Abstract
Connective tissue disorders (CTDs) are associated with the production of multiple autoantibodies, predominantly anti-nuclear antibodies (ANA) and their subsets known as extractable nuclear antigens (ENA). Although ANA detection by indirect immunofluorescence (IIF) and enzyme-linked immunosorbent assay (ELISA) is routinely used for screening CTDs, these methods are limited by non-specificity. The present study evaluated the clinical utility of ENA profiling in conjunction with conventional ANA testing for CTD screening. Clinically suspected CTD patients were screened for ANA using ELISA and IIF, followed by ENA antibody detection using ELISA and line blot immunoassay (LIA). Out of a total of 274 clinically suspected cases analyzed, ANA positivity was observed in 23.7% of cases by indirect immunofluorescence and 26.2% by enzyme-linked immunosorbent assay. ENA analysis among ANA-positive cases revealed systemic lupus erythematosus (SLE) as the most prevalent CTD (68%), while Sjögren’s syndrome was the least common (1%). Among ENA specificities, U-RNP antibodies showed the highest frequency (56.9%), whereas PM-Scl antibodies were least frequent (1%). Although IIF remains the gold standard for ANA detection, ELISA is a useful initial screening tool, as IIF may fail to detect low-positive ANA cases identified by ELISA. Interpretation of ANA positivity should always be made in appropriate clinical context and confirmed by more specific tests such as ENA profiling. The observed geographical variation in ENA antibody frequency and CTD patterns highlights the need for further region-specific studies to better define antibody prevalence in CTDs.
1. Introduction
Connective Tissue Disorders (CTDs) area type of chronic autoimmune inflammations referring to a group of diseases involving many systems. These are more prevalent in the Western countries, but incident rates, in past few years, appear to rise in both Western and Asian countries
. Improvement in control of infections, industrialization and consequently environmental changes are responsible for increase of CTDs in the developing countries like India
| [2] | Minz RW, Kumar Y, Anand S, Singh S, Bamberi P, Verma S, et al. Antinuclear antibody positive autoimmune disorders in North India: an appraisal. Rheumatology International. 2012; 32(9): 2883-2888.
https://doi.org/10.1007/s00296-011-2073-4 |
[2]
. The low socio-economic status of South-East Asia including India may be the reason for higher morbidity and mortality of CTDs when compared to the developed countries
.
The most common CTDs are: (a) Systemic Lupus Erythromatosus (SLE), (b) Systemic Sclerosis (SSc), (c) Siogren’s Syndrome, (d) Polymyositis Dermatomyositis (PM DM), (e) Mixed connective tissue. Systemic Lupus Erythromatosus (SLE) is seen as the most common subtype of CTD with widespread inflammation and tissue damage affecting multiple organs. In autoimmune CTDs, the immune system produces antibodies to cells. It has been claimed that antibodies can penetrate the living cells and react directly with the nucleus
| [4] | Gunnarsson R, Molberg Ø, Gilboe IM, Gran JT. The prevalence and incidence of mixed connective tissue disease. Annals of the Rheumatic Diseases. 2011; 70(6): 1047-1051.
https://doi.org/10.1136/ard.2010.143792 |
[4]
. So, these antinuclear antibodies (ANA) are autoantibodies to the nuclei of cells which constitute the basis for diagnosis and treatment of CTDs
| [5] | Kumar Y, Bhatia A, Minz R. Antinuclear antibodies and their detection methods in diagnosis of connective tissue diseases. Diagnostic Pathology. 2009; 4: 1.
https://doi.org/10.1186/1746-1596-4-1 |
[5]
.
There are various types of ANAs: (a) Autoantibodies to DNA and histone and b) Autoantibodies to Extractable Nuclear Antigen (ENA), a subset of ANA. The antigens were named ENA originally, as they were extracted from the nuclei of the cells. These are smith (Sm) which was detected first in 1966 and others are Ro, La, Jo, SS A, SS B, SCL 70, Rib PP, nucleosome, U-RNP
| [6] | Tan EM, Kunkel HG. Characteristics of a soluble nuclear antigen precipitating with sera of patients with systemic lupus erythematosus. Journal of Immunology. 1966; 96(3): 464-471. |
[6]
. To diagnose a case of CTD, ANA test is mandatory followed by ENA study (if ANA comes out to be positive). Anti-nuclear antibodies (ANA) are commonly detected using indirect immunofluorescence (IIF) and enzyme-linked immunosorbent assay (ELISA), a plate-based immunoassay that detects antigen-antibody interactions through enzyme-mediated colorimetric reactions. Further, IIF is accepted as gold standard for ANA because it picks up the auto antigens in patients which may have been missed by the ELISA
| [7] | Tozzoli R, Bizzaro N, Tonutti E, Villalta D, Bassetti D, Manoni F, et al. Guidelines for the laboratory use of autoantibody tests. American Journal of Clinical Pathology. 2002; 117(2): 316-324. https://doi.org/10.1309/Y5D3-8D7F-1C4M-MU0K |
[7]
. Subsequently anti ENA tests are advised those having ANA positive. Anti ENA test is mostly done by ELISA (having 6 Antigens) or by Line Immuno Assay (LIA) technique. Simultaneously anti ds DNA is being preferably done through IIF or ELISA procedure if SLE is suspected
. Consequently, the test for CTD are in 2 stages: First is the ANA screening tests (through IIF or ELISA) followed by confirmatory Anti ENA and Anti dsDNA test as necessary.
Lack of epidemiological data and advanced diagnostic facilities lead to under diagnosis of CTD cases. Keeping in view of the present scenario, the study was undertaken in Odisha (an eastern state of India) with aim and objective to know the prevalence of CTDs in this region by ANA & ENA profile and to help the clinicians in better understanding of the disease. At present most of the clinicians depend upon the ANA estimation rather than going for both. Hence, in this study we emphasize on the estimation of both ANA as well as ENA profile for better diagnosis, prognosis and monitoring the diseases.
2. Materials and Methods
2.1. Clinical Evaluation and Sample Collection
Ethical permission was obtained in accordance with the guidelines of Institutional Ethical Committee and the study was conducted at SCB Medical College, Cuttack (a premier institute of eastern Indian state of Odisha).
Blood samples were collected from 274 clinically suspected cases of various CTDs coming to SCB Medical College, Cuttack. Some non CTD and healthy individuals from the community having no chronic disease or any significant past history were taken as control. Clinical details of the patients were obtained from the patient case files and questionnaires used to interview patients and collect relevant data.
2.2. Inclusion Criteria
The suspected cases of CTDs having the signs and symptoms like unexplained prolonged fever, arthritis, anemia, skin rash, alopecia, pleuro pericarditis, muscle weakness, dryness of eye and mouth, puffiness of face and anasarca were taken into consideration for testing for ANA.
Exclusion Criteria (Based on earlier studies
| [9] | Kumar TS, Aggarwal A. Approach to a patient with connective tissue disease. Indian Journal of Pediatrics. 2010; 77(10): 1157-1164. https://doi.org/10.1007/s12098-010-0215-4 |
| [10] | Wiik AS, Gordon TP, Kavanaugh AF, Lahita RG, Reeves W, van Venrooij WJ, et al. Cutting edge diagnostics in rheumatology. Arthritis & Rheumatism. 2004; 51(2): 291-298.
https://doi.org/10.1002/art.20245 |
[9, 10]
):
1) Back pain or musculoskeletal pain.
2) Arthritis conditions like Osteoarthritis, sero-negative arthritis.
3) Patient with other co-existing infectious diseases.
4) Chronic inflammatory conditions like - Ulcerative colitis, Sclerosing cholangitis, Felty’s Syndrome and Systemic Vasculitides.
5) Older age group, Pregnant and lactating Women.
2.3. Diagnostic Tests Used for the Evaluation of Connective Tissue Disorders
The diagnosis of connective tissue disorders is based on the detection of autoantibodies against nuclear and cytoplasmic antigens. Anti-nuclear antibody (ANA) testing is the primary screening assay and is routinely performed using indirect immunofluorescence (IIF) on HEp-2 cells and enzyme-linked immunosorbent assay (ELISA). Indirect immunofluorescence provides information on antibody titer and fluorescence pattern, while ELISA serves as a sensitive screening method. In ANA-positive cases, extractable nuclear antigen (ENA) profiling is performed for disease-specific antibody identification using ELISA or line immunoblot assay (LIA). Anti-double-stranded DNA (anti-dsDNA) antibody testing is also commonly used, particularly in suspected systemic lupus erythematosus, due to its diagnostic and prognostic significance. Together, these assays constitute a complementary and stepwise diagnostic approach for connective tissue disorders.
2.4. Evaluation of ANA and ENA Profile
Blood /serum samples were subjected to ANA-ELISA and ANA IIF test to confirm the diagnosis of CTD and subsequently for ENA profile through different techniques to stamp a particular disease.
ANA ELISA was done by automated ELISA processor (BIORAD, USA) using ANA ELISA screening test kits of BIORAD which targets nuclear and cytoplasmic antigens
| [11] | Angel J, Thomas M, Appalaraju B. Evaluation of ELISA and indirect immunofluorescence in autoimmune diseases. Journal of Academic Clinical Microbiology. 2015; 17(1): 7-12. |
[11]
. The color intensity was read by ELISA reader at 450 nm and the values more than 1 were interpreted as positive.
ANA IIF test was carried out using EUROIMMUN kit (Germany) which use Hep 2 cells as substrate antigens
| [12] | Mariz HA, Sato EI, Barbosa SH, Rodrigues SH, Dellavance A, Andrade LEC. Pattern on the ANA-HEp-2 test. Arthritis & Rheumatism. 2011; 63(1): 191-200.
https://doi.org/10.1002/art.30084 |
[12]
. The fluorescent pattern and intensity were evaluated using Leica immunofluorescence microscope for ANA interpretation as per the guidelines of CDC
| [13] | Ghosh P, Dwivedi S, Naik S, Agarwal V, Verma A, Aggarwal A. Antinuclear antibodies by indirect immunofluorescence. Indian Journal of Medical Research. 2007; 126(1): 34-38. |
| [14] | Rigon A, Soda P, Zennaro D, Iannello G, Afeltra A. Indirect immunofluorescence in autoimmune diseases. Cytometry Part B. 2007; 72B (6): 472-477.
https://doi.org/10.1002/cyto.b.20205 |
[13, 14]
.
The ANA positive (by both IIF and ELISA) were taken for testing of antibodies against extractable nuclear antigen (ENA). It was done by 2 methods: (a) ENA ELISA (six profiles), (b) Line Immunoblot Assay (LIA). For ENA ELISA, ANA positive samples were tested for antibodies against six (SSA, SSB, Sm, RNP, Scl 70, Jo-1) antigens using the BIORAD Kit (USA). The test was performed by automated ELISA processor (BIORAD) and the intensity of colour was measured photometrically at 450 nm by Enzyme units (EUs) for each patient
| [15] | Maddison PJ, Skinner RP, Vlachoyiannopoulos P, Brennand DM, Hough D. Antibodies to nRNP, Sm, Ro and La detected by ELISA. Clinical and Experimental Immunology. 1985; 62(2): 337-345. |
[15]
. The value of EU >25 is taken as positive.
For ENA LIA, the ANA positive samples were scrutinized for antibodies against antigens like RNP, Sm, ssA, ssB, Scl-70, PM-Scl, Jo-1, CENP-B, PCNA, dsDNA, nucleosome, histones, ribosomal-P-Protein and AMA-M2 (14 antigens) using EUROIMMUN kit (Germany). In the presence of specific antibodies in the sample, a purple band appeared on the test strips indicating presence of that particular antigen. Based on signal intensity the results were divided as negative, borderline and positive marks.
2.5. Statical Analysis
All the data were analyzed and plotted by using GraphPad-Prism. Spearman’s rank correlation coefficient (ρ) was used to assess correlations, and p-values < 0.05 were considered statistically significant.
3. Results
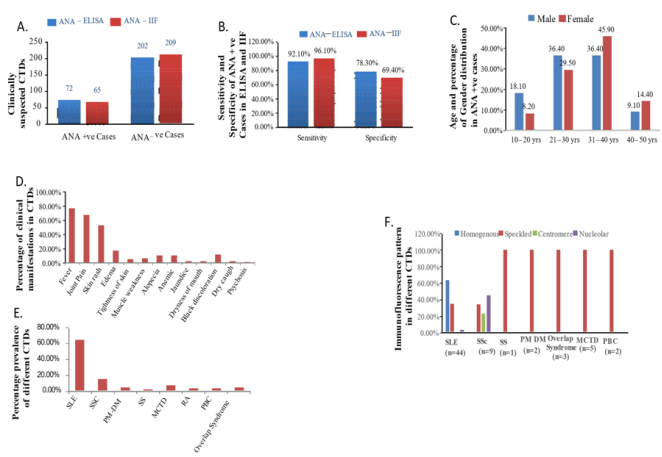
A total of 274 clinically suspected cases were analyzed using indirect immunofluorescence and enzyme-linked immunosorbent assay for anti-nuclear antibody detection. Of these, 65 cases (23.7%) were ANA-positive by indirect immunofluorescence, while 72 cases (26.2%) were positive by enzyme-linked immunosorbent assay (
Figure 1A). Sensitivity of ANA by IIF was 85.5%, while by ELISA it was 94.1% (
Figure 1B). On contrary specificity of ELISA was 70% as compared to 88.3% by IIF method (
Figure 1B). Both ANA-IIF and ANA-ELISA is equally sensitive to determine CTDs.
With the consideration of ANA-positive population, we found the distribution of CTDs more prevalent in middle age (21-40 ages) in both the sexes. Among the ANA-positive cases (n = 72), females showed higher susceptibility (45.9%). Within this ANA-positive population, the overall prevalence was highest in the 31-40 years age group (44.4%) (
Figure 1C). Further, we determined different CTDs using both ANA-ELISA and ANA-IIF test and found SLE as the most predominant form of CTD with fever and joint pain as the major clinical manifestations together with skin rash (
Figure 1D). Among the ANA-positive study population, systemic lupus erythematosus (SLE) was the most prevalent connective tissue disorder (68%), followed by systemic sclerosis (SSc) (15%). The rarest CTD was SS (1%), MCTD and Overlap syndrome (4%) (
Figure 1E).
While checking the pattern formation of different CTDs, we found homogenous pattern exclusively in SLE (42.5%), whereas Speckled pattern (46.9%) is seen in all CTDs. Centromere pattern (3.1%) is exclusively seen in SSc, but nucleolar pattern (7.5%) is mainly observed in SSc and to some extent in SLE (
Figure 1F). So fluorescence pattern except for speckled indicate the type of CTDs present in the sample. The result indicates that the speckled pattern has the highest frequency followed by homogenous pattern. The fluorescence intensity of 3+ was more frequent (53.9%) than that of 2+ (31.6%) in our study (
Figure 1F).
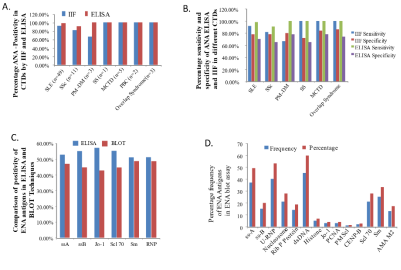
In our study positivity by IIF and ELISA methods were 91.8% and 98% for SLE; 81.8% and 90.9% for SSc; 100% both for SS; 66.7% and 100% for PM-DM; 100% in both for MCTD respectively. As the sample size for SS and PM-DM were less in our study the positivity results were discordant (
Figure 2A).
Comparing the sensitivity and specificity of individual CTDs in both ELISA and IIF methods, no difference was observed in both the technique (
Figure 2B).
Among the ANA-positive cases subjected to ENA profiling by both ELISA and line immunoblot (LIA) method showed prevalence of U-RNP as the highest (56.9%) followed by ss-A as 50%, dsDNA as 43%, Sm as 33.3% and scl70 as 27.7%.
In our study we compared the result of both ELISA and line immunoblot (LIA) method to determine different antigens and found there was no significant (p>0.05) differences between the two methods. The discrepancies ELISA and Blot results for ssA, ssB, Jo-I, scl-70, Sm and RNP were 1.38%, 2.78%, 1.39%, 0%, 1.39%, 1.39% respectively. Positivity of ENA antigens by ELISA method were more than by Blot technique (
Figure 2C).
Figure 1. Diagnostic performance, demographic distribution, clinical manifestations, and immunofluorescence patterns in connective tissue disorders (CTDs).
(A) Percentage of ANA positivity among clinically suspected CTD cases as detected by indirect immunofluorescence (IIF) and enzyme-linked immunosorbent assay (ELISA).
(B) Comparative sensitivity and specificity of ANA detection by IIF and ELISA methods, demonstrating higher sensitivity of ELISA and higher specificity of IIF.
(C) Age-wise and gender-wise distribution of ANA-positive cases, showing predominance in females and higher prevalence in the 31-40 years age group.
(D) Frequency distribution of major clinical manifestations observed in CTD patients, including fever, joint pain, skin rash, muscle weakness, and other systemic features.
(E) Percentage prevalence of different CTDs among ANA-positive cases, highlighting systemic lupus erythematosus (SLE) as the most prevalent disorder, followed by systemic sclerosis (SSc), mixed connective tissue disease (MCTD), overlap syndrome, polymyositis-dermatomyositis (PM-DM), and Sjögren’s syndrome (SS).
(F) Representative immunofluorescence staining patterns observed on HEp-2 cells by ANA-IIF, including homogeneous, speckled, nucleolar, and centromere patterns, illustrating their association with different CTDs and variation in fluorescence intensity.
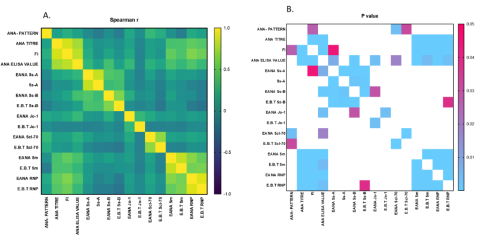
ANA ELISA value can be correlated with Immunofluorescent technique. The ELISA value had a good correlation with ANA titer and Fluorescent Intensity of Immunofluorescent method having Spearman correlation (ρ) 0.7322069 and 0.7990026 respectively. But the ELISA value did not correlate strongly with ANA pattern (ρ is 0.1334729) (
Figure 3A).
Comparing the antigens with both the ELISA and Blot technique there was a good correlation between ssA, Smith (Sm) and RNP antigens as spearman correlation (ρ) are 0.8248888, 0.8176809 and 0.893555048 respectively. Similarly significant correlation was seen in ssB, Jo-1 and Scl70 antigens as ρ value were 0.3625787, 0.331751586 and 0.672515422 respectively (
Figure 3A). After getting an idea of frequencies of different antigens in CTDs, we analyzed ENA specific antigens from different groups of CTDs. Frequency of anti-histone antibody in SLE is 10%, where the cases were associated with drug induced lupus. Similarly anti dsDNA were associated mostly with lupus nephritis, anti ssA and anti ssB with photosensitivity and anti Ribosomal P protein with lupus psychosis. Our study shows specificity of anti-nucleosome, anti Rib P Protein, anti dsDNA, anti PCNA, anti-histone and anti Sm antibody as 100% in SLE. So, these ENA antigens are exclusively seen in SLE suggesting that the presence of these antigens confirm the diagnosis of SLE. The frequencies of anti scl-70 in SSc was 81.8%, whereas anti ssA and anti ssB in SS were both 100%. Anti Jo-1 was again 100% in PM-DM showing 100% sensitivity and specificity. Regarding SS, our study showed the presence of anti ssA to be 80% in SLE, 8.6% in SSc and 3.8% in each of SS, MCTD and overlap syndrome and anti ssB to be 81.8% in SLE, 9.1% in SS and 9.1% in overlap syndrome (
Figure 2D). Both anti ssA and anti ssB though were 100% sensitive, were less specific.
Figure 2. Comparative analysis of ANA positivity, diagnostic accuracy, and ENA antibody profiling in connective tissue disorders (CTDs).
(A) Percentage of ANA positivity across different CTDs as determined by indirect immunofluorescence (IIF) and enzyme-linked immunosorbent assay (ELISA), showing comparable detection rates between the two methods for most CTDs.
(B) Sensitivity and specificity of ANA detection by ELISA and IIF for individual CTDs, indicating no statistically significant difference between the two techniques across disease categories.
(C) Comparison of the frequency of ENA antibody positivity detected by ELISA and line immunoblot assay (LIA), demonstrating slightly higher positivity rates by ELISA with minimal discrepancies between the two methods.
(D) Percentage distribution of individual ENA antibodies detected by line immunoblot assay among ANA-positive CTD cases, highlighting U-RNP as the most frequently detected antibody, followed by SSA/Ro, dsDNA, Sm, and Scl-70, and illustrating disease-specific antibody associations.
Figure 3. Spearman’s rank correlation analysis between ANA detection methods and ENA antibody assays in connective tissue disorders (CTDs).
(A) Correlation of ANA-ELISA values with ANA-IIF parameters showing strong positive correlation with ANA titers (ρ = 0.73) and fluorescence intensity (ρ = 0.80), but weak correlation with immunofluorescence patterns (ρ = 0.13).
(B) Correlation between ENA antibodies detected by ELISA and line immunoblot assay (LIA), demonstrating strong agreement for anti-RNP, anti-SSA/Ro, and anti-Sm, and moderate correlation for anti-SSB/La, anti-Jo-1, and anti-Scl-70.
4. Discussion
CTDs are group of diseases with chronic inflammatory condition in connective tissues. To identify a case of CTD, Anti-Nuclear Antibody (ANA) testing should be done, but to confirm a particular disease among CTDs (subtypes of CTDs) ENA testing is required. Not only the diagnosis, but it also signifies the prognosis of the disease. Presently in most of the cases, diagnoses of different CTDs are being done based on clinical history. The ANA positivity in suspected CTDs (by ANA IIF method) varies from 23.5 to 32.2% as studied by different authors, which is very similar to our study
| [16] | Abeles AM, Abeles M. The clinical utility of a positive ANA test result. The American Journal of Medicine. 2013; 126(4): 342-348. https://doi.org/10.1016/j.amjmed.2012.09.014 |
| [17] | Birtane M, Yavuz S, Taştekin N. Laboratory evaluation in rheumatic diseases. WJM. 2017; 7(1): 1. |
| [18] | Solomon DH, Katz JN, Jacobs JP, La Tourette AM, Coblyn J. Management of glucocorticoid‐induced osteoporosis in patients with rheumatoid arthritis: Rates and predictors of care in an academic rheumatology practice. Arthritis & Rheumatism. 2002 Dec; 46(12): 3136–42.
https://doi.org/10.1002/ART.10613 |
[16-18]
. However, in another study on Indian population much lower percentage of ANA positivity was reported
| [2] | Minz RW, Kumar Y, Anand S, Singh S, Bamberi P, Verma S, et al. Antinuclear antibody positive autoimmune disorders in North India: an appraisal. Rheumatology International. 2012; 32(9): 2883-2888.
https://doi.org/10.1007/s00296-011-2073-4 |
[2]
. It signifies the false positive cases with empirical treatment, leads to unnecessary exposure to drug regimen. Hence laboratory treatment through ANA and ENA profile is required before starting the treatment for CTD.
The sensitivity of ANA-ELISA and ANA-IIF (p value> 0.05) did not have significant difference, whereas the specificity became varied which can be comparable to many other reports
. The prevalence of CTDs in our experiment showed, females were more prone to the disease due to their hormonal make up and the disease is manifested mostly in their third decade of life. The incidence of SLE (68%) is highest and commonest followed by SSc among all CTDs
.
IIF method in CTD diagnosis is a gold standard procedure
| [5] | Kumar Y, Bhatia A, Minz R. Antinuclear antibodies and their detection methods in diagnosis of connective tissue diseases. Diagnostic Pathology. 2009; 4: 1.
https://doi.org/10.1186/1746-1596-4-1 |
[5]
. However, evaluation of fluorescence pattern, intensity and dilution factor of IIF technique makes the study more distinctive. Therefore, pattern analysis study in our experiment revealed that speckled pattern has the highest frequency followed by homogenous pattern which is similar to observation made by some authors
| [12] | Mariz HA, Sato EI, Barbosa SH, Rodrigues SH, Dellavance A, Andrade LEC. Pattern on the ANA-HEp-2 test. Arthritis & Rheumatism. 2011; 63(1): 191-200.
https://doi.org/10.1002/art.30084 |
[12]
. Contrasting observations were also reported by some groups where homogenous being higher than the speckled
| [14] | Rigon A, Soda P, Zennaro D, Iannello G, Afeltra A. Indirect immunofluorescence in autoimmune diseases. Cytometry Part B. 2007; 72B (6): 472-477.
https://doi.org/10.1002/cyto.b.20205 |
| [22] | Roberts‐Thomson PJ, Nikoloutsopoulos T, Cox S, Walker JG, Gordon TP. Antinuclear antibody testing in a regional immunopathology laboratory. Immunol Cell Biol. 2003 Oct; 81(5): 409–12. https://doi.org/10.1046/j.1440-1711.2003.01182.x |
[14, 22]
. Hence the differences observed in our pattern study might be due to the genetic and environmental make up of our eastern Indian population. Also the fluorescence intensity of 3+ was more frequent, which clearly indicates that it was more specific to antibody of 1:100 dilution also reported by Ghose et al
| [13] | Ghosh P, Dwivedi S, Naik S, Agarwal V, Verma A, Aggarwal A. Antinuclear antibodies by indirect immunofluorescence. Indian Journal of Medical Research. 2007; 126(1): 34-38. |
[13]
. Comparing both the technique, ELISA value is more or less correlated with both titer and fluorescent Intensity of IIF method, whereas it does not correlate with ANA pattern of IIF. This is because the pattern has no definite value, rather indicates a range. Consequently, it does not correlate with pattern.
The percentage of SLE and SSc positivity by IIF is comparable to many other studies reported
| [4] | Gunnarsson R, Molberg Ø, Gilboe IM, Gran JT. The prevalence and incidence of mixed connective tissue disease. Annals of the Rheumatic Diseases. 2011; 70(6): 1047-1051.
https://doi.org/10.1136/ard.2010.143792 |
| [20] | Habash-Bseiso DE, Yale SH, Glurich I, Goldberg JW. Serologic testing in connective tissue diseases. Clinical Medicine & Research. 2005; 3(3): 190-193.
https://doi.org/10.3121/cmr.3.3.190 |
| [23] | Satoh M, Vázquez-Del Mercado M, Chan EKL. Clinical interpretation of antinuclear antibody tests in systemic rheumatic diseases. Modern Rheumatology. 2009 Jun; 19(3): 219–28. https://doi.org/10.1007/s10165-009-0155-3 |
[4, 20, 23]
.
However, results of IIF positivity of SS, PM-DM and MCTD are discordant due to very low degree of freedom. When we compared the results of ANA estimation by IIF and ELISA, we find that percentage of SLE and SSc positive samples were almost same, indicates the sensitivity were comparable. But due to small sample size of SS, PM-DM and MCTD comparison will not accountable.
To provide insights into the antigen specific antibody related to CTDs, ANA positive cases were subjected to ENA assay through ELISA and line immunoblot (LIA) methods. A minimal discrepancy (p> 0.05) was observed between ELISA and Blot results for various ENA antibodies like ssA, ssB, Jo-I, scl-70, Sm and RNP.
The antigens in both the technique have either good or significant correlation, hence showing that both the procedures are taken into consideration. But no correlation was found out between different antigens conclude that for a concrete diagnosis all above antigens are important.
The blot technique revealed prevalence of U RNP as the highest followed by ssA, dsDNA, Sm and Nucleosome probably due to SLE patients which predominates among the study group. Unlike some other study, U-RNP is not confined to MCTD, rather seen in good percentage of cases like SLE and Systemic Sclerosis. This may be the reason being the highest frequency antigen among CTDs. As a result, there is an increased frequency of such ENA antigens in CTDs as a whole. The results observed by Von Muhlen CA et al was more or less similar to our study
.
While comparing the frequency of ENA antigens we observed anti-nucleosome, anti-Rib P Protein, anti dsDNA, anti PCNA, anti-histone and anti Sm antibody were exclusively found in SLE. The presence of these antigens confirmed the diagnosis of SLE which is in line with the observations reported by others
| [25] | Hamburger M, Hodes S, Barland P. The incidence and clinical significance of antibodies to extractable nuclear antigens. The American Journal of the Medical Sciences. 1977; 273(1): 21-28. https://doi.org/10.1097/00000441-197701000-00002 |
| [26] | Haddouk S, Marzouk S, Jallouli M, Fourati H, Frigui M, Hmida YBH, et al. Clinical and diagnostic value of ribosomal P autoantibodies in systemic lupus erythematosus. Rheumatology. 2009; 48(8): 953-957.
https://doi.org/10.1093/rheumatology/kep145 |
[25, 26]
. Frequency of anti-histone antibody in SLE is less and exclusively associated with drug induced lupus. Similarly anti dsDNA associated with lupus nephritis, anti ssA and anti ssB with photosensitivity and anti-Ribosomal P Protein with lupus psychosis. These antigens are crucial to access the disease progression, hence determines the prognosis of the disease particularly of SLE.
In the present study different frequency of ENA antigens are seen in different CTDs. In SSc patients, Scl70 is predominant followed by CENP, ssA and ssB but only CENP is exclusively found only in SSc. Similarly Anti Jo-1 is predominant and exclusive to PM-DM, but in our case we also found ssA and U-RNP in PM-DM. U-RNP and AMA-M2 exclusively associated with MCTD and Primary biliary cirrhosis. Ultimately from our observation it can be conclude that Jo-1, U-RNP, ssA/ssB, and AMA/M2 are key molecule to diagnose PM-DM, MCTD, SS, AMA/M2 respectively which is similar to observations made by others
| [25] | Hamburger M, Hodes S, Barland P. The incidence and clinical significance of antibodies to extractable nuclear antigens. The American Journal of the Medical Sciences. 1977; 273(1): 21-28. https://doi.org/10.1097/00000441-197701000-00002 |
| [26] | Haddouk S, Marzouk S, Jallouli M, Fourati H, Frigui M, Hmida YBH, et al. Clinical and diagnostic value of ribosomal P autoantibodies in systemic lupus erythematosus. Rheumatology. 2009; 48(8): 953-957.
https://doi.org/10.1093/rheumatology/kep145 |
| [27] | Dähnrich C, Pares A, Caballeria L, Rosemann A, Schlumberger W, Probst C, et al. New ELISA for detecting primary biliary cirrhosis-specific antimitochondrial antibodies. Clinical Chemistry. 2009; 55(5): 978-985.
https://doi.org/10.1373/clinchem.2008.121053 |
| [28] | Phan TG, Wong RCW, Adelstein S. Autoantibodies to extractable nuclear antigens: making detection and interpretation more meaningful. Clinical and Vaccine Immunology. 2002; 9(1): 1-7. https://doi.org/10.1128/CDLI.9.1.1-7.2002 |
| [29] | Ho KT, Reveille JD. The clinical relevance of autoantibodies in scleroderma. Arthritis Research & Therapy. 2003; 5(2): 80-93. https://doi.org/10.1186/ar628 |
[25-29]
. However, the prevalence of SSc differs from our result to others as we found 45% of patients have antigen other than Scl70
| [28] | Phan TG, Wong RCW, Adelstein S. Autoantibodies to extractable nuclear antigens: making detection and interpretation more meaningful. Clinical and Vaccine Immunology. 2002; 9(1): 1-7. https://doi.org/10.1128/CDLI.9.1.1-7.2002 |
[28]
. Prevalence of CENP in SSc differs as it is much less in our case than the result from other studies
| [28] | Phan TG, Wong RCW, Adelstein S. Autoantibodies to extractable nuclear antigens: making detection and interpretation more meaningful. Clinical and Vaccine Immunology. 2002; 9(1): 1-7. https://doi.org/10.1128/CDLI.9.1.1-7.2002 |
| [29] | Ho KT, Reveille JD. The clinical relevance of autoantibodies in scleroderma. Arthritis Research & Therapy. 2003; 5(2): 80-93. https://doi.org/10.1186/ar628 |
[28, 29]
. Different studies at different time periods had observed the presence of anti ssA, anti ssB, anti scl-70, and anti RNP in different CTDs like SLE, MCTD, SS, SSc, in different proportion
| [30] | Notman DD. Profiles of antinuclear antibodies in systemic rheumatic diseases. Annals of Internal Medicine. 1975; 83(4): 464-469. |
| [31] | Aganovic-Musinovic I, Karamehic J, Zecevic L, Gavrankapetanovic F, Avdagic N, Zaciragic A, et al. Evaluation of ENA-6 profile by ELISA immunoassay in patients with systemic lupus erythematosus. Autoimmune Diseases. 2012; 2012: 1-8. https://doi.org/10.1155/2012/321645 |
| [32] | Emad Y, Ragab Y, Hammam N, El-Shaarawy N, Ibrahim O, Gamal RM, et al. Autoantibodies to extractable nuclear antigens (ENAs) in rheumatoid arthritis patients. Reumatología Clínica. 2021; 17(5): 250-257.
https://doi.org/10.1016/j.reuma.2019.06.006 |
[30-32]
. It has been described the prevalence of ssA antibodies mainly in SLE, SS and overlap syndrome
. Some studies in past suggested that anti-RNP is prevalent in MCTD, SLE, SSc and overlapping conditions
.
Few Studies had seen the prevalence of anti scl-70 in SSc, SLE and overlap syndrome
. Hence in regards to the frequencies of different antigens in different CTDs, it is being sum up that there are some variations in different studies. This may be due to different geographical places with different populations.
In addition, there is some variability in the tests done for CTD diagnosis, within different laboratories and with different techniques as noted by Salamunic et al
Despite their widespread clinical use, current diagnostic methods for connective tissue disorders have certain limitations. Indirect immunofluorescence is observer-dependent and subject to inter-laboratory variability, while ELISA-based assays may lack sensitivity for low-titer or uncommon autoantibodies. Line immunoblot assays, although more specific, remain limited by fixed antigen panels. Recent advances such as multiplex immunoassays, addressable laser bead immunoassays, automated digital immunofluorescence interpretation systems, and proteomics-based autoantibody profiling may help overcome these limitations by enabling higher throughput, improved standardization, and enhanced diagnostic precision.
Further it is desirable that an international organization should make coordination between diagnostic laboratories performing different assays, more prominently an international organization should made to minimize the variations and make some standard at least for different populations.
5. Conclusion
CTD is a global problem with trends increasing in India, commonly seen among women frequently manifested by Fever, joint pain and skin rash. The commonest CTD is SLE followed by Systemic sclerosis (SSc) and for screening of CTDs ANA testing by IIF and ELISA procedures is the most ideal methods. ANA-IIF testing using HEp-2 substrate is the choice of investigation due to its different titer, pattern and intensity. ANA-IIF method ruled out the false positive ELISA results, it was taken as the gold standard for ANA testing. But as evident from the present study, IIF method is unable to detect low positive ELISA results hence screening of ANA should be done by ELISA before proceeding for IIF studies. At present most of the diagnosis are being done by the clinicians through clinical history with ANA testing. But there is a certain need for going through the ENA profiling for CTDs so as to pin point the particular disease, look for the prognosis of disease, prevention from the diseases and mode of treatment. The ENA profile can be done through Blot and ELISA techniques. Although there are some discrepancies between two methods, the blot test is more specific and therefore diagnostic. Moreover, it deals with 14 antigens assay in comparison to 6 antigens assay of ELISA. These antigens not only diagnostic for different diseases of CTDs, but also deals with prognostic values. As regards the variation in results between different techniques and different laboratories, it is important that definite standardization level should be established. Therefore, it is suggested that more such studies as the present one should be taken up in various geographical areas to sketch a clearer concept regarding the prevalence of various antibodies in CTDs. To conclude it is suggested that in all clinically suspected cases of CTDs, ANA along with ENA profile should be tested to diagnose, evaluate prognosis and to monitor the treatment.
Abbreviations
CTDs | Connective Tissue Disorders |
ANA | Anti-Nuclear Antibody |
ENA | Extractable Nuclear Antigen |
IIF | Indirect Immunofluorescence |
ELISA | Enzyme-linked Immunosorbent Assay |
LIA | Line-blot Immunoassay |
SLE | Systemic Lupus Erythematosus |
U-RNP | U Ribonucleoprotein |
PM-Scl | Polymyositis Systemic Sclerosis |
Acknowledgments
The authors would like to thank Department of Microbiology of S. C. B Medical College, Cuttack (Odisha) India for providing the laboratory facility in carrying out this research work. They would also like to thank Microbiology Lab of Desun Hospital, Kolkata, India for immunofluorescence study.
Author Contributions
Gutam Patnaik: Conceptualization, Data curation, Formal Analysis, Methodology, Investigation, Writing – original draft
Madhusmita Patnaik: Conceptualization, Investigation, Writing – original draft
Dharitri Mohapatra: Formal Analysis
Debasish Sahoo: Writing – original draft
Nirupama Chayani: Data curation, Methodology, Writing – original draft
Shrabanti Sarkar: Data curation, Methodology, Writing – original draft, Supervision
Ramesh Sethy: Conceptualization, Formal Analysis, Methodology, Writing – original draft, Supervision
Funding
This work is not supported by any external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
Data Availability Statement
The data is available from the corresponding author upon reasonable request.
References
| [1] |
Malaviya AN, Singh RR, Singh YN, Kapoor SK, Kumar A. Prevalence of systemic lupus erythematosus in India. Lupus. 1993; 2(2): 115-118.
https://doi.org/10.1177/096120339300200210
|
| [2] |
Minz RW, Kumar Y, Anand S, Singh S, Bamberi P, Verma S, et al. Antinuclear antibody positive autoimmune disorders in North India: an appraisal. Rheumatology International. 2012; 32(9): 2883-2888.
https://doi.org/10.1007/s00296-011-2073-4
|
| [3] |
Chandrasekaran AN, Radhakrishna B. Rheumatoid arthritis and connective tissue disorders: India and South-East Asia. Baillière’s Clinical Rheumatology. 1995; 9(1): 45-57.
https://doi.org/10.1016/S0950-3579(05)80155-3
|
| [4] |
Gunnarsson R, Molberg Ø, Gilboe IM, Gran JT. The prevalence and incidence of mixed connective tissue disease. Annals of the Rheumatic Diseases. 2011; 70(6): 1047-1051.
https://doi.org/10.1136/ard.2010.143792
|
| [5] |
Kumar Y, Bhatia A, Minz R. Antinuclear antibodies and their detection methods in diagnosis of connective tissue diseases. Diagnostic Pathology. 2009; 4: 1.
https://doi.org/10.1186/1746-1596-4-1
|
| [6] |
Tan EM, Kunkel HG. Characteristics of a soluble nuclear antigen precipitating with sera of patients with systemic lupus erythematosus. Journal of Immunology. 1966; 96(3): 464-471.
|
| [7] |
Tozzoli R, Bizzaro N, Tonutti E, Villalta D, Bassetti D, Manoni F, et al. Guidelines for the laboratory use of autoantibody tests. American Journal of Clinical Pathology. 2002; 117(2): 316-324.
https://doi.org/10.1309/Y5D3-8D7F-1C4M-MU0K
|
| [8] |
Isenberg DA, Manson JJ, Ehrenstein MR, Rahman A. Fifty years of anti-dsDNA antibodies. Rheumatology. 2007; 46(7): 1052-1056.
https://doi.org/10.1093/rheumatology/kem076
|
| [9] |
Kumar TS, Aggarwal A. Approach to a patient with connective tissue disease. Indian Journal of Pediatrics. 2010; 77(10): 1157-1164.
https://doi.org/10.1007/s12098-010-0215-4
|
| [10] |
Wiik AS, Gordon TP, Kavanaugh AF, Lahita RG, Reeves W, van Venrooij WJ, et al. Cutting edge diagnostics in rheumatology. Arthritis & Rheumatism. 2004; 51(2): 291-298.
https://doi.org/10.1002/art.20245
|
| [11] |
Angel J, Thomas M, Appalaraju B. Evaluation of ELISA and indirect immunofluorescence in autoimmune diseases. Journal of Academic Clinical Microbiology. 2015; 17(1): 7-12.
|
| [12] |
Mariz HA, Sato EI, Barbosa SH, Rodrigues SH, Dellavance A, Andrade LEC. Pattern on the ANA-HEp-2 test. Arthritis & Rheumatism. 2011; 63(1): 191-200.
https://doi.org/10.1002/art.30084
|
| [13] |
Ghosh P, Dwivedi S, Naik S, Agarwal V, Verma A, Aggarwal A. Antinuclear antibodies by indirect immunofluorescence. Indian Journal of Medical Research. 2007; 126(1): 34-38.
|
| [14] |
Rigon A, Soda P, Zennaro D, Iannello G, Afeltra A. Indirect immunofluorescence in autoimmune diseases. Cytometry Part B. 2007; 72B (6): 472-477.
https://doi.org/10.1002/cyto.b.20205
|
| [15] |
Maddison PJ, Skinner RP, Vlachoyiannopoulos P, Brennand DM, Hough D. Antibodies to nRNP, Sm, Ro and La detected by ELISA. Clinical and Experimental Immunology. 1985; 62(2): 337-345.
|
| [16] |
Abeles AM, Abeles M. The clinical utility of a positive ANA test result. The American Journal of Medicine. 2013; 126(4): 342-348.
https://doi.org/10.1016/j.amjmed.2012.09.014
|
| [17] |
Birtane M, Yavuz S, Taştekin N. Laboratory evaluation in rheumatic diseases. WJM. 2017; 7(1): 1.
|
| [18] |
Solomon DH, Katz JN, Jacobs JP, La Tourette AM, Coblyn J. Management of glucocorticoid‐induced osteoporosis in patients with rheumatoid arthritis: Rates and predictors of care in an academic rheumatology practice. Arthritis & Rheumatism. 2002 Dec; 46(12): 3136–42.
https://doi.org/10.1002/ART.10613
|
| [19] |
Meroni PL, Schur PH. ANA screening: an old test with new recommendations. Annals of the Rheumatic Diseases. 2010; 69(8): 1420-1422.
https://doi.org/10.1136/ard.2009.127100
|
| [20] |
Habash-Bseiso DE, Yale SH, Glurich I, Goldberg JW. Serologic testing in connective tissue diseases. Clinical Medicine & Research. 2005; 3(3): 190-193.
https://doi.org/10.3121/cmr.3.3.190
|
| [21] |
Gaubitz M. Epidemiology of connective tissue disorders. Rheumatology. 2006 Oct 1; 45(Supplement3): iii3–4.
https://doi.org/10.1093/rheumatology/kel282
|
| [22] |
Roberts‐Thomson PJ, Nikoloutsopoulos T, Cox S, Walker JG, Gordon TP. Antinuclear antibody testing in a regional immunopathology laboratory. Immunol Cell Biol. 2003 Oct; 81(5): 409–12.
https://doi.org/10.1046/j.1440-1711.2003.01182.x
|
| [23] |
Satoh M, Vázquez-Del Mercado M, Chan EKL. Clinical interpretation of antinuclear antibody tests in systemic rheumatic diseases. Modern Rheumatology. 2009 Jun; 19(3): 219–28.
https://doi.org/10.1007/s10165-009-0155-3
|
| [24] |
Von Mühlen CA, Tan EM. Autoantibodies in the diagnosis of systemicrheumatic diseases. Seminars in Arthritis and Rheumatism. 1995 Apr; 24(5): 323–58.
https://doi.org/10.1016/S0049-0172(95)80005-1
|
| [25] |
Hamburger M, Hodes S, Barland P. The incidence and clinical significance of antibodies to extractable nuclear antigens. The American Journal of the Medical Sciences. 1977; 273(1): 21-28.
https://doi.org/10.1097/00000441-197701000-00002
|
| [26] |
Haddouk S, Marzouk S, Jallouli M, Fourati H, Frigui M, Hmida YBH, et al. Clinical and diagnostic value of ribosomal P autoantibodies in systemic lupus erythematosus. Rheumatology. 2009; 48(8): 953-957.
https://doi.org/10.1093/rheumatology/kep145
|
| [27] |
Dähnrich C, Pares A, Caballeria L, Rosemann A, Schlumberger W, Probst C, et al. New ELISA for detecting primary biliary cirrhosis-specific antimitochondrial antibodies. Clinical Chemistry. 2009; 55(5): 978-985.
https://doi.org/10.1373/clinchem.2008.121053
|
| [28] |
Phan TG, Wong RCW, Adelstein S. Autoantibodies to extractable nuclear antigens: making detection and interpretation more meaningful. Clinical and Vaccine Immunology. 2002; 9(1): 1-7.
https://doi.org/10.1128/CDLI.9.1.1-7.2002
|
| [29] |
Ho KT, Reveille JD. The clinical relevance of autoantibodies in scleroderma. Arthritis Research & Therapy. 2003; 5(2): 80-93.
https://doi.org/10.1186/ar628
|
| [30] |
Notman DD. Profiles of antinuclear antibodies in systemic rheumatic diseases. Annals of Internal Medicine. 1975; 83(4): 464-469.
|
| [31] |
Aganovic-Musinovic I, Karamehic J, Zecevic L, Gavrankapetanovic F, Avdagic N, Zaciragic A, et al. Evaluation of ENA-6 profile by ELISA immunoassay in patients with systemic lupus erythematosus. Autoimmune Diseases. 2012; 2012: 1-8.
https://doi.org/10.1155/2012/321645
|
| [32] |
Emad Y, Ragab Y, Hammam N, El-Shaarawy N, Ibrahim O, Gamal RM, et al. Autoantibodies to extractable nuclear antigens (ENAs) in rheumatoid arthritis patients. Reumatología Clínica. 2021; 17(5): 250-257.
https://doi.org/10.1016/j.reuma.2019.06.006
|
| [33] |
Franceschini F, Cavazzana I. Anti-Ro/SSA and La/SSB antibodies. Autoimmunity. 2005; 38(1): 55-63.
https://doi.org/10.1080/08916930400022774
|
| [34] |
van Venrooij WJ, Pruijn GJ. Ribonucleoprotein complexes as autoantigens. Current Opinion in Immunology. 1995; 7(6): 819-824.
https://doi.org/10.1016/0952-7915(95)80051-3
|
| [35] |
Asano Y, Ihn H, Yamane K, Kubo M, Tamaki K. The prevalence and clinical significance of anti-U1 RNA antibodies in systemic sclerosis. Journal of Investigative Dermatology. 2003; 120(2): 204-210.
https://doi.org/10.1046/j.1523-1747.2003.12027.x
|
| [36] |
Tan EM. Antinuclear antibodies: diagnostic markers for autoimmune diseases and probes for cell biology. Advances in Immunology. 1989; 44: 93-151.
https://doi.org/10.1016/S0065-2776(08)60641-0
|
| [37] |
Helene A. Elicha Gussin GPI, John Varga, and Marius Teodorescu. Anti–Topoisomerase I (Anti–Scl-70) Antibodies in Patients with Systemic Lupus Erythematosus. Arthritis & Rheumatism. 2001, 44(2): 376–383.
https://doi.org/10.1002/1529-0131(200102)44:2<376::AID-ANR56>3.0.CO;2-2.
|
| [38] |
Mahler M, Silverman ED, Schulte-Pelkum J, Fritzler MJ. Anti-Scl-70 (topo-I) antibodies in SLE: Myth or reality? Autoimmunity reviews 2010, 9(11): 756-760.
https://doi.org/10.1016/j.autrev.2010.06.005
|
Cite This Article
-
APA Style
Patnaik, G., Patnaik, M., Mohapatra, D., Sahoo, D., Chayani, N., et al. (2026). Clinical Utility of Anti-nuclear Antibodies and Extractable Nuclear Antigen for Diagnosis of Connective Tissue Disorders. American Journal of Medical Science and Technology, 2(1), 10-18. https://doi.org/10.11648/j.ajmst.20260201.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Patnaik, G.; Patnaik, M.; Mohapatra, D.; Sahoo, D.; Chayani, N., et al. Clinical Utility of Anti-nuclear Antibodies and Extractable Nuclear Antigen for Diagnosis of Connective Tissue Disorders. Am. J. Med. Sci. Technol. 2026, 2(1), 10-18. doi: 10.11648/j.ajmst.20260201.12
Copy
|
Download
AMA Style
Patnaik G, Patnaik M, Mohapatra D, Sahoo D, Chayani N, et al. Clinical Utility of Anti-nuclear Antibodies and Extractable Nuclear Antigen for Diagnosis of Connective Tissue Disorders. Am J Med Sci Technol. 2026;2(1):10-18. doi: 10.11648/j.ajmst.20260201.12
Copy
|
Download
-
@article{10.11648/j.ajmst.20260201.12,
author = {Gutam Patnaik and Madhusmita Patnaik and Dharitri Mohapatra and Debasish Sahoo and Nirupama Chayani and Shrabanti Sarkar and Ramesh Sethy},
title = {Clinical Utility of Anti-nuclear Antibodies and Extractable Nuclear Antigen for Diagnosis of Connective Tissue Disorders},
journal = {American Journal of Medical Science and Technology},
volume = {2},
number = {1},
pages = {10-18},
doi = {10.11648/j.ajmst.20260201.12},
url = {https://doi.org/10.11648/j.ajmst.20260201.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajmst.20260201.12},
abstract = {Connective tissue disorders (CTDs) are associated with the production of multiple autoantibodies, predominantly anti-nuclear antibodies (ANA) and their subsets known as extractable nuclear antigens (ENA). Although ANA detection by indirect immunofluorescence (IIF) and enzyme-linked immunosorbent assay (ELISA) is routinely used for screening CTDs, these methods are limited by non-specificity. The present study evaluated the clinical utility of ENA profiling in conjunction with conventional ANA testing for CTD screening. Clinically suspected CTD patients were screened for ANA using ELISA and IIF, followed by ENA antibody detection using ELISA and line blot immunoassay (LIA). Out of a total of 274 clinically suspected cases analyzed, ANA positivity was observed in 23.7% of cases by indirect immunofluorescence and 26.2% by enzyme-linked immunosorbent assay. ENA analysis among ANA-positive cases revealed systemic lupus erythematosus (SLE) as the most prevalent CTD (68%), while Sjögren’s syndrome was the least common (1%). Among ENA specificities, U-RNP antibodies showed the highest frequency (56.9%), whereas PM-Scl antibodies were least frequent (1%). Although IIF remains the gold standard for ANA detection, ELISA is a useful initial screening tool, as IIF may fail to detect low-positive ANA cases identified by ELISA. Interpretation of ANA positivity should always be made in appropriate clinical context and confirmed by more specific tests such as ENA profiling. The observed geographical variation in ENA antibody frequency and CTD patterns highlights the need for further region-specific studies to better define antibody prevalence in CTDs.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Clinical Utility of Anti-nuclear Antibodies and Extractable Nuclear Antigen for Diagnosis of Connective Tissue Disorders
AU - Gutam Patnaik
AU - Madhusmita Patnaik
AU - Dharitri Mohapatra
AU - Debasish Sahoo
AU - Nirupama Chayani
AU - Shrabanti Sarkar
AU - Ramesh Sethy
Y1 - 2026/02/24
PY - 2026
N1 - https://doi.org/10.11648/j.ajmst.20260201.12
DO - 10.11648/j.ajmst.20260201.12
T2 - American Journal of Medical Science and Technology
JF - American Journal of Medical Science and Technology
JO - American Journal of Medical Science and Technology
SP - 10
EP - 18
PB - Science Publishing Group
UR - https://doi.org/10.11648/j.ajmst.20260201.12
AB - Connective tissue disorders (CTDs) are associated with the production of multiple autoantibodies, predominantly anti-nuclear antibodies (ANA) and their subsets known as extractable nuclear antigens (ENA). Although ANA detection by indirect immunofluorescence (IIF) and enzyme-linked immunosorbent assay (ELISA) is routinely used for screening CTDs, these methods are limited by non-specificity. The present study evaluated the clinical utility of ENA profiling in conjunction with conventional ANA testing for CTD screening. Clinically suspected CTD patients were screened for ANA using ELISA and IIF, followed by ENA antibody detection using ELISA and line blot immunoassay (LIA). Out of a total of 274 clinically suspected cases analyzed, ANA positivity was observed in 23.7% of cases by indirect immunofluorescence and 26.2% by enzyme-linked immunosorbent assay. ENA analysis among ANA-positive cases revealed systemic lupus erythematosus (SLE) as the most prevalent CTD (68%), while Sjögren’s syndrome was the least common (1%). Among ENA specificities, U-RNP antibodies showed the highest frequency (56.9%), whereas PM-Scl antibodies were least frequent (1%). Although IIF remains the gold standard for ANA detection, ELISA is a useful initial screening tool, as IIF may fail to detect low-positive ANA cases identified by ELISA. Interpretation of ANA positivity should always be made in appropriate clinical context and confirmed by more specific tests such as ENA profiling. The observed geographical variation in ENA antibody frequency and CTD patterns highlights the need for further region-specific studies to better define antibody prevalence in CTDs.
VL - 2
IS - 1
ER -
Copy
|
Download