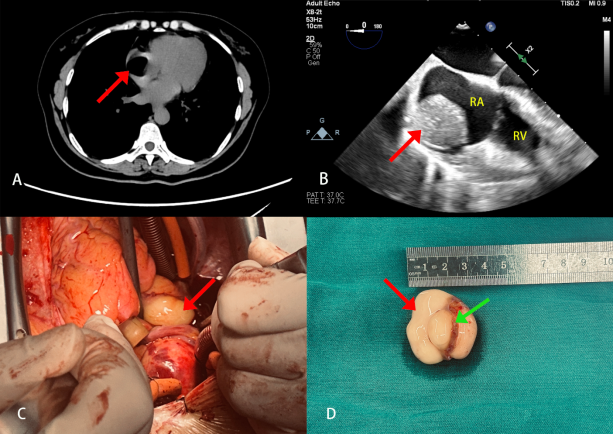
Primary cardiac tumors are a relatively rare disease. About 75% of primary cardiac tumors are benign. The most common histological type is myxoma, followed by cardiac fibroma, lipoma, etc. We report a case of a 53-year-old female patient admitted to the hospital due to "repeated palpitations and tightness of breath for 5 years, worsened for 2 days." Preoperative transthoracic echocardiography revealed a hypoechoic mass approximately 3.1 cm x 3.0 cm in size within the right atrium, suggesting an intracardiac mass: nature? Chest computed tomography (CT) indicated a fat-density nodule within the right atrium, with a larger cross-sectional size of about 3.0 cm x 2.5 cm, suggesting a lipoma. The patient underwent excision of the right atrial mass under cardiopulmonary bypass. Intraoperative transesophageal echocardiography (TEE) revealed a mass within the right atrium, closely connected to the atrial wall, with no signs of tricuspid valve obstruction. Exploration during surgery revealed a yellow, smooth-surfaced mass approximately 3.0 cm x 3.0 cm in size, penetrating the right atrial wall, from which the mass and an additional 2mm margin of the right atrial wall were completely excised. A suitable-sized bovine pericardial patch was used to repair the defect in the right atrial wall. Postoperative TEE showed the disappearance of the right atrial mass. The postoperative pathological result indicated a lipoma. Cardiac lipoma is a rare benign primary cardiac tumor. The common sites of occurrence of this tumor are the right atrium, left ventricle, and pericardium. Based on their location, cardiac lipomas can be divided into three types: subepicardial, intramyocardial, and subendocardial lipomas, with subendocardial lipomas being the most common, accounting for over 50% of primary cardiac lipomas. Clinical symptoms largely depend on the size and growth location of the tumor, and it is generally believed that most cardiac lipomas are asymptomatic. Symptomatic lipomas can be treated with curative surgical excision. Transmural lipomas of the right atrium are relatively rare, and such lipomas may affect adjacent structures both inside and outside the atrial wall. Although the lipoma in this case did not significantly affect valve function or blood flow, the patient experienced repeated symptoms of palpitations and tightness of breath. Despite being a benign tumor, the lipoma in this case exhibited transmural growth within the right atrium, showing a certain degree of invasiveness, making surgical excision an effective treatment method.
| Published in | Cardiology and Cardiovascular Research (Volume 8, Issue 2) |
| DOI | 10.11648/j.ccr.20240802.15 |
| Page(s) | 78-82 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Right Atrium, Transmural, Lipoma
CT | Computed Tomography |
TEE | Transesophageal Echocardiography |
RA | Right Atrium |
RV | Right Ventricle |
LHIS | Lipomatous Hypertrophy of the Interatrial Septum |
MRI | Magnetic Resonance Imaging |
| [1] | Wu S, Teng P, Zhou Y, Ni Y. A rare case report of giant epicardial lipoma compressing the right atrium with septal enhancement. J Cardiothorac Surg. 2015 Nov 5; 10: 150. |
| [2] | Petris AO, Alexandrescu DM, Costache II. Cardiac tumors. Rev Med Chir Soc Med Nat Iasi. 2014 Apr-Jun; 118(2): 289-92. |
| [3] | Ismail I, Al-Khafaji K, Mutyala M, Aggarwal S, et al. Cardiac lipoma. J Community Hosp Intern Med Perspect. 2015 Oct 19; 5(5): 28449. |
| [4] | Elbardissi AW, Dearani JA, Daly RC, Mullany CJ, et al. Survival after resection of primary cardiac tumors: a 48-year experience. Circulation. 2008 Sep 30; 118(14 Suppl): S7-15. |
| [5] | Shu S, Wang J, Zheng C. From pathogenesis to treatment, a systemic review of cardiac lipoma. J Cardiothorac Surg. 2021 Jan 6; 16(1): 1. |
| [6] | Ren DY, Fuller ND, Gilbert SAB, Zhang Y. Cardiac Tumors: Clinical Perspective and Therapeutic Considerations. Curr Drug Targets. 2017; 18(15): 1805-1809. |
| [7] | Rocha RV, Butany J, Cusimano RJ. Adipose tumors of the heart. J Card Surg. 2018 Aug; 33(8): 432-437. |
| [8] | Li FP, Wang XF, Xiao J, Xiao YB. Myocardial lipomatous infiltration of the left ventricular wall. J Card Surg. 2010 Sep; 25(5): 513-5. |
| [9] | D'Souza J, Shah R, Abbass A, Burt JR, et al. Invasive Cardiac Lipoma: a case report and review of literature. BMC Cardiovasc Disord. 2017 Jan 14; 17(1): 28. |
| [10] | Censi S, Squeri A, Baldelli M, Parizi ST. Ischemic stroke and incidental finding of a right atrial lipoma. J Cardiovasc Med (Hagerstown). 2013 Dec; 14(12): 905-6. |
| [11] |
Khalili A, Ghaffari S, Jodati A, Shokoohi B, et al. Giant right atrial lipoma mimicking tamponade. Asian Cardiovasc Thorac Ann. 2015 Mar; 23(3): 317-9.
https://doi.org/10.1177/0218492313504938 Epub 2013 Nov 19 |
| [12] | Cannavale G, Francone M, Galea N, Vullo F, et al. Fatty Images of the Heart: Spectrum of Normal and Pathological Findings by Computed Tomography and Cardiac Magnetic Resonance Imaging. Biomed Res Int. 2018 Jan 9; 2018: 5610347. |
| [13] | Shamsi F, Bajwa G, Ghalib H. "Left ventricular lipoma, a rare case", case report. J Cardiothorac Surg. 2020 May 12; 15(1): 85. |
| [14] | Sun X, Liu G, Kim H, Sun W. Left ventricular lipoma resected using thoracoscope-assisted limited sternotomy: A case report and literature review. Medicine (Baltimore). 2018 Aug; 97(31): e11436. |
| [15] | Wijesurendra RS, Sheppard KA, Westaby S, Ormerod O, et al. The many faces of cardiac lipoma-an egg in the heart! Eur Heart J Cardiovasc Imaging. 2017 Jul 1; 18(7): 821. |
APA Style
Song, L., Li, X. (2024). A Case of Transmural Lipoma of the Right Atrium. Cardiology and Cardiovascular Research, 8(2), 78-82. https://doi.org/10.11648/j.ccr.20240802.15
ACS Style
Song, L.; Li, X. A Case of Transmural Lipoma of the Right Atrium. Cardiol. Cardiovasc. Res. 2024, 8(2), 78-82. doi: 10.11648/j.ccr.20240802.15
AMA Style
Song L, Li X. A Case of Transmural Lipoma of the Right Atrium. Cardiol Cardiovasc Res. 2024;8(2):78-82. doi: 10.11648/j.ccr.20240802.15
@article{10.11648/j.ccr.20240802.15,
author = {Lin Song and Xuejie Li},
title = {A Case of Transmural Lipoma of the Right Atrium
},
journal = {Cardiology and Cardiovascular Research},
volume = {8},
number = {2},
pages = {78-82},
doi = {10.11648/j.ccr.20240802.15},
url = {https://doi.org/10.11648/j.ccr.20240802.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ccr.20240802.15},
abstract = {Primary cardiac tumors are a relatively rare disease. About 75% of primary cardiac tumors are benign. The most common histological type is myxoma, followed by cardiac fibroma, lipoma, etc. We report a case of a 53-year-old female patient admitted to the hospital due to "repeated palpitations and tightness of breath for 5 years, worsened for 2 days." Preoperative transthoracic echocardiography revealed a hypoechoic mass approximately 3.1 cm x 3.0 cm in size within the right atrium, suggesting an intracardiac mass: nature? Chest computed tomography (CT) indicated a fat-density nodule within the right atrium, with a larger cross-sectional size of about 3.0 cm x 2.5 cm, suggesting a lipoma. The patient underwent excision of the right atrial mass under cardiopulmonary bypass. Intraoperative transesophageal echocardiography (TEE) revealed a mass within the right atrium, closely connected to the atrial wall, with no signs of tricuspid valve obstruction. Exploration during surgery revealed a yellow, smooth-surfaced mass approximately 3.0 cm x 3.0 cm in size, penetrating the right atrial wall, from which the mass and an additional 2mm margin of the right atrial wall were completely excised. A suitable-sized bovine pericardial patch was used to repair the defect in the right atrial wall. Postoperative TEE showed the disappearance of the right atrial mass. The postoperative pathological result indicated a lipoma. Cardiac lipoma is a rare benign primary cardiac tumor. The common sites of occurrence of this tumor are the right atrium, left ventricle, and pericardium. Based on their location, cardiac lipomas can be divided into three types: subepicardial, intramyocardial, and subendocardial lipomas, with subendocardial lipomas being the most common, accounting for over 50% of primary cardiac lipomas. Clinical symptoms largely depend on the size and growth location of the tumor, and it is generally believed that most cardiac lipomas are asymptomatic. Symptomatic lipomas can be treated with curative surgical excision. Transmural lipomas of the right atrium are relatively rare, and such lipomas may affect adjacent structures both inside and outside the atrial wall. Although the lipoma in this case did not significantly affect valve function or blood flow, the patient experienced repeated symptoms of palpitations and tightness of breath. Despite being a benign tumor, the lipoma in this case exhibited transmural growth within the right atrium, showing a certain degree of invasiveness, making surgical excision an effective treatment method.
},
year = {2024}
}
TY - JOUR T1 - A Case of Transmural Lipoma of the Right Atrium AU - Lin Song AU - Xuejie Li Y1 - 2024/06/14 PY - 2024 N1 - https://doi.org/10.11648/j.ccr.20240802.15 DO - 10.11648/j.ccr.20240802.15 T2 - Cardiology and Cardiovascular Research JF - Cardiology and Cardiovascular Research JO - Cardiology and Cardiovascular Research SP - 78 EP - 82 PB - Science Publishing Group SN - 2578-8914 UR - https://doi.org/10.11648/j.ccr.20240802.15 AB - Primary cardiac tumors are a relatively rare disease. About 75% of primary cardiac tumors are benign. The most common histological type is myxoma, followed by cardiac fibroma, lipoma, etc. We report a case of a 53-year-old female patient admitted to the hospital due to "repeated palpitations and tightness of breath for 5 years, worsened for 2 days." Preoperative transthoracic echocardiography revealed a hypoechoic mass approximately 3.1 cm x 3.0 cm in size within the right atrium, suggesting an intracardiac mass: nature? Chest computed tomography (CT) indicated a fat-density nodule within the right atrium, with a larger cross-sectional size of about 3.0 cm x 2.5 cm, suggesting a lipoma. The patient underwent excision of the right atrial mass under cardiopulmonary bypass. Intraoperative transesophageal echocardiography (TEE) revealed a mass within the right atrium, closely connected to the atrial wall, with no signs of tricuspid valve obstruction. Exploration during surgery revealed a yellow, smooth-surfaced mass approximately 3.0 cm x 3.0 cm in size, penetrating the right atrial wall, from which the mass and an additional 2mm margin of the right atrial wall were completely excised. A suitable-sized bovine pericardial patch was used to repair the defect in the right atrial wall. Postoperative TEE showed the disappearance of the right atrial mass. The postoperative pathological result indicated a lipoma. Cardiac lipoma is a rare benign primary cardiac tumor. The common sites of occurrence of this tumor are the right atrium, left ventricle, and pericardium. Based on their location, cardiac lipomas can be divided into three types: subepicardial, intramyocardial, and subendocardial lipomas, with subendocardial lipomas being the most common, accounting for over 50% of primary cardiac lipomas. Clinical symptoms largely depend on the size and growth location of the tumor, and it is generally believed that most cardiac lipomas are asymptomatic. Symptomatic lipomas can be treated with curative surgical excision. Transmural lipomas of the right atrium are relatively rare, and such lipomas may affect adjacent structures both inside and outside the atrial wall. Although the lipoma in this case did not significantly affect valve function or blood flow, the patient experienced repeated symptoms of palpitations and tightness of breath. Despite being a benign tumor, the lipoma in this case exhibited transmural growth within the right atrium, showing a certain degree of invasiveness, making surgical excision an effective treatment method. VL - 8 IS - 2 ER -
Department of Anesthesiology, West China Hospital, Sichuan University and The Research Units of West China (2018RU012), Chinese Academy of Medical Sciences, Chengdu, China
Department of Anesthesiology, West China Hospital, Sichuan University and The Research Units of West China (2018RU012), Chinese Academy of Medical Sciences, Chengdu, China
Information