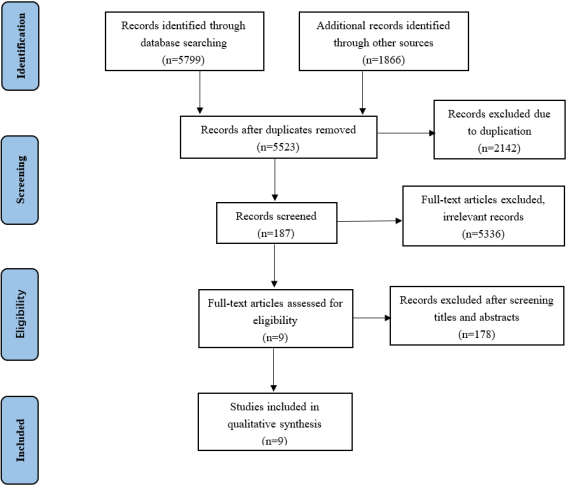
Non-alcoholic fatty liver disease (NAFLD) is one of the most common fatty liver diseases, leading to biochemical and histological disorders in NAFLD. It is characterized by kinds of pathologies, ranging from simple non-alcoholic fatty liver (NAFL) to serious non-alcoholic steatohepatitis (NASH) with the complication of steatosis, fibrosis, NASH cirrhosis and hepatocellular carcinoma (HCC). The most important potential risk factors including insulin resistance and increased oxidative stress, especially vitamin E, have significant influence on the treatment for NAFLD. Vitamin E, as a key fat-soluble antioxidant, presents potential therapeutic value in the intervention of NAFLD. At present, there are differences in the intervention measures proposed by various studies, and the efficacy of corresponding intervention measures has not yet reached a unified conclusion. To analyze the relevant research on the combination therapy of vitamin E in NAFLD patients, and to explore the intervention effect of vitamin E combination therapy on their biochemical indicators and histological abnormalities. PubMed, EMBASE, Medline, Cochrane, ScienceDirect, Web of science, and Google Scholar Database were systematically searched to screen studies on the intervention effect of vitamin E combination therapy on NAFLD from January 2005 to April 2025. A total of 9 randomized controlled trials (RCT) were included, which included 885 participants with an average age of 35~48.04 years. The combination therapy of vitamin E had significantly improved liver function indicators (aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), and gamma glutamyl transferase (GGT)) in NAFLD patients in most studies, and had also positive effects in improving liver histological parameters (NAFLD activity score (NAS), steatosis, fibrosis score, and inflammation), but there was heterogeneity among these studies. In addition, some studies did not observe significant improvement in ballooning, and only one study showed that combination therapy had no significant effect on liver function testing. The combination therapy of vitamin E has potential benefits in improving liver function indicators and some histological parameters in NAFLD patients, but its efficacy varies among studies. In the future, more high-quality and long-term RCT need to be conducted to further clarify the optimal regimen and applicable population of vitamin E in the treatment of NAFLD, providing a more comprehensive and reliable reference for clinical practice.
| Published in | American Journal of Internal Medicine (Volume 13, Issue 4) |
| DOI | 10.11648/j.ajim.20251304.12 |
| Page(s) | 54-63 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Vitamin E, Non-alcoholic Fatty Liver Disease, RCTs, Systematic Review
Authors and year | Type of study | Duration of study | Sample size | Mean age | Gender | Interventions used |
|---|---|---|---|---|---|---|
Akhondi-Meybodi et al. 2020 [ 29] | RCT | 4 months | Group1 (Vitamin E): 40 Group2 (Silymarin): 40 | Group1: 44.2 Group2: 43.7 | Group1: Females: 38% Males: 62% Group2: Females: 33% Males: 67% | Group1: Vitamin E 400 IU once Daily Group2: silymarin 140 mg BID once daily |
Ekhlasi et al. 2017 [1 9] | double-blinded RCT | 2 months | Group1 (symbiotic): 15 Group2 (alpha-tocopherol): 15 Group3 (symbiotic+alpha-tocopherol): 15 Group4 (placebo): 15 | 44 | Females: 20% Males: 80% | Group1: symbiotic 1 g once daily Group2: alpha-tocopherol 400 IU once daily Group3: symbiotic 1 g, alpha-tocopherol 400 IU once daily Group4: placebo 400 IU once daily |
Polyzos et al. 2017 [1 6] | RCT | 13 months | Group1 (spironolactone+ vitamin E): 14 Group2 (Vitamin E): 17 | - | Group1: Females: 85.7% Males: 14.3% Group2: Females: 64.7% Males: 35.3% | Group1: spironolactone 25 mg once daily, vitamin E 400 IU/day Group2: Vitamin E 400 IU/day |
Abedi et al. 2018 [1 7] | single-blind RCT | 2 months | Group1 (Vitamin E+soft gel CLA): 19 Group2 (vitamin E): 19 | Group1: 36.7 Group2: 38.6 | Group1: Females: 89.5% Males: 10.5% Group2: Females: 84.2% Males: 15.8% | Group1: Vitamin E 400, soft gel CLA 3000 mg/day Group2: vitamin E 400 mg/day |
Afzali et al. 2020 [ 11] | double-blind RCT | 6 months | Group1 (Beta vulgaris): 60 Group2 (Placebo): 57 | Group1: 47.5 Group2: 46.4 | Group1: Females: 45% Males: 55% Group2: Females: 49.1% Males: 50.9% | Group1: vitamin E pearl (300 IU/twice daily), Livergol tablet (140 mg/daily), Beta vulgaris capsule (400 mg/daily) Group2: vitamin E pearl (300 IU/twice daily), Livergol tablet (140 mg/daily), instead of Beta vulgaris capsule (400 mg/daily) |
Chandan et al 2021 [ 30] | RCT | 12 months | Group1 (Pentoxyphylline+Vitamin E): 36 Group2 (Vitamin E): 33 | Group1: 40 Group2: 35 | Group1: Males/Females 33/3 Group2: Males/Females 28/5 | Group1: Pentoxyphylline (400 mg/ thrice daily), vitamin E (400 IU/ twice daily) Group2: vitamin E (400 IU/ twice daily) |
Bilal et al 2024 [ 31] | RCT | 6 months | Group1 (Saroglitazar): 44 Group2 (Vitamin E): 41 Group3 (Saroglitazar +Vitamin E): 47 Group4 (control arm): 43 | 45 | Group1: Females: 19 Males: 25 Group2: Females: 17 Males: 24 Group3: Females: 14 Males: 33 Group4: Females: 13 Males: 30 | Group1: Saroglitazar (4 mg/ daily alone) Group2: vitamin E (800 IU/ daily alone) Group3: Saroglitazar (4 mg/ daily alone), vitamin E (800 IU/ daily alone) Group4: control arm |
Khaliq [ 32] | double-blind RCT | 6 months | Group1 (vitamin E): 42 Group2 (pioglitazone): 43 Group3 (ertugliflozin): 44 Group4 (vitamin E + ertugliflozin): 44 | 30-65 | Group1: Females: 11 Males: 31 Group2: Females: 10 Males: 33 Group3: Females: 9 Males: 35 Group4: Females: 10 Males: 34 | Group1: vitamin E (800 IU/ once daily) Group2: pioglitazone (30 mg/ once daily) Group3: ertugliflozin (15 mg/ once daily) Group4: ertugliflozin (15 mg/ once daily) vitamin E (800 IU/ once daily) |
Yu [ 33] | double-blind RCT | 24 months | Group1 (Vitamin E): 58 Group2 (placebo): 66 | Group1: 37.9 Group2: 39.0 | Group1: Females: 16 Males: 42 Group2: Females: 16 Males: 50 | Group1: vitamin E (300 mg / daily) Group2: placebo (300 mg / daily) |
Author and year | Improvement in liver function tests (ALT, AST, ALP, GGT) | Improvement in NAFLD Activity Score (NAS) | Improvement in steatosis | Improvement in fibrosis score | Improvement in ballooning | Improvement in inflammation |
|---|---|---|---|---|---|---|
Akhondi-Meybodi et al. 2020 [ 29] | significant decrease in ALT and AST in the treatment group | No | No | No | Not recorded | Not recorded |
Ekhlasi et al. 2017 [1 9] | significant decrease in AST, ALT and ALP level | Not recorded | No | No | Not recorded | No |
Polyzos et al. 2017 [1 6] | Not recorded | Not recorded | Yes | Not recorded | No | Not recorded |
Abedi et al. 2018 [1 7] | significant decrease in ALT/AST ratio in the treatment group | Not recorded | No | Not recorded | Not recorded | Yes |
Afzali et al. 2020 [ 11] | significant decrease in AST and ALT in the treatment group | Not recorded | Not recorded | No | Not recorded | Not recorded |
Chandan et al 2021 [ 30] | significant decrease in ALT level | Yes | Not recorded | Yes | Not recorded | Yes |
Bilal et al 2024 [ 31] | significant decrease in AST and ALT level | No | Yes | Yes | Not recorded | Not recorded |
Khaliq et al 2025 [ 32] | significant decrease in AST, ALT, ALP and GGT level | Not recorded | Yes | Yes | Not recorded | Not recorded |
Yu et al 2025 [ 33] | significant decrease in AST and ALT | Yes | Yes | No | No | Yes |
No. of results showing improvement | 9 | 2 | 4 | 3 | 0 | 3 |
No. of results showing no improvement | 0 | 2 | 3 | 4 | 2 | 1 |
No. of results not recorded | 1 | 5 | 2 | 2 | 7 | 5 |
NAFLD | Non-alcoholic Fatty Liver Disease |
NAFL | Non-Alcoholic Fatty Liver |
NASH | Non-alcoholic Steatohepatitis |
HCC | Hepatocellular Carcinoma |
RCT | Randomized Controlled Trials |
AST | Aspartate Aminotransferase |
ALT | Alanine Aminotransferase |
ALP | Alkaline Phosphatase |
GGT | Gamma Glutamyl Transferase |
NAS | NAFLD Activity Score |
IR | Insulin Resistance |
ROS | Reactive Oxygen Species |
T2DM | Type 2 Diabetes Mellitus |
CLA | Conjugated Linoleic Acid |
LDL | Low-density Lipoprotein |
| [1] | Derakhshandeh-Rishehri SM, Heidari-Beni M, Eftekhari MH. The effects of realsil (Silybin–phospholipid–vitamin e complex) on liver enzymes in patients with non-alcoholic fatty liver disease (nafld) or nonalcoholic steato-hepatitis (nash): A systematic review and meta-analysis of rcts [J]. Acta Endocrinologica. 2020, 16(2): 223-31. |
| [2] | Alberti G, Gana JC, Santos JL. Fructose, Omega 3 Fatty Acids, and Vitamin E: Involvement in Pediatric Non-Alcoholic Fatty Liver Disease [J]. Nutrients. 2020, 12(11). |
| [3] | Bellentani S. The epidemiology of non-alcoholic fatty liver disease [J]. Liver international: official journal of the International Association for the Study of the Liver. 2017, 37 Suppl 1: 81-4. |
| [4] | Argo CK, Caldwell SH. Epidemiology and natural history of non-alcoholic steatohepatitis [J]. Clin Liver Dis. 2009, 13(4): 511-31. |
| [5] | Lazo M, Clark JM. The epidemiology of nonalcoholic fatty liver disease: a global perspective [J]. Seminars in liver disease. 2008, 28(4): 339-50. |
| [6] | Khan, R. S., et al. Modulation of Insulin Resistance in Nonalcoholic Fatty Liver Disease [J]. Hepatology, 2019. 70(2): 711-724. |
| [7] | Smith, G. I., et al. Insulin resistance drives hepatic de novo lipogenesis in nonalcoholic fatty liver disease [J]. J Clin Invest, 2020. 130(3): 1453-1460. |
| [8] | Begriche, K., et al. Mitochondrial adaptations and dysfunctions in nonalcoholic fatty liver disease [J]. Hepatology, 2013. 58(4): 1497-507. |
| [9] | García-Ruiz, C. and J. C. Fernández-Checa. Mitochondrial Oxidative Stress and Antioxidants Balance in Fatty Liver Disease [J]. Hepatol Commun, 2018. 2(12): 1425-1439. |
| [10] | Tuma, D. J. Role of malondialdehyde-acetaldehyde adducts in liver [J]. Free Radical Biology and Medicine, 2002. 32(4): 303-308. |
| [11] | Afzali N, Ebadi SS, Afzali H, Sharif MR, Vazirian M, Ebadi SA, et al. Effect of Beta vulgaris Extract on Liver Enzymes in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Clinical Trial [J]. Hepatitis Monthly. 2020, 20(7): e102125. |
| [12] | Loguercio C, Federico A, Trappoliere M, Tuccillo C, de Sio I, Di Leva A, et al. The effect of a silybin-vitamin e-phospholipid complex on nonalcoholic fatty liver disease: a pilot study [J]. Digestive diseases and sciences. 2007, 52(9): 2387-95. |
| [13] | Lewis JD, Ferrara A, Peng T, Hedderson M, Bilker WB, Quesenberry CP, Jr., et al. Risk of bladder cancer among diabetic patients treated with pioglitazone: interim report of a longitudinal cohort study [J]. Diabetes care. 2011, 34(4): 916-22. |
| [14] | Schürks M, Glynn RJ, Rist PM, Tzourio C, Kurth T. Effects of vitamin E on stroke subtypes: meta-analysis of randomised controlled trials [J]. BMJ (Clinical research ed). 2010, 341: c5702. |
| [15] | Zhong S, Fan Y, Yan Q, Fan X, Wu B, Han Y, et al. The therapeutic effect of silymarin in the treatment of nonalcoholic fatty disease: A meta-analysis (PRISMA) of randomized control trials [J]. Medicine (Baltimore). 2017, 96(49): e9061. |
| [16] | Polyzos SA, Kountouras J, Mantzoros CS, Polymerou V, Katsinelos P. Effects of combined low-dose spironolactone plus vitamin E vs vitamin E monotherapy on insulin resistance, non-invasive indices of steatosis and fibrosis, and adipokine levels in non-alcoholic fatty liver disease: a randomized controlled trial [J]. Diabetes Obesity & Metabolism. 2017, 19(12): 1805-9. |
| [17] | Abedi R, Aref-Hosseini SR, Khoshbaten M, Ebrahimi-Mameghani M, Laleh HJ, Jalalypour F, et al. The Effect of conjugated linoleic acid (CLA) on inflammatory factors in Non-Alcoholic Fatty Liver Disease (NAFLD): A randomized controlled clinical trial [J]. Progress in Nutrition. 2018, 20: 173-81. |
| [18] | El Hadi H, Vettor R, Rossato M. Vitamin E as a Treatment for Nonalcoholic Fatty Liver Disease: Reality or Myth? [J]. Antioxidants (Basel, Switzerland). 2018, 7(1). |
| [19] | Ekhlasi G, Zarrati M, Agah S, Hosseini AF, Hosseini S, Shidfar S, et al. Effects of symbiotic and vitamin E supplementation on blood pressure, nitric oxide and inflammatory factors in non-alcoholic fatty liver disease [J]. EXCLI journal. 2017, 16: 278-90. |
| [20] | Rinella, M. E., et al. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease [J]. Hepatology, 2023. 77(5): 1797-1835. |
| [21] | Jiang, Q. Natural forms of vitamin E: metabolism, antioxidant, and anti-inflammatory activities and their role in disease prevention and therapy [J]. Free Radic Biol Med, 2014. 72: 76-90. |
| [22] | Napolitano, G., et al. Vitamin E Supplementation and Mitochondria in Experimental and Functional Hyperthyroidism: A Mini-Review [J]. Nutrients, 2019. 11(12): 2900. |
| [23] | Yogesha, S. D., et al. Unfurling of the band 4.1, ezrin, radixin, moesin (FERM) domain of the merlin tumor suppressor [J]. Protein Sci, 2011. 20(12): 2113-20. |
| [24] | Garg, A. and J. C. Lee. Vitamin E: Where Are We Now in Vascular Diseases? [J]. Life (Basel), 2022. 12(2): 310. |
| [25] | Lonn, E., et al. Effects of long-term vitamin E supplementation on cardiovascular events and cancer: a randomized controlled trial [J]. JAMA, 2005. 293(11): 1338-47. |
| [26] | Balbi, M. E., et al. Antioxidant effects of vitamins in type 2 diabetes: a meta-analysis of randomized controlled trials [J]. Diabetology & Metabolic Syndrome, 2018. 10(1): 18. |
| [27] | Dysken, M. W., et al. Effect of Vitamin E and Memantine on Functional Decline in Alzheimer Disease: The TEAM-AD VA Cooperative Randomized Trial [J]. JAMA, 2014. 311(1): 33-44. |
| [28] | Duell, P. B., et al. Nonalcoholic Fatty Liver Disease and Cardiovascular Risk: A Scientific Statement From the American Heart Association [J]. Arterioscler Thromb Vasc Biol, 2022. 42(6): e168-e185. |
| [29] | Akhondi-Meybodi M, Baghbanian M. The effect of silymarin and vitamin E in the treatment of non-alcoholic fatty liver disease: A randomized, double-blind clinical trial [J]. United European Gastroenterology Journal. 2019, 7(8): 758. |
| [30] | Kedarisetty CK, Bhardwaj A, Kumar G, et al. Efficacy of combining pentoxiphylline and vitamin E versus vitamin E alone in non-alcoholic steatohepatitis- A randomized pilot study [J]. Indian J Gastroenterol. 2021; 40(1): 41-49. |
| [31] | Mir BA, Sharma B, Sharma R, et al. A Prospective Randomised Comparative Four-arm Intervention Study of Efficacy and Safety of Saroglitazar and Vitamin E in Patients With Non-alcoholic Fatty Liver Disease (NAFLD)/Non-alcoholic Steatohepatitis (NASH)-SVIN TRIAL [J]. J Clin Exp Hepatol. 2024; 14(5): 101398. |
| [32] | Khaliq A, Badshah H, Shah Y. Combination therapy with vitamin E and ertugliflozin in patients with non-alcoholic fatty liver disease and type 2 diabetes mellitus: a randomized clinical trial [J]. Ir J Med Sci. 2025; 194(3): 899-908. |
| [33] | Song Y, Ni W, Zheng M, et al. Vitamin E (300 mg) in the treatment of MASH: A multi-center, randomized, double-blind, placebo-controlled study [J]. Cell Rep Med. 2025; 6(2): 101939. |
| [34] | Hamaguchi M, Kojima T, Takeda N, Nakagawa T, Taniguchi H, Fujii K, et al. The metabolic syndrome as a predictor of nonalcoholic fatty liver disease [J]. Annals of internal medicine. 2005, 143(10): 722-8. |
| [35] | Amanullah I, Khan YH, Anwar I, Gulzar A, Mallhi TH, Raja AA. Effect of vitamin E in non-alcoholic fatty liver disease: a systematic review and meta-analysis of randomised controlled trials [J]. Postgraduate medical journal. 2019, 95(1129): 601-11. |
| [36] | Leoni S, Tovoli F, Napoli L, Serio I, Ferri S, Bolondi L. Current guidelines for the management of non-alcoholic fatty liver disease: A systematic review with comparative analysis [J]. World journal of gastroenterology. 2018, 24(30): 3361-73. |
| [37] | Chalasani N, Younossi Z, Lavine JE, Diehl AM, Brunt EM, Cusi K, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association [J]. Hepatology. 2012, 55(6): 2005-23. |
| [38] | Loguercio C, Andreone P, Brisc C, et al. Silybin combined with phosphatidylcholine and vitamin E in patients with nonalcoholic fatty liver disease: a randomized controlled trial [J]. Free Radic Biol Med. 2012; 52(9): 1658-65. |
| [39] | Pietu F, Guillaud O, Walter T, Vallin M, Hervieu V, Scoazec JY, et al. Ursodeoxycholic acid with vitamin E in patients with nonalcoholic steatohepatitis: long-term results [J]. Clinics and research in hepatology and gastroenterology. 2012, 36(2): 146-55. |
| [40] | Bril F, Biernacki DM, Kalavalapalli S, Lomonaco R, Subbarayan SK, Lai J, et al. Role of Vitamin E for Nonalcoholic Steatohepatitis in Patients With Type 2 Diabetes: A Randomized Controlled Trial [J]. Diabetes care. 2019, 42(8): 1481-8. |
| [41] | Vadarlis A, Antza C, Bakaloudi DR, Doundoulakis I, Kalopitas G, Samara M, Dardavessis T, Maris T, Chourdakis M. Systematic review with meta-analysis: The effect of vitamin E supplementation in adult patients with non-alcoholic fatty liver disease [J]. J Gastroenterol Hepatol. 2021; 36(2): 311-319. |
| [42] | Fukui A, Kawabe N, Hashimoto S, Murao M, Nakano T, Shimazaki H, Kan T, Nakaoka K, Ohki M, Takagawa Y, Takamura T, Kamei H, Yoshioka K. Vitamin E reduces liver stiffness in nonalcoholic fatty liver disease [J]. World J Hepatol. 2015; 7(27): 2749-56. |
| [43] | Miller ER, 3rd, Pastor-Barriuso R, Dalal D, Riemersma RA, Appel LJ, Guallar E. Meta-analysis: high-dosage vitamin E supplementation may increase all-cause mortality [J]. Annals of internal medicine. 2005, 142(1): 37-46. |
| [44] | Berry D, Wathen JK, Newell M. Bayesian model averaging in meta-analysis: vitamin E supplementation and mortality [J]. Clinical trials (London, England). 2009, 6(1): 28-41. |
| [45] | Jiang S, Pan Z, Li H, Li F, Song Y, Qiu Y. Meta-analysis: low-dose intake of vitamin E combined with other vitamins or minerals may decrease all-cause mortality [J]. Journal of nutritional science and vitaminology. 2014, 60(3): 194-205. |
| [46] | Abdel-Maboud M, Menshawy A, Menshawy E, Emara A, Alshandidy M, Eid M. The efficacy of vitamin E in reducing non-alcoholic fatty liver disease: a systematic review, meta-analysis, and meta-regression [J]. Therapeutic advances in gastroenterology. 2020, 13: 1756284820974917. |
APA Style
Liu, C., Bai, Z., Cheng, J. (2025). Vitamin E as a Therapeutic Agent for NAFLD: A Systematic Review of Randomized Controlled Trials. American Journal of Internal Medicine, 13(4), 54-63. https://doi.org/10.11648/j.ajim.20251304.12
ACS Style
Liu, C.; Bai, Z.; Cheng, J. Vitamin E as a Therapeutic Agent for NAFLD: A Systematic Review of Randomized Controlled Trials. Am. J. Intern. Med. 2025, 13(4), 54-63. doi: 10.11648/j.ajim.20251304.12
@article{10.11648/j.ajim.20251304.12,
author = {Can Liu and Zeming Bai and Jingmin Cheng},
title = {Vitamin E as a Therapeutic Agent for NAFLD: A Systematic Review of Randomized Controlled Trials
},
journal = {American Journal of Internal Medicine},
volume = {13},
number = {4},
pages = {54-63},
doi = {10.11648/j.ajim.20251304.12},
url = {https://doi.org/10.11648/j.ajim.20251304.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajim.20251304.12},
abstract = {Non-alcoholic fatty liver disease (NAFLD) is one of the most common fatty liver diseases, leading to biochemical and histological disorders in NAFLD. It is characterized by kinds of pathologies, ranging from simple non-alcoholic fatty liver (NAFL) to serious non-alcoholic steatohepatitis (NASH) with the complication of steatosis, fibrosis, NASH cirrhosis and hepatocellular carcinoma (HCC). The most important potential risk factors including insulin resistance and increased oxidative stress, especially vitamin E, have significant influence on the treatment for NAFLD. Vitamin E, as a key fat-soluble antioxidant, presents potential therapeutic value in the intervention of NAFLD. At present, there are differences in the intervention measures proposed by various studies, and the efficacy of corresponding intervention measures has not yet reached a unified conclusion. To analyze the relevant research on the combination therapy of vitamin E in NAFLD patients, and to explore the intervention effect of vitamin E combination therapy on their biochemical indicators and histological abnormalities. PubMed, EMBASE, Medline, Cochrane, ScienceDirect, Web of science, and Google Scholar Database were systematically searched to screen studies on the intervention effect of vitamin E combination therapy on NAFLD from January 2005 to April 2025. A total of 9 randomized controlled trials (RCT) were included, which included 885 participants with an average age of 35~48.04 years. The combination therapy of vitamin E had significantly improved liver function indicators (aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), and gamma glutamyl transferase (GGT)) in NAFLD patients in most studies, and had also positive effects in improving liver histological parameters (NAFLD activity score (NAS), steatosis, fibrosis score, and inflammation), but there was heterogeneity among these studies. In addition, some studies did not observe significant improvement in ballooning, and only one study showed that combination therapy had no significant effect on liver function testing. The combination therapy of vitamin E has potential benefits in improving liver function indicators and some histological parameters in NAFLD patients, but its efficacy varies among studies. In the future, more high-quality and long-term RCT need to be conducted to further clarify the optimal regimen and applicable population of vitamin E in the treatment of NAFLD, providing a more comprehensive and reliable reference for clinical practice.
},
year = {2025}
}
TY - JOUR T1 - Vitamin E as a Therapeutic Agent for NAFLD: A Systematic Review of Randomized Controlled Trials AU - Can Liu AU - Zeming Bai AU - Jingmin Cheng Y1 - 2025/09/05 PY - 2025 N1 - https://doi.org/10.11648/j.ajim.20251304.12 DO - 10.11648/j.ajim.20251304.12 T2 - American Journal of Internal Medicine JF - American Journal of Internal Medicine JO - American Journal of Internal Medicine SP - 54 EP - 63 PB - Science Publishing Group SN - 2330-4324 UR - https://doi.org/10.11648/j.ajim.20251304.12 AB - Non-alcoholic fatty liver disease (NAFLD) is one of the most common fatty liver diseases, leading to biochemical and histological disorders in NAFLD. It is characterized by kinds of pathologies, ranging from simple non-alcoholic fatty liver (NAFL) to serious non-alcoholic steatohepatitis (NASH) with the complication of steatosis, fibrosis, NASH cirrhosis and hepatocellular carcinoma (HCC). The most important potential risk factors including insulin resistance and increased oxidative stress, especially vitamin E, have significant influence on the treatment for NAFLD. Vitamin E, as a key fat-soluble antioxidant, presents potential therapeutic value in the intervention of NAFLD. At present, there are differences in the intervention measures proposed by various studies, and the efficacy of corresponding intervention measures has not yet reached a unified conclusion. To analyze the relevant research on the combination therapy of vitamin E in NAFLD patients, and to explore the intervention effect of vitamin E combination therapy on their biochemical indicators and histological abnormalities. PubMed, EMBASE, Medline, Cochrane, ScienceDirect, Web of science, and Google Scholar Database were systematically searched to screen studies on the intervention effect of vitamin E combination therapy on NAFLD from January 2005 to April 2025. A total of 9 randomized controlled trials (RCT) were included, which included 885 participants with an average age of 35~48.04 years. The combination therapy of vitamin E had significantly improved liver function indicators (aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), and gamma glutamyl transferase (GGT)) in NAFLD patients in most studies, and had also positive effects in improving liver histological parameters (NAFLD activity score (NAS), steatosis, fibrosis score, and inflammation), but there was heterogeneity among these studies. In addition, some studies did not observe significant improvement in ballooning, and only one study showed that combination therapy had no significant effect on liver function testing. The combination therapy of vitamin E has potential benefits in improving liver function indicators and some histological parameters in NAFLD patients, but its efficacy varies among studies. In the future, more high-quality and long-term RCT need to be conducted to further clarify the optimal regimen and applicable population of vitamin E in the treatment of NAFLD, providing a more comprehensive and reliable reference for clinical practice. VL - 13 IS - 4 ER -
School of Management, Shanxi Medical University, Taiyuan, China; School of Public Health, Shanxi Medical University, Taiyuan, China
School of Medicine and Food Engineering, Shanxi University of Chinese Medicine, Jinzhong, China
School of Management, Shanxi Medical University, Taiyuan, China
Information