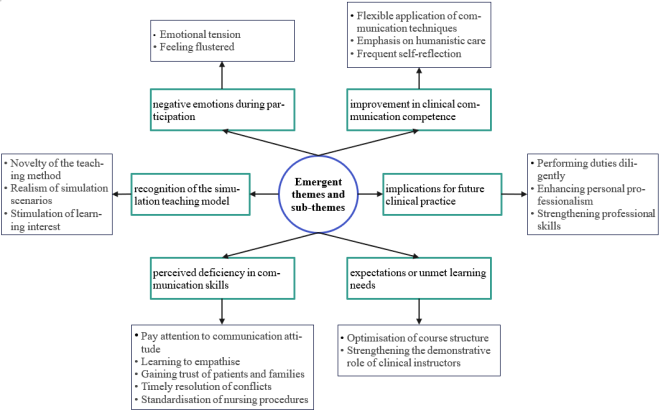
Background: Effective nurse-patient communication is essential for quality care, yet nursing interns often lack practical skills. Simulation-based education is promising, but qualitative research on interns' lived experiences remains limited. Purpose: This study explored the authentic experiences and needs of nursing interns during nurse-patient communication simulation training. Methods: A qualitative descriptive study with a phenomenological approach was conducted. Semi-structured interviews were held with 18 nursing interns from a Chinese university hospital between April and June 2024. Data were analyzed using Colaizzi's seven-step phenomenological method. Results: Six themes emerged: (1) negative emotional experiences during participation; (2) recognition of the Communication Simulation Training model; (3) perceived deficiency in communication skills; (4) improvement in clinical communication competence; (5) implications for future clinical practice; and (6) expectations or unmet learning needs. Participants experienced significant anxiety yet valued the realistic learning environment, recognizing both their communication limitations and growth opportunities. Conclusions: Communication Simulation Training effectively addresses the theory-practice gap in communication skills development. Clinical educators should enhance simulation-based teaching through standardized training management and diversified strategies to improve nursing interns' communication competence and foster higher-quality patient care.
| Published in | American Journal of Nursing Science (Volume 15, Issue 3) |
| DOI | 10.11648/j.ajns.20261503.14 |
| Page(s) | 68-82 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Clinical Communication, Communication Simulation Training, Nurse-Patient Relationship, Nursing Education, Nursing Interns, Qualitative Research
No. | Questions |
|---|---|
1 | What are your views on implementing the nurse-patient Communication Simulation Training model during clinical internship? |
2 | What were your thoughts and experiences during the simulation? |
3 | What did you gain from the nurse-patient communication simulation? |
4 | Which aspects do you think you performed well in, and which areas still need improvement? |
5 | What impact does this have on your future clinical practice? |
6 | Do you have any needs or suggestions regarding this teaching method or clinical instructors? |
Participant ID | gender | Age (years) | Educational Background |
|---|---|---|---|
C1 | Female | 21 | Junior College |
C2 | Female | 20 | Junior College |
C3 | Female | 22 | Junior College |
C4 | Female | 21 | Junior College |
C5 | Female | 20 | Bachelor's Degree |
C6 | Female | 21 | Bachelor's Degree |
C7 | Female | 22 | Junior College |
C8 | Female | 21 | Junior College |
C9 | Female | 21 | Junior College |
C10 | Female | 20 | Junior College |
C11 | Female | 20 | Junior College |
C12 | Female | 21 | Junior College |
C13 | Female | 21 | Junior College |
C14 | Female | 22 | Bachelor's Degree |
C15 | Female | 22 | Junior College |
C16 | Female | 21 | Junior College |
C17 | Female | 20 | Junior College |
C18 | Female | 21 | Junior College |
COREQ | Consolidated Criteria for Reporting Qualitative Research |
DOI | Digital Object Identifier |
ORCID | Open Researcher and Contributor ID |
SBAR | Situation-Background-Assessment-Recommendation |
| [1] | Berglund, L., von Knorring, J., & McGrath, A. (2023). When theory meets reality- a mismatch in communication: A qualitative study of clinical transition from communication skills training to the surgical ward. BMC Medical Education, 23(1), 728. |
| [2] | Chen, T.-T., Huang, Y.-J., Chen, C.-R., Hsu, C.-W., Huang, S.-L., & Hsieh, C.-L. (2025). Effects of feedback and reflection on communication skills training for occupational therapy students. The American Journal of Occupational Therapy: Official Publication of the American Occupational Therapy Association, 79(4), 7904205060. |
| [3] | Chen, Y., Hua, Y., Xu, Z. R., et al. (2020). The correlation between the hospital care atmosphere perception and clinical communication competence of nursing interns. Chinese Journal of Nursing Education, 17(05), 447–450. |
| [4] | Chen, Y. F., Lü, H. Q., Huang, L., et al. (2020). Status and influencing factors of nurse-patient communication competence among vocational nursing interns under a high-quality nursing model. Health Vocational Education, 38(22), 58–60. |
| [5] | Cusanza, S. A., Speroni, K. G., Curran, C. A., & Azizi, D. (2021). Effect of individualized learning plans on nurse learning outcomes and risk mitigation. Journal of Healthcare Risk Management: The Journal of the American Society for Healthcare Risk Management, 40(4), 17–29. |
| [6] | Del Vecchio, A., Moschella, P. C., Lanham, J. G., & Zavertnik, J. E. (2022). Acting to teach communication skills to nurses. The Clinical Teacher, 19(4), 289–293. |
| [7] | Desselle, S. P., Clubbs, B. H., & Darbishire, P. L. (2023). Motivating language and social provisions in the inculcation of pharmacy students’ professional identity. American Journal of Pharmaceutical Education, 87(6), 100010. |
| [8] | Dokoohaki, R., Rambod, M., Pasyar, N., Parviniannasab, A. M., Shaygan, M., Kalyani, M. N., Mohebbi, Z., & Jaberi, A. (2024). Comparison of professional competency and anxiety of nursing students trained based on two internship models: A comparative study. BMC Medical Education, 24(1), 968. |
| [9] | Edmiston, E. A., Hardin, H. K., & Dolansky, M. A. (2023). Making the case for a change in patient education techniques: Moving toward scenario and simulation-based approaches. Clinical Nursing Research, 32(5), 863–864. |
| [10] | Greene, J., & Ramos, C. (2021). A mixed methods examination of health care provider behaviors that build patients’ trust. Patient Education and Counseling, 104(5), 1222–1228. |
| [11] | Guo, Y. J., Guan, X. M., & Xu, T. (2013). The status quo of the caring character of baccalaureate students majoring in nursing and an analysis of the related factors. Chinese Journal of Practical Nursing, 29(5), 70–73. |
| [12] | Günay, U., & Kılınç, G. (2018). The transfer of theoretical knowledge to clinical practice by nursing students and the difficulties they experience: A qualitative study. Nurse Education Today, 65, 81–86. |
| [13] | Haddon Mullins, C., Roderick, A., Deaver, J., & Willig, J. (2020). Contemporary practice of standardised bedside teaching rounds. The Clinical Teacher, 17(5), 483–488. |
| [14] | Hong, X. F., He, J. K., Fu, L. X., et al. (2020). Effect of case study combined with Communication Simulation Training in the cultivation of doctor-patient communication ability of clinical medical interns. China Higher Medical Education, 286(10), 96–97. |
| [15] | Hu, H. Y., & Shi, T. T. (2021). The effect of standardized patient-based Communication Simulation Training teaching on nursing students’ communication and empathy skills. Health Vocational Education, 39(20), 99–101. |
| [16] | Jallad, S. T. (2025). Effectiveness of simulation-based education on educational practices of communication skills, satisfaction, and self-confidence among undergraduate nursing students. Creative Nursing, 31(2), 135–143. |
| [17] | Jin, J., & Zhang, Y. (2021). Evaluation of the effect of Communication Simulation Training teaching under OSCE-guided feedback in obstetric nursing education. China Higher Medical Education, 2021(01), 93–94. |
| [18] | Joolaee, S., Ashghali Farahani, M., Jafarian Amiri, S. R., & Varaei, S. (2016). Support in clinical settings as perceived by nursing students in Iran: A qualitative study. Nursing and Midwifery Studies, 5(1), e31292. |
| [19] | Kong, D. H., Yin, G., Feng, D. X., et al. (2021). The effect of outpatient practice teaching on interns' doctor-patient communication ability. China Higher Medical Education, 2021(09), 80–81. |
| [20] | Kuo, Y. L., Lee, J. T., & Yeh, M. Y. (2021). Intergenerational narrative learning to bridge the generation gap in humanistic care nursing education. Healthcare, 9(10), 1291. |
| [21] | Li, J., Li, X., Gu, L., Zhang, R., Zhao, R., Cai, Q., Lu, Y., Wang, H., Meng, Q., & Wei, H. (2019). Effects of simulation-based deliberate practice on nursing students’ communication, empathy, and self-efficacy. Journal of Nursing Education, 58(12), 681–689. |
| [22] | Li, M. Z. (2016). The application of the CICARE communication model between nurses and patients during the visiting period in the ICU [Master’s thesis, Nanhua University]. Nanhua University Institutional Repository. |
| [23] | Lincoln, Y. S., & Guba, E. (1985). Naturalistic inquiry. SAGE Publications Ltd. |
| [24] | Mei, Y. (2022). Application of the clinical case teaching mode in gynecological nursing teaching. Computational and Mathematical Methods in Medicine, 2022, 9739313. |
| [25] | Myers, K., & Chou, C. L. (2016). Collaborative and bidirectional feedback between students and clinical preceptors: Promoting effective communication skills on health care teams. Journal of Midwifery and Women’s Health, 61(S1), 22–27. |
| [26] | Nasrin, H., Soroor, P., & Soodabeh, J. (2012). Nursing challenges in motivating nursing students through clinical education: A grounded theory study. Nursing Research and Practice, 2012, 161359. |
| [27] | Ogunbiyi, M. O., & Obiri-Darko, E. (2020). Medical students’ corner: Barriers to communication during the COVID-19 pandemic. JMIR Medical Education, 6(2), e24989. |
| [28] | Padilha, J. M., Machado, P. P., Ribeiro, A., Ramos, J., & Costa, P. (2019). Clinical virtual simulation in nursing education: Randomized controlled trial. Journal of Medical Internet Research, 21(3), e11529. |
| [29] | Pan, F., Song, Z. L., & Shen, J. (2022). Application of interactive communication mode combined with problem-based learning in clinical teaching of undergraduate nursing students. Chinese Journal of Practical Nursing, 38(02), 140–146. |
| [30] | Park, J. E., & Kim, J. H. (2021). Nursing students' experiences of psychological safety in simulation education: A qualitative study. Nurse Education in Practice, 55, 103163. |
| [31] | Paterson, C., Paterson, N., Jackson, W., & Work, F. (2020). What are students’ needs and preferences for academic feedback in higher education? A systematic review. Nurse Education Today, 85, 104236. |
| [32] | Rock, L. K. (2021). Communication as a high-stakes clinical skill: “just-in-time” simulation and vicarious observational learning to promote patient- and family-centered care and to improve trainee skill. Academic Medicine: Journal of the Association of American Medical Colleges, 96(11), 1534–1539. |
| [33] | Saragih, I. D., Tarihoran, D. E. T. A. U., Lin, W.-T., & Lee, B.-O. (2024). Outcomes of scenario-based simulation courses in nursing education: A systematic review and meta-analysis. Nurse Education Today, 136, 106145. |
| [34] | Sharkiya, S. H. (2023). Quality communication can improve patient-centred health outcomes among older patients: A rapid review. BMC Health Services Research, 23(1), 886. |
| [35] | Smith, M. B., Macieira, T. G. R., Bumbach, M. D., Garbutt, S. J., Citty, S. W., Stephen, A., Ansell, M., Glover, T. L., & Keenan, G. (2018). The use of simulation to teach nursing students and clinicians palliative care and end-of-life communication: A systematic review. The American Journal of Hospice & Palliative Care, 35(8), 1140–1154. |
| [36] | Solli, H., Haukedal, T. A., Husebø, S. E., & Reierson, I. Å. (2020). The art of balancing: The facilitator’s role in briefing in simulation-based learning from the perspective of nursing students - a qualitative study. BMC Nursing, 19, 99. |
| [37] | Tong, A., P. Sainsbury, and J. Craig. 2007. “Consolidated Criteria for Reporting Qualitative Research (COREQ): A 32-Item Checklist for Interviews and Focus Groups.” International Journal for Quality in Health Care 19, no. 6: 349–357. |
| [38] | Wang, W., & Zhu, L. X. (2021). Research on special training of doctor-patient communication based on practical teaching in emergency environments. Chinese Journal of Medical Education Research, 20(05), 565–569. |
| [39] | Wang, Y., Zhang, Y., Liu, M., Zhou, L., Zhang, J., Tao, H., & Li, X. (2020). Research on the formation of humanistic care ability in nursing students: A structural equation approach. Nurse Education Today, 86, 104315. |
| [40] | Xie, J., Ding, S., Wang, C., & Liu, A. (2013). An evaluation of nursing students' communication ability during practical clinical training. Nurse Education Today, 33(8), 823–827. |
| [41] | Xu, S. L., Ding, C. Y., & Mao, J. (2021). A qualitative study on undergraduate nursing students' willingness for nurse-patient communication during internships based on Push-Pull Theory. Health Vocational Education, 39(17), 113–115. |
| [42] | Yang, L., Li, S. N., Wang, Q., Pan, S., & Zhao, W. (2025). Unveiling the relationships of professional identity, values and communication competence in nursing students’ clinical practice behaviours: A cross-sectional study and mediation model analysis. Nursing Open, 12(7), e70270. |
| [43] | Zhang, J., Yuan, Y., & Hu, L. Y. (2019). Research progress on training of clinical communication ability among nursing interns. Chinese Journal of Modern Nursing, 25(15), 1973–1977. |
| [44] | Zhu, X., Rask, M., & Xu, H. (2023). First year nursing students’ reflections about developing their verbal nursing skills during their nursing education in China: A qualitative study. Frontiers in Public Health, 11, 1149512. |
APA Style
Song, Y., Lai, H., Wu, G., Feng, M., Lin, Q., et al. (2026). Experiences and Needs of Nursing Interns in Nurse-Patient Communication Simulation Training: A Qualitative Study. American Journal of Nursing Science, 15(3), 68-82. https://doi.org/10.11648/j.ajns.20261503.14
ACS Style
Song, Y.; Lai, H.; Wu, G.; Feng, M.; Lin, Q., et al. Experiences and Needs of Nursing Interns in Nurse-Patient Communication Simulation Training: A Qualitative Study. Am. J. Nurs. Sci. 2026, 15(3), 68-82. doi: 10.11648/j.ajns.20261503.14
@article{10.11648/j.ajns.20261503.14,
author = {Yuying Song and Huixiang Lai and Guihong Wu and Mei Feng and Qingran Lin and Manli Liu},
title = {Experiences and Needs of Nursing Interns in Nurse-Patient Communication Simulation Training: A Qualitative Study},
journal = {American Journal of Nursing Science},
volume = {15},
number = {3},
pages = {68-82},
doi = {10.11648/j.ajns.20261503.14},
url = {https://doi.org/10.11648/j.ajns.20261503.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajns.20261503.14},
abstract = {Background: Effective nurse-patient communication is essential for quality care, yet nursing interns often lack practical skills. Simulation-based education is promising, but qualitative research on interns' lived experiences remains limited. Purpose: This study explored the authentic experiences and needs of nursing interns during nurse-patient communication simulation training. Methods: A qualitative descriptive study with a phenomenological approach was conducted. Semi-structured interviews were held with 18 nursing interns from a Chinese university hospital between April and June 2024. Data were analyzed using Colaizzi's seven-step phenomenological method. Results: Six themes emerged: (1) negative emotional experiences during participation; (2) recognition of the Communication Simulation Training model; (3) perceived deficiency in communication skills; (4) improvement in clinical communication competence; (5) implications for future clinical practice; and (6) expectations or unmet learning needs. Participants experienced significant anxiety yet valued the realistic learning environment, recognizing both their communication limitations and growth opportunities. Conclusions: Communication Simulation Training effectively addresses the theory-practice gap in communication skills development. Clinical educators should enhance simulation-based teaching through standardized training management and diversified strategies to improve nursing interns' communication competence and foster higher-quality patient care.},
year = {2026}
}
TY - JOUR T1 - Experiences and Needs of Nursing Interns in Nurse-Patient Communication Simulation Training: A Qualitative Study AU - Yuying Song AU - Huixiang Lai AU - Guihong Wu AU - Mei Feng AU - Qingran Lin AU - Manli Liu Y1 - 2026/06/26 PY - 2026 N1 - https://doi.org/10.11648/j.ajns.20261503.14 DO - 10.11648/j.ajns.20261503.14 T2 - American Journal of Nursing Science JF - American Journal of Nursing Science JO - American Journal of Nursing Science SP - 68 EP - 82 PB - Science Publishing Group SN - 2328-5753 UR - https://doi.org/10.11648/j.ajns.20261503.14 AB - Background: Effective nurse-patient communication is essential for quality care, yet nursing interns often lack practical skills. Simulation-based education is promising, but qualitative research on interns' lived experiences remains limited. Purpose: This study explored the authentic experiences and needs of nursing interns during nurse-patient communication simulation training. Methods: A qualitative descriptive study with a phenomenological approach was conducted. Semi-structured interviews were held with 18 nursing interns from a Chinese university hospital between April and June 2024. Data were analyzed using Colaizzi's seven-step phenomenological method. Results: Six themes emerged: (1) negative emotional experiences during participation; (2) recognition of the Communication Simulation Training model; (3) perceived deficiency in communication skills; (4) improvement in clinical communication competence; (5) implications for future clinical practice; and (6) expectations or unmet learning needs. Participants experienced significant anxiety yet valued the realistic learning environment, recognizing both their communication limitations and growth opportunities. Conclusions: Communication Simulation Training effectively addresses the theory-practice gap in communication skills development. Clinical educators should enhance simulation-based teaching through standardized training management and diversified strategies to improve nursing interns' communication competence and foster higher-quality patient care. VL - 15 IS - 3 ER -
School of Nursing, Jinan University, Guangzhou, China
Research Fields: Nursing education, Qualitative research
School of Nursing, Jinan University, Guangzhou, China
Research Fields: Nursing education, Clinical communication
Gastrointestinal Surgery, The First Affiliated Hospital of Jinan University, Guangzhou, China
Research Fields: Nursing education, Communication skills training
Gastrointestinal Surgery, The First Affiliated Hospital of Jinan University, Guangzhou, China
Research Fields: Nursing informatics, Data analysis
Information