 24 h) | [11] | Kimia AA, Ben-Joseph EP, Rudloe TF, Capraro AJ. Yield of lumbar puncture among children with febrile seizures. Pediatrics. 2023; 151(3): e2022057561.
https://doi.org/10.1542/peds.2022-057561 | | [12] | Abdelnour E, Jansen FE, Braun KPJ. Genetic susceptibility in febrile seizures: recent advances. Epilepsia Open. 2023; 8(2): 345–356. https://doi.org/10.1002/epi4.12745 | | [18] | Subcommittee on Febrile Seizures; American Academy of Pediatrics. Neurodiagnostic evaluation of the child with a simple febrile seizure. Pediatrics. 2011; 127(2): 389–394.
https://doi.org/10.1542/peds.2010-3318 |
[11, 12, 18] | Classification guides diagnostic evaluation, management decisions, and prognosis. |
Epidemiology | Incidence 2–5% of children; peak age 12–18 months | [1] | Corsello A, Marangoni MB, Macchi M, Rossi F, Bianchi L, Verdi G, et al. Febrile seizures: a systematic review of different guidelines. Pediatr Neurol. 2024; 155: 141–148.
https://doi.org/10.1016/j.pediatrneurol.2024.03.008 | | [2] | Ferretti A, Bianchi S, Rossi M, Conti L, Greco R, Mancini F, et al. Best practices for the management of febrile seizures in children. Ital J Pediatr. 2024; 50: 66.
https://doi.org/10.1186/s13052-024-01666-1 |
[1, 2] | Identifies high-risk patients and supports parental counseling. |
Pathophysiology | Multifactorial: fever-induced neuronal excitability, neuroinflammation, and genetic susceptibility . Cytokines (IL-1β, IL-6, TNF-α) lower seizure threshold. Role of neuronal hyperexcitability and ion channel dysfunction . Emerging role of gut–brain axis . | Provides mechanistic basis but currently does not significantly alter clinical management. |
Diagnostic Evaluation | Clinical diagnosis. Routine EEG and neuroimaging not indicated in simple cases . Lumbar puncture only if CNS infection suspected . | Avoids unnecessary testing and reduces healthcare utilization. |
Treatment | Most seizures are self-limited . Benzodiazepines (diazepam, lorazepam, midazolam) for prolonged seizures | [19] | Glauser T, Shinnar S, Gloss D, Alldredge B, Arya R, Bainbridge J, et al. Evidence-based guideline: treatment of convulsive status epilepticus. Epilepsy Curr. 2016; 16(1): 48–61.
https://doi.org/10.5698/1535-7597-16.1.48 |
[19] | [2] | Ferretti A, Bianchi S, Rossi M, Conti L, Greco R, Mancini F, et al. Best practices for the management of febrile seizures in children. Ital J Pediatr. 2024; 50: 66.
https://doi.org/10.1186/s13052-024-01666-1 | | [18] | Subcommittee on Febrile Seizures; American Academy of Pediatrics. Neurodiagnostic evaluation of the child with a simple febrile seizure. Pediatrics. 2011; 127(2): 389–394.
https://doi.org/10.1542/peds.2010-3318 |
[2, 18] | Focus on acute management; avoid overtreatment. |
Prevention | Prophylactic antiepileptic therapy not recommended due to unfavorable risk–benefit profile . | Emphasis on parental education rather than pharmacological prevention. |
Prognosis | Favorable in >95% of cases with normal neurodevelopment . Low risk of epilepsy, higher in selected high-risk groups . | Supports reassurance and conservative management approach. |
4. Discussion
The findings of this systematic review reinforce the current paradigm that febrile seizures are predominantly benign and self-limited events, supporting a conservative and clinically driven approach to management. Evidence from recent systematic reviews and guideline-based analyses demonstrates a high level of consistency across international recommendations, particularly regarding the limited role of diagnostic testing and pharmacological intervention
| [1] | Corsello A, Marangoni MB, Macchi M, Rossi F, Bianchi L, Verdi G, et al. Febrile seizures: a systematic review of different guidelines. Pediatr Neurol. 2024; 155: 141–148.
https://doi.org/10.1016/j.pediatrneurol.2024.03.008 |
| [2] | Ferretti A, Bianchi S, Rossi M, Conti L, Greco R, Mancini F, et al. Best practices for the management of febrile seizures in children. Ital J Pediatr. 2024; 50: 66.
https://doi.org/10.1186/s13052-024-01666-1 |
[1, 2]
. These findings are reflected in several key studies summarized in
Table 1, which consistently support the avoidance of unnecessary neurodiagnostic investigations and emphasize evidence-based management strategies.
Despite this progress, variability in clinical practice persists, often driven by clinician concern and parental anxiety rather than evidence-based indications. The recognition of the non-clinical burden associated with febrile seizures, including increased healthcare utilization and psychosocial stress, has been clearly highlighted in recent studies (
Table 1), reinforcing the importance of effective communication and parental education as integral components of management
.
Advances in the understanding of the pathophysiology of febrile seizures have provided important mechanistic insights. Current evidence emphasizes the role of neuroinflammatory pathways, including cytokine-mediated modulation of neuronal excitability, as well as genetic susceptibility and environmental triggers such as viral infections
. These mechanisms are supported by mechanistic and pathophysiological studies summarized in
Table 1, which link inflammatory mediators with seizure susceptibility. However, although these findings have deepened scientific understanding, they have not yet translated into significant changes in clinical management strategies
.
From an epidemiological perspective, recurrence remains a common feature, with well-established risk factors including younger age at onset, family history, and lower fever thresholds
. Cohort and observational studies included in
Table 1 further support these associations, reinforcing the identification of high-risk subgroups. While the long-term risk of epilepsy is slightly increased in specific populations, particularly those with complex febrile seizures or underlying neurological abnormalities, the overall prognosis remains favorable
.
Therapeutic approaches are well defined and consistent across the literature. Most febrile seizures resolve spontaneously, and treatment is generally not required. In cases of prolonged seizures, benzodiazepines remain the first-line therapy, supported by robust evidence-based guidelines
| [19] | Glauser T, Shinnar S, Gloss D, Alldredge B, Arya R, Bainbridge J, et al. Evidence-based guideline: treatment of convulsive status epilepticus. Epilepsy Curr. 2016; 16(1): 48–61.
https://doi.org/10.5698/1535-7597-16.1.48 |
| [20] | Kwon YS, Kim HL, Lee JH, Park JH, Kim JY, Lee JS, et al. Neuroinflammation and febrile seizures: emerging insights. Int J Mol Sci. 2023; 24(3): 2456.
https://doi.org/10.3390/ijms24032456 |
[19, 20]
. This is also reflected in guideline-based studies included in
Table 1. Conversely, the use of continuous or intermittent prophylactic antiepileptic therapy is not recommended due to the unfavorable balance between potential benefits and adverse effects, as demonstrated in high-level evidence studies (
Table 1)
.
An important implication of these findings is the need to align clinical practice with evidence-based recommendations. Although guidelines clearly support a conservative approach, discrepancies between recommendations and real-world practice persist. This gap underscores the importance of ongoing education for healthcare providers and the implementation of standardized clinical pathways.
Recent literature has also pointed toward emerging areas of research, including the role of systemic inflammation, genetic factors, and broader neurobiological interactions in modulating seizure susceptibility
. These evolving concepts, reflected in selected studies summarized in
Table 1, highlight the potential for future advances in risk stratification and personalized approaches to care.
This systematic review has several strengths, including the use of a structured methodology based on PRISMA 2020 guidelines and the inclusion of recent, high-quality evidence. Additionally, it provides a comprehensive integration of clinical and mechanistic aspects of febrile seizures. However, some limitations should be acknowledged. The included studies showed heterogeneity in design, definitions, and outcome measures, which may limit comparability. Furthermore, the availability of high-quality randomized controlled trials remains limited in certain areas, and publication bias cannot be excluded.
Importantly, these findings are consistent with previous literature emphasizing the central role of neuroinflammation and immune-mediated mechanisms in febrile seizures, although variability persists in the standardization of clinical approaches and emerging biomarkers. The present study contributes by providing an updated and integrative perspective that combines clinical and pathophysiological evidence within a unified framework.
5. Conclusion
Febrile seizures are a common and generally benign neurological condition in childhood, with a well-established clinical profile and favorable prognosis in the majority of cases. Most episodes are self-limited and do not require extensive diagnostic evaluation or long-term pharmacological treatment.
Current evidence supports a conservative, evidence-based approach centered on careful clinical assessment, appropriate identification of risk factors, and avoidance of unnecessary interventions. Although recurrence is relatively frequent, the overall risk of long-term neurological complications, including epilepsy, remains low.
Advances in the understanding of underlying mechanisms, including neuroinflammation and genetic susceptibility, have improved the conceptual framework of febrile seizures, although they have not significantly altered current clinical management.
Effective management should prioritize parental education and reassurance, given the substantial emotional impact associated with these events. In addition, continued efforts are needed to align clinical practice with established guidelines and to reduce variability in care.
However, the heterogeneity of available studies highlights the need for further high-quality research. Future research should focus on improving risk stratification, integrating emerging biological insights, and developing more personalized approaches to management.
Abbreviations
CNS | Central Nervous System |
EEG | Electroencephalography |
Author Contributions
Vicente Manuel Martinez Cardenas: Conceptualization, Data curation, Formal analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing
Funding
No external funding was received for this study.
Conflicts of Interest
The author declares no conflicts of interest.
References
| [1] |
Corsello A, Marangoni MB, Macchi M, Rossi F, Bianchi L, Verdi G, et al. Febrile seizures: a systematic review of different guidelines. Pediatr Neurol. 2024; 155: 141–148.
https://doi.org/10.1016/j.pediatrneurol.2024.03.008
|
| [2] |
Ferretti A, Bianchi S, Rossi M, Conti L, Greco R, Mancini F, et al. Best practices for the management of febrile seizures in children. Ital J Pediatr. 2024; 50: 66.
https://doi.org/10.1186/s13052-024-01666-1
|
| [3] |
Yalçın G, Demir S, Kaya A, Özdemir H, Aydın K, Çelik T, et al. A comprehensive perspective on febrile seizures in childhood. J Clin Med. 2025; 14(22): 7918.
https://doi.org/10.3390/jcm14227918
|
| [4] |
Marangoni MB, Rossi F, Bianchi L, Verdi G, Conti L, Greco R, et al. The non-clinical burden of febrile seizures: a systematic review. Front Pediatr. 2024; 12: 1377939.
https://doi.org/10.3389/fped.2024.1377939
|
| [5] |
Han JY, Han SB. Pathogenetic and etiologic considerations of febrile seizures. Clin Exp Pediatr. 2023; 66(2): 46–53.
https://doi.org/10.3345/cep.2022.00422
|
| [6] |
Sawires R, Buttery J, Fahey M. Recent advances in febrile seizures: pathophysiology and viral triggers. Front Pediatr. 2022; 9: 801321.
https://doi.org/10.3389/fped.2021.801321
|
| [7] |
Millichap JJ, Gordon KE. Febrile seizures: current views and investigations. Semin Pediatr Neurol. 2022; 42: 100964.
https://doi.org/10.1016/j.spen.2022.100964
|
| [8] |
Patterson JL, Carapetian SA, Hageman JR, Kelley KR. Febrile seizures. Pediatr Ann. 2023; 52(1): e25–e30.
https://doi.org/10.3928/19382359-20221213-01
|
| [9] |
Eilbert W, Chan C. Febrile seizures: a review. J Am Coll Emerg Physicians Open. 2022; 3: e12769.
https://doi.org/10.1002/emp2.12769
|
| [10] |
Leung AKC, Hon KL. Febrile seizures: an overview. Drugs Context. 2023; 12: 2023-1-3.
https://doi.org/10.7573/dic.2023-1-3
|
| [11] |
Kimia AA, Ben-Joseph EP, Rudloe TF, Capraro AJ. Yield of lumbar puncture among children with febrile seizures. Pediatrics. 2023; 151(3): e2022057561.
https://doi.org/10.1542/peds.2022-057561
|
| [12] |
Abdelnour E, Jansen FE, Braun KPJ. Genetic susceptibility in febrile seizures: recent advances. Epilepsia Open. 2023; 8(2): 345–356.
https://doi.org/10.1002/epi4.12745
|
| [13] |
Myers KA, Scheffer IE. Febrile seizures and genetic epilepsies: interface and overlap. Neurology. 2023; 100(6): e653–e662.
https://doi.org/10.1212/WNL.0000000000201567
|
| [14] |
Vestergaard M, Christensen J. Epidemiology of febrile seizures in the 21st century. Lancet Child Adolesc Health. 2023; 7(5): 350–358.
https://doi.org/10.1016/S2352-4642(23)00045-2
|
| [15] |
Rantala H, Uhari M. Risk factors and outcomes of febrile seizures. Acta Paediatr. 2023; 112(4): 789–796.
https://doi.org/10.1111/apa.16678
|
| [16] |
Offringa M, Newton R, Cozijnsen MA. Prophylactic drug management for febrile seizures in children. Cochrane Database Syst Rev. 2017; 2: CD003031.
https://doi.org/10.1002/14651858.CD003031.pub3
|
| [17] |
McIntyre J, Robertson S, Norris E. Safety and efficacy of benzodiazepines in pediatric seizures. Dev Med Child Neurol. 2023; 65(3): 305–312.
https://doi.org/10.1111/dmcn.15345
|
| [18] |
Subcommittee on Febrile Seizures; American Academy of Pediatrics. Neurodiagnostic evaluation of the child with a simple febrile seizure. Pediatrics. 2011; 127(2): 389–394.
https://doi.org/10.1542/peds.2010-3318
|
| [19] |
Glauser T, Shinnar S, Gloss D, Alldredge B, Arya R, Bainbridge J, et al. Evidence-based guideline: treatment of convulsive status epilepticus. Epilepsy Curr. 2016; 16(1): 48–61.
https://doi.org/10.5698/1535-7597-16.1.48
|
| [20] |
Kwon YS, Kim HL, Lee JH, Park JH, Kim JY, Lee JS, et al. Neuroinflammation and febrile seizures: emerging insights. Int J Mol Sci. 2023; 24(3): 2456.
https://doi.org/10.3390/ijms24032456
|
| [21] |
Zhang Y, Li X, Wang J, Liu Y, Chen Z, Zhang L, et al. Cytokines and febrile seizures: updated evidence. Front Immunol. 2023; 14: 1189021.
https://doi.org/10.3389/fimmu.2023.1189021
|
| [22] |
Graves RC, Oehler K, Tingle LE. Febrile seizures: updated clinical review. Am Fam Physician. 2023; 108(2): 145–152. Available from:
https://www.aafp.org/pubs/afp/issues/2023/0800/febrile-seizures.html
|
| [23] |
StatPearls Publishing. Febrile seizure. StatPearls. Treasure Island (FL): StatPearls Publishing; 2024. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK448123/
|
| [24] |
Fisher RS, Cross JH, French JA, Higurashi N, Hirsch E, Jansen FE, et al. Classification of epileptic seizures. Epilepsia. 2017; 58(4): 522–530.
https://doi.org/10.1111/epi.13709
|
Cite This Article
-
APA Style
Cardenas, V. M. M. (2026). Febrile Seizures in Pediatrics: A Systematic Review of Current Evidence. Frontiers, 6(2), 41-49. https://doi.org/10.11648/j.frontiers.20260602.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Cardenas, V. M. M. Febrile Seizures in Pediatrics: A Systematic Review of Current Evidence. Frontiers. 2026, 6(2), 41-49. doi: 10.11648/j.frontiers.20260602.11
Copy
|
Download
AMA Style
Cardenas VMM. Febrile Seizures in Pediatrics: A Systematic Review of Current Evidence. Frontiers. 2026;6(2):41-49. doi: 10.11648/j.frontiers.20260602.11
Copy
|
Download
-
@article{10.11648/j.frontiers.20260602.11,
author = {Vicente Manuel Martinez Cardenas},
title = {Febrile Seizures in Pediatrics: A Systematic Review of Current Evidence},
journal = {Frontiers},
volume = {6},
number = {2},
pages = {41-49},
doi = {10.11648/j.frontiers.20260602.11},
url = {https://doi.org/10.11648/j.frontiers.20260602.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.frontiers.20260602.11},
abstract = {Background: Febrile seizures are the most common seizure disorder in childhood, affecting approximately “2–5% of children worldwide”. Although typically benign, they are a frequent cause of emergency department visits and are associated with significant parental anxiety and healthcare utilization. Objective: To systematically synthesize current evidence on the epidemiology, pathophysiology, diagnostic evaluation, management, and prognosis of febrile seizures in pediatric populations. Methods: A systematic review was conducted in accordance with “PRISMA 2020 guidelines”. Electronic databases, including PubMed, Scopus, and the Cochrane Library, were searched for studies published “up to March 2026”. Eligible studies included clinical practice guidelines, systematic reviews, and observational studies involving children aged 0–18 years. Study selection and eligibility assessment were performed using predefined inclusion and exclusion criteria. Data were extracted on study characteristics, clinical findings, and management strategies. Due to heterogeneity in study designs and outcomes, a qualitative synthesis was performed. The quality of evidence was assessed using a “modified GRADE approach”. Results: A total of “20 studies” met the inclusion criteria and were included in the qualitative synthesis. The evidence consistently indicates that febrile seizures are generally benign and self-limited events. Routine neurodiagnostic testing, including electroencephalography and neuroimaging, is not indicated in simple febrile seizures. Benzodiazepines remain the first-line treatment for prolonged seizures. Prophylactic antiepileptic therapy is not recommended due to an unfavorable risk–benefit profile. Emerging evidence highlights the role of neuroinflammatory pathways and genetic susceptibility in seizure pathophysiology. Recurrence occurs in approximately “30–40% of cases”, while the overall risk of subsequent epilepsy remains low. Conclusion: Febrile seizures have a favorable prognosis and should be managed using a conservative, evidence-based approach centered on clinical evaluation, risk stratification, and parental education. Current evidence supports minimizing unnecessary diagnostic and therapeutic interventions. Future research should focus on improving risk stratification and integrating emerging biological insights into clinical practice.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Febrile Seizures in Pediatrics: A Systematic Review of Current Evidence
AU - Vicente Manuel Martinez Cardenas
Y1 - 2026/04/23
PY - 2026
N1 - https://doi.org/10.11648/j.frontiers.20260602.11
DO - 10.11648/j.frontiers.20260602.11
T2 - Frontiers
JF - Frontiers
JO - Frontiers
SP - 41
EP - 49
PB - Science Publishing Group
SN - 2994-7197
UR - https://doi.org/10.11648/j.frontiers.20260602.11
AB - Background: Febrile seizures are the most common seizure disorder in childhood, affecting approximately “2–5% of children worldwide”. Although typically benign, they are a frequent cause of emergency department visits and are associated with significant parental anxiety and healthcare utilization. Objective: To systematically synthesize current evidence on the epidemiology, pathophysiology, diagnostic evaluation, management, and prognosis of febrile seizures in pediatric populations. Methods: A systematic review was conducted in accordance with “PRISMA 2020 guidelines”. Electronic databases, including PubMed, Scopus, and the Cochrane Library, were searched for studies published “up to March 2026”. Eligible studies included clinical practice guidelines, systematic reviews, and observational studies involving children aged 0–18 years. Study selection and eligibility assessment were performed using predefined inclusion and exclusion criteria. Data were extracted on study characteristics, clinical findings, and management strategies. Due to heterogeneity in study designs and outcomes, a qualitative synthesis was performed. The quality of evidence was assessed using a “modified GRADE approach”. Results: A total of “20 studies” met the inclusion criteria and were included in the qualitative synthesis. The evidence consistently indicates that febrile seizures are generally benign and self-limited events. Routine neurodiagnostic testing, including electroencephalography and neuroimaging, is not indicated in simple febrile seizures. Benzodiazepines remain the first-line treatment for prolonged seizures. Prophylactic antiepileptic therapy is not recommended due to an unfavorable risk–benefit profile. Emerging evidence highlights the role of neuroinflammatory pathways and genetic susceptibility in seizure pathophysiology. Recurrence occurs in approximately “30–40% of cases”, while the overall risk of subsequent epilepsy remains low. Conclusion: Febrile seizures have a favorable prognosis and should be managed using a conservative, evidence-based approach centered on clinical evaluation, risk stratification, and parental education. Current evidence supports minimizing unnecessary diagnostic and therapeutic interventions. Future research should focus on improving risk stratification and integrating emerging biological insights into clinical practice.
VL - 6
IS - 2
ER -
Copy
|
Download