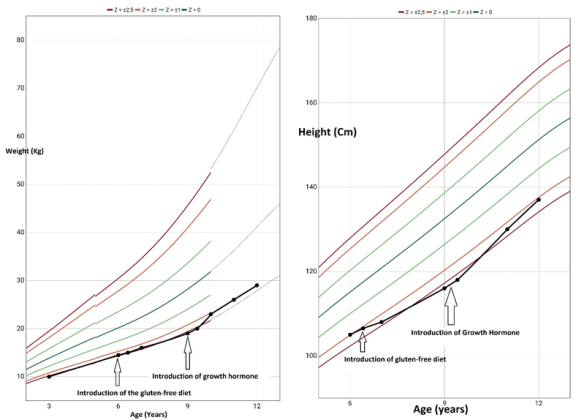
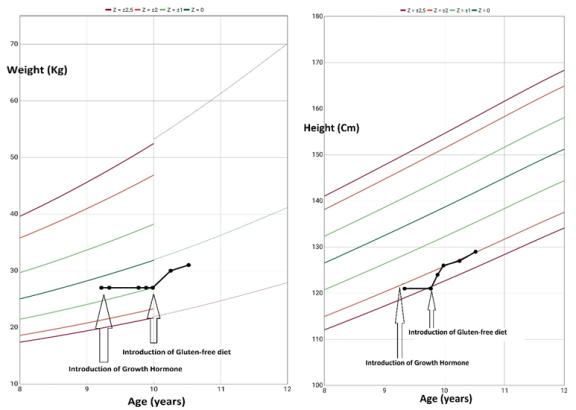
Growth is a complex and multifactorial process influenced by a combination of genetic, environmental, and hormonal factors. The regulation of growth involves a delicate balance of these factors, with hormones, such as growth hormone (GH), playing a pivotal role in the development of linear growth. Growth disorders, such as stunted growth, are common reasons for consultation in pediatric practices. However, diagnosing the cause of stunted growth can be a challenging task, as there are numerous potential contributing factors. These factors are often intertwined, with patients frequently presenting with two or more abnormalities simultaneously, such as growth hormone deficiency (GHD) and celiac disease. This overlapping of conditions can complicate diagnosis, as the symptoms of one condition may mask those of another, leading to a delay in identifying the true underlying cause. In our observation, we report two cases of patients who presented with growth disorders, each demonstrating how one condition can obscure another. The first patient was initially diagnosed with celiac disease, and while a gluten-free diet was implemented, there was little improvement in growth. Further investigations revealed an additional diagnosis of growth hormone deficiency, highlighting the importance of considering multiple diagnoses in cases of stunted growth. The second patient was first diagnosed with growth hormone deficiency, but after further evaluation, a diagnosis of celiac disease was made, which helped explain the persistence of the growth issues. In conclusion, stunted growth can result from various factors, and the presence of one disease can mask another. Thus, it is crucial to conduct thorough investigations and reconsider initial diagnoses to ensure that all potential causes are explored and appropriately addressed.
| Published in | American Journal of Pediatrics (Volume 11, Issue 2) |
| DOI | 10.11648/j.ajp.20251102.12 |
| Page(s) | 43-48 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Growth, Regulation, Growth Hormone, Celiac Disease, Autoimmune Diseases
GH | Growth Hormone |
GHD | Growth Hormone Deficiency |
ACT | Asthma Control Test |
SD | Standard Deviations |
IGF1 | Insulin-like Growth Factor 1 |
FSH | Follicle Stimulating Hormone |
LH | Luteinizing Hormone |
MRI | Magnetic Resonance Imaging |
NMDA | N-methyl-D-aspartate |
TSH | Thyroid Stimulating Hormone |
Anti-TPO | Anti-Thyroid Peroxidase |
ACTH | Adrenocorticotropic Hormone |
Kg | Kilogramme |
Cm | Centimeter |
| [1] | Erfanti DO, Setiabudi D, Rusmil K. The Relationship of Psychosocial Dysfunction and Stunting of Adolescents in Suburban, Indonesia. Open J Med Psychol. 8 sept 2016; 5(4): 57-65. |
| [2] | Giovenale D, Meazza C, Cardinale GM, Sposito M, Mastrangelo C, Messini B, et al. The Prevalence of Growth Hormone Deficiency and Celiac Disease in Short Children. Clin Med Res. 9 jan 2006; 4(3): 180-3. |
| [3] | Boguszewski MCS, Cardoso-Demartini A, Frey MCG, Celli A. Celiac disease, short stature and growth hormone deficiency. 2015; 4. |
| [4] | Feldt-Rasmussen U, Klose M. Adult Growth Hormone Deficiency- Clinical Management. In: Feingold KR, Anawalt B, Blackman MR, Boyce A, Chrousos G, Corpas E, et al., éditeurs. Endotext South Dartmouth (MA): MDText.com, Inc.; 2000. |
| [5] | Bozzola M, Giovenale D, Bozzola E, Meazza C, Martinetti M, Tinelli C, et al. Growth hormone deficiency and coeliac disease: an unusual association? Clin Endocrinol (Oxf). 2005; 62(3): 372-5. |
| [6] | Brand PLP. Inhaled corticosteroids reduce growth. Or do they? Eur Respir J. 1 feb 2001; 17(2): 287-94. |
| [7] | Prevalence of celiac disease in Tunisia: Mass-screening study in schoolchildren | 8 déc 2024 |
| [8] | Boutatss N, Essabah HN, El AS, Chadli A. Association of celiac disease and growth hormone deficiency: a report on 4 cases. In: Endocrine Abstracts. Bioscientifica; 2024 |
| [9] | Cavallo F, Mohn A, Chiarelli F, Giannini C. Evaluation of Bone Age in Children: A Mini-Review. Front Pediatr. 12 march 2021; 9: 580314. |
| [10] | Murray PG, Dattani MT, Clayton PE. Controversies in the diagnosis and management of growth hormone deficiency in childhood and adolescence. Arch Dis Child. jan 2016; 101: 96-100. |
| [11] | Mameli C, Guadagni L, Orso M, Calcaterra V, Wasniewska MG, Aversa T, et al. Epidemiology of growth hormone deficiency in children and adolescents: a systematic review. Endocrine. 2024; 85(1): 91-8. |
| [12] | Saadah OI. Short children with impaired growth hormone secretion. Saudi Med J. jan 2020; 41(1): 68-72. |
| [13] | Nemet D, Raz A, Zifman E, Morag H, Eliakim A. Short stature, celiac disease and growth hormone deficiency. J Pediatr Endocrinol Metab JPEM. oct 2009; 22(10): 979-83. |
| [14] |
Ramachandran S. Growth Hormone Treatment Outcomes in Indian Children with Celiac Disease and Growth Hormone Deficiency. 2023;
https://jajgastrohepto.org/wp-content/uploads/2023/11/JJGH-v10-1882.pdf |
| [15] | A G, F DD, V M, M M, Mi S, A M, et al. A retrospective evaluation of the association of celiac disease and growth hormone deficiency: more than a casual association? |
APA Style
Jelalia, N., Marzouk, A., Thebti, R., Garbaa, A., Jallouli, L., et al. (2025). Celiac Disease and GH Deficiency in Children: A Case Report. American Journal of Pediatrics, 11(2), 43-48. https://doi.org/10.11648/j.ajp.20251102.12
ACS Style
Jelalia, N.; Marzouk, A.; Thebti, R.; Garbaa, A.; Jallouli, L., et al. Celiac Disease and GH Deficiency in Children: A Case Report. Am. J. Pediatr. 2025, 11(2), 43-48. doi: 10.11648/j.ajp.20251102.12
AMA Style
Jelalia N, Marzouk A, Thebti R, Garbaa A, Jallouli L, et al. Celiac Disease and GH Deficiency in Children: A Case Report. Am J Pediatr. 2025;11(2):43-48. doi: 10.11648/j.ajp.20251102.12
@article{10.11648/j.ajp.20251102.12,
author = {Nour Jelalia and Asma Marzouk and Rahma Thebti and Altaf Garbaa and Leila Jallouli and Farida Fariha and Ahlem Kefi and Asma Bouaziz},
title = {Celiac Disease and GH Deficiency in Children: A Case Report
},
journal = {American Journal of Pediatrics},
volume = {11},
number = {2},
pages = {43-48},
doi = {10.11648/j.ajp.20251102.12},
url = {https://doi.org/10.11648/j.ajp.20251102.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20251102.12},
abstract = {Growth is a complex and multifactorial process influenced by a combination of genetic, environmental, and hormonal factors. The regulation of growth involves a delicate balance of these factors, with hormones, such as growth hormone (GH), playing a pivotal role in the development of linear growth. Growth disorders, such as stunted growth, are common reasons for consultation in pediatric practices. However, diagnosing the cause of stunted growth can be a challenging task, as there are numerous potential contributing factors. These factors are often intertwined, with patients frequently presenting with two or more abnormalities simultaneously, such as growth hormone deficiency (GHD) and celiac disease. This overlapping of conditions can complicate diagnosis, as the symptoms of one condition may mask those of another, leading to a delay in identifying the true underlying cause. In our observation, we report two cases of patients who presented with growth disorders, each demonstrating how one condition can obscure another. The first patient was initially diagnosed with celiac disease, and while a gluten-free diet was implemented, there was little improvement in growth. Further investigations revealed an additional diagnosis of growth hormone deficiency, highlighting the importance of considering multiple diagnoses in cases of stunted growth. The second patient was first diagnosed with growth hormone deficiency, but after further evaluation, a diagnosis of celiac disease was made, which helped explain the persistence of the growth issues. In conclusion, stunted growth can result from various factors, and the presence of one disease can mask another. Thus, it is crucial to conduct thorough investigations and reconsider initial diagnoses to ensure that all potential causes are explored and appropriately addressed.
},
year = {2025}
}
TY - JOUR T1 - Celiac Disease and GH Deficiency in Children: A Case Report AU - Nour Jelalia AU - Asma Marzouk AU - Rahma Thebti AU - Altaf Garbaa AU - Leila Jallouli AU - Farida Fariha AU - Ahlem Kefi AU - Asma Bouaziz Y1 - 2025/04/10 PY - 2025 N1 - https://doi.org/10.11648/j.ajp.20251102.12 DO - 10.11648/j.ajp.20251102.12 T2 - American Journal of Pediatrics JF - American Journal of Pediatrics JO - American Journal of Pediatrics SP - 43 EP - 48 PB - Science Publishing Group SN - 2472-0909 UR - https://doi.org/10.11648/j.ajp.20251102.12 AB - Growth is a complex and multifactorial process influenced by a combination of genetic, environmental, and hormonal factors. The regulation of growth involves a delicate balance of these factors, with hormones, such as growth hormone (GH), playing a pivotal role in the development of linear growth. Growth disorders, such as stunted growth, are common reasons for consultation in pediatric practices. However, diagnosing the cause of stunted growth can be a challenging task, as there are numerous potential contributing factors. These factors are often intertwined, with patients frequently presenting with two or more abnormalities simultaneously, such as growth hormone deficiency (GHD) and celiac disease. This overlapping of conditions can complicate diagnosis, as the symptoms of one condition may mask those of another, leading to a delay in identifying the true underlying cause. In our observation, we report two cases of patients who presented with growth disorders, each demonstrating how one condition can obscure another. The first patient was initially diagnosed with celiac disease, and while a gluten-free diet was implemented, there was little improvement in growth. Further investigations revealed an additional diagnosis of growth hormone deficiency, highlighting the importance of considering multiple diagnoses in cases of stunted growth. The second patient was first diagnosed with growth hormone deficiency, but after further evaluation, a diagnosis of celiac disease was made, which helped explain the persistence of the growth issues. In conclusion, stunted growth can result from various factors, and the presence of one disease can mask another. Thus, it is crucial to conduct thorough investigations and reconsider initial diagnoses to ensure that all potential causes are explored and appropriately addressed. VL - 11 IS - 2 ER -
Pediatrics and Neonatology Department, Faculty of Medecine of Tunis, University El Manar, Yasminette Ben Arous, Tunisia
Pediatrics and Neonatology Department, Faculty of Medecine of Tunis, University El Manar, Yasminette Ben Arous, Tunisia
Pediatrics and Neonatology Department, Faculty of Medecine of Tunis, University El Manar, Yasminette Ben Arous, Tunisia
Information