Abstract
Introduction: Despite the progress made, access to sexual and reproductive health (SRH) in sub-Saharan Africa (SSA) in general, and in the DRC in particular, faces major obstacles, resulting in high rates of maternal mortality, unwanted pregnancies, and sexually transmitted infections (STIs). The challenges currently being faced include the unavailability of reproductive health services, geographical inaccessibility, cultural and religious norms, stigmatization, and low levels of maternal education. Methodology: This observational cross-sectional study focuses on the knowledge, attitudes and practices of women of childbearing age (15 to 49 years) regarding family planning in the Mugunga health area, located in the Karisimbi health zone, city of Goma, in the east of the Democratic Republic of Congo (DRC). This research covers a short period of six months from 1 October 2024 to 31 March 2025. Data collection, entry and recording were carried out using the Open Data Kit Collect (KoBoToolbox) software, while the analysis was carried out on the statistics product and service solution (SPSS) software version 27.0. The Pearson Chi-Square (X2) statistical test was applied in this research. Results: Significant socio-demographic factors associated with low use of family planning services using modern contraceptive methods are single marital status (x² = 236.108), young age of study participants (x² = 155.83), low level of education of participants (x2 = 69.90), and low number of children at the time of the study (maximum of 2 children) (x2 = 161.69). Conclusion: adherence to modern family planning methods remains low in our study setting. Several socio-demographic, cultural and religious factors contribute to this low proportion. Promoting maternal and child health through community health workers would help improve adherence to modern family planning (FP).
|
Published in
|
Central African Journal of Public Health (Volume 12, Issue 1)
|
|
DOI
|
10.11648/j.cajph.20261201.14
|
|
Page(s)
|
34-45 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Factors, Family Planning, Adherence
1. Introduction
Sexual and reproductive health (SRH) is defined as a state of physical, mental and social well-being related to sexuality and reproduction. This approach obviously encompasses the right of every individual to decide about their sexual life, to have fulfilling and safe sexual relations, to have access to different methods of contraception and sex education, to treatment for sexually transmitted infections (STIs), and to maternal and child health services without any hindrance.
However, in many regions worldwide, the right to sexual and reproductive health is not systematically guaranteed. For instance, in 2021, 164 million women of reproductive age, amounting to 1.1 billion individuals, lacked access to modern contraceptive methods for various reasons
. This persistent situation would therefore justify the high maternal mortality rate of 249 maternal deaths per 100,000 live births recorded in 2021. The same data demonstrate that sub-Saharan Africa and South Asia accounted for 87% of global maternal deaths during the same period
| [2] | Sossoukpè N, Koufèdé R, Dénakpo N and Adjoavi M. Epidemiological characteristics of maternal deaths in the department of Couffo, Benin, January 2018-June 2022. Journal of Interventional Epidemiology and Public Health. 2025; 8(1): 6.
https://doi.org/10.37432/jieph.supp.2025.8.2.12 |
[2]
.
Unwanted pregnancies are also a result of problems accessing modern birth control. Right now, one in three young women under 20 is affected, and the highest rates are in sub-Saharan Africa. This is a big problem for public health and women's reproductive rights
| [3] | Ndayisenga JP, Oudshoorn A, Babenko-Mould Y, Jackson KT, Hynie M, Mukamana D, Uwajeneza P, Musabirema P. A narrative review of the literature on unintended adolescent pregnancies: Understanding their meaning, associated factors, and consequences. Afr J Reprod Health. 2025; 29(8): 154-172.
https://doi.org/10.29063/ajrh2025/v29i8.15 |
[3]
. On top of that, the ethical dilemma of illegal abortions due to limited access to sexual and reproductive health services is also responsible for preventable maternal deaths each year around the world
| [4] | Elomrani S, Utz B, De Brouwere V, Kajjoune I, Assarag B. Abortion in Morocco and a turn to tragedy: women and healthcare professionals speak out! A cross-sectional mixed-methods study in AgadirSex Reprod Health Matters. 2023; 31(5): 2279371.
https://doi.org/10.1080/26410397.2023.2279371 |
[4]
.
In Africa, it is very important to use contraceptives to reduce maternal and infant mortality, improve the health of women of childbearing age and their infants, support the continent's economic development and, finally, enable women to better plan their families, according to reliable information available on sexual and reproductive health.
A multicentric study involving 20 countries shows that the rate of use of these contraceptive methods remains low in sub-Saharan Africa, with an average overall prevalence of 20% and extreme prevalences of 6% in Guinea and 62% in Zimbabwe
| [5] | Apanga P, Kumbeni M, Ayamga E, Ulanja M and Akparibo R. Prevalence and factors associated with modern contraceptive use among women of reproductive age in 20 African countries: a large population-based study. BMJ Open. 2020; 10: e041103. https://doi.org/10.1136/bmjopen-2020-041103 |
[5]
. The documented determinants of this low adherence to contraceptive use are low levels of maternal education, disparities in access to accurate information, the unavailability of sexual and reproductive health services, particularly in rural areas, geographical constraints, financial limitations related to healthcare and transport costs, a shortage of qualified health personnel, socio-cultural barriers, and religious pressures
| [6] | Admasu K, Tamir T, Alemu M, Zeleke G and Zegeye A. Prevalence and determinants of exposure to family planning messages among reproductive age women in five Sub-Saharan African countries: a multilevel analysis of 2021-2023 demographic and health surveys. BMC Womens Health. 2025; 25(1): 365. https://doi.org/10.1186/s12905-025-03895-w |
| [7] | Dwomoh D, Amuasi S, Amoah E, Ama S, Gborgbortsi W and Tetteh J. Exposure to family planning messages and contraceptive use among women of reproductive age in sub-Saharan Africa: a cross-sectional program impact evaluation study. Sci Rep. 2022; 12: 18941.
https://doi.org/10.1038/s41598-022-22525-1 |
| [8] | Dramé L, Kolié D, Sidibé S, Yombouno J et Delamou A. The factors associated with contraceptive use among young female students in rural Guinea. Public Health 2023; 6(35): 129 à 140. https://doi.org/10.3917/spub.236.0129 |
| [9] | Sifora KK, De Wet-Billings N, Frade-Bekker S, Phiri M. Individual and community level factors influencing modern contraceptive use among women of reproductive age in South Africa: a multilevel analysis. Contracept Reprod Med. 2025; 10(1): 53. https://doi.org/10.1186/s40834-025-00392-1 |
[6-9]
.
Similar findings have also been reported in southern Africa, where few women who are able to have children use contraceptive methods: 57.3% in South Africa, 60.5% in Namibia, 43.9% in Zambia and 60% in Zimbabwe among HIV-positive women
| [10] | Michael T, Ojo T, Ijabadeniyi O, Ibikunle M, Oni J and Agboola A. Prevalence and factors associated with contraceptive use among sexually active adolescent girls in 25 sub-Saharan African countries. PLoS One. 2024; 19(2): e0297411. https://doi.org/10.1371/journal.pone.0297411 |
| [11] | Singata-Madliki M, Carayon-Lefebvre d'Hellencourt F, Lawrie TA, Balakrishna Y and Hofmeyr GJ. Effects of three contraceptive methods on depression and sexual function: An ancillary study of the ECHO randomized trial. Int J Gynaecol Obstet. 2021; 154(2): 256-262.
https://doi.org/10.1002/ijgo.13594 |
| [12] | Musuka G, Murewanhema G, Mukandavire Z, Chingombe I, Cuadros D, Mutenherwa F, Dzinamarira T, Eghtessadi R, Malunguza N and Mapingure M. HIV status and contraceptive use in Zimbabwe among sexually active adolescent girls and women: Secondary analysis of Zimbabwe Demographic Health survey data. S Afr Med J. 2024; 114(6b): e1407.
https://doi.org/10.11604/pamj.2022.41.262.32615 |
[10-12]
. The immediate consequences of this situation among young adolescents are early pregnancies, school dropouts and risky abortions.
East Africa, for its part, has a relatively low overall prevalence of contraceptive use, at around 33.8%, with significant disparities between different countries on the continent. The data collected reveal that the highest rates of use are recorded in Zambia (43.9%) and Kenya (42.0%), followed by Madagascar, Rwanda and Uganda, with rates above 30%. In contrast, Burundi has the lowest rate of modern contraceptive use in the region, at 14.7%, while Ethiopia, Tanzania and Mozambique also have lower rates, ranging from 25% to 30%
| [13] | Mankelkl G and Kinfe B. Pooled prevalence of modern contraceptive utilization and its associated factors among reproductive age women in East Africa: derived from demographic and health surveys. J Health Popul Nutr. 2025; 44: 261.
https://doi.org/10.1186/s41043-025-01019-6 |
[13]
.
Many factors are associated with this low use of modern contraceptives in this part of Africa, including maternal education level, occupation, religion, number of children, distance from health facilities, history of pregnancy termination, desire to have children, number of decisions in which women participate, births in the last five years, country of residence, and place of residence.
West Africa is not spared from women's low adherence to modern contraceptive methods. Very low rates are reported in Guinea-Conakry (12.8%), Niger (23%), Burkina Faso (30.1%), Senegal (23%)
| [14] | Youla Y, Sidibé S, Kourouma M, Camara S, Bangoura S, Olivier K, Grovogui M, Diaby M, Bongono E, Diallo O, Conté I, Traoré S, Djigui Keita A, Touré A and Delamou A. Prevalence and factors associated with the use of modern contraceptive methods among female healthcare providers in health facilities in Guinea. Front. Glob. Women’s Health. 2025; 1(6): 1-8.
https://doi.org/10.3389/fgwh |
[14]
, and Mali (35%)
| [15] | Kanthé D, Samaké Y, Koné O, Fomba D, Bagayoko TB, Kéita M, Samaké B, Kéita S, Traoré M, Dembélé BT, Togo AP. Determinants of Low Modern Contraceptive Prevalence in the Markala Health District: Case of the Diamarabougou Community Health Center Mali. Health Sciences and Disease. 2023; 24(7): 121-132.
https://doi.org/10.5281/hsd.v24i7.4613 |
[15]
.
In the Democratic Republic of Congo (DRC), data collected by the National Health Information System (SNIS) reveal that only 40% of health facilities report providing family planning services to the population
| [16] | Kwete D, Binanga A, Mukaba T, Nemuandjare T, Mbadu M, Kyungu M, Sutton P, Bertrand JT. Family Planning in the Democratic Republic of the Congo: Encouraging Momentum, Formidable Challenges. Glob Health Sci Pract. 2018 Mar 30; 6(1): 40-54.
https://doi.org.10.9745/GHSP-D-17-00346. |
[16]
. The national proportion of married women of childbearing age using modern contraceptive methods in this country is very low. It rose from 7.8% in 2014 to 10.7% in 2024
. The main obstacles identified are political instability, geographical inaccessibility due to inadequate road infrastructure in a country of continental dimensions, lack of regular funding to purchase adequate quantities of contraceptives, difficulties in the supply chain, inadequate transport logistics, inappropriate storage and cultural barriers.
Demographic data reveals that in North Kivu province, Eastern DRC, 39% of the reproductive-age population's needs are not being met, while in South Kivu province, the figure is 35%. In North Kivu province, the use of modern contraceptive methods remains insufficient. Data collected reveals that the use of these methods represents barely 20% of the population, a figure significantly higher than the national average estimated at 10.7% in 2024
.
A recent study conducted in the city of Kisangani, located in the eastern province, in 2025, revealed that the use of contraceptive methods remains marginal in this locality. Some respondents perceive the use of modern contraceptive methods as a form of shirking responsibility and a vector for prostitution. In addition, these same individuals express fears about potential side effects, such as cervical cancer, infertility, menstrual disorders, weight loss or obesity, and headaches. Socio-cultural factors, such as negative perceptions by husbands, religious beliefs and limited information, are the main reasons for the use of natural and traditional methods
| [18] | Koto-Te-Nyiwa Ngbolua J.-P, Mukandu B, Wembodinga U, Ngbolua K and Mbungu M. Perceptions and obstacles to the use of modern contraceptive methods among multiparous women in Kisangani, Democratic Republic of Congo. Revue Africaine des Sciences Sociales. 2025; 7(1), 313-328.
https://doi.org/10.4314/orapj.v6i2.18 |
[18]
.
In the provinces of North and South Kivu, despite low rates of modern contraceptive use, the intention to use modern family planning methods is significantly linked to high levels of maternal education and marital status
| [19] | Bapolisi W, Bisimwa G, Merten S. Barriers to family planning use in the Eastern Democratic Republic of Congo: an application of the theory of planned behaviors using a longitudinal survey. BMJ Open. 2023; 13(2): e061564.
https://doi.org/10.1136/bmjopen-2022-061564 |
[19]
. However, key barriers remain, including poor communication between spouses, socio-cultural constraints, religious prohibitions, fear of adverse effects, and lack of knowledge.
To our knowledge, no studies have been conducted to date in the Karisimbi health zone in the city of Goma on barriers to adherence to modern contraceptive methods. The main objective of this study is to identify the significant determinants associated with low adherence to modern contraceptive methods among women of reproductive age (15-49 years) in our study setting. A better overall understanding of the significant determinants will enable us to propose recommendations aimed at increasing the rates of modern contraceptive use in the Karisimbi health zone in Goma.
2. Materials and Methods
2.1. Study Site, Type and Period
This observational cross-sectional study focuses on the knowledge, attitudes and practices of women of childbearing age (15 to 49 years) regarding family planning in the Mugunga health area, located in the Karisimbi health zone, city of Goma, in the east of the Democratic Republic of Congo (DRC), which has experienced three decades of armed conflict, followed by persistent insecurity in the city of Goma, negatively impacting maternal and child health in this part of the country. This research covers a short period of six months from 1 October 2024 to 31 March 2025.
The Mugunga neighborhood is located west of downtown Goma, along National Road No. 2 (RN2). It is bordered to the north by a straight line extending the northern boundary of the Ndosho neighborhood. To the south by the Goma-Sake Road. To the west by Virunga National Park and finally, to the east by the Ndosho neighborhood.
In terms of climate, the Mugunga health area has a tropical mountain climate with two distinct seasons: the dry season and the rainy season. The dry season is characterized by higher temperatures and low rainfall. The rainy season is marked by regular rainfall and cooler temperatures, with an average of 25°C.
Historically, it is established that the Mugunga neighborhood was formerly an ancient notability of the Lutale locality, Kamuronza group, Bahunde community in Masisi territory. In the socio-political context of the time, this administrative entity was under the governance of a notable figure, who held the position of village chief. It should be noted that, throughout history, there has been topographical continuity between the Mugunga neighborhood and Lake Vert. It should be emphasized that on 22 May 1989, Mugunga was urbanized and annexed to the city of Goma as a neighborhood by Ordinance Law No. 89-127 of 22 May 1989. As a result of this geographical change, the Mugunga neighborhood now falls under the jurisdiction of the municipality of Karisimbi, while the Lac Vert neighborhood falls under the municipality of Goma.
In demographic terms, following the internal conflict in Rwanda (1990-1994) between the Rwandan Patriotic Front (RPF) army and the Rwandan Armed Forces (FAR), the locality of Mugunga welcomed displaced populations fleeing the conflicts in Rwanda and the repeated armed conflicts in various territories of North Kivu Province. It is therefore inhabited by a vulnerable and socio-economically poor population. It is interesting to note that the topography of the Mugunga neighborhood is like that of the city of Goma, particularly in terms of soil composition. Indeed, it is characterized by a predominance of volcanic rock, combined with areas of slightly sandy soil. This area is characterized by skeletal soil, due to the abundant presence of basalt at shallow depths.
In terms of social and health conditions, living conditions in the Mugunga health area are characterized by poor access to drinking water, food, healthcare and sanitation. Women and children are particularly vulnerable to sexual and gender-based violence, exploitation and abuse, risks that are exacerbated by a lack of privacy and overcrowding. Poor health conditions, due to lack of hygiene and limited access to water, promote waterborne diseases such as cholera and diarrhea. Malnutrition is a major concern, exacerbated by food insecurity and loss of livelihoods. Access to healthcare, which often must be paid for, remains a major obstacle.
2.2. Population, Sample Size, Sampling and Survey Steps
The study population consists of residents of the Mugunga health area, numbering 44,980 individuals in 8,032 households across 20 avenues. The study targets women of reproductive age, i.e. women aged 15 to 49, who represent 21% of the total population. Thus, the total population of women of childbearing age is estimated at 9,446 women. Given the constraints related to the resources and time allocated to data collection, we opted for a methodological approach based on stratified probability sampling. The application of Lychn's formula made it possible to determine the optimal sample size required for our study:
n: sample size.
N: target population.
P: prevalence, which is unknown and therefore estimated at 50% = 0.5.
Z² = standard deviation value at a confidence interval of 1.96.
d: margin of error of 5%.
n = = = = = 366 households corresponding to 366 women of childbearing age to be surveyed. Applying the sample correction formula n= n/1+n.N, our revised sample size is 350.
n = = = 350 households/woman of childbearing age
The following table illustrates that cluster sampling facilitated the retention of 350 households for survey purposes, out of a total of 8,032 households dispersed across 20 avenues within the designated study area. The survey base was the 23rd household in each avenue.
Table 1. Sample presentation and survey steps.
N | Avenues | Households per avenue | Households | Survey basis |
01 | Lushagala | 114 | 5 | 23 |
02 | Rutanda | 255 | 11 | 23 |
03 | Shabindu | 318 | 14 | 23 |
04 | Kashaka | 765 | 33 | 23 |
05 | 17 janvier | 820 | 36 | 23 |
06 | Hewa Bora 1 | 414 | 18 | 23 |
07 | Hewa Bora 2 | 565 | 25 | 23 |
08 | Baraka | 226 | 10 | 23 |
09 | Maendeleo 1 | 741 | 32 | 23 |
10 | Maendeleo 2 | 552 | 24 | 23 |
11 | Rusayo 1 | 496 | 22 | 23 |
12 | Rusayo 2 | 282 | 12 | 23 |
13 | Du Marche | 341 | 15 | 23 |
14 | Mushebere | 465 | 20 | 23 |
15 | Kishanga | 92 | 4 | 23 |
16 | Kalamo | 68 | 3 | 23 |
17 | Ndjili 1 | 520 | 23 | 23 |
18 | Ndjili 2 | 213 | 9 | 23 |
19 | Kahongozi | 412 | 18 | 23 |
20 | Du Ceavu | 373 | 16 | 23 |
| Total | 8032 | 350 | |
2.3. Sample Selection Criteria
To be included in this study, a woman of childbearing age (15-49) living in the Mugunga area, Karisimbi health zone, city of Goma, who was present at the time of the survey, had freely agreed to answer our survey questionary. All women of childbearing age (15-49) not living in the Mugunga area, all women meeting the selection criteria but absent at the time of the survey, and all women of childbearing age who had freely expressed their refusal to answer our survey questionnaire were excluded from this study.
2.4. Data Collection and Analysis Tools
Data collection, entry and recording were carried out using Open Data Kit Collect (KoBoToolbox) software, while analysis was carried out using Statistics Product and Service Solution (SPSS) version 27.0 software. The Pearson Chi-square (X2) statistical test was applied in this study to investigate the relationship of independence or dependence between certain factors and underutilization of family planning services in Karisimbi health zone, Goma city’s, Democratic Republic of Congo. At the 95% confidence interval, the significance level was set at P<0.05. The null hypothesis (H0) was rejected if the calculated chi-square was greater than 3.841 or P>0.05 (significant dependence). However, the null hypothesis (H0) was accepted when the calculated Chi-square was less than 3.841 or P<0.05 (significant independence).
2.5. Variables Measured
The data collection technique used in this study was the use of an interview guide installed in the interviewers' mobile phones. The guide contained open and closed questions depending on the quality of the data to be collected. The open-ended questions concerned the socio-demographic data of the participants, and the knowledge, attitudes and family planning practices of women of childbearing age.
The following variables were measured: age, education level, occupation, marital status and number of children for Socio-demographic characteristics of participants.
3. Results
Table 2. Socio-demographic characteristic of participants.
Variables | N=350 | 100% |
Age (year) | | |
15-20 | 61 | 17.4 |
21-30 | 89 | 25.4 |
31-40 | 148 | 42.3 |
41-49 | 52 | 14.9 |
Education level | | |
Primary | 75 | 21.4 |
Secondary | 171 | 48.9 |
University | 107 | 29.7 |
Occupation | | |
Household | 116 | 33.1 |
Civil Servant | 23 | 06.6 |
Private sector | 38 | 10.9 |
Trader | 102 | 29.1 |
Student | 71 | 20.3 |
Marital satus | | |
Single | 69 | 19.7 |
Married | 174 | 49.7 |
Cohabitation | 86 | 24.6 |
Widowed | 21 | 06.6 |
Number of children | | |
0 | 72 | 20.6 |
1-2 | 187 | 53.4 |
3-5 | 53 | 15.1 |
>5 | 38 | 10.9 |
Analysis of the data in the table above reveals that most respondents (42.3%) are in the 31-40 age bracket, 48.9% have secondary education, most are housewives (33.1%) and shopkeepers (29.1%). Finally, 49.7% of participants are married, while a significant proportion (53.4%) have 1-2 children.
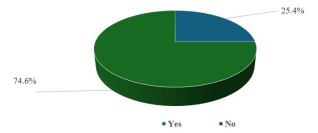
Figure 1 below shows that 261 of the 350 women taking part in this study. 74.6% were not using the family planning service using modern contraceptive methods at the time of our survey, compared with 25.4% who were using these modern methods.
Figure 1. Proportion of women using modern contraceptive methods for family planning in our study area.
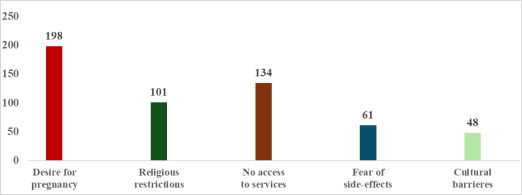
Analysis of diagram 2 below highlights the main reasons for non-use of the family planning service. Most participants (198/350 or 56.6%) wanted to conceive, while 38.3% had difficulty accessing family planning services (138/350). In addition, 28.9% (101/350) observe religious restriction and 17.4% of participants (61/350) mentioned a fear of potential side-effects, including menstrual disorders, overweight or secondary infertility. Finally, cultural barriers such as stigma and misperceptions accounted for 13.7% of the reasons given (48/350).
Figure 2. Reasons for not using modern contraceptive methods for family planning in our study area.
Table 3. Knowledge of the advantages of modern contraceptive methods, duration of use and sources of information for participants.
Variables | N=351 | 100% |
Benefits of using contraceptives | | |
Prevention of unwanted pregnancy | 187 | 53,4 |
Maternity budget reduction | 47 | 13,4 |
Prevents close pregnancies | 96 | 27,4 |
Family balance | 62 | 17,7 |
Prevents sexually-transmitted infections | 67 | 19,1 |
Improves maternal health | 34 | 09,7 |
Type of contraceptive methods available | | |
Condoms | 247 | 70,6 |
Pills | 109 | 31,1 |
Hormonal injections | 32 | 09,1 |
Implants | 69 | 19,7 |
Sexual abstinence | 98 | 28,0 |
Breastfeeding | 35 | 10,0 |
Interrupted coitus | 11 | 03,4 |
Duration of contraceptive use (years) | | |
< 1 | 30 | 08,6 |
1-2 | 57 | 16,3 |
3-5 | 80 | 22,3 |
>5 | 96 | 27,4 |
Don't know | 87 | 24,9 |
Sources of information | | |
Hospital center | 94 | 26,9 |
Radiodiffusion and TV | 59 | 16,9 |
Through a close person | 78 | 22,3 |
Health promotor | 12 | 03,4 |
Don’t know | 107 | 30,6 |
The table shows that the advantage of using modern contraceptive methods most reported by the study participants is the prevention of unwanted pregnancies (53.4%) and the prevention of sexually transmitted infections (19.1%). Condoms and pills were the contraceptive methods with which participants were most familiar (56.3% and 30.3% respectively). Most participants (53.3%) believe that modern contraceptive methods can be used for 3 years or more. A significant proportion (30.6%) did not know where to obtain reliable information on modern contraceptive methods.
Table 4. Socio-demographic factors associated with low adherence to a modern contraceptive method.
Factors | Adherence | to contraceptive | methods | dff | P-value |
Yes N=89 | No N=261 | X2 |
Information source | | | | | |
Don’t know | 00 | 107 | 0,0262 | 4 | 0,8715 |
Hospital Center | 68 | 26 | | | |
Radiodiffusion/TV | 09 | 50 | | | |
A close friend | 10 | 68 | | | |
Health promotor | 02 | 10 | | | |
Marital status | | | | | |
Single | 67 | 02 | 236,108 | 3 | <0,0001 |
Married | 20 | 154 | | | |
Cohabitation | 02 | 84 | | | |
Widowed | 00 | 21 | | | |
Age (year) | | | | | |
< 19 | 49 | 03 | 155,83 | 2 | <0,0001 |
19-35 | 26 | 121 | | | |
>35 | 14 | 138 | | | |
School level | | | | | |
Primary | 51 | 24 | 69,90 | 2 | <0,0001 |
Secondary | 31 | 140 | | | |
University | 07 | 45 | | | |
Number of children | | | | | |
0 | 61 | 11 | 106,3988 | 3 | <0,0001 |
1-2 | 26 | 161 | | | |
3-5 | 02 | 51 | | | |
>5 | 00 | 38 | | | |
A thorough examination of the data presented in
Table 1 indicates that several notable socio-demographic factors are associated with the underutilization of family planning services that utilize modern contraception methods. These factors include the marital status of unmarried women (x2 = 236.108), the age of the study participants (x2 = 155.83), the educational level of the participants (x2 = 69.90), and the number of children the participants have at the time of the study, with a maximum of two children (x2 = 161.69).
Table 5. Socio-cultural and religious determinants associated with low adherence to a modern contraceptive method.
Factors | Adherence | To contraceptive | Methods | dff | P-value |
Yes N=89 | No N=261 | X2 |
Husband’s support | | | | | |
Unfavourable | 06 | 67 | 14,365 | 1 | <0,0002 |
Favourable | 83 | 194 | | | |
Desire for pregnancy | | | | | |
Yes | 02 | 196 | 143,561 | 1 | <0,0001 |
No | 87 | 65 | | | |
Religious restrictions | | | | | |
Yes | 12 | 89 | 13,701 | 1 | <0,0002 |
No | 77 | 172 | | | |
Service accessibility | | | | | |
Difficult | 06 | 128 | 50,118 | 1 | <0,0001 |
Easier | 83 | 133 | | | |
Barrière culturelle | | | | | |
None | 68 | 234 | 2,981 | 2 | 0,225 |
Stigma | 07 | 28 | | | |
Misperception | 14 | 27 | | | |
Fear side- effects | | | | | |
No | 78 | 211 | 2,401 | 3 | 0,493 |
Overweight | 08 | 34 | | | |
Menstrual disorders | 02 | 08 | | | |
Secondary sterility | 01 | 08 | | | |
This analytical table shows that the significant socio-cultural and religious factors associated with low use of modern contraceptive methods are the unfavourable opinion of the spouse does not influence adherence to contraceptive methods (x2 = 14.365), compared with the desire to conceive (x2 = 14.365), which favours low use of family planning services using modern methods. Religious prohibitions (x2 = 13.701) and difficult access to family planning services (x2 = 50.118). However, the absence of cultural barriers and fear of adverse effects are beneficial protective factors for the use of contraceptives. The respective chi-squares calculated were 2.981 for the first factor and 2.401 for the second.
4. Discussions
As a reminder, the main objective of this study was to identify the significant determinants associated with low adherence to modern contraceptive methods among women of childbearing age (15-49 years) in the Karisimbi health zone, located in the city of Goma, in the east of the Democratic Republic of Congo. It is evident that the socio-demographic profile of study participants varies considerably depending on the context, the study environment considered, and, most notably, the objective of the study. The results of the study indicate that 42.3% of the women included in the study were between the ages of 31 and 40. The majority (48.9%) of the subjects had received a secondary education. Most of the subjects in the study were household, constituting 33.1% of the sample, while 29.1% were shopkeepers. The data indicates that 49.7% of the population was married, while a significant proportion (66.8%) had three or more children.
This profile is comparable to the profile described by Ouédraogo S et al. in the Djibo health district in the Sahel region of Burkina Faso, which also exclusively included women of childbearing age (15-49) in the study. In their study, the authors found that 42.2% of the women were between the ages of 21 and 30. A substantial proportion of the women in the study exhibited a low level of education, with 67.8% having received minimal schooling. Furthermore, 69% of the women were married, and 20% were engaged in commercial or agricultural activities
| [20] | Ouédraogo S, Ouattara A, Sarigda M, Ouédraogo L and Ouédraogo C. Prevalence and factors associated with the use of modern contraceptive methods in the health district of Djibo, Sahel region in Burkina Faso. J Interval Epidemiol Public Health. 2023; 6(2): 3.
https://www.doi.org/10.37432/jieph.2023.6.2.80 |
[20]
. The sole discrepancy between the two studies pertained to the study environment. The study by Ouédraogo S et al was conducted in a rural health district, whereas our study was conducted in an urban health zone.
However, the socio-demographic profile described in the two above studies, differs completely from that reported by Masoda M et al., who included only men in their study. Most of these men (37.5%) were between the ages of 50 and 59, and 94.8% of them were married and monogamous. Many of the participants had a low level of primary education (75.7%) and 67.4% were Catholic Christians
| [21] | Masoda MN, Buloze JM, Kabwe AM, Mishika PL, Bondekwe JCA, Mukuku O, Mpoy CW, Ngwala PL, Wembonyama SO, Tsongo ZK. Determinants of family planning use among married men in Idjwi, Democratic Republic of Congo. Journal of Medicine, Public Health and Policy Research. 2022; 2(1): 1-9. |
[21]
. The authors of the study provide a justification for their research by pointing to the influence that males, particularly in developing countries, often have on the use of family planning by couples. The objective of this study on the island of Idjwi, situated in the province of Sud-Kivu in the eastern region of the Democratic Republic of Congo, was to ascertain the substantial impediments to the utilization of modern contraceptive methods by men within their respective study environments. This strategy enabled the development of pertinent community programs, thereby integrating male participation in the selection of family planning methods.
In our study, diagram 1 shows that 261 women out of 350, or 74.6%, were not using the family planning service using modern contraceptive methods at the time of our survey, compared with 25.4% who were using these modern methods. This low proportion of 25.4% of women of childbearing age 15-49 using family planning in our study area is lower than the 27.6% recorded in the Mumbunda health zone in Lubumbashi
| [22] | Matungulu CM, Kandolo SI, Mukengeshayi AN, Nkola AM, Mpoyi DI, Mumba SK, Kabamba JN, Cowgill K, Kaj FM. Determinants of contraceptive use in the Mumbunda health zone in Lubumbashi, Democratic Republic of Congo. Pan Afr Med J. 2015; 22: 329. |
[22]
, significantly higher than the 20% recorded for the whole of North Kivu province
, higher than the 18.4% observed in the Dibindi Dibindi health zone in Mbuji-Mayi
| [23] | Ntambue AM, Tshiala RN, Malonga FK, Ilunga TM, Kamonayi JM, Kazadi ST, Matungulu CM, Musau AN, Mulamba D, Dramaix-Wilmet M, Donnen P. Use of modern contraceptive methods in the Democratic Republic of Congo: prevalence and barriers in the Dibindi health zone in Mbuji-Mayi. Pan Afr Med J. 2017; 26: 199. |
[23]
. This is significantly higher than the national average, estimated at 10.7% in 2024
, and much lower than the 61.9% reported among female healthcare providers in Guinea-Conakry
| [14] | Youla Y, Sidibé S, Kourouma M, Camara S, Bangoura S, Olivier K, Grovogui M, Diaby M, Bongono E, Diallo O, Conté I, Traoré S, Djigui Keita A, Touré A and Delamou A. Prevalence and factors associated with the use of modern contraceptive methods among female healthcare providers in health facilities in Guinea. Front. Glob. Women’s Health. 2025; 1(6): 1-8.
https://doi.org/10.3389/fgwh |
[14]
.
The observed discrepancies in the adoption of contemporary contraceptive methods can be attributed to a multitude of factors. Firstly, these disparities could be attributable to differences in the socio-demographic profile of the participants included in the study. Secondly, the availability of family planning services in the study environment could play a determining role. The context of the study, whether rural or urban, and the location of the study, whether in a community or a health facility, could influence the results. The period of the study, whether prospective or retrospective, could also be a determining factor.
There exists a multitude of reasons why individuals do not utilize family planning services. These factors generally encompass barriers associated with the services themselves, such as cost, accessibility, and quality; individual concerns, including side effects and misinformation; and social and cultural factors, such as partner opposition, religious norms, and gender stereotypes. These factors underpin the prevalence of unmet need, defined as instances wherein women find themselves unable to access contraception despite their personal desire to avoid conception.
As demonstrated in the following diagram, the investigation revealed the primary factors contributing to the underutilization of family planning services. Most participants (198/350, 56.6%) expressed a desire to conceive, while 38.3% of them (138/350) encountered challenges in accessing family planning services. 17.4% of participants (61/350) reported a fear of potential side effects, including menstrual problems, being overweight, or secondary infertility. Finally, cultural barriers, including stigma and misperceptions, accounted for 13.7% of the reasons provided (48/350).
Similar results have been reported in Guinea-Conakry
| [14] | Youla Y, Sidibé S, Kourouma M, Camara S, Bangoura S, Olivier K, Grovogui M, Diaby M, Bongono E, Diallo O, Conté I, Traoré S, Djigui Keita A, Touré A and Delamou A. Prevalence and factors associated with the use of modern contraceptive methods among female healthcare providers in health facilities in Guinea. Front. Glob. Women’s Health. 2025; 1(6): 1-8.
https://doi.org/10.3389/fgwh |
[14]
. It is also known that modern contraceptive methods are the ideal solution for avoiding unwanted pregnancies, improving reproductive and sexual health, and significantly reducing the risk of maternal illness. These modern methods are the key to more serene and safer pregnancy planning, and are proof that medical advances can improve maternal, child and family well-being. There is no doubt that some methods offer benefits that go well beyond contraception, regulating menstruation and protecting couples against sexually transmitted infections (STIs).
The third table of this study presents the results of an assessment of participants' knowledge regarding contraceptive methods. The results indicate that the primary advantage of modern contraceptive methods, as reported by participants, is the prevention of unwanted pregnancies (53.4%) and sexually transmitted infections (19.1%). The most utilized contraceptive methods among the study participants were condoms and pills, with 56.3% and 30.3% of the participants, respectively, reporting their use. Most participants (53.3%) expressed the opinion that contemporary contraceptive methods can be utilized for a period of three years or more. A considerable proportion of the respondents (30.6%) reported a lack of awareness regarding reliable sources of information concerning modern contraceptive methods. The present observations align with those of Matondo G et al., who determined that condoms, implants, and pills were the most widely known modern contraceptive methods in their study in Matadi, in the province of Congo-Centrale
| [14] | Youla Y, Sidibé S, Kourouma M, Camara S, Bangoura S, Olivier K, Grovogui M, Diaby M, Bongono E, Diallo O, Conté I, Traoré S, Djigui Keita A, Touré A and Delamou A. Prevalence and factors associated with the use of modern contraceptive methods among female healthcare providers in health facilities in Guinea. Front. Glob. Women’s Health. 2025; 1(6): 1-8.
https://doi.org/10.3389/fgwh |
[14]
.
In the context of our study, which is taking place in a region of the Democratic Republic of Congo where there has been a great deal of sexual violence and violence against women for more than thirty years of war
| [25] | Nyakio O, Mukwege D, Balagizi F, Oduoye MO, Banga S, Onesime J, Bhattacharjee P, Elembwe H, Cakwira H, Kihanduka E, Amiri A, Rugendabanga E, Hangi S, Makungu C, Akilimali A. A call for action to stop sexual violence against women in the Democratic Republic of Congo: A brief report. Int J Gynaecol Obstet. 2025 Jan; 168(1): 397-399.
https://doi.org/10.1002/ijgo.15801 |
[25]
, the level of knowledge of the women participating in this study about the advantages of using modern contraceptive methods is unsatisfactory. The persistent armed conflict has destroyed basic health infrastructures, the socio-economic fabric, skilled human resources and drug supply channels. All these factors combined make women in this part of the country vulnerable, exposing them to unwanted pregnancies and sexually transmitted diseases. Consequently, this study revealed a major challenge in informing and raising awareness among women about the advantages of using modern contraceptive methods, and above all in sharing information about the availability of family planning services in the Karisimbi health zone, in the town of Goma, in the east of the Democratic Republic of Congo.
A detailed analysis of
Table 4 reveals that the significant socio-demographic factors associated with low use of family planning services using modern contraceptive methods are single marital status (x2 = 236.108), the young age of the participant in the study (x2 = 155.83), the participant's low level of education (x2 = 69.90), and low maternity at the time of the study of no more than 2 children (x2 = 161.69). Analytical table N V, on the analysis of socio-cultural and religious factors, shows that the unfavorable opinion of the spouse does not influence adherence to contraceptive methods (x2 = 14.365), compared with the desire to conceive (x2 = 14.365), which favor’s low recourse to family planning services using modern methods. Religious prohibitions (x2 = 13.701) and difficult access to family planning services (x2 = 50.118). However, the absence of cultural barriers and fear of adverse effects are beneficial protective factors for the use of contraceptives. The respective chi-squares calculated were 2.981 for the first factor and 2.401 for the second.
These results corroborate those of Acotchéou P
et al in Benin, who observed in their comparable study that older women are more likely to use modern contraceptives than younger women aged 15-22. This probability is also high when women do not discuss the subject with their partner. Women's use of modern contraceptives is 4.9 times positively influenced by household size. The same was true for women who had already given birth, compared with those who had never given birth (OR: 2.313). On the other hand, for these authors, wanting fewer children makes her more likely to use these contraceptives than when she wants more (OR: 1.244)
| [26] | Acotchéou P, Affo M, Dansou J, Delvaux T et Saizonou ZJ. Modern contraceptive use among adolescents in Benin: trends, determinants and prospects. Sex Reprod Health Matters. 2023; 31(5): 2267200.
https://doi.org/10.1080/26410397.2023.2267200 |
[26]
. At Dibindi Dibindi health zone in Mbuji-Mayi, the availability of family planning services and related information does not guarantee the use of modern contraceptive methods. The reasons for this include the desire to have children, religious prohibitions, the opposition of the partner, and fear of potential side effects
| [23] | Ntambue AM, Tshiala RN, Malonga FK, Ilunga TM, Kamonayi JM, Kazadi ST, Matungulu CM, Musau AN, Mulamba D, Dramaix-Wilmet M, Donnen P. Use of modern contraceptive methods in the Democratic Republic of Congo: prevalence and barriers in the Dibindi health zone in Mbuji-Mayi. Pan Afr Med J. 2017; 26: 199. |
[23]
. In Kongo Centrale, the level of education does not appear to influence the selection of modern contraceptive methods. The utilization of family planning services is influenced by several factors, including the number of pregnancies that are carried to term, the number of living children, the number of children who have died, and the advanced maternal age of the patient
| [24] | Matondo G, Mahoya L, Kiangebeni J, Nkodila A, Kintaudi N, Minuku F, Ntumba Aet Ngwala P. Determinants of low use of modern contraceptive methods among women of childbearing age: the case of the Gombe Matadi Health Zone. Open Journal of Obstetrics and Gynecology. 2021; 11(5): 9. |
[24]
.
As in most developing countries, unmarried, sexually active teenage girls with no official partner have difficulty accessing contraception. Those who use these contraceptive methods are often frowned upon by their communities, who associate the practice with prostitution. In addition, this category of the population is the victim of stigmatization and social condemnation. This socio-cultural barrier exposes girls to unwanted pregnancies, abortions and high maternal morbidity.
5. Conclusion
Adherence to modern family planning methods remains low in our study setting. Several reducible factors contribute to this low proportion of adherence among women of childbearing age, including single women, the young age of the study participants, the low level of education of the participants and low fertility at the time of the study (maximum of two children), desire to conceive, religious prohibitions and difficult access to family planning services.
6. Recommendations
To improve adherence to family planning (FP) within our community, we must adopt a multidimensional approach that considers access, education, religious and social norms. The strategic vision must strengthen the promotion of maternal and child health through community promotors and various healthcare providers, breaking down cultural and religious barriers.
Abbreviations
BMI | Body Mass Index. |
DRC | Democratic Republic of Congo |
i.e | Id Est/ That Is |
TV | Television |
Author Contributions
Bahati Desire: Conceptualization, Data curation, Investigation
Maombi Gashegu Felicien: Conceptualization, Data curation, Investigation
Mutubuki Herbert: Methodology, Formal analysis, Writing – review & editing
Bitwe Mihanda Richard: Methodology, Formal analysis, Writing – review & editing
Mashako Ruhanga Many: Data validation, Writing – review & editing, Writing – original draft
Mashako Katonda Yves: Data validation, Writing – review & editing, Writing – original draft
Kanyange Kanyamihigo Sylvie: Conceptualization, Data curation, Investigation
Kajibwami Esperance: Conceptualization, Data curation, Investigation
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
WHO, Family planning/contraception Methods Available on:
https://www.who.int/fr/news-room/fact-sheets/detail/family-planning-contraception
October 30th, 2025. 1: 35 PM.
|
| [2] |
Sossoukpè N, Koufèdé R, Dénakpo N and Adjoavi M. Epidemiological characteristics of maternal deaths in the department of Couffo, Benin, January 2018-June 2022. Journal of Interventional Epidemiology and Public Health. 2025; 8(1): 6.
https://doi.org/10.37432/jieph.supp.2025.8.2.12
|
| [3] |
Ndayisenga JP, Oudshoorn A, Babenko-Mould Y, Jackson KT, Hynie M, Mukamana D, Uwajeneza P, Musabirema P. A narrative review of the literature on unintended adolescent pregnancies: Understanding their meaning, associated factors, and consequences. Afr J Reprod Health. 2025; 29(8): 154-172.
https://doi.org/10.29063/ajrh2025/v29i8.15
|
| [4] |
Elomrani S, Utz B, De Brouwere V, Kajjoune I, Assarag B. Abortion in Morocco and a turn to tragedy: women and healthcare professionals speak out! A cross-sectional mixed-methods study in AgadirSex Reprod Health Matters. 2023; 31(5): 2279371.
https://doi.org/10.1080/26410397.2023.2279371
|
| [5] |
Apanga P, Kumbeni M, Ayamga E, Ulanja M and Akparibo R. Prevalence and factors associated with modern contraceptive use among women of reproductive age in 20 African countries: a large population-based study. BMJ Open. 2020; 10: e041103.
https://doi.org/10.1136/bmjopen-2020-041103
|
| [6] |
Admasu K, Tamir T, Alemu M, Zeleke G and Zegeye A. Prevalence and determinants of exposure to family planning messages among reproductive age women in five Sub-Saharan African countries: a multilevel analysis of 2021-2023 demographic and health surveys. BMC Womens Health. 2025; 25(1): 365.
https://doi.org/10.1186/s12905-025-03895-w
|
| [7] |
Dwomoh D, Amuasi S, Amoah E, Ama S, Gborgbortsi W and Tetteh J. Exposure to family planning messages and contraceptive use among women of reproductive age in sub-Saharan Africa: a cross-sectional program impact evaluation study. Sci Rep. 2022; 12: 18941.
https://doi.org/10.1038/s41598-022-22525-1
|
| [8] |
Dramé L, Kolié D, Sidibé S, Yombouno J et Delamou A. The factors associated with contraceptive use among young female students in rural Guinea. Public Health 2023; 6(35): 129 à 140.
https://doi.org/10.3917/spub.236.0129
|
| [9] |
Sifora KK, De Wet-Billings N, Frade-Bekker S, Phiri M. Individual and community level factors influencing modern contraceptive use among women of reproductive age in South Africa: a multilevel analysis. Contracept Reprod Med. 2025; 10(1): 53.
https://doi.org/10.1186/s40834-025-00392-1
|
| [10] |
Michael T, Ojo T, Ijabadeniyi O, Ibikunle M, Oni J and Agboola A. Prevalence and factors associated with contraceptive use among sexually active adolescent girls in 25 sub-Saharan African countries. PLoS One. 2024; 19(2): e0297411.
https://doi.org/10.1371/journal.pone.0297411
|
| [11] |
Singata-Madliki M, Carayon-Lefebvre d'Hellencourt F, Lawrie TA, Balakrishna Y and Hofmeyr GJ. Effects of three contraceptive methods on depression and sexual function: An ancillary study of the ECHO randomized trial. Int J Gynaecol Obstet. 2021; 154(2): 256-262.
https://doi.org/10.1002/ijgo.13594
|
| [12] |
Musuka G, Murewanhema G, Mukandavire Z, Chingombe I, Cuadros D, Mutenherwa F, Dzinamarira T, Eghtessadi R, Malunguza N and Mapingure M. HIV status and contraceptive use in Zimbabwe among sexually active adolescent girls and women: Secondary analysis of Zimbabwe Demographic Health survey data. S Afr Med J. 2024; 114(6b): e1407.
https://doi.org/10.11604/pamj.2022.41.262.32615
|
| [13] |
Mankelkl G and Kinfe B. Pooled prevalence of modern contraceptive utilization and its associated factors among reproductive age women in East Africa: derived from demographic and health surveys. J Health Popul Nutr. 2025; 44: 261.
https://doi.org/10.1186/s41043-025-01019-6
|
| [14] |
Youla Y, Sidibé S, Kourouma M, Camara S, Bangoura S, Olivier K, Grovogui M, Diaby M, Bongono E, Diallo O, Conté I, Traoré S, Djigui Keita A, Touré A and Delamou A. Prevalence and factors associated with the use of modern contraceptive methods among female healthcare providers in health facilities in Guinea. Front. Glob. Women’s Health. 2025; 1(6): 1-8.
https://doi.org/10.3389/fgwh
|
| [15] |
Kanthé D, Samaké Y, Koné O, Fomba D, Bagayoko TB, Kéita M, Samaké B, Kéita S, Traoré M, Dembélé BT, Togo AP. Determinants of Low Modern Contraceptive Prevalence in the Markala Health District: Case of the Diamarabougou Community Health Center Mali. Health Sciences and Disease. 2023; 24(7): 121-132.
https://doi.org/10.5281/hsd.v24i7.4613
|
| [16] |
Kwete D, Binanga A, Mukaba T, Nemuandjare T, Mbadu M, Kyungu M, Sutton P, Bertrand JT. Family Planning in the Democratic Republic of the Congo: Encouraging Momentum, Formidable Challenges. Glob Health Sci Pract. 2018 Mar 30; 6(1): 40-54.
https://doi.org.10.9745/GHSP-D-17-00346.
|
| [17] |
National Institute of Statistics (INS) and School of Public Health (ESP) of Kinshasa. The third Demographic and Health Survey (DHS) of the Democratic Republic of Congo in 2023–24 (DHS-DRC III 2023–24) Kinshasa, 2025. Available on:
https://drc.unfpa.org/fr/publications/enqu%C3%AAte-d%C3%A9mographique-et-de-sant%C3%A9-iii-eds-rdc-iii-2023%E2%80%932024
November 9th, 2025, at 11: 37 AM.
|
| [18] |
Koto-Te-Nyiwa Ngbolua J.-P, Mukandu B, Wembodinga U, Ngbolua K and Mbungu M. Perceptions and obstacles to the use of modern contraceptive methods among multiparous women in Kisangani, Democratic Republic of Congo. Revue Africaine des Sciences Sociales. 2025; 7(1), 313-328.
https://doi.org/10.4314/orapj.v6i2.18
|
| [19] |
Bapolisi W, Bisimwa G, Merten S. Barriers to family planning use in the Eastern Democratic Republic of Congo: an application of the theory of planned behaviors using a longitudinal survey. BMJ Open. 2023; 13(2): e061564.
https://doi.org/10.1136/bmjopen-2022-061564
|
| [20] |
Ouédraogo S, Ouattara A, Sarigda M, Ouédraogo L and Ouédraogo C. Prevalence and factors associated with the use of modern contraceptive methods in the health district of Djibo, Sahel region in Burkina Faso. J Interval Epidemiol Public Health. 2023; 6(2): 3.
https://www.doi.org/10.37432/jieph.2023.6.2.80
|
| [21] |
Masoda MN, Buloze JM, Kabwe AM, Mishika PL, Bondekwe JCA, Mukuku O, Mpoy CW, Ngwala PL, Wembonyama SO, Tsongo ZK. Determinants of family planning use among married men in Idjwi, Democratic Republic of Congo. Journal of Medicine, Public Health and Policy Research. 2022; 2(1): 1-9.
|
| [22] |
Matungulu CM, Kandolo SI, Mukengeshayi AN, Nkola AM, Mpoyi DI, Mumba SK, Kabamba JN, Cowgill K, Kaj FM. Determinants of contraceptive use in the Mumbunda health zone in Lubumbashi, Democratic Republic of Congo. Pan Afr Med J. 2015; 22: 329.
|
| [23] |
Ntambue AM, Tshiala RN, Malonga FK, Ilunga TM, Kamonayi JM, Kazadi ST, Matungulu CM, Musau AN, Mulamba D, Dramaix-Wilmet M, Donnen P. Use of modern contraceptive methods in the Democratic Republic of Congo: prevalence and barriers in the Dibindi health zone in Mbuji-Mayi. Pan Afr Med J. 2017; 26: 199.
|
| [24] |
Matondo G, Mahoya L, Kiangebeni J, Nkodila A, Kintaudi N, Minuku F, Ntumba Aet Ngwala P. Determinants of low use of modern contraceptive methods among women of childbearing age: the case of the Gombe Matadi Health Zone. Open Journal of Obstetrics and Gynecology. 2021; 11(5): 9.
|
| [25] |
Nyakio O, Mukwege D, Balagizi F, Oduoye MO, Banga S, Onesime J, Bhattacharjee P, Elembwe H, Cakwira H, Kihanduka E, Amiri A, Rugendabanga E, Hangi S, Makungu C, Akilimali A. A call for action to stop sexual violence against women in the Democratic Republic of Congo: A brief report. Int J Gynaecol Obstet. 2025 Jan; 168(1): 397-399.
https://doi.org/10.1002/ijgo.15801
|
| [26] |
Acotchéou P, Affo M, Dansou J, Delvaux T et Saizonou ZJ. Modern contraceptive use among adolescents in Benin: trends, determinants and prospects. Sex Reprod Health Matters. 2023; 31(5): 2267200.
https://doi.org/10.1080/26410397.2023.2267200
|
Cite This Article
-
APA Style
Desire, B., Felicien, M. G., Herbert, M., Richard, B. M., Many, M. R., et al. (2026). Contributor Factors Associate to Underutilization of Family Planning Services in Karisimbi Health Zone, Goma City’s, Democratic Republic of Congo. Central African Journal of Public Health, 12(1), 34-45. https://doi.org/10.11648/j.cajph.20261201.14
 Copy
|
Copy
|
 Download
Download
ACS Style
Desire, B.; Felicien, M. G.; Herbert, M.; Richard, B. M.; Many, M. R., et al. Contributor Factors Associate to Underutilization of Family Planning Services in Karisimbi Health Zone, Goma City’s, Democratic Republic of Congo. Cent. Afr. J. Public Health 2026, 12(1), 34-45. doi: 10.11648/j.cajph.20261201.14
Copy
|
Download
AMA Style
Desire B, Felicien MG, Herbert M, Richard BM, Many MR, et al. Contributor Factors Associate to Underutilization of Family Planning Services in Karisimbi Health Zone, Goma City’s, Democratic Republic of Congo. Cent Afr J Public Health. 2026;12(1):34-45. doi: 10.11648/j.cajph.20261201.14
Copy
|
Download
-
@article{10.11648/j.cajph.20261201.14,
author = {Bahati Desire and Maombi Gashegu Felicien and Mutubuki Herbert and Bitwe Mihanda Richard and Mashako Ruhanga Many and Mashako Katonda Yves and Kanyange Kanyamihigo Sylvie and Kajibwami Esperance},
title = {Contributor Factors Associate to Underutilization of Family Planning Services in Karisimbi Health Zone, Goma City’s, Democratic Republic of Congo},
journal = {Central African Journal of Public Health},
volume = {12},
number = {1},
pages = {34-45},
doi = {10.11648/j.cajph.20261201.14},
url = {https://doi.org/10.11648/j.cajph.20261201.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cajph.20261201.14},
abstract = {Introduction: Despite the progress made, access to sexual and reproductive health (SRH) in sub-Saharan Africa (SSA) in general, and in the DRC in particular, faces major obstacles, resulting in high rates of maternal mortality, unwanted pregnancies, and sexually transmitted infections (STIs). The challenges currently being faced include the unavailability of reproductive health services, geographical inaccessibility, cultural and religious norms, stigmatization, and low levels of maternal education. Methodology: This observational cross-sectional study focuses on the knowledge, attitudes and practices of women of childbearing age (15 to 49 years) regarding family planning in the Mugunga health area, located in the Karisimbi health zone, city of Goma, in the east of the Democratic Republic of Congo (DRC). This research covers a short period of six months from 1 October 2024 to 31 March 2025. Data collection, entry and recording were carried out using the Open Data Kit Collect (KoBoToolbox) software, while the analysis was carried out on the statistics product and service solution (SPSS) software version 27.0. The Pearson Chi-Square (X2) statistical test was applied in this research. Results: Significant socio-demographic factors associated with low use of family planning services using modern contraceptive methods are single marital status (x² = 236.108), young age of study participants (x² = 155.83), low level of education of participants (x2 = 69.90), and low number of children at the time of the study (maximum of 2 children) (x2 = 161.69). Conclusion: adherence to modern family planning methods remains low in our study setting. Several socio-demographic, cultural and religious factors contribute to this low proportion. Promoting maternal and child health through community health workers would help improve adherence to modern family planning (FP).},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Contributor Factors Associate to Underutilization of Family Planning Services in Karisimbi Health Zone, Goma City’s, Democratic Republic of Congo
AU - Bahati Desire
AU - Maombi Gashegu Felicien
AU - Mutubuki Herbert
AU - Bitwe Mihanda Richard
AU - Mashako Ruhanga Many
AU - Mashako Katonda Yves
AU - Kanyange Kanyamihigo Sylvie
AU - Kajibwami Esperance
Y1 - 2026/02/24
PY - 2026
N1 - https://doi.org/10.11648/j.cajph.20261201.14
DO - 10.11648/j.cajph.20261201.14
T2 - Central African Journal of Public Health
JF - Central African Journal of Public Health
JO - Central African Journal of Public Health
SP - 34
EP - 45
PB - Science Publishing Group
SN - 2575-5781
UR - https://doi.org/10.11648/j.cajph.20261201.14
AB - Introduction: Despite the progress made, access to sexual and reproductive health (SRH) in sub-Saharan Africa (SSA) in general, and in the DRC in particular, faces major obstacles, resulting in high rates of maternal mortality, unwanted pregnancies, and sexually transmitted infections (STIs). The challenges currently being faced include the unavailability of reproductive health services, geographical inaccessibility, cultural and religious norms, stigmatization, and low levels of maternal education. Methodology: This observational cross-sectional study focuses on the knowledge, attitudes and practices of women of childbearing age (15 to 49 years) regarding family planning in the Mugunga health area, located in the Karisimbi health zone, city of Goma, in the east of the Democratic Republic of Congo (DRC). This research covers a short period of six months from 1 October 2024 to 31 March 2025. Data collection, entry and recording were carried out using the Open Data Kit Collect (KoBoToolbox) software, while the analysis was carried out on the statistics product and service solution (SPSS) software version 27.0. The Pearson Chi-Square (X2) statistical test was applied in this research. Results: Significant socio-demographic factors associated with low use of family planning services using modern contraceptive methods are single marital status (x² = 236.108), young age of study participants (x² = 155.83), low level of education of participants (x2 = 69.90), and low number of children at the time of the study (maximum of 2 children) (x2 = 161.69). Conclusion: adherence to modern family planning methods remains low in our study setting. Several socio-demographic, cultural and religious factors contribute to this low proportion. Promoting maternal and child health through community health workers would help improve adherence to modern family planning (FP).
VL - 12
IS - 1
ER -
Copy
|
Download