Introduction: An inguinal hernia is a protrusion of abdominal cavity contents or pre-peritoneal fat through a hernial defect in the inguinal region. Desarda's technique is an aponeuroplasty, based on closure of the posterior wall of the inguinal canal by a flap of the external oblique fascia. This technique has the advantage over prosthetic cures in that it is a tension-free cure and does not require an implant. The aim of this study is to demonstrate the feasibility of curing inguinal hernias using the Desarda technique, and to evaluate the initial results in our practice. Material And Method: This is a prospective study over a 2-year period (January 2017 - December 2018), covering 100 cases of uncomplicated inguinal hernia cure in 98 patients operated on by aponeurotic plasty (Desarda technique), in the general surgery department of Ignace DEEN Hospital. Selection criteria were: informed consent, age over 15 years, uncomplicated primary inguinal hernias, normal prostate ultrasound and PSA results for adult males over 50 years of age. Results: The study included 100 cases of uncomplicated inguinal hernia repair in 94 patients operated on by aponeurotic plasty (Desarda technique). The patients were 88 men (94%) and 6 women (6%), with a mean age of 44.7 years and extremes of 19 and 78 years. The majority of patients (37 or 39.36%) were blue-collar workers. The hernia was unilateral in 88 patients and bilateral in 6. One woman had a bilateral hernia. The hernia was located only on the right in 72 cases and only on the left in 20. According to the Nyhus classification, type IIIb 45% was the most frequent. The patients were operated on under spinal anesthesia in 68 cases. On the first postoperative day, nine patients (9.57%) were assessed as having moderate pain. Beyond the third month, pain assessment revealed five cases of chronic pain. Surgical site infection was the most frequent complication. With an average follow-up of 17 months, no cases of recurrence were noted.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Inguinal hernia is a protrusion of abdominal cavity contents or pre-peritoneal fat through a hernial defect in the inguinal region
[1]
Berri T; Brahmi K. Inguinal hernias. Algerian medical journal 2021; (36): 62-71.
[1]
. It is a frequent surgical condition, and its etiology is multifactorial
[2]
Huang et al. Lichtenstein inguinal hernia repair with porcine small bowel submucosa: a 5-year follow-up. A prospective randomized controlled study; Regenerative Biomaterials; China-2021; (20) 1-5.
[2]
.
Surgical treatment of inguinal hernia consists in replacing its contents in the abdomen and repairing the abdominal wall.
There is a plethora of techniques for this repair. Regardless of the procedure used, two main objectives are pursued: reducing the recurrence rate and minimizing postoperative pain. Patients are also concerned about when they can return to work. The Lichtenstein procedure, a tension-free prosthetic cure, is considered the gold standard
[3]
Marre P, Pitre J, Timores A. Inguinal hernia repair in adults using the Lichtenstein procedure. Results at 10 years. EMem Acad Natl Chir 2009; 8(2): 46-7.
[3]
. This technique requires the use of prostheses, the cost of which is not within the reach of all our patients. Laparoscopic surgery, which also enables tension-free cure
[4]
Bonnichon Ph, Oberlin O. Evolution of medical thinking in the surgical treatment of male inguinal hernias. E-Mem Acad Natl Chir 2010; 9(4): 30-5.
[5]
Johanet H. Laparoscopic groin hernia repair, the transabdomino preperitoneal route (TAPP): technical aspects and results. E-Mem Acad Natl Chir 2009; 8(2): 38-40.
[4, 5]
, is in its infancy in our practice.
With this in mind, an aponeuroplasty technique based on closure of the posterior wall of the inguinal canal with a flap of the external oblique fascia deserves to be tried out in our country, given the satisfactory results reported by its author
[6]
Desarda MP. Physiological repair of inguinal hernia: a new technique (study of 860 patients). Hernia 2006; 10: 143–6.
[6]
. This technique has the advantage over prosthetic cures in that it is a tension-free cure and does not require an implant.
The aim of this study is to demonstrate the feasibility of curing inguinal hernias using the Desarda technique, and to evaluate the initial results in our practice.
2. Material and Method
This is a prospective study over a 2-year period (January 2017 - December 2018), covering 100 cases of uncomplicated inguinal hernia cure in 98 patients operated on by aponeurotic plasty (Desarda technique), in the general surgery department of Ignace DEEN Hospital.
Selection criteria were: informed consent, age over 15 years, uncomplicated primary inguinal hernias, normal prostate ultrasound and PSA results for adult males over 50 years of age.
2.1. Surgical Method
The patients were operated on by four surgeons familiar with this technique.
The skin incision was a low transverse incision at the level of the lower abdominal fold, or an oblique incision over the projection of the inguinal ligament (figure 1).
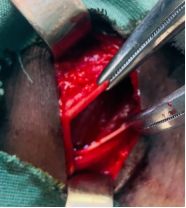
The incision of the aponeurosis of the external oblique muscle was made parallel to the inguinal ligament. This incision revealed two lips: a medial lip and a lateral lip (figure 2).
According to the Nyhus classification, in some cases the hernia sac was found, and the type of hernia was specified.
In cases of external oblique hernia, dissection and ligation of the sac with absorbable suture2/0 or 0 was performed, with isolation of the spermatic cord elements and resection of the cremaster fibers.
In cases of direct hernia, as in this case, the sac was pushed back.
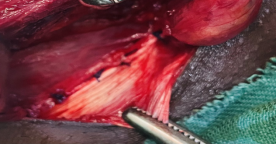
The aponeurotic plasty began by suturing the edge of the medial lip of the external oblique g aponeurosis to the crural arch, currently the inguinal ligament, in separate stitches using non-absorbable monofilament USP 2/0 or 0 (Figure 4).
Suturing began at the pubic spine and continued as far up as possible to the deep inguinal orifice, without strangling the spermatic cord.
An incision was then made over the sutured aponeurosis to obtain a 1-2 cm aponeurotic flap (Figure 3).
Next, the free edge of the aponeurotic flap was sutured to the muscle at the level of the conjoint tendon using separate stitches of non-absorbable monofilament USP 2/0 or 0 thread (Figure 4).
Aponeurotic closure was achieved anteriorly to the cord, by overlocking with USP 2/0 absorbable thread, bringing the lateral lip of the external oblique aponeurosis into contact with the new medial lip of the same aponeurosis (Figure 5).
Finally, the skin was closed in the conventional way (figure 6).
The following parameters were studied: socio-demographic data, type of hernia according to the Nyhus classification, acute postoperative pain assessed on the first postoperative day and chronic pain (from the third postoperative month) assessed using the visual analog scale (VAS), morbidity and recurrence.
3. Results
3.1. Socio Demographic Data
The study included 100 cases of uncomplicated inguinal hernia repair in 94 patients operated on by aponeurotic plasty (Desarda technique). The patients were 88 men (94%) and 6 women (6%), with a mean age of 44.7 years and extremes of 19 and 78 years. The majority of patients (37 or 39.36%) were blue-collar workers.
3.2. Hernia Type
The hernia was unilateral in 88 patients and bilateral in 6. One woman had a bilateral hernia. The hernia was only on the right in 72 cases and only on the left in 20. According to Nyhus classification: type I was 14%, type II 11%, type IIIa 30% and type IIIb 45%.
The hernia was external oblique in 76 cases, direct in 14 and mixed in 2.
3.3. Anaesthesia
Patients underwent rachi anesthesia in 68 cases, followed by local anesthesia in 17 cases and general anesthesia in 9 cases.
3.4. Acute Postoperative Pain (VAS)
On the first postoperative day, nine patients (9.57%) were assessed as having moderate pain, and 08 patients (8.51%) as having mild pain. No patient reported severe pain. Pain was absent in 71 patients (75.53%).
3.5. Chronic Postoperative Pain (VAS)
After the third month, pain assessment revealed five cases of mild chronic pain in the fifth, eighth and tenth months (VAS = 1) and twelfth and fourteenth months (VAS = 2).
3.6. Morbidity
Postoperative complications were reported in 09 patients (9.57%). Surgical site infection was the most frequent (07 patients, 7.44%). Scrotal hematoma was also noted in two patients (2.12%).
3.7. Recurrence
No cases of recurrence were noted in our study; the mean follow-up was 17 months, with extremes of 3 and 27 months.
4. Discussion
External oblique inguinal hernia was the most common type of inguinal hernia in male heavy-duty workers. This predominance of external oblique hernia has been reported by several authors
[7]
M Dieng, M Cissé, M Seck, FK Diallo, AO Touré, I Konaté, O Ka, A Dia, CT Touré Adults inguinal hernia repair by plasty using the large oblique muscle aponevrose: Desarda's tech-nique e-mémoires de l'Académie Nationale de Chirurgie, 2012, 11(2): 069-074.
[8]
Gainant A, Geballa R, Bouvier S, Cubertafond P, Mathonnet M. Prosthetic treatment of bilateral inguinal hernias by laparoscopy or Stoppa operation. Ann Chir 2000; 125: 560-5.
[9]
Manyilirah W, Kijambu S, Upoki A, Kiryabwire J. Comparison of non-mesh (Desarda) and non-mesh (Lichtenstein). Methods for inguinal hernia repair at Mulago hospital. A double-blind randomized controlled trial. Hernia 2012; 16: 133-44.
[7-9]
.
The male predominance may be related to the anatomical features of the male inguinal canal, and to men's daily activities, which often involve repeated physical exertion, exposing them to aggravation of the parietal defect
[10]
Bay-Nielsen M, Kehlet H, Strand L. Quality assessment of 26304 herniorraphies in Denmark: à prospective nationwide study. Lancet 2001, 358: 1124-8.
[10]
.
4.1. Hernia Type
The Nyhus classification enabled us to record 45%.
Dieng reported a comparable result, with type IIIb in 51% of cases
[7]
M Dieng, M Cissé, M Seck, FK Diallo, AO Touré, I Konaté, O Ka, A Dia, CT Touré Adults inguinal hernia repair by plasty using the large oblique muscle aponevrose: Desarda's tech-nique e-mémoires de l'Académie Nationale de Chirurgie, 2012, 11(2): 069-074.
[7]
.
4.2. Anaesthesia
Patients underwent rachi anesthesia in 68 cases, followed by local anesthesia in 17 cases and general anesthesia in 9 cases.
These results correspond well to those of most inguinal hernia operations. Desarda, who performed his technique more often under local or locoregional anesthesia in 98.95% of cases
[7]
M Dieng, M Cissé, M Seck, FK Diallo, AO Touré, I Konaté, O Ka, A Dia, CT Touré Adults inguinal hernia repair by plasty using the large oblique muscle aponevrose: Desarda's tech-nique e-mémoires de l'Académie Nationale de Chirurgie, 2012, 11(2): 069-074.
[7]
.
4.3. Morbidity
Parietal infectious complications after hernia surgery are rare. Desarda reported a parietal infection rate of 0.6% in his series.
Surgical site infection was superficial, with a rate of 7.44%. Hematoma in two patients in 07 patients (7.44%). We also noted a scrotal hematoma in two patients (2.12%). The rate of hematoma in Dieng's study (M) was similar (2.1%). Desarda reported even lower rates, of the order of 0.1%
[7]
M Dieng, M Cissé, M Seck, FK Diallo, AO Touré, I Konaté, O Ka, A Dia, CT Touré Adults inguinal hernia repair by plasty using the large oblique muscle aponevrose: Desarda's tech-nique e-mémoires de l'Académie Nationale de Chirurgie, 2012, 11(2): 069-074.
[7]
. However, his series included a larger number of patients.
4.4. Postoperative Pain
Postoperative pain is an important factor in assessing patient satisfaction after herniorrhaphy. Postoperative pain is an indicator of quality of life and patient satisfaction
[11]
Ananian P, Barrau K, Balandraud P, Le Treut YP. Surgical cure of adult inguinal hernias. Clinical, functional and economic issues of surgical practices. J Chir 2006; 143: 76-83.
[11]
. All hernia surgery techniques, whether performed anteriorly or posteriorly, with or without prosthesis, are thought to be responsible for acute pain, the severity of which depends significantly on the degree of dissection and tissue damage
[12]
Situma SM, Kaggwa S, Masiira NM, et al. Comparison of Desarda versus Modified Bassini inguinal Hernia Repair: A Randomizedcontrolled trial. East and Central African Journal of Surgery 2009; 14: 2.
[12]
.
The results concerning acute postoperative pain are comparable to those reported in the literature.
Chronic pain, i.e. pain occurring 3 months after the operation, i.e. beyond the tissue healing process, is sometimes badly experienced by patients
[11]
Ananian P, Barrau K, Balandraud P, Le Treut YP. Surgical cure of adult inguinal hernias. Clinical, functional and economic issues of surgical practices. J Chir 2006; 143: 76-83.
[13]
Aasvang EK, Bay-Nielsen M, Kehlet H. Pain and functional impairment 6 years after inguinal herniorrhaphy. Hernia 2006; 10: 316–21.
[14]
Vuilleumier H, Hübner M, Demartines N. Neuropathy after herniorrhaphy: Indication for surgical treatment and outcome. World J Surg 2009; 33: 841-5.
[11, 13, 14]
.
The study of this chronic pain was simplified by Cunningham's team, who classified it into three types
[15]
Cunningham J, Temple WJ, Mitchell P, Nixon JA, Preshaw RM, Hagen NA, Cooperative hernia study. Pain in the post-repair patient. Ann Surg 1996; 224: 598 602.
[15]
: somatic pain linked to tension in musculoaponeurotic structures and typically triggered by exertion; neuralgic pain linked to nerve damage in the inguinal canal, spontaneous or triggered, typically violent and brief; and visceral pain linked to obstruction of the vas deferens by scar fibrosis and typically triggered by ejaculation.
Dieng noted the presence of this chronic pain in four patients, all rated as mild on the VAS. Five cases of chronic postoperative pain were reported, all rated as mild.
4.5. Recurrence
Several studies have been carried out on the recurrence rate of hernia surgery. A 0.2% recurrence rate was reported in a retrospective study of 540 patients operated on using the Lichtenstein technique
[16]
Sakorafas GH, Halikias I, Nissotakis C, Kotsifopoulos N, Stavrou A, et al. Open tension free repair of inguinal hernias; the Lichtenstein technique. BMC Surg 2001; 1: 3.
[16]
.
The recurrence rates reported by its author are similar to those of prosthetic genioplasties, with, in addition, a lower direct operative cost
[6]
Desarda MP. Physiological repair of inguinal hernia: a new technique (study of 860 patients). Hernia 2006; 10: 143–6.
[6]
.
Recurrence rates similar to those of prosthetic techniques have also been reported with the aponeurotic plasty of the rectus abdominis according to Vayre Petit Pazos, with a rate of 1.2% at a mean follow-up of 71 months
[17]
Phe V, Bitker MO, Misrai V, Richard F. Cure de hernie inguinale selon la technique de Vayre Petit Pazos: Étude rétrospective à propos de 83 patients consécutifs. E-Mem Acad Natl Chir 2008; 7(2): 26-32.
[17]
.
Dieng also reported no cases of recurrence, with a follow-up of 3 months.
These results are superimposed on those of our study, in which no cases of recurrence were reported with a mean follow-up of 20 months.
5. Conclusion
The Desarda technique, given the low rates of recurrence and chronic postoperative pain that we have noted, and also the lower cost of management compared to prosthetic techniques, may constitute a reliable alternative to the various techniques for inguinal hernia repair in our countries.
Abbreviations
PSA: Prostatic Specific Antigen
VAS: Visual Analog Scale
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Berri T; Brahmi K. Inguinal hernias. Algerian medical journal 2021; (36): 62-71.
[2]
Huang et al. Lichtenstein inguinal hernia repair with porcine small bowel submucosa: a 5-year follow-up. A prospective randomized controlled study; Regenerative Biomaterials; China-2021; (20) 1-5.
[3]
Marre P, Pitre J, Timores A. Inguinal hernia repair in adults using the Lichtenstein procedure. Results at 10 years. EMem Acad Natl Chir 2009; 8(2): 46-7.
[4]
Bonnichon Ph, Oberlin O. Evolution of medical thinking in the surgical treatment of male inguinal hernias. E-Mem Acad Natl Chir 2010; 9(4): 30-5.
[5]
Johanet H. Laparoscopic groin hernia repair, the transabdomino preperitoneal route (TAPP): technical aspects and results. E-Mem Acad Natl Chir 2009; 8(2): 38-40.
[6]
Desarda MP. Physiological repair of inguinal hernia: a new technique (study of 860 patients). Hernia 2006; 10: 143–6.
[7]
M Dieng, M Cissé, M Seck, FK Diallo, AO Touré, I Konaté, O Ka, A Dia, CT Touré Adults inguinal hernia repair by plasty using the large oblique muscle aponevrose: Desarda's tech-nique e-mémoires de l'Académie Nationale de Chirurgie, 2012, 11(2): 069-074.
[8]
Gainant A, Geballa R, Bouvier S, Cubertafond P, Mathonnet M. Prosthetic treatment of bilateral inguinal hernias by laparoscopy or Stoppa operation. Ann Chir 2000; 125: 560-5.
[9]
Manyilirah W, Kijambu S, Upoki A, Kiryabwire J. Comparison of non-mesh (Desarda) and non-mesh (Lichtenstein). Methods for inguinal hernia repair at Mulago hospital. A double-blind randomized controlled trial. Hernia 2012; 16: 133-44.
[10]
Bay-Nielsen M, Kehlet H, Strand L. Quality assessment of 26304 herniorraphies in Denmark: à prospective nationwide study. Lancet 2001, 358: 1124-8.
[11]
Ananian P, Barrau K, Balandraud P, Le Treut YP. Surgical cure of adult inguinal hernias. Clinical, functional and economic issues of surgical practices. J Chir 2006; 143: 76-83.
[12]
Situma SM, Kaggwa S, Masiira NM, et al. Comparison of Desarda versus Modified Bassini inguinal Hernia Repair: A Randomizedcontrolled trial. East and Central African Journal of Surgery 2009; 14: 2.
[13]
Aasvang EK, Bay-Nielsen M, Kehlet H. Pain and functional impairment 6 years after inguinal herniorrhaphy. Hernia 2006; 10: 316–21.
[14]
Vuilleumier H, Hübner M, Demartines N. Neuropathy after herniorrhaphy: Indication for surgical treatment and outcome. World J Surg 2009; 33: 841-5.
[15]
Cunningham J, Temple WJ, Mitchell P, Nixon JA, Preshaw RM, Hagen NA, Cooperative hernia study. Pain in the post-repair patient. Ann Surg 1996; 224: 598 602.
[16]
Sakorafas GH, Halikias I, Nissotakis C, Kotsifopoulos N, Stavrou A, et al. Open tension free repair of inguinal hernias; the Lichtenstein technique. BMC Surg 2001; 1: 3.
[17]
Phe V, Bitker MO, Misrai V, Richard F. Cure de hernie inguinale selon la technique de Vayre Petit Pazos: Étude rétrospective à propos de 83 patients consécutifs. E-Mem Acad Natl Chir 2008; 7(2): 26-32.
Sandaly, D., Lansana, C. F., Togba, S. L., Yaya, D. S., Naby, F., et al. (2024). Inguinal Hernia Repair Using the External Oblique Muscle Fascia: Desarda Technique. Advances in Surgical Sciences, 12(1), 1-5. https://doi.org/10.11648/j.ass.20241201.11
@article{10.11648/j.ass.20241201.11,
author = {Diakite Sandaly and Camara Fode Lansana and Soumaoro Labile Togba and Diakite Saikou Yaya and Fofana Naby and Kondano Saa Yawo and Condé Ansoumane and Camara Mariame and Condé Ousmane and Diallo Mamadou Saliou and Ousmane Abakar and Yom Petang Steve Cyrille and Toure Aboubacar},
title = {Inguinal Hernia Repair Using the External Oblique Muscle Fascia: Desarda Technique
},
journal = {Advances in Surgical Sciences},
volume = {12},
number = {1},
pages = {1-5},
doi = {10.11648/j.ass.20241201.11},
url = {https://doi.org/10.11648/j.ass.20241201.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ass.20241201.11},
abstract = {Introduction: An inguinal hernia is a protrusion of abdominal cavity contents or pre-peritoneal fat through a hernial defect in the inguinal region. Desarda's technique is an aponeuroplasty, based on closure of the posterior wall of the inguinal canal by a flap of the external oblique fascia. This technique has the advantage over prosthetic cures in that it is a tension-free cure and does not require an implant. The aim of this study is to demonstrate the feasibility of curing inguinal hernias using the Desarda technique, and to evaluate the initial results in our practice. Material And Method: This is a prospective study over a 2-year period (January 2017 - December 2018), covering 100 cases of uncomplicated inguinal hernia cure in 98 patients operated on by aponeurotic plasty (Desarda technique), in the general surgery department of Ignace DEEN Hospital. Selection criteria were: informed consent, age over 15 years, uncomplicated primary inguinal hernias, normal prostate ultrasound and PSA results for adult males over 50 years of age. Results: The study included 100 cases of uncomplicated inguinal hernia repair in 94 patients operated on by aponeurotic plasty (Desarda technique). The patients were 88 men (94%) and 6 women (6%), with a mean age of 44.7 years and extremes of 19 and 78 years. The majority of patients (37 or 39.36%) were blue-collar workers. The hernia was unilateral in 88 patients and bilateral in 6. One woman had a bilateral hernia. The hernia was located only on the right in 72 cases and only on the left in 20. According to the Nyhus classification, type IIIb 45% was the most frequent. The patients were operated on under spinal anesthesia in 68 cases. On the first postoperative day, nine patients (9.57%) were assessed as having moderate pain. Beyond the third month, pain assessment revealed five cases of chronic pain. Surgical site infection was the most frequent complication. With an average follow-up of 17 months, no cases of recurrence were noted.
},
year = {2024}
}
TY - JOUR
T1 - Inguinal Hernia Repair Using the External Oblique Muscle Fascia: Desarda Technique
AU - Diakite Sandaly
AU - Camara Fode Lansana
AU - Soumaoro Labile Togba
AU - Diakite Saikou Yaya
AU - Fofana Naby
AU - Kondano Saa Yawo
AU - Condé Ansoumane
AU - Camara Mariame
AU - Condé Ousmane
AU - Diallo Mamadou Saliou
AU - Ousmane Abakar
AU - Yom Petang Steve Cyrille
AU - Toure Aboubacar
Y1 - 2024/04/02
PY - 2024
N1 - https://doi.org/10.11648/j.ass.20241201.11
DO - 10.11648/j.ass.20241201.11
T2 - Advances in Surgical Sciences
JF - Advances in Surgical Sciences
JO - Advances in Surgical Sciences
SP - 1
EP - 5
PB - Science Publishing Group
SN - 2376-6182
UR - https://doi.org/10.11648/j.ass.20241201.11
AB - Introduction: An inguinal hernia is a protrusion of abdominal cavity contents or pre-peritoneal fat through a hernial defect in the inguinal region. Desarda's technique is an aponeuroplasty, based on closure of the posterior wall of the inguinal canal by a flap of the external oblique fascia. This technique has the advantage over prosthetic cures in that it is a tension-free cure and does not require an implant. The aim of this study is to demonstrate the feasibility of curing inguinal hernias using the Desarda technique, and to evaluate the initial results in our practice. Material And Method: This is a prospective study over a 2-year period (January 2017 - December 2018), covering 100 cases of uncomplicated inguinal hernia cure in 98 patients operated on by aponeurotic plasty (Desarda technique), in the general surgery department of Ignace DEEN Hospital. Selection criteria were: informed consent, age over 15 years, uncomplicated primary inguinal hernias, normal prostate ultrasound and PSA results for adult males over 50 years of age. Results: The study included 100 cases of uncomplicated inguinal hernia repair in 94 patients operated on by aponeurotic plasty (Desarda technique). The patients were 88 men (94%) and 6 women (6%), with a mean age of 44.7 years and extremes of 19 and 78 years. The majority of patients (37 or 39.36%) were blue-collar workers. The hernia was unilateral in 88 patients and bilateral in 6. One woman had a bilateral hernia. The hernia was located only on the right in 72 cases and only on the left in 20. According to the Nyhus classification, type IIIb 45% was the most frequent. The patients were operated on under spinal anesthesia in 68 cases. On the first postoperative day, nine patients (9.57%) were assessed as having moderate pain. Beyond the third month, pain assessment revealed five cases of chronic pain. Surgical site infection was the most frequent complication. With an average follow-up of 17 months, no cases of recurrence were noted.
VL - 12
IS - 1
ER -
Sandaly, D., Lansana, C. F., Togba, S. L., Yaya, D. S., Naby, F., et al. (2024). Inguinal Hernia Repair Using the External Oblique Muscle Fascia: Desarda Technique. Advances in Surgical Sciences, 12(1), 1-5. https://doi.org/10.11648/j.ass.20241201.11
@article{10.11648/j.ass.20241201.11,
author = {Diakite Sandaly and Camara Fode Lansana and Soumaoro Labile Togba and Diakite Saikou Yaya and Fofana Naby and Kondano Saa Yawo and Condé Ansoumane and Camara Mariame and Condé Ousmane and Diallo Mamadou Saliou and Ousmane Abakar and Yom Petang Steve Cyrille and Toure Aboubacar},
title = {Inguinal Hernia Repair Using the External Oblique Muscle Fascia: Desarda Technique
},
journal = {Advances in Surgical Sciences},
volume = {12},
number = {1},
pages = {1-5},
doi = {10.11648/j.ass.20241201.11},
url = {https://doi.org/10.11648/j.ass.20241201.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ass.20241201.11},
abstract = {Introduction: An inguinal hernia is a protrusion of abdominal cavity contents or pre-peritoneal fat through a hernial defect in the inguinal region. Desarda's technique is an aponeuroplasty, based on closure of the posterior wall of the inguinal canal by a flap of the external oblique fascia. This technique has the advantage over prosthetic cures in that it is a tension-free cure and does not require an implant. The aim of this study is to demonstrate the feasibility of curing inguinal hernias using the Desarda technique, and to evaluate the initial results in our practice. Material And Method: This is a prospective study over a 2-year period (January 2017 - December 2018), covering 100 cases of uncomplicated inguinal hernia cure in 98 patients operated on by aponeurotic plasty (Desarda technique), in the general surgery department of Ignace DEEN Hospital. Selection criteria were: informed consent, age over 15 years, uncomplicated primary inguinal hernias, normal prostate ultrasound and PSA results for adult males over 50 years of age. Results: The study included 100 cases of uncomplicated inguinal hernia repair in 94 patients operated on by aponeurotic plasty (Desarda technique). The patients were 88 men (94%) and 6 women (6%), with a mean age of 44.7 years and extremes of 19 and 78 years. The majority of patients (37 or 39.36%) were blue-collar workers. The hernia was unilateral in 88 patients and bilateral in 6. One woman had a bilateral hernia. The hernia was located only on the right in 72 cases and only on the left in 20. According to the Nyhus classification, type IIIb 45% was the most frequent. The patients were operated on under spinal anesthesia in 68 cases. On the first postoperative day, nine patients (9.57%) were assessed as having moderate pain. Beyond the third month, pain assessment revealed five cases of chronic pain. Surgical site infection was the most frequent complication. With an average follow-up of 17 months, no cases of recurrence were noted.
},
year = {2024}
}
TY - JOUR
T1 - Inguinal Hernia Repair Using the External Oblique Muscle Fascia: Desarda Technique
AU - Diakite Sandaly
AU - Camara Fode Lansana
AU - Soumaoro Labile Togba
AU - Diakite Saikou Yaya
AU - Fofana Naby
AU - Kondano Saa Yawo
AU - Condé Ansoumane
AU - Camara Mariame
AU - Condé Ousmane
AU - Diallo Mamadou Saliou
AU - Ousmane Abakar
AU - Yom Petang Steve Cyrille
AU - Toure Aboubacar
Y1 - 2024/04/02
PY - 2024
N1 - https://doi.org/10.11648/j.ass.20241201.11
DO - 10.11648/j.ass.20241201.11
T2 - Advances in Surgical Sciences
JF - Advances in Surgical Sciences
JO - Advances in Surgical Sciences
SP - 1
EP - 5
PB - Science Publishing Group
SN - 2376-6182
UR - https://doi.org/10.11648/j.ass.20241201.11
AB - Introduction: An inguinal hernia is a protrusion of abdominal cavity contents or pre-peritoneal fat through a hernial defect in the inguinal region. Desarda's technique is an aponeuroplasty, based on closure of the posterior wall of the inguinal canal by a flap of the external oblique fascia. This technique has the advantage over prosthetic cures in that it is a tension-free cure and does not require an implant. The aim of this study is to demonstrate the feasibility of curing inguinal hernias using the Desarda technique, and to evaluate the initial results in our practice. Material And Method: This is a prospective study over a 2-year period (January 2017 - December 2018), covering 100 cases of uncomplicated inguinal hernia cure in 98 patients operated on by aponeurotic plasty (Desarda technique), in the general surgery department of Ignace DEEN Hospital. Selection criteria were: informed consent, age over 15 years, uncomplicated primary inguinal hernias, normal prostate ultrasound and PSA results for adult males over 50 years of age. Results: The study included 100 cases of uncomplicated inguinal hernia repair in 94 patients operated on by aponeurotic plasty (Desarda technique). The patients were 88 men (94%) and 6 women (6%), with a mean age of 44.7 years and extremes of 19 and 78 years. The majority of patients (37 or 39.36%) were blue-collar workers. The hernia was unilateral in 88 patients and bilateral in 6. One woman had a bilateral hernia. The hernia was located only on the right in 72 cases and only on the left in 20. According to the Nyhus classification, type IIIb 45% was the most frequent. The patients were operated on under spinal anesthesia in 68 cases. On the first postoperative day, nine patients (9.57%) were assessed as having moderate pain. Beyond the third month, pain assessment revealed five cases of chronic pain. Surgical site infection was the most frequent complication. With an average follow-up of 17 months, no cases of recurrence were noted.
VL - 12
IS - 1
ER -