Introduction: Gallbladder volvulus (GBV) is a rare but critical condition characterized by torsion of the gallbladder on its mesentery. Prompt surgical intervention is crucial in preventing complications and improving patient outcomes. Despite advancements in imaging techniques, diagnosing GBV remains challenging due to its nonspecific clinical presentation and low preoperative detection rates. Case Details: This paper presents the case of a 79-year-old female presenting with symptoms suggestive of acute appendicitis and urinary tract infection. Imaging, including Computed Tomography (CT), ultrasound, (US) and magnetic resonance cholangiopancreatography (MRCP), were indicative of acute acalculous cholecystitis. Intraoperatively, a necrotic gangrenous gallbladder was encountered, resulting from GBV. Discussion: GBV poses diagnostic difficulties due to its variable presentation and low preoperative detection rates. Misdiagnoses poses significant risk of mismanagement, especially in the elderly and high risk populations, where non-operative management is attempted (antibiotics, percutaneous cholecystostomy, etc.) leading to increased morbidity and mortality. Therefore, high index of suspicion and correlation with imaging findings are crucial for accurate diagnosis. While various imaging modalities can assist in diagnosis, interpretation may be challenging, as demonstrated in this case. Surgical intervention, preferably through laparoscopy, is the cornerstone of treatment and offers favorable outcomes when performed promptly. Conclusion: In conclusion, GBV is a rare but potentially life-threatening condition that necessitates early recognition and surgical intervention. Despite challenges in diagnosis, a comprehensive clinical and radiological approach is crucial for timely management and optimal patient outcomes. Further research and awareness are warranted to enhance early diagnosis of this uncommon entity.
| Published in | Advances in Surgical Sciences (Volume 12, Issue 1) |
| DOI | 10.11648/j.ass.20241201.16 |
| Page(s) | 36-42 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Gallbladder Volvulus, Gallbladder Torsion, Floating Gallbladder, Acute Abdomen, Acute Appendicitis, Urinary Tract Infection (UTI)
GBV | Gallbladder Volvulus |
CT | Computed Tomography |
MRCP | Magnetic Resonance Cholangiopancreatography |
BMI | Body Mass Index |
MR | Mitral Regurgitation |
UTI | Urinary Tract Infection |
ED | Emergency Department |
OSH | Outside Hospital |
CBD | Common Bile Duct |
RVEF | Right Ventricular Ejection Fraction |
HIDA | Hepatobiliary Iminodiacetic Acid |
MRI | Magnetic Resonance Imaging |
AAC | Acute Acalculous Cholecystitis |
ACC | Acute Calculous Cholecystitis |
LC | Laparoscopic Cholecystectomy |
PCT | Percutaneous Cholecystostomy Tube |
| [1] | Keeratibharat, N., & Chansangrat, J. (2022). Gallbladder volvulus: A Review. Cureus. |
| [2] | Reilly, D. J., Kalogeropoulos, G., & Thiruchelvam, D. (2012). Torsion of the gallbladder: A systematic review. HPB, 14(10), 669–672. |
| [3] | Pottorf, B. J., Alfaro, L., & Hollis, H. W. (2013). A clinician’s guide to the diagnosis and management of gallbladder volvulus. The Permanente Journal, 17(2), 80–83. |
| [4] | Mouawad, N. J., Crofts, B., Streu, R., Desrochers, R., & Kimball, B. C. (2011). Acute gallbladder torsion - a continued pre-operative diagnostic dilemma. World Journal of Emergency Surgery, 6(1), 13. |
| [5] | Lau, W. Y., Fan, S. T., &Wong, S. H. (1982). Acute torsion of the gall bladder in the aged: A re-emphasis on clinical diagnosis. ANZ Journal of Surgery, 52(5), 492–494. |
| [6] | Shah, N., Ballecer, E., Hanna, I., Levin, G., &Khalife, M. E. (2021). Gallbladder volvulus presenting as acute appendicitis. Cureus. |
| [7] | Bauman, Z., Ruggero, J., & Lim, J. (2015). Gallbladder volvulus presenting as acute appendicitis. Case Reports in Surgery, 2015, 1–4. |
| [8] | Vedanayagam, M. S., Nikolopoulos, I., Janakan, G., & El-Gaddal, A. (2013). Gallbladder volvulus: A case of mimicry. Case Reports, 2013 (jan16 1). |
| [9] | Rueda-Martínez, J. L., Cascales-Sánchez, P., Vázquez-Aragón, P., Serafín Valero-Liñán, A., & Prat-Calero, A. (2011). Gallbladder volvulus: Clinical presentation mimicking acute appendicitis of the elderly. Revista Española de Enfermedades Digestivas, 103(12), 656–657. |
| [10] | Nakao, A., Matsuda, T., Funabiki, S., Mori, T., Koguchi, K., Iwado, T., Matsuda, K., Takakura, N., Isozaki, H., & Tanaka, N. (1999). Gallbladder torsion: Case report and review of 245 cases reported in the Japanese literature. Journal of Hepato-Biliary-Pancreatic Surgery, 6(4), 418–421. |
| [11] | Baig, Z., Ljubojevic, V., & Christian, F. (2021). The diagnostic dilemma of a gallbladder volvulus: An unusual case report and review of the literature. International Journal of Surgery Case Reports, 80, 105614. |
| [12] | Miyata, T., San-nomiya, Y., Nagayama, T., Kin, R., Nishiki, H., Hashimoto, A., Fujii, Y., Miura, S., Kaida, D., Tomita, Y., Nakamura, N., Miyashita, T., Fujita, H., Ueda, N., & Takamura, H. (2022). Preoperative diagnosis of gallbladder torsion by magnetic resonance cholangiopancreatography: A case report. Clinical Case Reports, 10(2). |
| [13] | Kalyanasundaram, S., & Fernando, S. (2022). Atypical presentation of cholecystitis with torsion of the gallbladder diagnosed preoperatively in an unusual location. BJR|case Reports, 8(1). |
| [14] | Layton, B., Rudralingam, V., & Lamb, R. (2016). Gallbladder volvulus: It’s a small whirl. BJR|case Reports, 2(3), 20150360. |
| [15] | Sato, O., Kotani, T., Kanayama, T., Tokuda, B., & Yamada, K. (2023). Utility of hyperdense whirl sign for the diagnosis of gallbladder torsion. Acta Radiologica Open, 12(11). |
| [16] | Dasyam, A. K., Koo, J., Stahlfeld Miller, M., Sell, H. W., & Tublin, M. E. (2015). The cystic duct knot sign: Case report with description of a new ultrasound sign of gallbladder torsion. Emergency Radiology, 22(4), 445–447. |
| [17] | Matsuhashi, N. (2006). Volvulus of the gall bladder diagnosed by ultrasonography, computed tomography, coronal magnetic resonance imaging and Magnetic Resonance Cholangio-Pancreatography. World Journal of Gastroenterology, 12(28), 4599. |
| [18] | Laydi, M., Charpentier, K., Paquette, B., & Heyd, B. (2017). Combined treatment of a gallbladder volvulus with a common bile duct obstruction. Case Reports in Surgery, 2017, 1–2. |
| [19] | Aroori, S., Mangan, C., Reza, L., & Gafoor, N. (2018). Percutaneous cholecystostomy for severe acute cholecystitis: A useful procedure in high-risk patients for surgery. Scandinavian Journal of Surgery, 108(2), 124–129. |
| [20] | Kirkegård, J., Horn, T., Christensen, S. D., Larsen, L. P., Knudsen, A. R., & Mortensen, F. V. (2015). Percutaneous cholecystostomy is an effective definitive treatment option for acute acalculous cholecystitis. Scandinavian Journal of Surgery, 104(4), 238–243. |
| [21] | Horn, Torben., Christensen, S. D., Kirkegård, Jakob., Larsen, L. P., Knudsen, A. R., & Mortensen, F. V. (2015). Percutaneous cholecystostomy is an effective treatment option for acute calculous cholecystitis: A 10-Year experience. HPB, 17(4), 326–331. |
| [22] | Walter, K. (2022). Acute cholecystitis. JAMA, 327(15), 1514. |
| [23] | Cao, A. M., Eslick, G. D., & Cox, M. R. (2015). Early laparoscopic cholecystectomy is superior to delayed acute cholecystitis: A meta-analysis of case–control studies. Surgical Endoscopy, 30(3), 1172–1182. |
| [24] | Morales-Maza, J., Rodríguez-Quintero, J. H., Santes, O., Hernández-Villegas, A. C., Clemente-Gutiérrez, U., Sánchez-Morales, G. E., Mier y Terán-Ellis, S., Pantoja, J. P., & Mercado, M. A. (2019). Percutaneous cholecystostomy as treatment for acute cholecystitis: What has happened over the last five years? A literature review. Revista de Gastroenterología de México (English Edition), 84(4), 482–491. |
APA Style
Mittal, K., Panthi, S., Donahue, T., Kevorkian, N. (2024). Gallbladder Volvulus: A Rare Case of Pre-operative Diagnostic Quandary. Advances in Surgical Sciences, 12(1), 36-42. https://doi.org/10.11648/j.ass.20241201.16
ACS Style
Mittal, K.; Panthi, S.; Donahue, T.; Kevorkian, N. Gallbladder Volvulus: A Rare Case of Pre-operative Diagnostic Quandary. Adv. Surg. Sci. 2024, 12(1), 36-42. doi: 10.11648/j.ass.20241201.16
AMA Style
Mittal K, Panthi S, Donahue T, Kevorkian N. Gallbladder Volvulus: A Rare Case of Pre-operative Diagnostic Quandary. Adv Surg Sci. 2024;12(1):36-42. doi: 10.11648/j.ass.20241201.16
@article{10.11648/j.ass.20241201.16,
author = {Kriti Mittal and Sagar Panthi and Terrence Donahue and Noubar Kevorkian},
title = {Gallbladder Volvulus: A Rare Case of Pre-operative Diagnostic Quandary
},
journal = {Advances in Surgical Sciences},
volume = {12},
number = {1},
pages = {36-42},
doi = {10.11648/j.ass.20241201.16},
url = {https://doi.org/10.11648/j.ass.20241201.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ass.20241201.16},
abstract = {Introduction: Gallbladder volvulus (GBV) is a rare but critical condition characterized by torsion of the gallbladder on its mesentery. Prompt surgical intervention is crucial in preventing complications and improving patient outcomes. Despite advancements in imaging techniques, diagnosing GBV remains challenging due to its nonspecific clinical presentation and low preoperative detection rates. Case Details: This paper presents the case of a 79-year-old female presenting with symptoms suggestive of acute appendicitis and urinary tract infection. Imaging, including Computed Tomography (CT), ultrasound, (US) and magnetic resonance cholangiopancreatography (MRCP), were indicative of acute acalculous cholecystitis. Intraoperatively, a necrotic gangrenous gallbladder was encountered, resulting from GBV. Discussion: GBV poses diagnostic difficulties due to its variable presentation and low preoperative detection rates. Misdiagnoses poses significant risk of mismanagement, especially in the elderly and high risk populations, where non-operative management is attempted (antibiotics, percutaneous cholecystostomy, etc.) leading to increased morbidity and mortality. Therefore, high index of suspicion and correlation with imaging findings are crucial for accurate diagnosis. While various imaging modalities can assist in diagnosis, interpretation may be challenging, as demonstrated in this case. Surgical intervention, preferably through laparoscopy, is the cornerstone of treatment and offers favorable outcomes when performed promptly. Conclusion: In conclusion, GBV is a rare but potentially life-threatening condition that necessitates early recognition and surgical intervention. Despite challenges in diagnosis, a comprehensive clinical and radiological approach is crucial for timely management and optimal patient outcomes. Further research and awareness are warranted to enhance early diagnosis of this uncommon entity.
},
year = {2024}
}
TY - JOUR T1 - Gallbladder Volvulus: A Rare Case of Pre-operative Diagnostic Quandary AU - Kriti Mittal AU - Sagar Panthi AU - Terrence Donahue AU - Noubar Kevorkian Y1 - 2024/06/19 PY - 2024 N1 - https://doi.org/10.11648/j.ass.20241201.16 DO - 10.11648/j.ass.20241201.16 T2 - Advances in Surgical Sciences JF - Advances in Surgical Sciences JO - Advances in Surgical Sciences SP - 36 EP - 42 PB - Science Publishing Group SN - 2376-6182 UR - https://doi.org/10.11648/j.ass.20241201.16 AB - Introduction: Gallbladder volvulus (GBV) is a rare but critical condition characterized by torsion of the gallbladder on its mesentery. Prompt surgical intervention is crucial in preventing complications and improving patient outcomes. Despite advancements in imaging techniques, diagnosing GBV remains challenging due to its nonspecific clinical presentation and low preoperative detection rates. Case Details: This paper presents the case of a 79-year-old female presenting with symptoms suggestive of acute appendicitis and urinary tract infection. Imaging, including Computed Tomography (CT), ultrasound, (US) and magnetic resonance cholangiopancreatography (MRCP), were indicative of acute acalculous cholecystitis. Intraoperatively, a necrotic gangrenous gallbladder was encountered, resulting from GBV. Discussion: GBV poses diagnostic difficulties due to its variable presentation and low preoperative detection rates. Misdiagnoses poses significant risk of mismanagement, especially in the elderly and high risk populations, where non-operative management is attempted (antibiotics, percutaneous cholecystostomy, etc.) leading to increased morbidity and mortality. Therefore, high index of suspicion and correlation with imaging findings are crucial for accurate diagnosis. While various imaging modalities can assist in diagnosis, interpretation may be challenging, as demonstrated in this case. Surgical intervention, preferably through laparoscopy, is the cornerstone of treatment and offers favorable outcomes when performed promptly. Conclusion: In conclusion, GBV is a rare but potentially life-threatening condition that necessitates early recognition and surgical intervention. Despite challenges in diagnosis, a comprehensive clinical and radiological approach is crucial for timely management and optimal patient outcomes. Further research and awareness are warranted to enhance early diagnosis of this uncommon entity. VL - 12 IS - 1 ER -
General Surgery, University of Connecticut Health, Hartford, USA
General Surgery, BP Koirala Institute of Health and Sciences, Dharan, Nepal
General Surgery, University of Connecticut Health, Hartford, USA
General Surgery, University of Connecticut Health, Hartford, USA

Figure 1. (CT Abdomen and Pelvis): Markedly distended gallbladder with wall thickening and pericholecystic inflammation. No definite gallstones. Mild to moderate intrahepatic biliary ductal dilation and enlargement of the common bile duct.
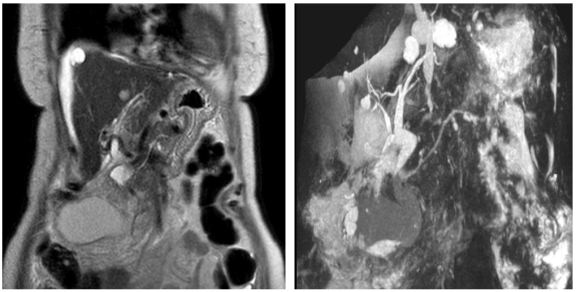
Figure 2. (MRCP): Mild free fluid adjacent to the liver and spleen consistent with ascites. Markedly distended and thick-walled gallbladder suggestive of acute cholecystitis. No definite intraluminal filling defects identified. The extrahepatic common bile duct does appear somewhat distended measuring a maximum of 11 mm. It tapers normally. No definite intrahepatic biliary dilatation. No intraluminal filling defects identified.
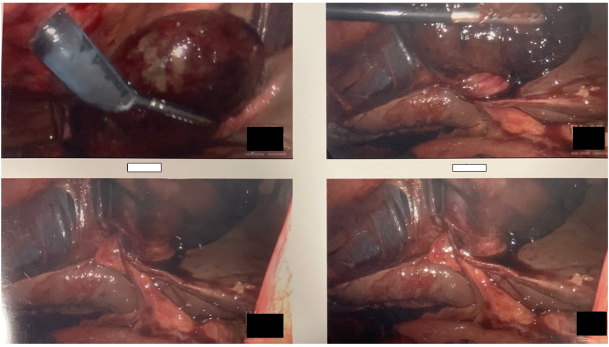
Figure 3. Gangrenous gallbladder pedunculated on its stalk and torsed 180 degrees.
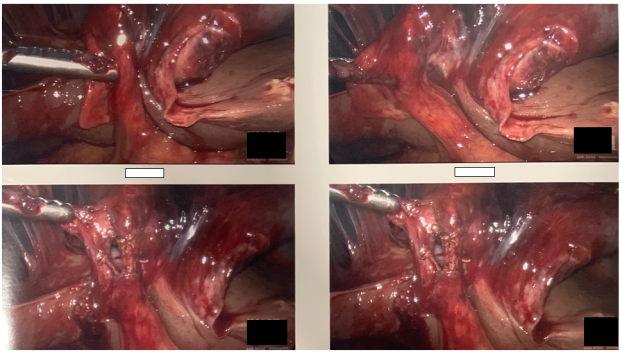
Figure 4. Necrotic gallbladder after detorsion.
Information

