Background: Urinary tract infections (UTI) are common in children and pose a significant public health concern, particularly in low-resource settings like Bangladesh. Rapid, cost-effective diagnostic tools such as urinary nitrite and leukocyte esterase dipstick tests offer an alternative to traditional urine culture, which is often time-consuming and resource-intensive. This study aimed to evaluate the diagnostic accuracy of urinary nitrite and leukocyte esterase tests in detecting UTI in children. Methods: This cross-sectional study was conducted at Shaheed Suhrawardy Medical College Hospital, Dhaka, Bangladesh, from July 2019 to December 2019. A total of 200 children, including 100 cases with proven UTI by culture or microscopy and 100 controls, were enrolled. Urinary nitrite and leukocyte esterase tests were performed on urine samples, with urine culture used as the gold standard. Sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) were calculated to assess diagnostic performance. Results: The urinary nitrite test demonstrated a sensitivity of 75.56% and a specificity of 97.00%, with an overall accuracy of 90.34%. The PPV was 91.89%, and the NPV was 89.81%. The leukocyte esterase test showed a sensitivity of 88.89% and a specificity of 82.00%, with an accuracy of 84.14%, PPV of 68.97%, and NPV of 94.25%. Compared with urine R/E, the urinary nitrate test had strong specificity (97.00%) but moderate sensitivity (47.78%), while the leukocyte esterase test maintained high sensitivity (86.67%) and reliable NPV (87.23%). Conclusion: Both urinary nitrite and leukocyte esterase dipstick tests are effective rapid screening tools for diagnosing UTI in children, with high specificity and sensitivity, respectively. Their combined use can enhance diagnostic accuracy, particularly in settings where access to culture testing is limited. These findings support the implementation of dipstick tests as a reliable first-line diagnostic method for pediatric UTI.
| Published in | American Journal of Pediatrics (Volume 10, Issue 4) |
| DOI | 10.11648/j.ajp.20241004.18 |
| Page(s) | 206-214 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Urinary Tract Infection, Urinary Nitrite, Leukocyte Esterase, Pediatric UTI, Diagnostic Accuracy, Urine Culture, Bangladesh
Variables | Case (n=100) | Control (n=100) | p-value | ||
|---|---|---|---|---|---|
n | % | n | % | ||
Age | |||||
2-5 years | 40 | 40.0% | 30 | 30.0% | 0.182 |
6-12 years | 60 | 60.0% | 70 | 70.0% | |
Mean±SD | 6.68±2.78 | 7.20±2.73 | 0.184 | ||
Sex | |||||
Male | 36 | 36.0% | 38 | 38.0% | 0.884 |
Female | 64 | 64.0% | 62 | 62.0% | |
Residence | |||||
Rural | 42 | 42.0% | 38 | 38.0% | 0.17 |
Urban | 28 | 28.0% | 40 | 40.0% | |
Urban-Slum | 30 | 30.0% | 22 | 22.0% | |
Clinical Presentation | n | % |
|---|---|---|
Fever | 74 | 74.0% |
Abdominal pain | 49 | 49.0% |
Dysuria | 40 | 40.0% |
Frequency of Micturition | 42 | 42.0% |
Vomiting | 36 | 36.0% |
Malodorous Urine | 22 | 22.0% |
Hematuria | 8 | 8.0% |
Crying during Micturition | 14 | 14.0% |
Failure to thrive | 12 | 12.0% |
CBC | Case (n=100) | Control (n=100) | p-value | ||
|---|---|---|---|---|---|
n | % | n | % | ||
<4000/mm3 | 6 | 6.0% | 18 | 18.0% | 0.001 |
4000-11000/mm3 | 41 | 41.0% | 52 | 52.0% | |
>11000/mmm3 | 53 | 53.0% | 30 | 30.0% | |
Laboratory findings | n | % |
|---|---|---|
Urine C/S | ||
Positive | 45 | 45.0% |
Negative | 55 | 55.0% |
Urine R/E (pus cells) | ||
Positive (pus cell >5/HPF) | 90 | 90.0% |
Negative (pus cell ≤5/HPF) | 10 | 10.0% |
Urinary Nitrate | Urine Culture Sensitivity | Total | |
|---|---|---|---|
Culture Positive (n=45) | Control (n=100) | ||
Urinary Nitrate Positive | 34 (TP) | 3 (FP) | 37 |
Urinary Nitrate Negative | 11 (FN) | 97 (TN) | 108 |
Urinary Leukocyte Esterase | Urine Culture Sensitivity | Total | |
|---|---|---|---|
Culture Positive (n=45) | Control (n=100) | ||
Urinary Leukocyte Esterase Positive | 40 (TP) | 18 (FP) | 58 |
Urinary Leukocyte Esterase Negative | 5 (FN) | 82 (TN) | 87 |
Urinary Nitrate | Urinary R/E sensitivity | Total | |
|---|---|---|---|
R/E pus cell >5/HPF (n=90) | Control (n=100) | ||
Urinary Nitrate Positive | 43 (TP) | 3 (FP) | 46 |
Urinary Nitrate Negative | 47 (FN) | 97 (TN) | 144 |
Urinary Leukocyte Esterase | Urine Culture Sensitivity | Total | |
|---|---|---|---|
R/E pus cell >5/HPF (n=90) | Control (n=100) | ||
Urinary Leukocyte Esterase Positive | 78 (TP) | 18 (FP) | 96 |
Urinary Leukocyte Esterase Negative | 12 (FN) | 82 (TN) | 94 |
UTI | Urinary Tract Infections |
PPV | Positive Predictive Value |
NPV | Negative Predictive Value |
| [1] | Sharmin LS, Haque MA, Begum F, Parvez AKS, Uddin MB. Bacteriological Profile and Antimicrobial Sensitivity Pattern of Urinary Tract Infection in a Tertiary Care Hospital of Bangladesh. TAJ: Journal of Teachers Association. 2020 Dec 31; 33(2): 27–31. |
| [2] | Yasmeen BN, Islam S, Islam S, Uddin MM, Jahan R. Prevalence of urinary tract infection, its causative agents and antibiotic sensitivity pattern : A study in Northern International Medical College Hospital, Dhaka. Northern International Medical College Journal. 2015 Nov 16; 7(1): 105–9. |
| [3] | Bhat RG, Katy TA, Place FC. Pediatric Urinary Tract Infections. Emergency Medicine Clinics of North America. 2011 Aug 1; 29(3): 637–53. |
| [4] | Sinha MD, Postlethwaite RJ. Urinary tract infections and the long-term risk of hypertension. Current Paediatrics. 2003 Dec 1; 13(7): 508–12. |
| [5] | Robino L, Scavone P, Araujo L, Algorta G, Zunino P, Pírez MC, et al. Intracellular Bacteria in the Pathogenesis of Escherichia coli Urinary Tract Infection in Children. Clinical Infectious Diseases. 2014 Dec 1; 59(11): e158–64. |
| [6] | Burall LS, Harro JM, Li X, Lockatell CV, Himpsl SD, Hebel JR, et al. Proteus mirabilis Genes That Contribute to Pathogenesis of Urinary Tract Infection: Identification of 25 Signature-Tagged Mutants Attenuated at Least 100-Fold. Infection and Immunity. 2004 May; 72(5): 2922–38. |
| [7] | Nielubowicz GR, Mobley HLT. Host–pathogen interactions in urinary tract infection. Nat Rev Urol. 2010 Aug; 7(8): 430–41. |
| [8] | Mollick S, Dasgupta T, Hasnain MJ, Ahmed M. Isolation and Characterization of Pathogens Responsible for Urinary Tract Infection in Bangladesh and Determination of their Antibiotic Susceptibility Pattern. J App Pharm Sci. 2016 Apr 30; 6,(4): 072–6. |
| [9] | Ferdaus J, Moinuddin G, Islam MT, Rashid MHO, Shawly MR, Alim A. Risk Factors of urinary tract infection in preschool children in Dhaka, Bangladesh. Bangladesh Medical Journal. 2016; 45(3): 134–7. |
| [10] | Sultana S, Khatun M, Ali MK, Mawla N, Akhter N. Pattern of antibiotic sensitivity of bacteria causing urinary tract infection in a private medical college hospital in Dhaka. Bangladesh Journal of Medical Science. 2015 Jan 10; 14(1): 70–4. |
| [11] | Huda N, Nabonee MA, Yusuf MA, Hossain M, Sabiha K. Diagnostic Value of Dipstick Test (Leukocyte Esterase and Nitrite) in Diagnosis of Urinary Tract Infection. Bangladesh Journal of Medical Microbiology. 2023 Dec 10; 17(2): 55–9. |
| [12] | Appenheimer AB, Ford B. Urine Dipstick: Urinary Nitrites and Leukocyte Esterase – Dipping into Murky Waters. In: Sharp VJA, Antes LM, Sanders ML, Lockwood GM, editors. Urine Tests: A Case-Based Guide to Clinical Evaluation and Application [Internet]. Cham: Springer International Publishing; 2020 [cited 2024 Oct 9]. p. 97–115. Available from: |
| [13] | Taneja N, Chatterjee SS, Singh M, Sivapriya S, Sharma M, Sharma SK. Validity of quantitative unspun urine microscopy, dipstick test leucocyte esterase and nitrite tests in rapidly diagnosing urinary tract infections. J Assoc Physicians India. 2010 Aug; 58: 485–7. |
| [14] | Suresh J, Krishnamurthy S, Mandal J, Mondal N, Sivamurukan P. Diagnostic Accuracy of Point-of-care Nitrite and Leukocyte Esterase Dipstick Test for the Screening of Pediatric Urinary Tract Infections. Saudi Journal of Kidney Diseases and Transplantation. 2021 Jun; 32(3): 703. |
| [15] | Williams GJ, Macaskill P, Chan SF, Turner RM, Hodson E, Craig JC. Absolute and relative accuracy of rapid urine tests for urinary tract infection in children: a meta-analysis. The Lancet Infectious Diseases. 2010 Apr 1; 10(4): 240–50. |
| [16] | Koeijers JJ, Kessels AGH, Nys S, Bartelds A, Donker G, Stobberingh EE, et al. Evaluation of the Nitrite and Leukocyte Esterase Activity Tests for the Diagnosis of Acute Symptomatic Urinary Tract Infection in Men. Clinical Infectious Diseases. 2007 Oct 1; 45(7): 894–6. |
| [17] | Forster CS, Haslam DB, Jackson E, Goldstein SL. Utility of a routine urinalysis in children who require clean intermittent catheterization. Journal of Pediatric Urology. 2017 Oct 1; 13(5): 488.e1-488.e5. |
| [18] | Das R, Ahmed T, Saha H, Shahrin L, Afroze F, Shahid ASMSB, et al. Clinical risk factors, bacterial aetiology, and outcome of urinary tract infection in children hospitalized with diarrhoea in Bangladesh. Epidemiology & Infection. 2017 Apr; 145(5): 1018–24. |
| [19] | Nava MO, Mirzaei N, Ebrahimian V, Molaei M, Tohidnia F, Pursafar M. Diagnostic Value of Leukocyte esterase and Nitrite Tests for the Detection of Urinary TractInfection. Biomedical and Pharmacology Journal. 2015 Apr 26; 5(2): 257–60. |
| [20] | Faruk O, Hasan SE, Jubayer A, Akter K, Shiam SAA, Rahman K, et al. Microbial Isolates from Urinary Tract Infection and their Antibiotic Resistance Pattern in Dhaka city of Bangladesh. Journal of Knowledge Learning and Science Technology ISSN: 2959-6386 (online). 2023 Dec 20; 2(3): 76–87. |
| [21] | Shaikh N, Morone NE, Bost JE, Farrell MH. Prevalence of Urinary Tract Infection in Childhood: A Meta-Analysis. The Pediatric Infectious Disease Journal. 2008 Apr; 27(4): 302. |
| [22] | Clark AW, Durkin M, Olsen MA, Keller MR, Ma Y, Butler AM. 241. Rural-urban differences in antibiotic prescribing for uncomplicated urinary tract infections. Open Forum Infectious Diseases. 2020 Oct 1; 7(Supplement_1): S120–1. |
| [23] | Mallick A, Dangwal V, Kumar A. Clinical spectrum of urinary tract infection in children. J Med Allied Sci. 2022; 12(2): 38. |
| [24] | Garrido D, Garrido S, Gutiérrez M, Calvopiña L, Harrison AS, Fuseau M, et al. Clinical characterization and antimicrobial resistance of Escherichia coli in pediatric patients with urinary tract infection at a third level hospital of Quito, Ecuador. Boletín Médico del Hospital Infantil de México. 2017 Jul 1; 74(4): 265–71. |
| [25] | Ayazi P, Mahyar A, Daneshi MM, Jahani Hashemi H, Pirouzi M, Esmailzadehha N. Diagnostic Accuracy of the Quantitative C-Reactive Protein, Erythrocyte Sedimentation Rate and White Blood Cell Count in Urinary Tract Infections among Infants and Children. Malays J Med Sci. 2013 Oct; 20(5): 40–6. |
| [26] | Baral R, Nepal SK. Rapid Nitrite Dip Stick Vs Urine culture for diagnosis of Urinary tract Infections (UTI): Laboratory prospective. International journal of biomedical research [Internet]. 2017 [cited 2024 Oct 26]; Available from: |
| [27] | Eldaif WEAEWAH. SENSITIVITY AND SPECIFICITY OF NITRATE REDUCTASE AND LEUCOCYTES ESTERASE AS RAPID SCREENING TESTS FOR DIAGNOSIS URINARY TRACT INFECTIONS. Journal of Biomedical and Pharmaceutical Research [Internet]. 2013 Jun 28 [cited 2024 Oct 9]; Available from: |
| [28] | Arif A, Afzal MF, Hamid H. Diagnostic accuracy of leukocyte esterase in confirmed cases of urinary tract infection in children. Journal of Rawalpindi Medical College [Internet]. 2023 Jan 2 [cited 2024 Oct 12]; 26(4). Available from: |
| [29] | Huysal K, Budak YU, Karaca AU, Aydos M, Kahvecioğlu S, Bulut M, et al. Diagnostic accuracy of UriSed automated urine microscopic sediment analyzer and dipstick parameters in predicting urine culture test results. Biochem Med. 2013 Jun 15; 23(2): 211–7. |
| [30] | Adhikari S, Sapkota S, Poudel P, Regmi RS, Kafle S, Baral S, et al. Comparison of Urine Dipstick Nitrite Test with Urine Culture in the Diagnosis of Urinary Tract Infection. Journal of College of Medical Sciences-Nepal. 2021 Dec 31; 17(4): 331–40. |
| [31] | Yuen SF, Ng FN, So LY. Evaluation of the accuracy of leukocyte esterase testing to detect pyuria in young febrile children: prospective study. Hong Kong Med J. 2001 Mar; 7(1): 5–8. |
| [32] | Watson JR, Hains DS, Cohen DM, Spencer JD, Kline JM, Yin H, et al. Evaluation of novel urinary tract infection biomarkers in children. Pediatr Res. 2016 Jun; 79(6): 934–9. |
APA Style
Sultana, A., Jui, F. A., Sonia, U. Q., Thakur, M., Jesmine, J., et al. (2024). Diagnostic Role of Urinary Nitrites and Leukocyte Esterase in Detection of UTI in Children. American Journal of Pediatrics, 10(4), 206-214. https://doi.org/10.11648/j.ajp.20241004.18
ACS Style
Sultana, A.; Jui, F. A.; Sonia, U. Q.; Thakur, M.; Jesmine, J., et al. Diagnostic Role of Urinary Nitrites and Leukocyte Esterase in Detection of UTI in Children. Am. J. Pediatr. 2024, 10(4), 206-214. doi: 10.11648/j.ajp.20241004.18
AMA Style
Sultana A, Jui FA, Sonia UQ, Thakur M, Jesmine J, et al. Diagnostic Role of Urinary Nitrites and Leukocyte Esterase in Detection of UTI in Children. Am J Pediatr. 2024;10(4):206-214. doi: 10.11648/j.ajp.20241004.18
@article{10.11648/j.ajp.20241004.18,
author = {Ajmiri Sultana and Farjana Afroze Jui and Umme Qulsum Sonia and Mukta Thakur and Jakiya Jesmine and Syed Ali Imam and M. A. Rouf and Md. Al-Amin Mridha},
title = {Diagnostic Role of Urinary Nitrites and Leukocyte Esterase in Detection of UTI in Children
},
journal = {American Journal of Pediatrics},
volume = {10},
number = {4},
pages = {206-214},
doi = {10.11648/j.ajp.20241004.18},
url = {https://doi.org/10.11648/j.ajp.20241004.18},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20241004.18},
abstract = {Background: Urinary tract infections (UTI) are common in children and pose a significant public health concern, particularly in low-resource settings like Bangladesh. Rapid, cost-effective diagnostic tools such as urinary nitrite and leukocyte esterase dipstick tests offer an alternative to traditional urine culture, which is often time-consuming and resource-intensive. This study aimed to evaluate the diagnostic accuracy of urinary nitrite and leukocyte esterase tests in detecting UTI in children. Methods: This cross-sectional study was conducted at Shaheed Suhrawardy Medical College Hospital, Dhaka, Bangladesh, from July 2019 to December 2019. A total of 200 children, including 100 cases with proven UTI by culture or microscopy and 100 controls, were enrolled. Urinary nitrite and leukocyte esterase tests were performed on urine samples, with urine culture used as the gold standard. Sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) were calculated to assess diagnostic performance. Results: The urinary nitrite test demonstrated a sensitivity of 75.56% and a specificity of 97.00%, with an overall accuracy of 90.34%. The PPV was 91.89%, and the NPV was 89.81%. The leukocyte esterase test showed a sensitivity of 88.89% and a specificity of 82.00%, with an accuracy of 84.14%, PPV of 68.97%, and NPV of 94.25%. Compared with urine R/E, the urinary nitrate test had strong specificity (97.00%) but moderate sensitivity (47.78%), while the leukocyte esterase test maintained high sensitivity (86.67%) and reliable NPV (87.23%). Conclusion: Both urinary nitrite and leukocyte esterase dipstick tests are effective rapid screening tools for diagnosing UTI in children, with high specificity and sensitivity, respectively. Their combined use can enhance diagnostic accuracy, particularly in settings where access to culture testing is limited. These findings support the implementation of dipstick tests as a reliable first-line diagnostic method for pediatric UTI.
},
year = {2024}
}
TY - JOUR T1 - Diagnostic Role of Urinary Nitrites and Leukocyte Esterase in Detection of UTI in Children AU - Ajmiri Sultana AU - Farjana Afroze Jui AU - Umme Qulsum Sonia AU - Mukta Thakur AU - Jakiya Jesmine AU - Syed Ali Imam AU - M. A. Rouf AU - Md. Al-Amin Mridha Y1 - 2024/12/16 PY - 2024 N1 - https://doi.org/10.11648/j.ajp.20241004.18 DO - 10.11648/j.ajp.20241004.18 T2 - American Journal of Pediatrics JF - American Journal of Pediatrics JO - American Journal of Pediatrics SP - 206 EP - 214 PB - Science Publishing Group SN - 2472-0909 UR - https://doi.org/10.11648/j.ajp.20241004.18 AB - Background: Urinary tract infections (UTI) are common in children and pose a significant public health concern, particularly in low-resource settings like Bangladesh. Rapid, cost-effective diagnostic tools such as urinary nitrite and leukocyte esterase dipstick tests offer an alternative to traditional urine culture, which is often time-consuming and resource-intensive. This study aimed to evaluate the diagnostic accuracy of urinary nitrite and leukocyte esterase tests in detecting UTI in children. Methods: This cross-sectional study was conducted at Shaheed Suhrawardy Medical College Hospital, Dhaka, Bangladesh, from July 2019 to December 2019. A total of 200 children, including 100 cases with proven UTI by culture or microscopy and 100 controls, were enrolled. Urinary nitrite and leukocyte esterase tests were performed on urine samples, with urine culture used as the gold standard. Sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) were calculated to assess diagnostic performance. Results: The urinary nitrite test demonstrated a sensitivity of 75.56% and a specificity of 97.00%, with an overall accuracy of 90.34%. The PPV was 91.89%, and the NPV was 89.81%. The leukocyte esterase test showed a sensitivity of 88.89% and a specificity of 82.00%, with an accuracy of 84.14%, PPV of 68.97%, and NPV of 94.25%. Compared with urine R/E, the urinary nitrate test had strong specificity (97.00%) but moderate sensitivity (47.78%), while the leukocyte esterase test maintained high sensitivity (86.67%) and reliable NPV (87.23%). Conclusion: Both urinary nitrite and leukocyte esterase dipstick tests are effective rapid screening tools for diagnosing UTI in children, with high specificity and sensitivity, respectively. Their combined use can enhance diagnostic accuracy, particularly in settings where access to culture testing is limited. These findings support the implementation of dipstick tests as a reliable first-line diagnostic method for pediatric UTI. VL - 10 IS - 4 ER -
Department of Paediatrics, Shaheed Suhrawardy Medical College and Hospital, Dhaka, Bangladesh
Department of Paediatrics, Shaheed Suhrawardy Medical College and Hospital, Dhaka, Bangladesh
Department of Paediatrics, Shaheed Suhrawardy Medical College and Hospital, Dhaka, Bangladesh
Department of Paediatrics, Shaheed Suhrawardy Medical College and Hospital, Dhaka, Bangladesh
Department of Paediatrics, Shaheed Suhrawardy Medical College and Hospital, Dhaka, Bangladesh
Department of Medicine, National Institute of Burn and Plastic Surgery, Dhaka, Bangladesh
Department of Neonatology, Dhaka Medical College Hospital, Dhaka, Bangladesh
Department of Pediatrics, Dr. M R Khan Shishu Hospital and ICH, Mirpur-2, Dhaka, Bangladesh
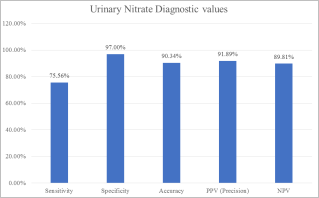
Figure 1. Diagnostic value of urinary nitrate holding culture test as the gold standard.
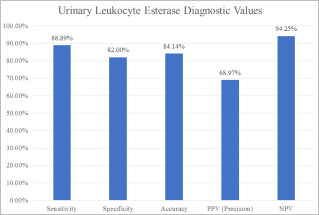
Figure 2. Diagnostic value of urinary leukocyte esterase holding culture test as the gold standard.
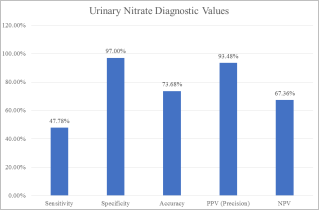
Figure 3. Diagnostic value of urinary nitrate holding urinary R/E as the gold standard.
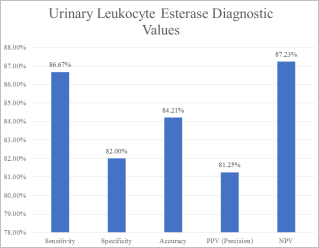
Figure 4. Diagnostic value of urinary leukocyte esterase holding urinary R/E as the gold standard.
Information

