Abstract
Introduction: Guillain-Barre syndrome (GBS) faces many diagnostic and therapeutic challenges in sub-Saharan Africa, negatively impacting patient prognosis. The aim of this study was to describe the therapeutic and evolutionary modalities of GBS in the university hospitals of Ouagadougou, Burkina Faso. Patients and methods: This was a descriptive cross-sectional study with prospective data collection, conducted in the university hospitals of Ouagadougou (Yalgado Ouedraogo, Tengandogo, Bogodogo) from March 2018 to May 2022. Patients aged ˃ 16 years admitted for GBS according to the modified Brighton criteria were included. Clinical severity at the time of admission and at the end of hospitalization was assessed using the GBS Disability Score (GBSDS). Socio-demographic, clinical, therapeutic, and in-hospital progression data were analyzed. Results: A total of 79 patients were consecutively hospitalized for GBS, with a mean age of 38 years and a male-to-female ratio of 1.25. The mean time to admission was 22 days. The clinical picture consisted of hypo- or areflexic tetraparesis/plegia (100%) with respiratory muscle deficit (44.3%), cranial nerve involvement (58.2%), dysautonomia (55.7%), and albumin-cytological dissociation (100%). ENMG showed demyelinating and axonal forms in 57.6% and 42.4% of cases, respectively. At the plateau phase, 36% and 21% of patients had very severe deficits (Guillain-Barre Syndrome Disability Score (GBSDS 4)) and respiratory distress (GBSDS 5), respectively. Corticosteroid therapy (58.2%) and intravenous immunoglobulins (IVIg) (6.8%) were the specific therapies used. Infectious complications (41.8%), particularly inhalation pneumonia (27.8%), acute respiratory distress (13.9%), and cardiac dysautonomia complications (6.3%), were the most common hospital complications. Eighteen patients (22.8%) were transferred to intensive care, mainly due to the onset of respiratory distress (13.9%). At the end of hospitalization, the hospital mortality rate was 22.8%, with acute respiratory distress (44.4%) and dysautonomic cardiac arrest (16.7%) being the most common immediate causes of death. Conclusion: In Burkina Faso, GBS is confronted with delays in patient admission, low availability and access to IVIG and EP, and high hospital mortality. Early admission and improved access to emergency immunotherapy and intensive care beds in ASS will help improve the prognosis for patients with GBS.
|
Published in
|
Clinical Neurology and Neuroscience (Volume 10, Issue 1)
|
|
DOI
|
10.11648/j.cnn.20261001.12
|
|
Page(s)
|
5-14 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
GBS, Corticosteroid Therapy, Intravenous Immunoglobulins, Hospital Mortality, Respiratory Distress, Burkina Faso
1. Introduction
Guillain-Barre syndrome (GBS) is the leading cause of acute flaccid paralysis of neurological origin worldwide, with mortality rates ranging from 3% to 20% depending on a country's level of resources. In low-income countries, including those in sub-Saharan Africa, the management of GBS continues to face major challenges, including delayed diagnosis, limited access to intravenous immunoglobulin (IVIG), plasma exchange (PE), and intensive care, as well as a higher incidence of respiratory and dysautonomic complications
| [1] | Leonhard, S. E., Mandarakas, M. R., Gondim, F. A. A. et al. Diagnosis and management of Guillain-Barre syndrome in ten steps. Nat Rev Neurol 15, 671-683 (2019).
https://doi.org/10.1038/s41582-019-0250-9 |
| [2] | Dabilgou AA, Kabore R, Drave A, et al. Guillain-Barre syndrome in Sub-Saharan Africa: experience from a tertiary hospital in Burkina Faso. PAMJ Clin Med. 2022; 8(15).
https://doi.org/10.11604/pamj-cm.2022.8.15.31957 |
| [3] | Lompo DL, Kabore RMP, Ouedraogo AM, et al. Clinical and Evaluative Profile of Guillain-Barre Syndrome in Burkina Faso. Clin Neurol Neurosci. 2023; 7: 56-64.
https://doi.org/10.11648/j.cnn.20230703.13 |
| [4] | Apetse, K., Tajeuna, J. D., Kumako, V. K., Waklatsi, K. P., Kombate, D., Assogba, K., & Balogou, A. K. (2021). Guillain-Barre syndrome in hospitals in Togo. Tropical Medicine and International Health, 1(3), mtsibulletin-2021.
https://doi.org/10.48327/mtsibulletin.2021.124 |
[1-4]
. Several studies show that mortality is significantly higher than in high-income countries, mainly due to the unavailability of specific immunological therapies and the lack of mechanical ventilation
. In Burkina Faso, retrospective studies of historical data from 2003 to 2020 have reported that treatment is largely based on corticosteroid therapy, despite the lack of demonstrated benefit, the virtual absence of IVIG and PE, and poor access to mechanical ventilation, with morbidity and mortality remaining high
. In this context, understanding the current therapeutic and evolutionary modalities of GBS is a major clinical challenge. The present study therefore aims to describe the therapeutic practices and intra-hospital evolution of adult patients with GBS in the University Hospital Centers (CHU) of Ouagadougou. Understanding the current therapeutic and evolutionary modalities of GBS in our context is an essential prerequisite for supporting advocacy efforts with health authorities to improve the availability and accessibility of the diagnostic, therapeutic, and intensive care resources necessary for optimal management of GBS in Burkina Faso.
2. Patients and Methods
This was a cross-sectional, descriptive, prospective data collection study conducted from March 1, 2018, to May 30, 2022, at the university hospitals (UH) of Ouagadougou (UH-Tengandogo, UH -Yalgado Ouedraogo, and UH-Bogodogo) who had been diagnosed with GBS.
All patients who met the following criteria were included in this study: they had been admitted and/or monitored at the UH of Ouagadougou (Yalgado Ouedraogo, Tengandogo, Bogodogo) for a clear diagnosis of GBS according to the modified Brighton criteria
| [6] | Fokke, C., van den Berg, B., Drenthen, J., Walgaard, C., van Doorn, P. A., & Jacobs, B. C. (2014). Diagnosis of Guillain-Barre syndrome and validation of Brighton criteria. Brain, 137(1), 33-43. https://doi.org/10.1093/brain/awt285 |
[6]
. These criteria are based on clinical manifestations, the results of electro-neuro-myographic (ENMG) examinations and lumbar puncture (LP) with cytochemical and microbiological analysis of cerebro spinal fluid (CSF). Patients diagnosed with GBS were those classified as level 1 (highest degree of diagnostic certainty) or level 2 (intermediate degree of diagnostic certainty).
Table 1 below presents the Brighton diagnostic criteria for GBS.
Table 1. Diagnostic criteria for Guillain-Barre syndrome.
Diagnostic criteria | Level of diagnostic certainty |
1 | 2 |
Bilateral flaccid motor deficit in the limbs | + | + |
Decreased or absent deep tendon reflexes in affected limbs | + | + |
Monophasic progression and delay between onset and nadir of 12 hours to 28 days | + | + |
Cytorachia <10 elements/mm3 | + | +a |
Proteinorachia > 0.45g/l | + | +\-a |
ENMG in favor of a subtype of GBS | + | +\- |
No other diagnostic alternatives for motor deficit | + | + |
Not included in this study were suspected cases of GBS that did not meet the Brighton criteria, cases of secondary polyradiculoneuritis, cases of chronic polyradiculoneuritis, patients who did not consent, patients who died, or patients who were discharged against medical advice before any investigation.
Data collection was carried out using a data collection form designed for this purpose, and the information gathered (medical history, background, physical examination, follow-up, additional tests) was collected from the patient during their hospital stay and during post-hospital outpatient consultations, then entered onto the data collection form. Some data could be supplemented with departmental records, patient clinical files, notebooks, and additional test results.
Study protocol
Rajabally's electrophysiological criteria
| [7] | Rajabally, Y. A., Durand, M.-C., Mitchell, J., Orlikowski, D., & Nicolas, G. (2015). Electrophysiological diagnosis of Guillain-Barre syndrome subtype: could a single study suffice? Journal of Neurology, Neurosurgery & Psychiatry, 86(1), 115-119.
https://doi.org/10.1136/jnnp-2014-307815 |
[7]
, adapted to the diagnosis of Guillain-Barre syndrome (GBS) in settings where diagnostic resources are limited (such as the Ouagadougou University Hospital), were used.
Nerves examined (minimum requirement):
1) 4 motor nerves: median, ulnar, fibular (peroneal), tibial
2) 1 sensory nerve: sural (optional but useful for distinguishing between Acute Inflammatory Demyelinating Polyradiculoneuropathy (AIDP) and Acute Motor Axonal Neuropathy (AMAN))
3) F waves: at least on one motor nerve (ulnar or tibial)
Rajabally 2015 criteria used for the diagnosis of probable acute inflammatory demyelinating polyradiculoneuropathy (AIDP): patients were classified as probable AIDP if at least 2 nerves showed one or more demyelinating abnormalities according to the thresholds below.
Table 2. Diagnostic criteria for Guillain-Barré syndrome according to Rajabally.
Parameter | Demyelination threshold (≥1 abnormality sufficient) |
Distal motor latency (DML) | ≥ 125% of the upper normal limit (UNL) |
Motor conduction velocity (MCV) | ≤ 90% of the lower normal limit (LNL) |
Conduction block | Proximal amplitude reduction ≥ 50% compared to distal, with <30% prolongation of duration |
Temporal dispersion | Proximal Compound Muscle Action Potential (CMAP) duration prolongation ≥ 30% vs distal |
Minimal F-wave latency | ≥ 120% of ULN, or absent F-wave with preserved CMAP (>1 mV) |
Absence of distal response | CMAP <1 mV at the wrist (if not explained by clear axonal damage) |
Criteria for axonal forms, acute motor axonal neuropathies/acute sensory-motor axonal neuropathies (AMAN/ Acute Motor and Sensory Axonal Neuropathy (AMSAN))
1) Reduction in distal CMAP amplitude <80% LIN without conduction abnormalities characteristic of demyelination.
2) Conduction velocity and distal latencies preserved or slightly altered.
3) F waves often absent or prolonged, but CMAP low early on.
4) SNAP (sensory potential): normal in AMAN, decreased in AMSAN.
Table 3. Final classification according to Rajabally.
Category | Criteria |
AIDP | ≥2 nerves with demyelinating abnormalities according to the above thresholds |
AMAN/AMSAN | Reduced CMAP amplitude without demyelination criteria |
Equivocal | Insufficient abnormalities to classify |
Normal | No criteria met |
The following variables were analyzed: 1) age, sex, comorbidities, clinical and paraclinical aspects (albumin-cytological dissociation on lumbar puncture, ENMG classification: Acute inflammatory demyelinating polyradiculoneuropathy (AIDP), Acute motor axonal neuropathy (AMAN), Acute motor and sensory axonal neuropathy (AMSAN), equivocal or unclassifiable form); treatments administered, hospital progression (duration of the three phases of the disease (days), length of hospital stay (days), transfer due to intercurrent complications, transfer to intensive care, clinical outcome (survivors/deceased), functional outcome of survivors at the end of hospitalization according to the GBS Disability Scale (GBSDS) or Hughes Functional Assessment Scale.
Table 4. Guillain-Barre Disability Scale (GBSDS) or Hughes Functional Assessment Scale.
Score | Level of disability | Clinical description |
0 | Normal | No signs or symptoms of disease. |
1 | Minimal impairment | Minor signs of GBS but able to run. |
2 | Moderate impairment | Able to walk ≥ 10 meters without assistance but unable to run. |
3 | Severe impairment | Able to walk ≥ 10 meters with assistance (cane, walker, or human assistance). |
4 | Very severe impairment | Bedridden or unable to move independently (neither walking nor standing). |
5 | Respiratory dependence | Requires assisted ventilation (intubation or mechanical ventilation). |
The data collected were entered and analyzed on a microcomputer using Epi-Info software version 7.5.2.0. The tables and figures were created using Word 2016 and Microsoft Excel 2016 software. Quantitative variables were described as means, standard deviations, first quartiles, thirdquartiles, and extremes. Qualitative variables were grouped as proportions.
Data collection was carried out with the authorization of the general management of the Tengandogo, Bogodogo, and Yalgado Ouedraogo UHs.
Anonymity and confidentiality of the data were guaranteed.
3. Results
We consecutively collected data on 79 patients hospitalized for GBS during our study period over a period of 5 years (2018 to 2023).
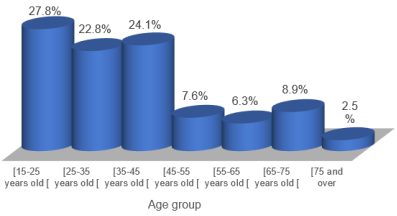
The average age of patients was 38.2 ± 16 years (range 15 to 79 years); patients aged ≤ 45 years were the most represented, with 55 cases (69.6%).
Figure 1 shows the distribution of patients by age group.
Figure 1. Distribution of patients by age group.
There were 44 men (55.7%) and 35 women (44.3%), giving a male-to-female ratio of 1.25.
The average consultation time was 22 days +/- 10 (range 5 to 90 days). At the time of assessment, motor deficit and decreased/absent ROT were present in all patients (100%); tetraparesis in 42 cases (53.2%) and respiratory muscle weakness in 35 cases (44.3%) were the most common types of motor deficit. Deep hypoesthesia/anesthesia was found in 33 patients (41.8%). Cranial nerve involvement was noted in 46 cases (58.2%), with facial involvement being the most common (16 cases, 20.2%). Dysautonomic disorders were found in 36 patients (45.6%), dominated by blood pressure fluctuations (20 cases, 25.3%), constipation (12 cases, 15%), and tachycardia (7 cases, 8.9%).
Table 5 below shows the distribution of patients with GBS according to the clinical characteristics found in the status phase.
Table 5. Distribution of patients with GBS according to clinical characteristics in the steady state phase.
Clinical characteristics at the steady state phase | Number (N=79) | Percentage |
Initial physical examination data | | |
Motor deficit | 79 | 100.0 |
All 4 limbs | 56 | 70.9 |
Tetraparesis with or without paresis of the trunk muscles | 42 | 53.2 |
Quadriplegia with respiratory distress | 14 | 17.7 |
Lower limbs | 23 | 29.1 |
Paraparesis | 16 | 20.3 |
Paraplegia | 7 | 8.9 |
Respiratory muscles | 35 | 44.3 |
Distal hypoesthesia/anesthesia of the four limbs | 33 | 41.8 |
Proprioceptive ataxia | 24 | 30.4 |
Cranial nerve involvement | 46 | 58.2 |
Facial paralysis/paresis | 16 | 20.2 |
Swallowing disorders | 14 | 17.7 |
Lingual paresis | 6 | 7.6 |
Oculomotor paresis | 4 | 5.1 |
Hearing loss | 3 | 3.8 |
Alteration of osteotendinous reflexes | 79 | 100 |
Dysautonomic disorders (associated) | 36 | 45.6 |
Cardiovascular | 30 | 38 |
Blood pressure fluctuations | 20 | 25.3 |
Tachycardia | 7 | 8.9 |
Orthostatic hypotension | 6 | 7.6 |
Cardiac arrhythmia | 5 | 6.3 |
Other disorders | 18 | 22.8 |
Constipation | 12 | 15.2 |
Acute urinary retention | 4 | 5.1 |
Hypersudation | 2 | 2.5 |
Lumbar puncture (LP) was performed in 70 patients (88.6%), with hyperproteinorachia and albumin-cytological dissociation found in 67/70 patients (95.7%) respectively.
Electroneuromyography (ENMG) could only be performed in 26 patients (32.9%). Demyelinating lesions and axonal lesions were found in 15 cases (57.7%) and 11 cases (42.3%), respectively. No equivocal cases were observed.
The mean durations of the extension and plateau phases were 10.8 days +/- 13.2 (range 2 to 24 days) and 20.8 days +/- 39.3 (range 6 to 68 days), respectively. The duration of the recovery phase was not assessed.
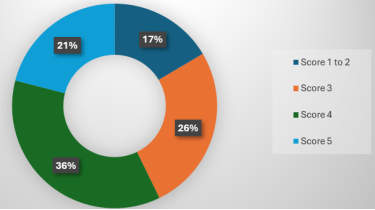
At the peak of the plateau phase, clinical severity assessed according to the GBSDS showed that 28 patients (36%) and 17 patients (21%) had very severe deficits (GBSDS 4) and respiratory distress (GBSDS 5), respectively. (
Figure 2).
Figure 2. Distribution of patients with GBS according to the GBSDS at the peak of the disease phase.
With regard to specific treatment, corticosteroid therapy (although its efficacy has not been proven) was administered to 46 patients, or 58.22%. Only 6 patients (7.6%) received polyvalent IVIG treatment at a dose of 0.4 g/kg/day for 5 days. None of our patients received EP. Physical therapy was indicated for all patients, but only 58 patients (75.4%) received it.
With regard to non-specific treatment, analgesics (62 patients (78.48%)), broad-spectrum antibiotics (38 patients (48.1%)), and preventive anticoagulation (51 patients (64.6%)) were administered.
Table 6 below shows the distribution of patients according to the types of treatment received.
Table 6. Distribution of patients according to the types of treatment received.
Treatment | Number | Percentage |
Specific treatment | | |
Corticosteroid therapy (prednisone, prednisolone) | 46 | 58.2 |
IV polyvalent immunoglobulins (IVIg) | 6 | 7.6 |
Plasma exchange (PE) | 0 | 0 |
Physical Therapy | 58 | 75.4 |
Non-specific treatments | | |
Broad-spectrum antibiotic therapy | 38 | 48.1 |
Preventive doses of anticoagulants | 51 | 64.6 |
Analgesics (paracetamol and/or pregabalin or gabapentin) | 62 | 78.5 |
Other treatments | |
Urinary catheter | 29 | 37.7 |
Antihypertensive drugs (amlodipine and/or telmisartan) | 24 | 31.2 |
Vitamins (B1 + B6 + B12) | 22 | 28.6 |
Oxygen therapy with mask | 21 | 27.3 |
Anxiolytics (lorazepam) | 19 | 24.7 |
Proton pump inhibitors (esomeprazole or omeprazole) | 17 | 22.1 |
Laxatives (macrogol) | 15 | 19.5 |
Nasogastric tube | 10 | 13 |
Mechanical ventilation | 7 | 9.1 |
Tracheotomy | 6 | 7.6 |
The average length of hospital stay was 19.8 days +/- 12.6 (range 1 to 45 days).
Infectious complications were the most common, with 33 cases (41.8%), dominated by bronchopulmonary infections (22 cases, 27.8%); acute respiratory distress, with 11 cases (13.9%), and cardiac dysautonomia complications (5 cases; 6.3%), dominated by cardiac arrest (3 patients; 3.8%), were the most serious. Eighteen patients (22.8%) were transferred to intensive care. Acute respiratory distress in 11 patients (13.9%), major swallowing disorders in 4 patients (5.1%), and severe cardiac dysautonomia such as cardiac arrest in 3 patients (3.8%) were the reasons for transfer to intensive care. In intensive care, mechanical ventilation was performed in 13 patients (16.4%) for respiratory distress with or without major swallowing disorders, including 6 patients (7.6%) who underwent tracheotomy.
The distribution of patients according to the various hospital complications observed is summarized in
Table 7 below.
Table 7. Distribution of patients according to intercurrent complications that occurred during hospitalization.
Complications | Number | Percentage |
Cardiac dysautonomia | 5 | 6.3 |
Cardiac arrest | 3 | 3.8 |
Severe arrhythmia | 2 | 2.5 |
Infectious | 33 | 41.8 |
Pulmonary | 22 | 66.7 |
Urinary | 8 | 24.2 |
Digestive | 3 | 9.1 |
Pressure sores | 6 | 26.1 |
Malnutrition | 6 | 26.1 |
Refractory neuropathic pain | 5 | 21.7 |
Psychomotor agitation | 4 | 17.4 |
Pulmonary embolism | 2 | 8.7 |
Acute respiratory distress | 11 | 13.9 |
Major swallowing disorder | 5 | 6.3 |
Transfers to intensive care and reasons for transfer | 18 | 22.8 |
Acute respiratory distress | 11 | 13.9 |
Major swallowing disorder | 4 | 5.1 |
Severe cardiac dysautonomia: cardiac arrest | 3 | 3.8 |
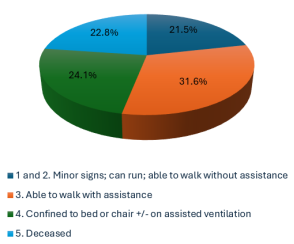
A total of 18 patients died during hospitalization, representing a hospital mortality rate of 22.8%, and 19 patients (24.1%) were still confined to bed or chair with or without assisted ventilation (GBSDS at 4).
Figure 3 below shows the distribution of patients according to the results of the clinical outcome assessment at the end of hospitalization according to the GBSDS.
Figure 3. Distribution of patients according to the evolution of functional disability according to the GBSDS.
Severe respiratory distress (8 cases; 44.4%) and cardiac arrest (3 cases; 16.7%) were the main immediate causes of in-hospital deaths (
Table 8).
Table 8. Distribution of causes of death according to frequency.
Causes | Number (N=18) | Percentage |
Severe respiratory distress | 8 | 4 |
Cardiac arrest | 3 | 16.7 |
Septic shock | 2 | 11.1 |
Acute bronchopneumonia | 2 | 11.1 |
Pulmonary embolism | 1 | 5.6 |
Undetermined | 2 | 11.1 |
4. Discussion
In our series, specific treatment consisted of corticosteroid therapy and intravenous immunoglobulin (IVIg) in 58.2% and 7.6% of patients, respectively. No patients underwent plasma exchange (PE). Our results are consistent with certain data from sub-Saharan Africa (SSA), which show significant use of corticosteroids in the treatment of GBS: 80% in the study by Dabilgou et al. in Burkina Faso
| [4] | Apetse, K., Tajeuna, J. D., Kumako, V. K., Waklatsi, K. P., Kombate, D., Assogba, K., & Balogou, A. K. (2021). Guillain-Barre syndrome in hospitals in Togo. Tropical Medicine and International Health, 1(3), mtsibulletin-2021.
https://doi.org/10.48327/mtsibulletin.2021.124 |
[4]
, 53% in Dakar, Senegal
| [8] | Basse AM, Boubacar S, Sow AD, et al. Epidemiology of acute polyradiculoneuritis at Fann Department of Neurology Dakar, Senegal. Clin Neurol Neurosci. 2017; 1(4): 76-79.
https://doi.org/10.11648/j.cnn.20170104.11 |
[8]
, and 50% in Togo
| [4] | Apetse, K., Tajeuna, J. D., Kumako, V. K., Waklatsi, K. P., Kombate, D., Assogba, K., & Balogou, A. K. (2021). Guillain-Barre syndrome in hospitals in Togo. Tropical Medicine and International Health, 1(3), mtsibulletin-2021.
https://doi.org/10.48327/mtsibulletin.2021.124 |
[4]
. However, this significant use of corticosteroid therapy is unfounded when referring to the results of international reviews, which conclude that there is no proven benefit of corticosteroids and even suggest a possible deleterious effect of oral corticosteroids
| [1] | Leonhard, S. E., Mandarakas, M. R., Gondim, F. A. A. et al. Diagnosis and management of Guillain-Barre syndrome in ten steps. Nat Rev Neurol 15, 671-683 (2019).
https://doi.org/10.1038/s41582-019-0250-9 |
[1]
. This high and unfounded use of corticosteroids in SSA contrasts paradoxically with the low use of proven reference treatments such as IVIG and EP: no patients in the series by Dabilgou et al. in Burkina Faso
, Basse A et al. in Senegal
| [8] | Basse AM, Boubacar S, Sow AD, et al. Epidemiology of acute polyradiculoneuritis at Fann Department of Neurology Dakar, Senegal. Clin Neurol Neurosci. 2017; 1(4): 76-79.
https://doi.org/10.11648/j.cnn.20170104.11 |
[8]
, or Joshua et al. in Zambia
| [9] | Joshua Saisha, Margaret M. Mweshi, Martha Banda-Chalwe, Loveness A. Nkhata, Elliot Kafumukache, Micah Simpamba, Namalambo Mwenda - Ng’uni. The Prevalence of Guillain-Barre Syndrome and the Rate of Physiotherapy Referral at the University Teaching Hospital, Lusaka, Zambia. International Journal of Neurologic Physical Therapy. Vol. 2, No. 1, 2015, pp. 1-4. https://doi.org/10.11648/j.ijnpt.20160201.11 |
[9]
received these reference treatments. In our previous study in 2023 and in the study by Apetse et al. in Togo, 6% and 18% of patients, respectively, received IVIG treatment
| [3] | Lompo DL, Kabore RMP, Ouedraogo AM, et al. Clinical and Evaluative Profile of Guillain-Barre Syndrome in Burkina Faso. Clin Neurol Neurosci. 2023; 7: 56-64.
https://doi.org/10.11648/j.cnn.20230703.13 |
| [4] | Apetse, K., Tajeuna, J. D., Kumako, V. K., Waklatsi, K. P., Kombate, D., Assogba, K., & Balogou, A. K. (2021). Guillain-Barre syndrome in hospitals in Togo. Tropical Medicine and International Health, 1(3), mtsibulletin-2021.
https://doi.org/10.48327/mtsibulletin.2021.124 |
[3, 4]
, while 51.7% of patients in Kenya benefited from it
| [10] | Muindi SK, Onyango M, Masika MM. Demographic and clinical characteristics of Guillain-Barre syndrome at Kenyatta National Hospital, Kenya. BMJ Neurol Open. 2025; 7(1): e001074. https://doi.org/10.1136/bmjno-2025-001074 |
[10]
. The low use of IVIG and PE can be explained by 1) the financial inaccessibility of IVIG due to its prohibitive cost, which is beyond the reach of most patients (€9,000 for a course of IVIG, for example), 2) the chronic unavailability of PE infrastructure (PE machines and accessories, plasma or albumin, human resources) in almost all hospitals in SSA
| [1] | Leonhard, S. E., Mandarakas, M. R., Gondim, F. A. A. et al. Diagnosis and management of Guillain-Barre syndrome in ten steps. Nat Rev Neurol 15, 671-683 (2019).
https://doi.org/10.1038/s41582-019-0250-9 |
| [3] | Lompo DL, Kabore RMP, Ouedraogo AM, et al. Clinical and Evaluative Profile of Guillain-Barre Syndrome in Burkina Faso. Clin Neurol Neurosci. 2023; 7: 56-64.
https://doi.org/10.11648/j.cnn.20230703.13 |
| [8] | Basse AM, Boubacar S, Sow AD, et al. Epidemiology of acute polyradiculoneuritis at Fann Department of Neurology Dakar, Senegal. Clin Neurol Neurosci. 2017; 1(4): 76-79.
https://doi.org/10.11648/j.cnn.20170104.11 |
| [10] | Muindi SK, Onyango M, Masika MM. Demographic and clinical characteristics of Guillain-Barre syndrome at Kenyatta National Hospital, Kenya. BMJ Neurol Open. 2025; 7(1): e001074. https://doi.org/10.1136/bmjno-2025-001074 |
| [11] | Hughes RA, Swan AV, van Doorn PA. Intravenous immunoglobulin for Guillain-Barre syndrome. Cochrane Database Syst Rev. 2014 Sep 19; 2014(9): CD002063.
https://doi.org/10.1002/14651858.CD002063 |
[1, 3, 8, 10, 11]
. Furthermore, in SSA countries, IVIG and PE are not perceived by decision-makers as vital health products whose availability should be ensured at all times
| [12] | WHO Model List of Essential Medicines, regional analyses, 2021. |
[12]
. It is also important to emphasize the late admission of patients beyond the optimal period of effectiveness of IVIG and PB, which is within two weeks of the onset of GBS, thus limiting the value of this therapy
| [2] | Dabilgou AA, Kabore R, Drave A, et al. Guillain-Barre syndrome in Sub-Saharan Africa: experience from a tertiary hospital in Burkina Faso. PAMJ Clin Med. 2022; 8(15).
https://doi.org/10.11604/pamj-cm.2022.8.15.31957 |
| [3] | Lompo DL, Kabore RMP, Ouedraogo AM, et al. Clinical and Evaluative Profile of Guillain-Barre Syndrome in Burkina Faso. Clin Neurol Neurosci. 2023; 7: 56-64.
https://doi.org/10.11648/j.cnn.20230703.13 |
| [4] | Apetse, K., Tajeuna, J. D., Kumako, V. K., Waklatsi, K. P., Kombate, D., Assogba, K., & Balogou, A. K. (2021). Guillain-Barre syndrome in hospitals in Togo. Tropical Medicine and International Health, 1(3), mtsibulletin-2021.
https://doi.org/10.48327/mtsibulletin.2021.124 |
| [8] | Basse AM, Boubacar S, Sow AD, et al. Epidemiology of acute polyradiculoneuritis at Fann Department of Neurology Dakar, Senegal. Clin Neurol Neurosci. 2017; 1(4): 76-79.
https://doi.org/10.11648/j.cnn.20170104.11 |
[2, 3, 4, 8]
. In our study, the average time to admission was 22 days, and in the series by Bayu et al (Ethiopia), late referral after traditional medicine was identified as an independent risk factor for mortality
| [13] | Bayu HT, Demilie AE, Molla MT, Kumie FT, Endeshaw AS. Mortality and its predictors among patients with Guillain-Barre syndrome in the intensive care unit of a low-income country, Ethiopia: a multicenter retrospective cohort study. Front Neurol. 2024 Oct 30; 15: 1484661.
https://doi.org/10.3389/fneur.2024.1484661 |
[13]
.
In our series, hospital mortality was 22.8%, close to the range of mortality rates of 10 to 20% or even higher, usually reported in low-income countries such as those in sub-Saharan Africa and South Asia: 11% in Togo
| [4] | Apetse, K., Tajeuna, J. D., Kumako, V. K., Waklatsi, K. P., Kombate, D., Assogba, K., & Balogou, A. K. (2021). Guillain-Barre syndrome in hospitals in Togo. Tropical Medicine and International Health, 1(3), mtsibulletin-2021.
https://doi.org/10.48327/mtsibulletin.2021.124 |
[4]
, 10-15% in Senegal
| [8] | Basse AM, Boubacar S, Sow AD, et al. Epidemiology of acute polyradiculoneuritis at Fann Department of Neurology Dakar, Senegal. Clin Neurol Neurosci. 2017; 1(4): 76-79.
https://doi.org/10.11648/j.cnn.20170104.11 |
[8]
, 14-18% in Burkina Faso
, 19.2% in intensive care in Ethiopia
| [13] | Bayu HT, Demilie AE, Molla MT, Kumie FT, Endeshaw AS. Mortality and its predictors among patients with Guillain-Barre syndrome in the intensive care unit of a low-income country, Ethiopia: a multicenter retrospective cohort study. Front Neurol. 2024 Oct 30; 15: 1484661.
https://doi.org/10.3389/fneur.2024.1484661 |
[13]
, and 12-20% in hospital cohorts in Bangladesh and Pakistan
| [14] | Kaur S, Khan S, Iqbal J, et al. Predictors of mechanical ventilation and mortality in patients with Guillain-Barre syndrome: a tertiary care experience from Pakistan. J Pak Med Assoc. 2019; 69(6): 837-842. |
| [15] | Khan Z, Al-Barry M, Ahmed N, et al. Clinical profile and outcome of patients with Guillain-Barre syndrome in a tertiary care hospital in Pakistan. Pak J Med Sci. 2017; 33(2): 378-382. |
| [16] | Khan SI, Rahman A, Sarker MS, et al. Outcome of Guillain-Barre syndrome patients in a low-resource country: a prospective observational study. PLoS One. 2020; 15(6): e0234111.
https://doi.org/10.1371/journal.pone.0234111 |
[14, 15, 16]
. However, the mortality rate in our series is significantly higher than the 5-10% rate reported in middle-income countries (India, Brazil, rural China, South Africa)
and the low hospital mortality rate of 5-7% reported in high-income countries
. The low mortality rates observed in high-income countries (Europe, North America, Australia, Japan) can be explained by the near-universal access of patients to emergency immunotherapy, advanced intensive care units, and standardized protocols in these countries
.
Low-income countries often have mortality rates 2 to 4 times higher than those in rich countries, due to lack of access to IVIg, plasmapheresis, resuscitation or intensive care beds, and mechanical ventilation
. In our series, EP was not available, only 8% of patients received IVIg, and 23% of patients were transferred to intensive care. In contrast, in the Kenyan series, GBS mortality was significantly reduced in patients who received IVIg, but remained high overall in the absence of early access to intensive care
| [10] | Muindi SK, Onyango M, Masika MM. Demographic and clinical characteristics of Guillain-Barre syndrome at Kenyatta National Hospital, Kenya. BMJ Neurol Open. 2025; 7(1): e001074. https://doi.org/10.1136/bmjno-2025-001074 |
[10]
. When analyzing the immediate causes of in-hospital deaths in our series and in other series from low-income countries, acute respiratory distress, severe cardiac dysautonomia, and nosocomial infectious complications are the most common
| [1] | Leonhard, S. E., Mandarakas, M. R., Gondim, F. A. A. et al. Diagnosis and management of Guillain-Barre syndrome in ten steps. Nat Rev Neurol 15, 671-683 (2019).
https://doi.org/10.1038/s41582-019-0250-9 |
| [3] | Lompo DL, Kabore RMP, Ouedraogo AM, et al. Clinical and Evaluative Profile of Guillain-Barre Syndrome in Burkina Faso. Clin Neurol Neurosci. 2023; 7: 56-64.
https://doi.org/10.11648/j.cnn.20230703.13 |
| [4] | Apetse, K., Tajeuna, J. D., Kumako, V. K., Waklatsi, K. P., Kombate, D., Assogba, K., & Balogou, A. K. (2021). Guillain-Barre syndrome in hospitals in Togo. Tropical Medicine and International Health, 1(3), mtsibulletin-2021.
https://doi.org/10.48327/mtsibulletin.2021.124 |
| [13] | Bayu HT, Demilie AE, Molla MT, Kumie FT, Endeshaw AS. Mortality and its predictors among patients with Guillain-Barre syndrome in the intensive care unit of a low-income country, Ethiopia: a multicenter retrospective cohort study. Front Neurol. 2024 Oct 30; 15: 1484661.
https://doi.org/10.3389/fneur.2024.1484661 |
[1, 3, 4, 13]
. Deaths due to respiratory failure are frequently linked to delayed intubation, lack of ventilators, and limited availability of intensive care or resuscitation beds
| [2] | Dabilgou AA, Kabore R, Drave A, et al. Guillain-Barre syndrome in Sub-Saharan Africa: experience from a tertiary hospital in Burkina Faso. PAMJ Clin Med. 2022; 8(15).
https://doi.org/10.11604/pamj-cm.2022.8.15.31957 |
| [3] | Lompo DL, Kabore RMP, Ouedraogo AM, et al. Clinical and Evaluative Profile of Guillain-Barre Syndrome in Burkina Faso. Clin Neurol Neurosci. 2023; 7: 56-64.
https://doi.org/10.11648/j.cnn.20230703.13 |
| [13] | Bayu HT, Demilie AE, Molla MT, Kumie FT, Endeshaw AS. Mortality and its predictors among patients with Guillain-Barre syndrome in the intensive care unit of a low-income country, Ethiopia: a multicenter retrospective cohort study. Front Neurol. 2024 Oct 30; 15: 1484661.
https://doi.org/10.3389/fneur.2024.1484661 |
[2, 3, 13]
. Cardiac arrest, the leading cause of death related to severe cardiac dysautonomia, particularly in low-income countries
| [2] | Dabilgou AA, Kabore R, Drave A, et al. Guillain-Barre syndrome in Sub-Saharan Africa: experience from a tertiary hospital in Burkina Faso. PAMJ Clin Med. 2022; 8(15).
https://doi.org/10.11604/pamj-cm.2022.8.15.31957 |
| [3] | Lompo DL, Kabore RMP, Ouedraogo AM, et al. Clinical and Evaluative Profile of Guillain-Barre Syndrome in Burkina Faso. Clin Neurol Neurosci. 2023; 7: 56-64.
https://doi.org/10.11648/j.cnn.20230703.13 |
| [13] | Bayu HT, Demilie AE, Molla MT, Kumie FT, Endeshaw AS. Mortality and its predictors among patients with Guillain-Barre syndrome in the intensive care unit of a low-income country, Ethiopia: a multicenter retrospective cohort study. Front Neurol. 2024 Oct 30; 15: 1484661.
https://doi.org/10.3389/fneur.2024.1484661 |
[2, 3, 13]
, is exacerbated by limited access to or availability of intensive care or resuscitation beds, which are the only beds equipped with continuous monitoring systems for cardiovascular and respiratory vital signs
| [5] | Willison HJ, Jacobs BC, van Doorn PA. Guillain-Barré syndrome. Lancet. 2016 Aug 13; 388(10045): 717-27.
https://doi.org/10.1016/S0140-6736(16)00339-1 |
| [13] | Bayu HT, Demilie AE, Molla MT, Kumie FT, Endeshaw AS. Mortality and its predictors among patients with Guillain-Barre syndrome in the intensive care unit of a low-income country, Ethiopia: a multicenter retrospective cohort study. Front Neurol. 2024 Oct 30; 15: 1484661.
https://doi.org/10.3389/fneur.2024.1484661 |
[5, 13]
.
Limitations and strengths of our study
The limited availability of IVIg and resuscitation may artificially increase the observed severity and reduce the generalizability of the results. The descriptive and non-comparative nature of the study does not allow for the formal identification of independent prognostic determinants.
However, the prospective collection of data, including a relatively large number of patients with GBS in an African context, reinforces the quality and reliability of the clinical data collected. It also provides a detailed description of the therapeutic and evolutionary modalities in three university hospitals, shedding light on the management of GBS in sub-Saharan Africa.
5. Conclusion
In Burkina Faso, GBS is confronted with delayed admission, unjustified use of corticosteroid therapy, and low availability and access to IVIG and EP. Hospital mortality remains high, caused by acute respiratory distress and dysautonomic cardiac arrest. Early admission and improved access to IVIG, EP, and Intensive care units (ICU) or intensive care beds in SSA will help improve the prognosis for patients with GBS.
Abbreviations
AIDPP | Acute Inflammatory Demyelinating Polyradiculoneuropathy |
AMANN | Acute Motor Axonal Neuropathy |
AMSANN | Acute Motor and Sensory Axonal Neuropathy |
CMAP | Compound Muscle Action Potential |
CSF | Cereboro spinal Fluid |
ENMG | Electro Neuro Myographic |
GBS | Guillain-Barre Syndrome |
GBSDS | Guillain-Barre Syndrome Dysability Scale |
ICU | Intensive Care Unit |
IVIG | Intravenous Immuonglobulin |
LP | Lumbar Puncture |
PE | Plasma Exchange |
SSA | Sub Saharan Africa |
UH | University Hospital |
Author Contributions
Lompo Djingri Labodi: Conceptualization, Formal analysis, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing
Zoungrana Alassane: Data curation, Investigation, Methodology, Resources, Software, Visualization
Gnampa Zeinab Melody: Data Curation, Formal analysis, Investigation, Resources, Visualization, Software
Carama Emeline Agathe: Validation
Kere M Fabienne: Validation
Napon Christian: Peoject administration, Supervision, Validation
Millogo Athanase: Project administration, Supervision, Validation
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Leonhard, S. E., Mandarakas, M. R., Gondim, F. A. A. et al. Diagnosis and management of Guillain-Barre syndrome in ten steps. Nat Rev Neurol 15, 671-683 (2019).
https://doi.org/10.1038/s41582-019-0250-9
|
| [2] |
Dabilgou AA, Kabore R, Drave A, et al. Guillain-Barre syndrome in Sub-Saharan Africa: experience from a tertiary hospital in Burkina Faso. PAMJ Clin Med. 2022; 8(15).
https://doi.org/10.11604/pamj-cm.2022.8.15.31957
|
| [3] |
Lompo DL, Kabore RMP, Ouedraogo AM, et al. Clinical and Evaluative Profile of Guillain-Barre Syndrome in Burkina Faso. Clin Neurol Neurosci. 2023; 7: 56-64.
https://doi.org/10.11648/j.cnn.20230703.13
|
| [4] |
Apetse, K., Tajeuna, J. D., Kumako, V. K., Waklatsi, K. P., Kombate, D., Assogba, K., & Balogou, A. K. (2021). Guillain-Barre syndrome in hospitals in Togo. Tropical Medicine and International Health, 1(3), mtsibulletin-2021.
https://doi.org/10.48327/mtsibulletin.2021.124
|
| [5] |
Willison HJ, Jacobs BC, van Doorn PA. Guillain-Barré syndrome. Lancet. 2016 Aug 13; 388(10045): 717-27.
https://doi.org/10.1016/S0140-6736(16)00339-1
|
| [6] |
Fokke, C., van den Berg, B., Drenthen, J., Walgaard, C., van Doorn, P. A., & Jacobs, B. C. (2014). Diagnosis of Guillain-Barre syndrome and validation of Brighton criteria. Brain, 137(1), 33-43.
https://doi.org/10.1093/brain/awt285
|
| [7] |
Rajabally, Y. A., Durand, M.-C., Mitchell, J., Orlikowski, D., & Nicolas, G. (2015). Electrophysiological diagnosis of Guillain-Barre syndrome subtype: could a single study suffice? Journal of Neurology, Neurosurgery & Psychiatry, 86(1), 115-119.
https://doi.org/10.1136/jnnp-2014-307815
|
| [8] |
Basse AM, Boubacar S, Sow AD, et al. Epidemiology of acute polyradiculoneuritis at Fann Department of Neurology Dakar, Senegal. Clin Neurol Neurosci. 2017; 1(4): 76-79.
https://doi.org/10.11648/j.cnn.20170104.11
|
| [9] |
Joshua Saisha, Margaret M. Mweshi, Martha Banda-Chalwe, Loveness A. Nkhata, Elliot Kafumukache, Micah Simpamba, Namalambo Mwenda - Ng’uni. The Prevalence of Guillain-Barre Syndrome and the Rate of Physiotherapy Referral at the University Teaching Hospital, Lusaka, Zambia. International Journal of Neurologic Physical Therapy. Vol. 2, No. 1, 2015, pp. 1-4.
https://doi.org/10.11648/j.ijnpt.20160201.11
|
| [10] |
Muindi SK, Onyango M, Masika MM. Demographic and clinical characteristics of Guillain-Barre syndrome at Kenyatta National Hospital, Kenya. BMJ Neurol Open. 2025; 7(1): e001074.
https://doi.org/10.1136/bmjno-2025-001074
|
| [11] |
Hughes RA, Swan AV, van Doorn PA. Intravenous immunoglobulin for Guillain-Barre syndrome. Cochrane Database Syst Rev. 2014 Sep 19; 2014(9): CD002063.
https://doi.org/10.1002/14651858.CD002063
|
| [12] |
WHO Model List of Essential Medicines, regional analyses, 2021.
|
| [13] |
Bayu HT, Demilie AE, Molla MT, Kumie FT, Endeshaw AS. Mortality and its predictors among patients with Guillain-Barre syndrome in the intensive care unit of a low-income country, Ethiopia: a multicenter retrospective cohort study. Front Neurol. 2024 Oct 30; 15: 1484661.
https://doi.org/10.3389/fneur.2024.1484661
|
| [14] |
Kaur S, Khan S, Iqbal J, et al. Predictors of mechanical ventilation and mortality in patients with Guillain-Barre syndrome: a tertiary care experience from Pakistan. J Pak Med Assoc. 2019; 69(6): 837-842.
|
| [15] |
Khan Z, Al-Barry M, Ahmed N, et al. Clinical profile and outcome of patients with Guillain-Barre syndrome in a tertiary care hospital in Pakistan. Pak J Med Sci. 2017; 33(2): 378-382.
|
| [16] |
Khan SI, Rahman A, Sarker MS, et al. Outcome of Guillain-Barre syndrome patients in a low-resource country: a prospective observational study. PLoS One. 2020; 15(6): e0234111.
https://doi.org/10.1371/journal.pone.0234111
|
Cite This Article
-
APA Style
Labodi, L. D., Alassane, Z., Melody, G. Z., Agathe, C. E., Fabienne, K., et al. (2026). Management and Progression of Guillain-Barre Syndrome in a Resource-limited Setting: A Multicenter Study in the University Hospitals of Ouagadougou, Burkina Faso. Clinical Neurology and Neuroscience, 10(1), 5-14. https://doi.org/10.11648/j.cnn.20261001.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Labodi, L. D.; Alassane, Z.; Melody, G. Z.; Agathe, C. E.; Fabienne, K., et al. Management and Progression of Guillain-Barre Syndrome in a Resource-limited Setting: A Multicenter Study in the University Hospitals of Ouagadougou, Burkina Faso. Clin. Neurol. Neurosci. 2026, 10(1), 5-14. doi: 10.11648/j.cnn.20261001.12
Copy
|
Download
AMA Style
Labodi LD, Alassane Z, Melody GZ, Agathe CE, Fabienne K, et al. Management and Progression of Guillain-Barre Syndrome in a Resource-limited Setting: A Multicenter Study in the University Hospitals of Ouagadougou, Burkina Faso. Clin Neurol Neurosci. 2026;10(1):5-14. doi: 10.11648/j.cnn.20261001.12
Copy
|
Download
-
@article{10.11648/j.cnn.20261001.12,
author = {Lompo Djingri Labodi and Zoungrana Alassane and Gnampa Zeinab Melody and Carama Emeline Agathe and Kere Fabienne and Napon Christian and Millogo Athanase},
title = {Management and Progression of Guillain-Barre Syndrome in a Resource-limited Setting: A Multicenter Study in the University Hospitals of Ouagadougou, Burkina Faso},
journal = {Clinical Neurology and Neuroscience},
volume = {10},
number = {1},
pages = {5-14},
doi = {10.11648/j.cnn.20261001.12},
url = {https://doi.org/10.11648/j.cnn.20261001.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cnn.20261001.12},
abstract = {Introduction: Guillain-Barre syndrome (GBS) faces many diagnostic and therapeutic challenges in sub-Saharan Africa, negatively impacting patient prognosis. The aim of this study was to describe the therapeutic and evolutionary modalities of GBS in the university hospitals of Ouagadougou, Burkina Faso. Patients and methods: This was a descriptive cross-sectional study with prospective data collection, conducted in the university hospitals of Ouagadougou (Yalgado Ouedraogo, Tengandogo, Bogodogo) from March 2018 to May 2022. Patients aged ˃ 16 years admitted for GBS according to the modified Brighton criteria were included. Clinical severity at the time of admission and at the end of hospitalization was assessed using the GBS Disability Score (GBSDS). Socio-demographic, clinical, therapeutic, and in-hospital progression data were analyzed. Results: A total of 79 patients were consecutively hospitalized for GBS, with a mean age of 38 years and a male-to-female ratio of 1.25. The mean time to admission was 22 days. The clinical picture consisted of hypo- or areflexic tetraparesis/plegia (100%) with respiratory muscle deficit (44.3%), cranial nerve involvement (58.2%), dysautonomia (55.7%), and albumin-cytological dissociation (100%). ENMG showed demyelinating and axonal forms in 57.6% and 42.4% of cases, respectively. At the plateau phase, 36% and 21% of patients had very severe deficits (Guillain-Barre Syndrome Disability Score (GBSDS 4)) and respiratory distress (GBSDS 5), respectively. Corticosteroid therapy (58.2%) and intravenous immunoglobulins (IVIg) (6.8%) were the specific therapies used. Infectious complications (41.8%), particularly inhalation pneumonia (27.8%), acute respiratory distress (13.9%), and cardiac dysautonomia complications (6.3%), were the most common hospital complications. Eighteen patients (22.8%) were transferred to intensive care, mainly due to the onset of respiratory distress (13.9%). At the end of hospitalization, the hospital mortality rate was 22.8%, with acute respiratory distress (44.4%) and dysautonomic cardiac arrest (16.7%) being the most common immediate causes of death. Conclusion: In Burkina Faso, GBS is confronted with delays in patient admission, low availability and access to IVIG and EP, and high hospital mortality. Early admission and improved access to emergency immunotherapy and intensive care beds in ASS will help improve the prognosis for patients with GBS.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Management and Progression of Guillain-Barre Syndrome in a Resource-limited Setting: A Multicenter Study in the University Hospitals of Ouagadougou, Burkina Faso
AU - Lompo Djingri Labodi
AU - Zoungrana Alassane
AU - Gnampa Zeinab Melody
AU - Carama Emeline Agathe
AU - Kere Fabienne
AU - Napon Christian
AU - Millogo Athanase
Y1 - 2026/02/25
PY - 2026
N1 - https://doi.org/10.11648/j.cnn.20261001.12
DO - 10.11648/j.cnn.20261001.12
T2 - Clinical Neurology and Neuroscience
JF - Clinical Neurology and Neuroscience
JO - Clinical Neurology and Neuroscience
SP - 5
EP - 14
PB - Science Publishing Group
SN - 2578-8930
UR - https://doi.org/10.11648/j.cnn.20261001.12
AB - Introduction: Guillain-Barre syndrome (GBS) faces many diagnostic and therapeutic challenges in sub-Saharan Africa, negatively impacting patient prognosis. The aim of this study was to describe the therapeutic and evolutionary modalities of GBS in the university hospitals of Ouagadougou, Burkina Faso. Patients and methods: This was a descriptive cross-sectional study with prospective data collection, conducted in the university hospitals of Ouagadougou (Yalgado Ouedraogo, Tengandogo, Bogodogo) from March 2018 to May 2022. Patients aged ˃ 16 years admitted for GBS according to the modified Brighton criteria were included. Clinical severity at the time of admission and at the end of hospitalization was assessed using the GBS Disability Score (GBSDS). Socio-demographic, clinical, therapeutic, and in-hospital progression data were analyzed. Results: A total of 79 patients were consecutively hospitalized for GBS, with a mean age of 38 years and a male-to-female ratio of 1.25. The mean time to admission was 22 days. The clinical picture consisted of hypo- or areflexic tetraparesis/plegia (100%) with respiratory muscle deficit (44.3%), cranial nerve involvement (58.2%), dysautonomia (55.7%), and albumin-cytological dissociation (100%). ENMG showed demyelinating and axonal forms in 57.6% and 42.4% of cases, respectively. At the plateau phase, 36% and 21% of patients had very severe deficits (Guillain-Barre Syndrome Disability Score (GBSDS 4)) and respiratory distress (GBSDS 5), respectively. Corticosteroid therapy (58.2%) and intravenous immunoglobulins (IVIg) (6.8%) were the specific therapies used. Infectious complications (41.8%), particularly inhalation pneumonia (27.8%), acute respiratory distress (13.9%), and cardiac dysautonomia complications (6.3%), were the most common hospital complications. Eighteen patients (22.8%) were transferred to intensive care, mainly due to the onset of respiratory distress (13.9%). At the end of hospitalization, the hospital mortality rate was 22.8%, with acute respiratory distress (44.4%) and dysautonomic cardiac arrest (16.7%) being the most common immediate causes of death. Conclusion: In Burkina Faso, GBS is confronted with delays in patient admission, low availability and access to IVIG and EP, and high hospital mortality. Early admission and improved access to emergency immunotherapy and intensive care beds in ASS will help improve the prognosis for patients with GBS.
VL - 10
IS - 1
ER -
Copy
|
Download