Abstract
Hallucinations are perceptual experiences occurring without external stimuli, presenting in auditory, visual, tactile, olfactory, or gustatory forms. These symptoms are linked to various psychiatric, neurological, and medical conditions, often complicating diagnosis. In this case report, we describe a 67-year-old female with a week-long history of visual hallucinations and cognitive decline. Initial workup, including CT, chest X-ray, CBC/CMP, ECG, and urine drug screen, showed no significant abnormalities except for hyperglycemia and hypomagnesemia. The absence of acute findings, coupled with psychosocial stressors, led to a suspected psychiatric etiology, prompting the emergency department to consult the psychiatric term for primary management. However, a comprehensive, multidisciplinary approach—including neurology and medicine consultations—revealed a much more complex picture. It was discovered later that the patient had a seven-year history of tremors and progressive memory decline, alongside neurological findings such as truncal ataxia, poor coordination, and a wide-based gait during the present hospitalization. Brain MRI later demonstrated cerebellar atrophy and chronic microvascular ischemic changes, leading to a diagnosis of neurocognitive disorder, with a high suspicion for vascular dementia. This case emphasizes the importance of maintaining a broad differential diagnosis when evaluating visual hallucinations, as attributing them prematurely to psychiatric causes can result in delays in appropriate treatment. In cases where the etiology of hallucinations is uncertain, obtaining a detailed history is vital in providing clinicians with the necessary pieces to elucidate the underlying etiology. Recognizing the multiple etiologies of visual hallucinations and remaining meticulous when managing patients with this symptom is essential to prevent diagnostic errors and improve patient outcomes.
Keywords
Visual Hallucinations, Cerebellar Atrophy, Cerebellar Ataxia, Neurocognitive Disorder, Memory Loss, Vascular Dementia, Temporal Lobe Degeneration
1. Introduction
Hallucinations are defined as conscious perceptual experiences in the absence of external stimuli, involving auditory, visual, tactile, olfactory, and/or gustatory modalities. Hallucinations can manifest secondary to multiple medical, psychiatric, and neurological conditions. The wide range of pathologies that can produce hallucinations poses significant diagnostic challenges for patients presenting with this symptom
.
Hallucinations are classically linked with psychiatric disorders (e.g., schizophrenia and mood disorders with psychotic features)
. However, hallucinatory experiences transcend psychiatric etiologies to include conditions such as migraines and epilepsy
. Acute conditions (e.g., severe dehydration, hypoglycemia, high fevers, substance use, and alcohol withdrawal) can also cause visual or auditory hallucinations
. Additional hallucination-evoking pathologies are neoplasms of the brain, Charles Bonnet Syndrome (CBS), temporal lobe epilepsy, delirium, and multiple forms of major neurocognitive disorder
. Of these etiologies, delirium and dementia are frequently overlooked as initial symptomatology may be subtle, atypical, or overlap with psychiatric disorders. The prevalence of hallucinations in non-psychiatric contexts emphasizes the need for a broad differential diagnosis when evaluating patients with this symptom.
This case underscores the importance of a meticulous differential diagnosis and thorough workup when evaluating patients with hallucinations. The subject of this case initially presented with persistent visual hallucinations and cognitive. Her condition was attributed to a psychiatric etiology after the primary workup revealed no medical or neurologic abnormalities. Later in the patient’s hospital stay, after expending additional time and resources, the etiology of the patient’s presentation was suspected to be parenchymal atrophy secondary to neurocognitive disorder (NCD), likely vascular dementia. This case exemplifies that failure to appropriately consider extra-psychiatric explanations for hallucinatory events can lead to delays in diagnosis and worse patient outcomes.
2. Case Presentation
A 67-year-old female with a past medical history of hypertension, hyperlipidemia, type 2 diabetes mellitus, hypothyroidism, and recurrent urinary tract infections (UTIs) with associated mental status changes presented to the emergency department (ED) with a one-week history of visual hallucinations and cognitive decline. According to her husband, the patient exhibited impaired ability to engage in conversation, difficulty completing thoughts and sentences, memory deficits, and several episodes of disorientation. Upon direct questioning, the patient vaguely described visions of “a knight in shining armor” and reported seeing flashes of light, which she attributed to hypoglycemia, as the symptoms improved after eating. The patient denied a history of consistent visual hallucinations. Her husband reports that the patient has no prior psychiatric history, stating that she had been fully independent and free from these symptoms before the onset of hallucinations. However, two weeks before presentation, she had been started on duloxetine (Cymbalta) for decreased energy and motivation secondary to various psychosocial stressors. The husband also reported noticing a tremor in the patient’s upper extremities for the past month.
An initial workup for suspected delirium was conducted in the ED, including a non-contrast head CT, chest X-ray, CBC, CMP, 12-lead ECG, and urine drug screen. The only significant findings were hyperglycemia (149 mg/dL) and hypomagnesemia (1.4 mg/dL). Repeat CBC, CMP, and chest X-ray were unremarkable. Given the psychosocial stressors present at symptom onset, her alert and oriented state to person, place, time, and situation upon arrival to the ED, and the absence of acute pathological findings, the emergency physician suspected a psychiatric etiology. The psychiatry team was consulted for further evaluation.
Upon the psychiatrist’s initial mental status examination, the patient displayed delayed reaction time, blunted affect, poor attention, poor concentration, and impaired memory. These findings raised suspicion for catatonia, but an Ativan challenge (1 mg) failed to produce any clinical improvement. The psychiatrist also performed a neurological exam which yielded cerebellar symptoms such as: truncal ataxia, a wide-based gait, and poor coordination. These symptoms prompted the Psychiatry team to order an MRI of the brain which was interpreted by the radiologist as displaying diffuse parenchymal volume loss representative of chronic disease. A Montreal Cognitive Assessment (MoCA) was performed, yielding a score of 22/30. An EEG revealed mild generalized slowing, indicative of diffuse cerebral dysfunction without focal abnormalities or epileptiform activity. With no definitive diagnosis from the initial workup, the patient was admitted to the inpatient psychiatric unit for further evaluation and management.
During the first day of hospitalization, the patient was restarted on her home medications for diabetes, hypothyroidism, and hypertension. Additionally, low-dose risperidone (0.5 mg orally at night) was initiated to address her visual hallucinations and confusion. Due to her poorly controlled diabetes, the medicine service was consulted, and their intervention helped stabilize her blood glucose levels.
On the second day of hospitalization, neurology services are consulted to determine the underlying etiology of the patient’s condition. A detailed interview with the patient’s daughter revealed that the patient had experienced a tremor for the past seven years and progressive memory decline over the past five years, impairing her ability to maintain employment. Neurological examination revealed signs of cerebellar dysfunction, including severe truncal ataxia, a wide-based gait, and poor coordination. The neurologist also reviewed the previously obtained MRI brain and interpreted the imaging as displaying marked cerebellar atrophy as well as a periventricular and subcortical white matter hyperintense signal possibly representative of chronic microvascular ischemic disease changes. This comprehensive assessment lead the Neurology team to suspect cerebellar atrophy induced neurocognitive disorder as the root of the patients symptoms. This discovery by the consulting neurologist allows the patient to be transferred to the medicine service and receive more optimal care for the remainder of her hospital stay.
Unfortunately, the nature of the patient’s disease process restricts the scope of therapeutic intervention to focus on supporting her capacity to complete mobility-related activities of daily living (MRADLs) through physical and occupational therapy. This case highlights how easily hallucinations can be misattributed to a psychiatric pathology and exemplifies the importance of adequately considering the various etiologies of this symptom.
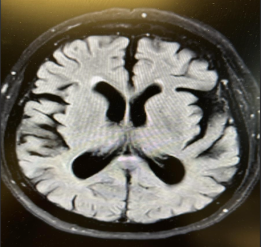
Figure 1. This figure is a T2 weighted MRI image of the patients, that appropriately displays the Temporal lobe atrophy.
Figure 2. This figure is a T1 weighted MRI image of the patients, that appropriately displays the cerebellar atrophy.
3. Discussion
Identifying the cause of a patient’s hallucinations poses a significant diagnostic challenge due to the multitude of potential etiologies; this was further complicated by the patient lacking a history of any previous psychiatric diagnosis or episodes of psychosis. This case exemplifies such complexity, where an extensive workup was conducted without yielding a definitive diagnosis. Presently, it is suspected by the authors that underlying NCD caused neurodegeneration in regions of the brain that prompted the patient to experience visual hallucinations. It is the hope of the authors that by analyzing this case, clinicians may enhance their ability to evaluate and manage hallucinations more effectively.
Hallucinations are inherently conspicuous —they can be vivid, disruptive, and alarming. The nature of hallucinations can lead both the patient and clinician to place excess focus on this symptom during the initial history and diagnostic workup. While this emphasis can be justified when hallucinations arise from a psychiatric etiology, it may detract from the quality of care delivered if the underlying cause is non-psychiatric. As such, an understanding of the interplay between NCDs, psychiatric disorders, and hallucinations is essential for optimal patient care. We present a differential diagnosis to rule in/out common etiologies:
3.1. Psychiatric Causes
A urine drug screen ruled out Illicit substance use, and the family also confirmed no illicit substance use in her lifetime. The family reports that the patient has no prior history of psychosis. It is essential to consider that the emergence of psychotic symptoms in older age often indicates underlying organic conditions that may require further investigation.
3.2. Acute Neurological Causes
All signs of acute neurological infection were negative in this patient.
3.3. Ophthalmological Conditions
The patient's family indicated that she did not present with any eye complications associated with her diabetes, and her visual acuity was normal during the neurological examination. She was negative for cortical blindness, Anton's syndrome, Bálint's syndrome, and Charles Bonnet syndrome, which could potentially contribute to the occurrence of visual hallucinations. However, it is essential to note that the possibility of other eye disorders could not be entirely excluded, given the hospital's limited access to inpatient ophthalmological expertise.
3.4. Limbic Encephalitis
Limbic encephalitis can present with symptoms such as confusion, psychiatric issues, seizures, personality changes, and autonomic instability. In this case, the patient experienced acute confusion and visual hallucinations; however, there were no significant signs of seizures, personality changes, or autonomic instability. The EEG results did not indicate any seizures, and all potential causes of limbic encephalitis were ruled out.
3.5. Paraneoplastic Neurological Syndrome
Paraneoplastic neurological syndromes (PNS) are disorders associated with cancer but are not caused by direct invasion, metastasis, or the effects of treatment. These syndromes are typically autoimmune and often present before the actual signs of cancer. Onconeural antibodies play a crucial role in diagnosing and managing these conditions. The neurology team aimed to rule out PNS for the patient, who had been transferred to the medical floor for further evaluation. After conducting the necessary scans and laboratory tests, PNS was ruled out.
3.6. Cerebellar Cognitive Syndrome
The patient demonstrated involvement of the cerebellum, prompting the medical team to consider a differential diagnosis of Cerebellar Cognitive Syndrome
. Notably, behavioral changes were especially pronounced in patients with lesions in the cerebellum's posterior lobe and the vermis. In certain instances, these alterations in behavior constituted the most prominent aspect of the patient's clinical presentation. The observed impairments in our patient included significant challenges in executive functions, such as planning, set-shifting, verbal fluency, abstract reasoning, and working memory, which would coincide with vascular dementia. As patient did not have any posterior cerebellar lobe or vermis involved this diagnosis was ruled out.
This interplay between NCDs, psychiatric disorders, and hallucinations has been well-documented
| [12] | Waters F, Fernyhough C. Hallucinations: A Systematic Review of Points of Similarity and Difference Across Diagnostic Classes. SCHBUL. 2017; 43(1): 32-43. https://doi.org/10.1093/schbul/sbw132 |
| [13] | O’Brien J, Taylor JP, Ballard C, et al. Visual hallucinations in neurological and ophthalmological disease: pathophysiology and management. J Neurol Neurosurg Psychiatry. 2020; 91(5): 512-519. https://doi.org/10.1136/jnnp-2019-322702 |
[12, 13]
. For example, Lewy body dementia, a classification of NCD, frequently manifests with visual hallucinations
. In contrast, late-stage schizophrenia—a psychiatric disorder characterized by hallucinations— may cause cognitive deficits such as memory loss and impaired executive function, which are usually associated with NCD
| [15] | Sachdev PS, Blacker D, Blazer DG, et al. Classifying neurocognitive disorders: the DSM-5 approach. Nat Rev Neurol. 2014; 10(11): 634-642. https://doi.org/10.1038/nrneurol.2014.181 |
| [16] | Yang VX, Sin Fai Lam CC, Kane JPM. Cognitive impairment and development of dementia in very late-onset schizophrenia-like psychosis: a systematic review. Ir j psychol Med. 2023; 40(4): 616-628. https://doi.org/10.1017/ipm.2021.48 |
[15, 16]
. In the present case, the leading hypothesis of the authors is that vascular dementia (a classification of NCD) is the primary etiology of the patient’s condition. This hypothesis is supported by the patient’s age at presentation, history of hypertension, hypercholesterolemia, and hyperglycemia, stepwise progression of symptoms, and evidence of intracranial atherosclerotic disease. Upon intracranial CTA obtained during subsequent hospitalization, the authors were able to identify extensive cerebellar atrophy, diffuse parenchymal atrophy, periventricular and deep white matter lesions, and significant temporal lobe atrophy. These MRI images, when evaluated using the Fazeki’s scale, demonstrated degeneration consistent with 2-3 on the scale; this indicates the patient had significant, chronic small vessel ischemia (source). These findings, when accounting for the patient’s history, risk factors, and general neuroimaging findings, are supportive of vascular dementia being the most likely etiology. Identifying the regions of the patient’s brain that are lesioned likely explains the onset of her hallucinations.
Existing literature highlights a strong association between visual hallucinations and the occipital lobe
| [17] | Holroyd S, Shepherd ML, Downs JH. Occipital Atrophy Is Associated With Visual Hallucinations in Alzheimer’s Disease. JNP. 2000; 12(1): 25-28. https://doi.org/10.1176/jnp.12.1.25 |
[17]
. However, recent studies implicate other brain regions in the pathogenesis of visual hallucinations, including the supramarginal, fusiform, and cingulate gyri, thalamus, temporal lobe, and cerebellum
| [18] | Matar E, Brooks D, Lewis SJG, Halliday GM. Limbic thalamus atrophy is associated with visual hallucinations in Lewy body disorders. Neurobiol Aging. 2022; 112: 122-128. https://doi.org/10.1016/j.neurobiolaging.2022.01.001 |
| [19] | Watanabe H, Senda J, Kato S, et al. Cortical and subcortical brain atrophy in Parkinson’s disease with visual hallucination. Mov Disord. 2013; 28(12): 1732-1736. https://doi.org/10.1002/mds.25641 |
| [20] | Carter R, Ffytche DH. On visual hallucinations and cortical networks: a trans-diagnostic review. J Neurol. 2015; 262(7): 1780-1790. https://doi.org/10.1007/s00415-015-7687-6 |
| [21] | Rollins CPE, Garrison JR, Simons JS, et al. Meta-analytic Evidence for the Plurality of Mechanisms in Transdiagnostic Structural MRI Studies of Hallucination Status. EClinicalMedicine. 2019; 8: 57-71. https://doi.org/10.1016/j.eclinm.2019.01.012 |
[18-21]
. Understanding that many neuroanatomic regions are associated with visual hallucinations, maintaining an index of suspicion for neurologic involvement when this symptom manifests, particularly when the initial workup is inconclusive, is warranted. In this case, it was only after a neurology consultation was placed that notable exam findings—such as severe truncal ataxia, a wide-based gait, and bilateral decrement in rapid finger tapping—were discovered, and cerebellar dysfunction was revealed. It was not until a meticulous review of neuroimaging post-discharge that lesions in the temporal lobe and supramarginal gyrus were also uncovered. The presence of pathology in hallucination-associated brain regions, alongside the patient’s exam findings, supports the hypothesis that NCD is the underlying cause of the patient’s clinical picture.
4. Conclusion
This case highlights the importance of maintaining a broad differential diagnosis and conducting a thorough workup when evaluating patients with hallucinations. Clinicians should first exclude common medical causes such as hypoglycemia, infection, and substance use. If further workup is indicated, a detailed neurologic examination is warranted, accompanied by appropriate neuroimaging. Clinicians can improve diagnostic accuracy and enhance patient outcomes by employing a systematic approach that integrates the patient’s history, physical examination, laboratory and imaging studies, while ruling out medical, neurologic, and other non-psychiatric causes before attributing hallucinations to a psychiatric origin.
Abbreviations
CBS | Charles Bonnet Syndrome |
NCD | Neurocognitive Disorder |
UTI | Urinary Tract Infection |
ED | Emergency Department |
CT | Computed Tomography Scan |
CBC | Complete Blood Count |
CMP | Comprehensive Metabolic Panel |
ECG | Electrocardiogram |
MRI | Magnetic Resonance Imaging |
MOCA | Montreal Cognitive Assessment |
EEG | electroencephalogram |
MRADLs | Mobility-Related Activities Of Daily Living |
CTA | Computed Tomography Angiography |
PNS | Paraneoplastic Neurological Syndromes |
Acknowledgments
The authors would like to recognize the suggestions and guidance offered by Sarah Hughes on this paper.
Author Contributions
Michael Watcher: Conceptualization, Supervision, Visualization, Writing- Original Draft, Writing – review & editing
Nicholas Coyne: Conceptualization, Investigation Writing- Original Draft, Writing – review & editing
Emma Shychuck: Investigation, Writing – original draft, Writing – review & editing
Thivijan Arivalahan: Writing – original draft, Writing – review & editing
Ankit Chalia: Writing – review & editing
Michael Ang-Rabanes: Writing-Review & Editing
Raja Mogallapu: Conceptualization, Supervision, Visualization, Writing – review & editing
Funding
This work is not supported by any external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Hare SM. Hallucinations: A Functional Network Model of How Sensory Representations Become Selected for Conscious Awareness in Schizophrenia. Front Neurosci. 2021; 15: 733038.
https://doi.org/10.3389/fnins.2021.733038
|
| [2] |
Chaudhury S. Hallucinations: Clinical aspects and management. Ind Psychiatry J. 2010; 19(1): 5.
https://doi.org/10.4103/0972-6748.77625
|
| [3] |
Gudlavalleti A, Tenny S. Cerebellar Neurological Signs. In: StatPearls. StatPearls Publishing; 2024. Accessed September 14, 2024.
http://www.ncbi.nlm.nih.gov/books/NBK556080/
|
| [4] |
Pezzoli S, Cagnin A, Bandmann O, Venneri A. Structural and Functional Neuroimaging of Visual Hallucinations in Lewy Body Disease: A Systematic Literature Review. Brain Sciences. 2017; 7(7): 84.
https://doi.org/10.3390/brainsci7070084
|
| [5] |
Hwang K. Hallucinations in Children with Plague: A Point of View from 400 Years Ago. Infect Chemother. 2022; 54(3): 563.
https://doi.org/10.3947/ic.2022.0055
|
| [6] |
Sharma V, Shah K, Reddy Mallimala P, Sharma K. A Rare Case of Visual Hallucinations Associated With Hyponatremia. Cureus. Published online August 31, 2023.
https://doi.org/10.7759/cureus.44485
|
| [7] |
Bhat P, Ryali V, Srivastava K, Kumar S, Prakash J, Singal A. Alcoholic hallucinosis. Ind Psychiatry J. 2012; 21(2): 155.
https://doi.org/10.4103/0972-6748.119646
|
| [8] |
Lyra A, Cordeiro Q, Shiozawa P. Catatonia After Glioblastoma Multiforme in a Patient With Schizophrenia: The Importance of Establishing Etiology. JNP. 2015; 27(3): e216-e217.
https://doi.org/10.1176/appi.neuropsych.14120388
|
| [9] |
Hamedani AG, Pelak VS. The Charles Bonnet Syndrome: a Systematic Review of Diagnostic Criteria. Curr Treat Options Neurol. 2019; 21(9): 41.
https://doi.org/10.1007/s11940-019-0582-1
|
| [10] |
Vinti V, Dell’Isola GB, Tascini G, et al. Temporal Lobe Epilepsy and Psychiatric Comorbidity. Front Neurol. 2021; 12: 775781.
https://doi.org/10.3389/fneur.2021.775781
|
| [11] |
Schmahmann JD, Sherman JC. The cerebellar cognitive affective syndrome. Brain. 1998; 121 (Pt 4): 561-579.
https://doi.org/10.1093/brain/121.4.561
|
| [12] |
Waters F, Fernyhough C. Hallucinations: A Systematic Review of Points of Similarity and Difference Across Diagnostic Classes. SCHBUL. 2017; 43(1): 32-43.
https://doi.org/10.1093/schbul/sbw132
|
| [13] |
O’Brien J, Taylor JP, Ballard C, et al. Visual hallucinations in neurological and ophthalmological disease: pathophysiology and management. J Neurol Neurosurg Psychiatry. 2020; 91(5): 512-519.
https://doi.org/10.1136/jnnp-2019-322702
|
| [14] |
Hanson JC, Lippa CF. Lewy body dementia. Int Rev Neurobiol. 2009; 84: 215-228.
https://doi.org/10.1016/S0074-7742(09)00411-5
|
| [15] |
Sachdev PS, Blacker D, Blazer DG, et al. Classifying neurocognitive disorders: the DSM-5 approach. Nat Rev Neurol. 2014; 10(11): 634-642.
https://doi.org/10.1038/nrneurol.2014.181
|
| [16] |
Yang VX, Sin Fai Lam CC, Kane JPM. Cognitive impairment and development of dementia in very late-onset schizophrenia-like psychosis: a systematic review. Ir j psychol Med. 2023; 40(4): 616-628.
https://doi.org/10.1017/ipm.2021.48
|
| [17] |
Holroyd S, Shepherd ML, Downs JH. Occipital Atrophy Is Associated With Visual Hallucinations in Alzheimer’s Disease. JNP. 2000; 12(1): 25-28.
https://doi.org/10.1176/jnp.12.1.25
|
| [18] |
Matar E, Brooks D, Lewis SJG, Halliday GM. Limbic thalamus atrophy is associated with visual hallucinations in Lewy body disorders. Neurobiol Aging. 2022; 112: 122-128.
https://doi.org/10.1016/j.neurobiolaging.2022.01.001
|
| [19] |
Watanabe H, Senda J, Kato S, et al. Cortical and subcortical brain atrophy in Parkinson’s disease with visual hallucination. Mov Disord. 2013; 28(12): 1732-1736.
https://doi.org/10.1002/mds.25641
|
| [20] |
Carter R, Ffytche DH. On visual hallucinations and cortical networks: a trans-diagnostic review. J Neurol. 2015; 262(7): 1780-1790.
https://doi.org/10.1007/s00415-015-7687-6
|
| [21] |
Rollins CPE, Garrison JR, Simons JS, et al. Meta-analytic Evidence for the Plurality of Mechanisms in Transdiagnostic Structural MRI Studies of Hallucination Status. EClinicalMedicine. 2019; 8: 57-71.
https://doi.org/10.1016/j.eclinm.2019.01.012
|
Cite This Article
-
APA Style
Watcher, M., Coyne, N., Shychuck, E., Arivalahan, T., Chalia, A., et al. (2024). Evaluating Hallucinations: An Instructional Case Report on Common Mistakes in Developing a Differential Diagnosis. American Journal of Psychiatry and Neuroscience, 12(4), 74-79. https://doi.org/10.11648/j.ajpn.20241204.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Watcher, M.; Coyne, N.; Shychuck, E.; Arivalahan, T.; Chalia, A., et al. Evaluating Hallucinations: An Instructional Case Report on Common Mistakes in Developing a Differential Diagnosis. Am. J. Psychiatry Neurosci. 2024, 12(4), 74-79. doi: 10.11648/j.ajpn.20241204.13
Copy
|
Download
AMA Style
Watcher M, Coyne N, Shychuck E, Arivalahan T, Chalia A, et al. Evaluating Hallucinations: An Instructional Case Report on Common Mistakes in Developing a Differential Diagnosis. Am J Psychiatry Neurosci. 2024;12(4):74-79. doi: 10.11648/j.ajpn.20241204.13
Copy
|
Download
-
@article{10.11648/j.ajpn.20241204.13,
author = {Michael Watcher and Nick Coyne and Emma Shychuck and Thivijiana Arivalahan and Ankit Chalia and Michael Ang-Rabanes and Raja Mogallapu},
title = {Evaluating Hallucinations: An Instructional Case Report on Common Mistakes in Developing a Differential Diagnosis},
journal = {American Journal of Psychiatry and Neuroscience},
volume = {12},
number = {4},
pages = {74-79},
doi = {10.11648/j.ajpn.20241204.13},
url = {https://doi.org/10.11648/j.ajpn.20241204.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajpn.20241204.13},
abstract = {Hallucinations are perceptual experiences occurring without external stimuli, presenting in auditory, visual, tactile, olfactory, or gustatory forms. These symptoms are linked to various psychiatric, neurological, and medical conditions, often complicating diagnosis. In this case report, we describe a 67-year-old female with a week-long history of visual hallucinations and cognitive decline. Initial workup, including CT, chest X-ray, CBC/CMP, ECG, and urine drug screen, showed no significant abnormalities except for hyperglycemia and hypomagnesemia. The absence of acute findings, coupled with psychosocial stressors, led to a suspected psychiatric etiology, prompting the emergency department to consult the psychiatric term for primary management. However, a comprehensive, multidisciplinary approach—including neurology and medicine consultations—revealed a much more complex picture. It was discovered later that the patient had a seven-year history of tremors and progressive memory decline, alongside neurological findings such as truncal ataxia, poor coordination, and a wide-based gait during the present hospitalization. Brain MRI later demonstrated cerebellar atrophy and chronic microvascular ischemic changes, leading to a diagnosis of neurocognitive disorder, with a high suspicion for vascular dementia. This case emphasizes the importance of maintaining a broad differential diagnosis when evaluating visual hallucinations, as attributing them prematurely to psychiatric causes can result in delays in appropriate treatment. In cases where the etiology of hallucinations is uncertain, obtaining a detailed history is vital in providing clinicians with the necessary pieces to elucidate the underlying etiology. Recognizing the multiple etiologies of visual hallucinations and remaining meticulous when managing patients with this symptom is essential to prevent diagnostic errors and improve patient outcomes.},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Evaluating Hallucinations: An Instructional Case Report on Common Mistakes in Developing a Differential Diagnosis
AU - Michael Watcher
AU - Nick Coyne
AU - Emma Shychuck
AU - Thivijiana Arivalahan
AU - Ankit Chalia
AU - Michael Ang-Rabanes
AU - Raja Mogallapu
Y1 - 2024/12/30
PY - 2024
N1 - https://doi.org/10.11648/j.ajpn.20241204.13
DO - 10.11648/j.ajpn.20241204.13
T2 - American Journal of Psychiatry and Neuroscience
JF - American Journal of Psychiatry and Neuroscience
JO - American Journal of Psychiatry and Neuroscience
SP - 74
EP - 79
PB - Science Publishing Group
SN - 2330-426X
UR - https://doi.org/10.11648/j.ajpn.20241204.13
AB - Hallucinations are perceptual experiences occurring without external stimuli, presenting in auditory, visual, tactile, olfactory, or gustatory forms. These symptoms are linked to various psychiatric, neurological, and medical conditions, often complicating diagnosis. In this case report, we describe a 67-year-old female with a week-long history of visual hallucinations and cognitive decline. Initial workup, including CT, chest X-ray, CBC/CMP, ECG, and urine drug screen, showed no significant abnormalities except for hyperglycemia and hypomagnesemia. The absence of acute findings, coupled with psychosocial stressors, led to a suspected psychiatric etiology, prompting the emergency department to consult the psychiatric term for primary management. However, a comprehensive, multidisciplinary approach—including neurology and medicine consultations—revealed a much more complex picture. It was discovered later that the patient had a seven-year history of tremors and progressive memory decline, alongside neurological findings such as truncal ataxia, poor coordination, and a wide-based gait during the present hospitalization. Brain MRI later demonstrated cerebellar atrophy and chronic microvascular ischemic changes, leading to a diagnosis of neurocognitive disorder, with a high suspicion for vascular dementia. This case emphasizes the importance of maintaining a broad differential diagnosis when evaluating visual hallucinations, as attributing them prematurely to psychiatric causes can result in delays in appropriate treatment. In cases where the etiology of hallucinations is uncertain, obtaining a detailed history is vital in providing clinicians with the necessary pieces to elucidate the underlying etiology. Recognizing the multiple etiologies of visual hallucinations and remaining meticulous when managing patients with this symptom is essential to prevent diagnostic errors and improve patient outcomes.
VL - 12
IS - 4
ER -
Copy
|
Download