Abstract
Menière's disease (MD) is a chronic inner ear disorder characterised by vertigo, fluctuating hearing loss, and fullness, frequently associated with migraine. The aetiology of MD is multifactorial but unclear. Endolymphatic hydrops (EH) is the histopathological marker. The correlation between venous disorders and MD is described in the literature. Our study aims to evaluate the incidence of Transverse Sinus Asymmetries (TSA) in patients with Menière Disease (MD) and non-migrainous headaches to test a physiopathological hypothesis. Materials and Methods: We conducted a retrospective study of 32 patients with symptoms of MD and non-migrainous headaches who presented to TSA on Magnetic Resonance Imaging (MR). Each patient underwent clinical evaluation, Audiometry, impedanceometry, VHIT, VEMPS, RM Angiography (RMA), transcranial colour doppler ultrasound (TCD) to study the intracranial venous system and vascular flow. Results: All patients were diagnosed as probable in 41% and certain in 59%. On RMA results, 91% showed TSA. We propose four TSA stages. RMA showed 83% left TS hypoplasia and 17% right TS hypoplasia. All patients with TSA showed MD. Patients with left TSA showed right MD; patients with right TSA showed left or bilateral MD. We used TCD in 15 patients: 10 patients showed alteration or flow reversal. In 5 subjects was not possible due to mastoid ossification. Conclusions: Ultimately, a clear association exists between TS absence or hypoplasia in many Menière’s patients with non-migrainous headaches. Moreover, there is a correspondence between the side of MD and TSA, which is contralateral. Our study suggests to follow-up patients with TSA to prevent the onset of EH.
|
Published in
|
American Journal of Internal Medicine (Volume 13, Issue 3)
|
|
DOI
|
10.11648/j.ajim.20251303.11
|
|
Page(s)
|
32-42 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Menière Disease, Transverse Sinus, Non-migrainous Headache, Vestibular Evoked Potentials, Magnetic Resonance Angiography
1. Introduction
Menière’s disease (MD) is a chronic disorder of the inner ear characterised by vertigo attacks, fluctuating hearing loss, tinnitus, and aural fullness, with a prevalence of 190/100,000 in the USA
and 513/100,000 in Finland
. Probably the significant differences among the cases published in the literature are due, on the one hand, to the difficulty of establishing the diagnosis by primary care physicians
, to the methods of data collection and analysis, and finally, to the greater or lesser confidence of physicians with other chronic conditions presenting the same symptomatology as essential intracranial hypertension or migraine
| [4] | Attanasio G, Cagnoni L, Masci E, Ciciarello F, Diaferia F, et al. Chronic cerebrospinal venous insufficiency as a cause of inner ear diseases. Acta Otolaryngol. 2017 May; 137(5): 460-463. https://doi.org/10.1080/00016489.2016.1252853 Epub 2016 Nov 16. |
[4]
. The aetiology of MD is multifactorial but not yet fully understood, and its histologic marker is endolymphatic hydrops (EH)
| [5] | Committee on Hearing and Equilibrium guidelines for the diagnosis and evaluation of therapy in Meniere's disease. American Academy of Otolaryngology-Head and Neck Foundation, Inc, author. Otolaryngol Head Neck Surg. 1995; 113: 181–185. |
[5]
that, through the increase of endolymphatic pressure, leads to damage to the cochlear and then the vestibular hair cells. The primary symptoms, such as episodic vertigo, fluctuating hearing loss and tinnitus, are sufficient to lead to diagnosis in a high percentage of patients. However, the same symptoms can underlie arterial, venous and cerebrospinal fluid (CSF) disorders
| [4] | Attanasio G, Cagnoni L, Masci E, Ciciarello F, Diaferia F, et al. Chronic cerebrospinal venous insufficiency as a cause of inner ear diseases. Acta Otolaryngol. 2017 May; 137(5): 460-463. https://doi.org/10.1080/00016489.2016.1252853 Epub 2016 Nov 16. |
[4]
.
Tinnitus, for example, has also been clinically associated with brain perfusion asymmetries, identified by three-dimensional real inversion recovery (3D-real IR) MRI, and reflects an interference in homeostasis in EH grades and the degree of perilymphatic enhancement
| [6] | Li J, Jin X, Kong X, Hu N, Li X, Wang L, Liu M, Li C, Liu Y, Sun L, Gong R. Correlation of endolymphatic hydrops and perilymphatic enhancement with the clinical features of Ménière's disease. Eur Radiol. 2024 Feb 3. https://doi.org/10.1007/s00330-024-10620-y Epub ahead of print. |
[6]
. The major veins that drain venous blood out from the inner ear to the jugular system are the transverse sinus (TS), Sigmoid sinus (SS) and, after the Jugular hole, the inner Jugular Vein. Abnormalities in the Jugular system often occur even in people with underestimated symptoms. They may arise from congenital or acquired conditions, but abnormalities of the TS appear to play a crucial role in the development of the EH
| [4] | Attanasio G, Cagnoni L, Masci E, Ciciarello F, Diaferia F, et al. Chronic cerebrospinal venous insufficiency as a cause of inner ear diseases. Acta Otolaryngol. 2017 May; 137(5): 460-463. https://doi.org/10.1080/00016489.2016.1252853 Epub 2016 Nov 16. |
[4]
. The association between headache and MD is still to be discovered: it occurs in 70% of patients with MD and may be related to the different concurrent situations (CCSVI, Jugular Bulb’s Kinking, primary intracranial hypertension and others)
; overall, headache may be the primary and only symptom related to abnormalities of the intracranial venous system, in particular of the TS, as said before
| [8] | Iannachero, R. et al. Diagnosis and treatment of headache probably attributed to cerebral venous sinus thrombosis. Clinical Management Issues, [S.l.], v. 8, n. 4, p. 97-101, dec. 2014. ISSN 2283-3137. Date accessed: 19 jan. 2024. Available at: https://doi.org/10.7175/cmi.v8i4.966 |
[8]
. But the question of how maybe menière patients have TSA and how TSA can lead to EH is unknown? Alper, in 2004, reported that in the normal population, 24% presented TSA, 26,8% with hypoplasia, and 3,3% with aplasia or atresia
| [9] | Alper F, Kantarci M, Dane S, et al. Importance of anatomical asymmetries of transverse sinuses: an MR venographic study. Cerebrovasc Dis 2004; 18: 236–9. |
[9]
; the Author defines these abnormalities as “anatomical variants”, but his data reported only people with radiological normality. A correlation between radiological findings and clinical signs is missing. Unfortunately, this work has led radiologists to consider abnormalities of the transverse and sigmoid sinuses as paraphysiological conditions to be considered only in the differential diagnosis of dural sinus thrombosis. The lack of the patient's clinical appearance, anamnesis, instrumental tests, and symptoms prompted us to investigate whether alterations of this kind could be a radiological sign of internal ear dysfunction, particularly MD. In our work, we aimed to consider the clinical aspects (MD and non-migrainous headache) as a starting point to evaluate whether alterations of the venous sinuses were present, and review the pathophysiological correlation.
The TSA, like atresia and hypoplasia, are congenital. At the same time, thrombosis is acquired. It occurs in all situations that may induce hypercoagulability (such as pregnancy, oral contraceptives, cancer, recent major surgery, V factor of Leiden mutation) but also in head traumas or injury and ENT pathologies (as middle ear infection, sinusitis, brain and neck infections)
| [10] | Capecchi M, Abbattista M, Martinelli I. Cerebral venous sinus thrombosis. J Thromb Haemost. 2018 Oct; 16(10): 1918-1931. https://doi.org/10.1111/jth.14210 Epub 2018 Jul 11 |
[10]
. In all cases, TSA can be unnoticed overall if the contralateral TS has a normal size. The partial or total occlusion can manifest with vertigo and headache, only described as continuous, oppressive, worsening, and lying in bed (if in this position, the major venous drainage is at the Jugular system’s charge), non-migrainous-like according to IHS criteria
| [11] | International Headache Society: The International Classification of Headache Disorders 3ed. |
[11]
.
Recently, Mamikoglu et al. demonstrated that an increase or decrease in cerebrospinal fluid pressure appears to cause headaches, and this pressure change may result in increased perilymphatic pressure, leading to EH and dizziness over time
| [12] | Mamikoglu B, Algın O, Mengü G, Erdoğan-Küçükdağlı F, Kessler A. Transverse sinus pathologies, vestibular migraine and intracranial hypertension without papilledema. Am J Otolaryngol. 2023 Sep-Oct; 44(5): 103931. https://doi.org/10.1016/j.amjoto.2023.103931 |
[12]
. The association between headache and MD is still to be discovered: it occurs in 70% of patients with MD and may be related to the different concurrent situations (CCSVI, Jugular Bulb’s Kinking, primary intracranial hypertension and others)
| [5] | Committee on Hearing and Equilibrium guidelines for the diagnosis and evaluation of therapy in Meniere's disease. American Academy of Otolaryngology-Head and Neck Foundation, Inc, author. Otolaryngol Head Neck Surg. 1995; 113: 181–185. |
[5]
; overall, headache may be the primary and only symptom related to abnormalities of the intracranial venous system, in particular of the TS, as said before
| [9] | Alper F, Kantarci M, Dane S, et al. Importance of anatomical asymmetries of transverse sinuses: an MR venographic study. Cerebrovasc Dis 2004; 18: 236–9. |
[9]
. But how can TSA lead to EH? The answer could be in the compensatory dynamics of the transverse sinuses’ pressures. In the presence of TSA on one side, the pressures are compensated by the more patent side, which dilates. In the contralateral sinus, ultimately, the blood pressure increases. This amount of pressure, even if not elevated, may lead to venous blood stasis and the reflow of toxic metabolites in the inner ear, which may be a determinant in vestibular damage and contribute to EH. According to this hypothetical physiopathological mechanism, asymmetries in TS size may be a cause of EH and, subsequently, of MD. Imaging is used with gadodiamide to visualise hydrops directly or to exclude other causes of illness (neurinoma, neurological pathologies, etc.). The goal of the study is to establish a radiological correlation between TSA and MD to improve the radiological diagnosis of MD’s causes.
2. Material and Methods
A retrospective experimental study was conducted on 32 patients aged 12 to 89, with a mean age of 57, who presented to the Otolaryngological observation from May 2018 to June 2019 due to Menière-like symptoms associated with non-migrainous headaches.
2.1. Inclusion Criteria
1) Supposed or defined MD according to AAO-HNS, committee of Hearing and Equilibrium guidelines (1995)
| [5] | Committee on Hearing and Equilibrium guidelines for the diagnosis and evaluation of therapy in Meniere's disease. American Academy of Otolaryngology-Head and Neck Foundation, Inc, author. Otolaryngol Head Neck Surg. 1995; 113: 181–185. |
[5]
.
2) At least one-lifetime episode of acute intense non-migraine or non-tensive headache according to ICHD-3
| [11] | International Headache Society: The International Classification of Headache Disorders 3ed. |
[11]
, lasting no less than 24 hours.
2.2. Exclusion Criteria
1) No evidence of lifetime headache.
2) Bedside and instrumental examination, BPPV positivity;
3) Neoplastic pathology;
4) Use of hearing aid;
5) Neurological disease.
Each patient underwent a standardised clinical pathway composed of the following:
2.3. Clinical Evaluation
History and objectivity are used to evaluate each patient’s current condition and identify inclusion or exclusion criteria, as well as to determine therapies that may interfere with EH, such as diuretics. This assessment also helps identify whether the patient has a family history of other MD cases or a thrombotic history.
VIDEO NYSTAGMUS SCOPE (VNS) Bedside Exam (BE): The Euroclinic VNS was used to study spontaneous and induced nystagmus in response to various stimulations. According to the literature, the most valuable methods for studying nystagmus in MD are the HST (head shaking test), SVINT (skull vibration-induced nystagmus test), and spontaneous nystagmus induced by irritating phenomena.
Instrumental evaluation:
AUDIOMETRY is used to evaluate a hearing loss and its pattern over time, according to the patient’s sensation, and compared, when possible, to past exams, which may confirm fluctuations in the hearing loss
| [13] | Belinchon A, Perez-Garrigues H, Tenias JM, Lopez A. Hearing assessment in Menière's disease. Laryngoscope. 2011 Mar; 121(3): 622-6. https://doi.org/10.1002/lary.21335 |
[13]
. The test is performed in a silent booth. Generally, the ambient noise should not exceed 35 dB. The patient sits in a chair in the audiometric booth. The operator should be visible to the patient, but he should not be able to view the control panel of the audiometer. Immediate and efficient communication between the operator and patient must be ensured. The examiner instructs the patient on the execution: the patient is asked to raise his hand or press the button whenever he perceives a sound. The examination starts with the measurement of the threshold in the ear that the patient feels is best at 1000 Hz. Next, the frequencies of 2000, 4000, 8000, 500, and 250 Hz are assessed. The contralateral ear is then examined in the same order. The duration of the stimulus presented should be between 1 and 3 seconds.
IMPEDENZOMETRY: Objective instrumental examination to study the function and integrity of the transmission structures of the middle ear. It allows evaluation of the tympanogram (elasticity of the tympanic membrane in response to pressure changes) and the search for ipsi and contralateral stapedial reflexes (validation of proper functioning of the ossicular chain). It is performed by introducing a probe into the external auditory canal. In patients with MD, the audiogram typically shows a sensorineural type of hearing loss. Still, it may be mixed in low frequencies if a transmissible component is associated, which can be assessed by gap calculation. In addition, the presence of recruitment can be verified by a positive response to the Metz test (a difference of more than 70 dB between the audiometric curve and the stapedial reflex threshold).
OCULAR AND CERVICAL VESTIBULAR EVOKED MYOGENIC POTENTIALS (VEMPS)
Different studies have proven the role of ocular (oVEMPs) and cervical (cVEMPs) VEMPS, as a tool in diagnosing MD
| [14] | Scarpa A, Gioacchini FM, Cassandro E, Tulli M, Ralli M, Re M, Cassandro C. Clinical application of cVEMPs and oVEMPs in patients affected by Ménière's disease, vestibular neuritis and benign paroxysmal positional vertigo: a systematic review. Acta Otorhinolaryngol Ital. 2019 Oct; 39(5): 298-307. https://doi.org/10.14639/0392-100X-2104 |
[14]
. cVEMP responses are characterised by biphasic waves with initial positivity (p13) followed by a negative wave (n23). cVEMP pathway originates in the saccular macula. It continues through the vestibular nerve and nucleus, vestibulospinal tracts, spinal motor nuclei, and sternocleidomastoid muscles
. oVEMP is a myogenic response recorded from contralateral extraocular muscles in response to acoustic stimuli, which are the manifestation of crossed vestibulo-ocular reflex. Their pathway probably proceeds through the medial longitudinal fasciculus, oculomotor nuclei nerves and extraocular muscles after activating the vestibular nerve and nucleus
. oVEMP responses are characterised by biphasic waves with an initial negative peak (n1) followed by a positive peak (p1).
The cVEMP and the oVEMPS were assessed using the LABAT System and considering air conduction. Cervical and ocular VEMPS have been evaluated for their latency in response to acoustic stimulation. The test is administered as follows:
In case of cVEMPs, the patient is positioned sitting semi-supine with the head flexed. Four electrodes are used: the positive electrode is placed on the anterior edge of the sternocleidomastoid muscle on one side, and the other is placed on the contralateral side. The ground electrode is placed on the forehead, and the negative electrode is placed on the sternum. The headset is used to deliver auditory stimuli. The patient is asked to turn his head to the opposite tested side, looking toward the shoulder
| [17] | Dorbeau C, Bourget K, Renard L, Calais C, Bakhos D. Vestibular evoked myogenic potentials. Eur Ann Otorhinolaryngol Head Neck Dis. 2021 Dec; 138(6): 483-488. https://doi.org/10.1016/j.anorl.2021.01.001 Epub 2021 Jan 19. |
[17]
. The sound stimulus elicits an inhibitory response to muscle contraction. It is characterised by a biphasic complex consisting of an initial positive deflection followed by a negative deflection of the tracing. The deflections appear after a latency of 13 and 23 msec (p13, n23 in the graph). The response will be absent in the case of saccular and inferior vestibular nerve branch deficits and lesions
| [18] | Marcelli, Vincenzo. “VESTIBOLOGIA CLINICA.” 72. Cap. 15. NEMS-MNAMON Editor., 2021, ISBN 979-12-80296-10-8. |
[18]
.
In the case of oVEMPs, the patient is sitting and looking upward. The position of the electrodes is as follows: the ground electrode (black) is placed on the forehead or sternum, the active electrodes are placed infraorbital just below the pupil, and the reference electrodes are 1-2 cm below the active electrodes.
VIDEO HEAD IMPULSE TEST (VHIT) was assessed for its essential role in detecting channel pathologies (such as lithiasis) and in the study of VOR asymmetries. It is the recording of the head-impulse test through an accelerometer for head movements and a camera for eye movements. The test allows the Vestibulo-Ocular Reflex (VOR) gain value (head movement velocity ratio to eye counter-rotation velocity, expressed as a percentage) to be evaluated through a trace. Still, there is no relationship between the proportion of abnormal VHIT test results in patients with MD and the duration or stage of the disease
| [19] | Van Esch BF, Abolhosseini K, Masius-Olthof S, van der Zaag-Loonen HJ, van Benthem PPG, Bruintjes TD. Video-head impulse test results in patients with Menière's disease related to duration and stage of disease. J Vestib Res. 2018; 28(5-6): 401-407. https://doi.org/10.3233/VES-190654 |
[19]
. This study was used to identify exclusion criteria.
THE SKULL VIBRATION-INDUCED NYSTAGMUS TEST (SVINT) This test, also called the vibratory test, assesses vestibular asymmetry (VOR gain asymmetry) at high frequencies. The stimulus involves all labyrinthine structures, including the semicircular canals and otoliths, bilaterally
| [20] | Georges Dumas, Ian S Curthoys, Alexis Lion, Philippe Perrin, Sebastien Schmerber. The Skull vibration- induced Nystagmus Test of vestibular Function-A Review. Frontiers in Neurology, 2017, 8, pp. 41. https://doi.org/10.3389/fneur.2017.00041 |
[20]
. The test uses a 100Hz vibrator applied for 5-6 seconds on the vertex of the frontal bone and the right and left mastoid, while the patient is seated. The subject's response is assessed for each stimulated area. Fixation inhibition, using Frenzel goggles or videonystagmoscopy, is required for this examination. Stimulation of the mastoids and vertex leads to simultaneous and synchronous excitation of the hair cells of both bilateral vestibular structures. When the dynamic gain of the VOR is symmetrical both vestibular signals will cancel out each other, resulting in no SVINT response. However, if an asymmetry of the VOR is present, it will result in a nystagmus directed toward the prevailing side. When the vibratory stimulus is applied, it spreads instantly throughout the head. This vibratory stimulus excites the labyrinth cells. If the labyrinth cells are present and there is no deficit, they will be excited; conversely, if there is a lesion or deficit of the labyrinth cells, they will not be excited. The latency and fatigability of this test are absent, so nystagmus appears when the vibratory pulse is applied and shags when it is removed. It has high specificity, and it is proportional to the deficit: if the lesion is >50%, nystagmus will be present, while if the lesion is <50%, it will be absent. If the patient has no areflexia (absence of nystagmus), there are two possibilities: either the patient is totally areflexic (neither labyrinth is excited), or they have central pathology
| [21] | DUMAS Georges DUMAS, Christol FABRE, Flavio PEROTTINO, Haoyue TAN, Patrick PROY, Sébastien SCHMERBER Skull vibration induced nystagmus test in Menière’s disease Otorinolaringologia 2020 December; 70(4): 121-7 https://doi.org/10.23736/S0392-6621.20.02320-6 |
[21]
.
RMA is used to study the venous intracranial system, to evaluate the presence, absence, atresia, and asymmetry of both TS
| [22] | Han K, Chao AC, Chang FC, Hsu HY, Chung CP, Sheng WY, Chan L, Wu J, Hu HH. Diagnosis of Transverse Sinus Hypoplasia in Magnetic Resonance Venography: New Insights Based on Magnetic Resonance Imaging in Combined Dataset of Venous Outflow Impairment Case-Control Studies: Post Hoc Case-Control Study. Medicine (Baltimore). 2016 Mar; 95(10): e2862. https://doi.org/10.1097/MD.0000000000002862 |
[22]
. In this study, cerebral AngioRM will be considered. Flow-dependent RMA methods have been used to exploit the kinematics of red blood cells to distinguish them from static tissues based on contrast medium (Gadolinium) injection. Among them, we consider the TOF-MRA, time-of-flight Angiography, in its 2D multi-slice, 3D single-slab, and 3D multi-slab variants. For the study of the venous compartment, a short TR, i.e., the time between one resonance pulse and the next, and a flip angle between 50° and 70° were used to determine a constant inflow enhancement that ensures contrast of the vessel respecting the tissues even in slow-flowing vessels.
TRANSCRANIAL COLOR DOPPLER (TCD). Intracranial flow is one-way, low velocity and low resistance index; dural sinuses can be analysed with a 3-5 MHz probe by SonoVue® ultrasound MDC technology, which analyses with a three-dimensional view the Doppler profile of several flows acquired simultaneously by Multigate technique. According to the DIR algorithm, the spectra are processed and presented to highlight the flow direction in real-time. Ultrasound is a qualitative and quantitative, dynamic and noninvasive study of intracranial vascular and nonvascular structures
. It is performed with very high-frequency probes capable of bypassing the cranial theca. Several windows can be used: in the study of the cranial fossa, the mesencephalic window, commonly known as the temporoauricular window, has been chosen.
2.4. Statistical Analysis
The Shapiro-Wilk test was used to assess the normality of the sample distribution, while Levene's test was used to calculate the homogeneity of variance. At the end of the diagnostic pathway, qualitative data from the radiological study of the posterior cranial fossa were correlated with the patient's clinical findings. We used MANOVA parametric tests and one-way ANOVA to highlight differences in different stages for the parameters considered (
Tables 2-6).
3. Results
We have recruited 32 subjects, ranging in age from 12 to 89 years (with an average age of 57). From the data obtained, according to Bàràny Society’s criteria, all patients received the diagnosis of 3 clinical classes:
1) Probable MD: 41% (n=13)
2) Definite MD: 59% (n=19).
3.1. Resonance Magnetic Angiography
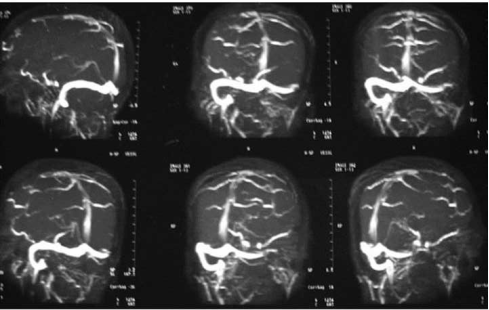
In 29 of all 32 patients (91%), RMA showed TSA in different patterns, affecting venous flow differently. Based on these patterns, we divided the patients into four classes according to anatomical and flow alterations (
Table 1,
Figure 1).
Table 1. Incidence of each anatomical variable of ST: Stage 0: no evidence of TS alteration. Stage 1: TS hypoplasia; evidence of a reduction in vessel size with no impact on blood flow. Stage 2: TS hypoplasia with evidence of inverted flow (from sigmoid sinus to crux cerebri). Stage 3: no evidence of blood flow in TS, compatible with atresia.
| STAGE 0 | STAGE 1 | STAGE 2 | STAGE 3 |
N patients | 3 | 18 | 7 | 4 |
Incidence percentage | 9% | 56% | 22% | 13% |
Figure 1. RMA of the intracranial circulation with evidence of no visualization of Transverse Sinus.
Therefore, attention was paid to the possible concordance between the side of the anatomical alteration and the side affected by Menière syndrome.
The side of TS’ alteration in RMA has been evaluated: 24 (83%) Left TS’ hypoplasia and 5 (17%) Right TS’ hypoplasia. No patient has reported being previously diagnosed with TS hypoplasia.
The side of TS alteration has been related to the side of the MD to determine if there could be a side association.
1) Between 29 patients, all 24 patients with LEFT TSA have shown RIGHT MD (100%);
2) Of the 5 patients with right TSA, 3 (60%) showed left MD, and 2 (40%) showed bilateral MD.
3.2. Transcranial Colour Doppler Ultrasound
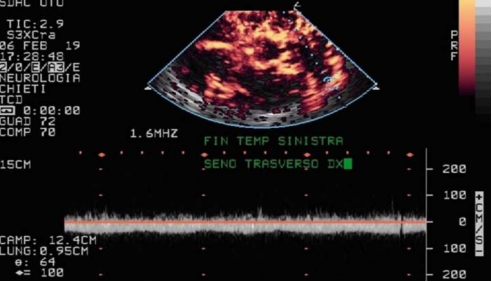
In association with RMA, we evaluated a randomised subgroup of 15 patients using TCD with SonoVue MDC ultrasound. In 10 cases, an acoustic window suitable for the study was visible. At the same time, in the remaining five subjects, the degree of mastoid ossification prevented high-frequency ultrasound from passing. We considered three parameters: identification of the presence/absence of the TS, observation of vessel patency, and the orthodromic/antidromic nature of the flow (
Figure 2). In these 10 cases, we obtained results consistent with RMA.
Figure 2. Late phase TCD analysis with ROI on the right transverse sinus.
3.3. VEMPS
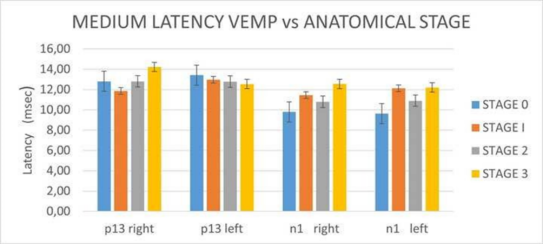
We considered the periods of the latency of p13 (c-VEMPS) and n1 (o-VEMPS) and related the results to the anatomical classes (
figure 3).
Figure 3. Relationship between medium latency of Vemps and anatomical stage. Bilaterally n1: MANOVA is not significant.
3.4. Audiometry
The right ear analysis shows a progressive increase in hearing threshold, directly proportional to the progression through the stages of RMA. The left ear analysis shows an uneven trend in the hearing threshold. The sample size needs to be larger to obtain statistically significant data.
3.5. VNS
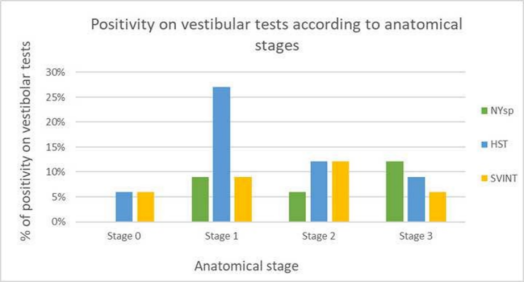
The VNS examination provides a qualitative assessment of the patient's vestibular condition. Three main parameters were considered: HST, SVINT, and spontaneous nystagmus (NYsp) in relation to the anatomical stage (
Figure 4). In particular, the presence/absence of NYsp in the different positions of examination, the presence/absence of HST Ny and the presence/absence of SVINT. In the present study, conducted on 33 patients, it was possible to identify NYsp in 9 patients (27%), while 12 presented with SVINT (36%) and 18 had post-impulsive HST NY (54%).
Figure 4. Positivity on vestibular tests according to anatomical stages.
4. Discussion
The association between migraine and MD is well known and has been described in literature that considers migrainous patients to have a 1.95-fold higher risk of developing MD
. Our study, however, focused on Menière's syndrome associated with non-migrainous headache and its correlation with the intracranial venous system, which has been widely shown to be a contributory cause of Menière's disease
| [25] | Attanasio G, Califano L, Bruno A, Giugliano V, Ralli M, Martellucci S, Milella C, de Vincentiis M, Russo FY, Greco A. Chronic cerebrospinal venous insufficiency and menière's disease: Interventional versus medical therapy. Laryngoscope. 2020 Aug; 130(8): 2040-2046. https://doi.org/10.1002/lary.28389 |
| [26] | Filipo R, Ciciarello F, Attanasio G, Mancini P, Covelli E, Agati L, Fedele F, Viccaro M. Chronic cerebrospinal venous insufficiency in patients with Ménière's disease. Eur Arch Otorhinolaryngol. 2015 Jan; 272(1): 77-82. https://doi.org/10.1007/s00405-013-2841-1 Epub 2013 Dec 7. |
| [27] | Di Berardino F, Alpini DC, Bavera PM, Cecconi P, Farabola M, Mattei V, Ambrosetti U, Cesarani A. Chronic cerebrospinal venous insufficiency in Ménière disease. Phlebology. 2015 May; 30(4): 274-9. https://doi.org/10.1177/0268355514526871 |
[25-27]
. The MD diagnosis can be efficiently conducted through the above vestibular and audiological tests; the TSA can be evaluated with angiography and TCD. The symptoms are comparable to those associated with headaches, which do not meet the minimum criteria for a migraine diagnosis, according to the IHS. In the context of non-migraine headaches related to Menière’s syndrome, we believe that attention should be paid to alterations in the efferent cerebrovascular system, particularly the venous system (TS). Our result shows that MD patients with non-migrainous headaches strongly correlate with TSA (88%). (
Table 2)
Table 2. HEADACHE Results of statistical comparison with MANOVA p<0.05 F(3,32)=1350.65. and Post-hoc ANOVA analysis between the stages of venous alterations. The values of normality and homogeneity between samples were considered. Normality Shapiro-Wilk test W= 0.798. Homogeneity of variance Levene’s Test p=0.492.
HEADACHE | F | p |
stage 0 vs. 1 | (1.5) 355.55 | <0.05 |
stage 0 vs. 2 | (1,9) 832.13 | <0.05 |
stage 0 vs. 3 | (1,20) 2373.80 | <0.05 |
stage 1 vs. 2 | (1,11) 390 | <0.05 |
stage 1 vs. 3 | (1,22) 2041.01 | <0.05 |
stage 2 vs. 3 | (1.26) 804.05 | <0.05 |
We have determined the association between the two phenomena and the side of MD. We found that in the population studied, all samples have MD contralateral to hypoplasia or absent TS. This asymmetry causes low flow on the hypoplastic side, and to compensate, a contralateral increase in venous pressure occurs, which in turn increases vessel size. This amount of pressure, even if not elevated, may lead to venous blood stasis and reflow of toxic metabolites in the inner ear due to the opening of secondary capillary circulation, resulting in stasis with portalization of the entire inner ear venous system
. Inner ear sensory cells are highly susceptible to the action of toxic products of degradation, which may be a determinant of vestibular damage and ultimately lead to EH. TSA may act as a predisposition factor for MD development, perhaps at a younger age and with specific manifestations or prodromic syndromes, such as an increase in headache or tinnitus. It has been demonstrated in several studies that altered venous outflow determines alterations in Cerebrospinal fluid dynamics (CSF) [4], which can be assessed using MRI to analyse flow velocity at the level of the Sylvian aqueduct
| [29] | Beggs CB, Magnano C, Shepherd SJ, Marr K, Valnarov V, Hojnacki D, Bergsland N, Belov P, Grisafi S, Dwyer MG, Carl E, Weinstock-Guttman B, Zivadinov R. Aqueductal cerebrospinal fluid pulsatility in healthy individuals is affected by impaired cerebral venous outflow. J Magn Reson Imaging. 2014 Nov; 40(5): 1215-22. https://doi.org/10.1002/jmri.24468 |
[29]
. These alterations can determine the onset of CSF stasis, leading to the development of headache and altered perilymph outflow in direct continuity with the CSF system via the vestibular aqueduct.
In 83% of the patients considered, the hypoplasia affects the left TS. As is well known in the literature
| [6] | Li J, Jin X, Kong X, Hu N, Li X, Wang L, Liu M, Li C, Liu Y, Sun L, Gong R. Correlation of endolymphatic hydrops and perilymphatic enhancement with the clinical features of Ménière's disease. Eur Radiol. 2024 Feb 3. https://doi.org/10.1007/s00330-024-10620-y Epub ahead of print. |
[6]
, dysembryogenetic and thrombotic manifestations are more frequent in the left TS; however, a univocal explanation for this phenomenon has not yet been established. The compensation of the contralateral sinus effectively supports the flow, albeit slowly; however, it indirectly causes venous stasis in the ear contralateral to the hypoplasia. To this pathophysiological mechanism, which alone is not sufficient for MD to manifest itself, it is hypothesised that in the long term, the hydrops characteristic of MD may be added to the physiopathology; therefore, continuous cycles of increased endolymphatic pressure ultimately determine damage to the inner ear. However, an analysis of the incidence percentages of Menière’s syndrome in patients with alterations of the right TS (17%) offers a significant clue for consideration. As the monolateral concordance between the side of anatomical alteration and the contralateral onset of Menière syndrome exists, a fair percentage of the subgroup mentioned above (40%) presents evidence of bilateral disease. A possible explanation for the damage ipsilateral to the lesion could lie in the fact that the compensation may not be entirely adequate, leading to the onset of slowed venous outflow and blood stasis in the relevant areas.
We, therefore, wanted to observe whether the MR Angiography method, which represents the diagnostic gold standard, was comparable to another imaging method, such as TCD with SonoVue® ultrasound MDC, by evaluating three parameters: the ability to identify the presence/absence of the TS, the possibility of observing the vessel's patency, and the orthodromic/antidromic flow’s nature.
Table 3. RM ANGIOGRAPHY. Results of statistical comparison with MANOVA p<0.05 F(3,25)=1065.86. and Post-hoc ANOVA analysis between the stages of venous alterations. The values of normality (Shapiro-Wilk test W= 0.746) and homogeneity (variance Levene’s Test p=0.807) between samples were considered.
RM ANGIOGRAPHY | F | p |
stage 0 vs. 1 | (1,17) | 275.94 | <0.05 |
stage 0 vs. 2 | (1,5) | 1422.22 | <0.05 |
stage 0 vs. 3 | (1,5) | 3200 | <0.05 |
stage 1 vs. 2 | (1,19) | 520.07 | <0.05 |
stage 1 vs. 3 | (1,19) | 2039.37 | <0.05 |
stage 2 vs. 3 | (1.7) | 600 | <0.05 |
We evaluated a randomized subgroup of 15 patients with this method. In 10 cases, an acoustic window suitable for the study was visible, while in the remaining five subjects, the degree of mastoid ossification prevented the passage of high-frequency ultrasound. On the other hand, TCD didn’t show any limitations in its execution, and it also demonstrated the possibility of being performed risk-free in patients with Gadolinium intolerance due to nephrogenic systemic fibrosis, exploiting the intrinsic contrast of moving structures such as the blood.
The specificity will not be examined as it cannot be accurately assessed based on necessary epidemiological criteria; however, the sensitivity will be evaluated. Based on the data analysis, the TCD showed a sensitivity of 61.5%, with a confidence interval of 52% to 70%. However, the data also indicate that the TCD has lower sensitivity, which can be attributed to specific characteristics of the region under study. As the patient ages, there is a decrease in sensitivity, which worsens particularly from the age of 70. This decrease is an inverse linear function. Even with high-frequency probes and ultrasound contrast medium, bypassing the temporal bone and accessing a bony window is impossible, resulting in an almost complete loss of visibility
. As we age, the mastoid bone in our body deposits and progresses, leading to a phenomenon. This phenomenon is known to occur regardless of the degree of systemic ossification. Another relevant limitation of transcranial Doppler (TCD) is that it is operator-dependent, and that the ultrasound contrast medium is contraindicated in patients with significant arteriovenous shunts and severe respiratory insufficiency. On the other hand, the benefits of using a contrast medium include its simplicity of administration and intrinsic safety, which does not require a preliminary evaluation of renal function. The procedure can be safely performed on patients with significant reductions in GFR. In addition, TCD can be used to evaluate the time it takes for the contrast agent to enter the tissue, the time it takes for the contrast to reach the perfusion window and the time it takes for the contrast to wash out of the tissue. These measurements can help identify pathological conditions that may cause a decrease or slowing of venous outflow, as observed in the patients studied (
Table 4).
Table 4. TCD/RM Results of statistical comparison with MANOVA p<0.05 F(3,32)=1157.6. and Post-hoc ANOVA analysis TCD/RM between the stages of venous alterations. The values of normality and homogeneity between samples were considered. Normality Shapiro-Wilk test W= 0.859. Homogeneity of variance Levene’s Test p=0.807.
TCD/RM | F | p |
stage 0 vs. stage 1 | (1,21) | 469.61 | <0.05 |
stage 0 vs. stage 2 | (1,10) | 1217.55 | <0.05 |
stage 0 vs. stage 3 | (1,7) | 2311.74 | <0.05 |
stage 1 vs. stage 2 | (1,24) | 809.71 | <0.05 |
stage 1 vs. stage 3 | (1,21) | 2200.58 | <0.05 |
stage 2 vs. stage 3 | (1.10) | 343.71 | <0.05 |
The analysis of hearing loss patterns (audiometry) revealed sensorineural deficits in the patients, which were then studied using the values expressed in decibels for each sound band. We have investigated the relationship between the frequency under examination and the degree of alteration of the TS. It is possible to notice an increase in the acoustic threshold according to the diagnostic stage, particularly for the right side, coherently with the increased percentage of patients who present a left anatomical anomaly and manifest right MD, as previously demonstrated. Furthermore, this correlation's weakness and heterogeneity reside primarily in the intrinsic characteristic of Menière syndrome, i.e., the instability of the hearing loss until the late stages of the pathology. The correlation would acquire greater strength and accuracy if it were possible to identify the phase in which the audiometric test is conducted. Still, in MD, this is difficult, if not almost impossible.
The modifications of evoked potentials (Vemps), according to Giuliano
| [31] | Giuliano D. A., Gallina S., Speciale R., Cupido G., Restivo S. Analisi dei potenziali evocati miogeni nelle turbe dell'equilibrio.” Otorinolaringoiatria, 2002. September; 52(3): 101-6. |
[31]
, in the acute phase show an increased pattern in 59% of cases and a non-evocable pattern in 12%; in the intercritical phase, a pathological pattern is found in only 18% of patients. Therefore, a correlation with the acute event would be more specific but is prospectively difficult as the acute/subacute phase is difficult to observe. In the present study, however, we found that the anatomical changes of the TS correlate to the alterations of the Vemps, particularly in classes 1 and 2 on the left (
Tables 5, 6).
Table 5. LATENCY p13 RIGHT. Results of statistical comparison with MANOVA p<0.05 F(3,32)=3.580 and Post- hoc ANOVA analysis between the stages of venous alterations. The values of normality and homogeneity between samples were considered. Normality Shapiro-Wilk test W= 0.919. Homogeneity of variance Levene’s Test p=0.200. ANOVA is insignificant for stage 0 vs. 2, 1 vs. 3, and 2 vs. 3 comparisons.
LATENCY p13 RIGHT | F | p |
stage 0 vs. 1 | (1,21) 5.998 | <0.05 |
stage 0 vs. 3 | (1,7) 6.419 | <0.05 |
stage 1 vs. 2 | (1,24) 4.909 | <0.05 |
Table 6. LATENCY p13 LEFT Results of statistical comparison with MANOVA p<0.05 F(3,32)= 4.037 and Post-hoc ANOVA analysis between the stages of venous alterations. The values of normality and homogeneity between samples were considered. Normality Shapiro-Wilk test W= 0.897. Homogeneity of variance Levene’s Test p=0.100. For stage 0vs.2, 0vs.2, 0vs.3, 1vs.3, 2vs.3 comparisons: ANOVA is not significant.
LATENCY p13 LEFT | F | p |
stage 1 vs. 2 | (1,24) 5.6408 | <0.05 |
The search for NYsp is essential as it is an irritative sign typical of a subacute phase or relevant/advanced pathology. SVINT represents the result of very high-frequency stimulation, and its presence indicates vestibular injury affecting at least 50% of the labyrinthine reactive capacity. Studying the global function of the vestibular system even during a crisis is possible. According to the literature, the most helpful proof (HST) has shown an inhomogeneous pattern
| [32] | Di Stadio A, Ricci G, Ralli M, Paolo T, Agostini G, Faralli M. Head-Shaking Nystagmus in the Early Stage of Unilateral Meniere's Disease. J Int Adv Otol. 2019 Dec; 15(3): 425-430. https://doi.org/10.5152/iao.2019.7338 |
[32]
. This says that HST progressively turns negative during the natural history of the pathology as a compensatory phenomenon, while being frequently positive at first due to the imbalance of the two labyrinths. Ultimately, the most significant association concerns the post-impulsive test, which classically shows a reversal of NYsp, typical of MD we observed. SVINT in the patients studied is also significant
| [33] | Teggi R, Gatti O, Familiari M, Cangiano I, Bussi M. Skull Vibration-Induced Nystagmus Test (SVINT) in Vestibular Migraine and Menière's Disease. Audiol Res. 2021 Nov 8; 11(4): 603-608. https://doi.org/10.3390/audiolres11040054 |
[33]
. The correlation of the tests examined with the anatomical class evaluated in RMA showed an overall increase in incidence as a function of the progression of the anatomical variant, which is more pronounced for NYsp (
figure 4).
5. Limit of Study
The data we have collected, and the study involve a small number of patients. This could be a limitation of the study; therefore, our next step is to continue the study by expanding the number of subjects examined and exploring the potential use of instrumental diagnosis as a preventive measure in the development of MD associated with TS’s anatomical alterations.
6. Conclusion
In conclusion, MD diagnosis, when associated with non-migrainous headache, among the many clinical pathological conditions that contribute to it, must also recognize the presence of cerebral venous disorders, particularly of the TS which is frequently associated with headache. Hypoplasia of this important endocranial vessel causes a slower flow and hypertension in the contralateral sinus, which dilates to compensate. This imbalance in venous outflow necessarily results in reduced outflow of the Aqueduct vein, with upstream repercussions in the portal circle of the inner ear. Venous hypertension leads to the return of degradation products and toxic metabolites into endolymphatic circulation, as described in the literature
. This reflux can cause the onset of hydrops on the side, presenting with a dilated vessel. However, according to the data from the present study, this mechanism does not automatically result in the onset of MD. Not all the patients under study, although they had varying anatomical alterations of the TS, were clinically compatible with Menière. However, the onset of pathology is clearly correlated with the lesion’s site, particularly contralateral to the altered TS, in a considerable percentage of cases assumed to have bilateral character and clinical class in linear function with the degree of anatomical alteration. For this reason, the grading system of alterations in TCD and RMA of the TS has acquired a prognostic tool in characterising the Menière patients. This study aims to suggest a follow-up of all patients with anatomical abnormalities of the TS to prevent the onset of hydropic damage. This study also highlights the importance of RMA, which should be performed in all MD cases to facilitate better framing and more targeted follow-up therapy.
The goal of our study and its conclusion can be the first step to increase the focus on the venous vascular hypothesis related to the MD’s pathogenesis, thus allowing a proportional increase in early-stage diagnosis [34]. We have demonstrated that evaluating the sigmoid and transverse sinuses in all patients with menière-like symptoms is necessary, particularly when headache coexists. This study could serve as a starting point for future research in this area. The early diagnosis can develop appropriate therapies to prolong the inter-critical phase, if not its eradication while reducing its related auditory, vestibular, psychological, and social complications.
Abbreviations
MD | Menière's Disease |
EH | Endolymphatic Hydrops |
TSA | Transverse Sinus Asymmetries |
TS | Transverse Sinus |
MR | Magnetic Resonance |
VHIT | Video Head Impulse Test |
oVEMPS | ocular Vestibular Evoked Myogenic Potentials |
cVEMPS | Cervical Evoked Myogenic Vestibular Potentials |
RMA | RM Angiography |
TCD | Transcranial Colour Doppler Ultrasound |
SVINT | Skull Vibration-Induced Ny Test |
HST | Head Shaking Test |
VNS | Video Nystagmus Scope |
BE | Bedside Exam |
VOR | Vestibulo-Ocular Reflex |
Informed Consent Statement
All participants gave informed consent before data collection, according to the current ethical laws, and all tests were performed according to the Helsinki II Declaration.
Institutional Review Board Statement
This study does not require ethical approval. Data Availability Statement: University of Chieti-Pescara, ENT Unit.
Author Contributions
Giampiero Neri: Conceptualization, Methodology, Writing - original draft preparation, Writing - review and editing, Supervision
Letizia Neri: Writing - review and editing, Supervision
Giovanni Sanese: Methodology, Data collecting
Klajdi Xhepa: Writing - original draft preparation, Supervision
Andrea Mazzatenta: Formal analysis and investigation
Anna Rita Fetoni: Funding acquisition
Giuseppe Chiarella: Data collecting, Funding acquisition
Funding
This research was funded “dall’Unione europea- Next Generation EU, Missione 4 Componente 1 CUP D53D23021460001 project P20222CZJB—Vestibular Migraine or Menière’s Disease? New insights by the VIP Project (proteomics, volabolomics, imaging) (DD n. 1409 14 September 2022).
Conflicts of Interest
All authors declare no conflicts of interest.
References
| [1] |
Alexander TH, Harris JP. Current epidemiology of Meniere's syndrome. Otolaryngol Clin North Am. 2010 Oct; 43(5): 965-70.
https://doi.org/10.1016/j.otc.2010.05.001
|
| [2] |
Havia M, Kentala E, Pyykkö I. Prevalence of Menière's disease in general population of Southern Finland. Otolaryngol Head Neck Surg. 2005 Nov; 133(5): 762-8.
https://doi.org/10.1016/j.otohns.2005.06.015
|
| [3] |
da Costa SS, de Sousa LC, Piza MR. Meniere's disease: overview, epidemiology, and natural history. Otolaryngol Clin North Am. 2002 Jun; 35(3): 455-95.
https://doi.org/10.1016/s0030-6665(02)00028-2
|
| [4] |
Attanasio G, Cagnoni L, Masci E, Ciciarello F, Diaferia F, et al. Chronic cerebrospinal venous insufficiency as a cause of inner ear diseases. Acta Otolaryngol. 2017 May; 137(5): 460-463.
https://doi.org/10.1080/00016489.2016.1252853
Epub 2016 Nov 16.
|
| [5] |
Committee on Hearing and Equilibrium guidelines for the diagnosis and evaluation of therapy in Meniere's disease. American Academy of Otolaryngology-Head and Neck Foundation, Inc, author. Otolaryngol Head Neck Surg. 1995; 113: 181–185.
|
| [6] |
Li J, Jin X, Kong X, Hu N, Li X, Wang L, Liu M, Li C, Liu Y, Sun L, Gong R. Correlation of endolymphatic hydrops and perilymphatic enhancement with the clinical features of Ménière's disease. Eur Radiol. 2024 Feb 3.
https://doi.org/10.1007/s00330-024-10620-y
Epub ahead of print.
|
| [7] |
Eklund S. Headache in Meniere's disease. Auris Nasus Larynx. 1999 Oct; 26(4): 427-33.
https://doi.org/10.1016/s0385-8146(99)00022-x
|
| [8] |
Iannachero, R. et al. Diagnosis and treatment of headache probably attributed to cerebral venous sinus thrombosis. Clinical Management Issues, [S.l.], v. 8, n. 4, p. 97-101, dec. 2014. ISSN 2283-3137. Date accessed: 19 jan. 2024. Available at:
https://doi.org/10.7175/cmi.v8i4.966
|
| [9] |
Alper F, Kantarci M, Dane S, et al. Importance of anatomical asymmetries of transverse sinuses: an MR venographic study. Cerebrovasc Dis 2004; 18: 236–9.
|
| [10] |
Capecchi M, Abbattista M, Martinelli I. Cerebral venous sinus thrombosis. J Thromb Haemost. 2018 Oct; 16(10): 1918-1931.
https://doi.org/10.1111/jth.14210
Epub 2018 Jul 11
|
| [11] |
International Headache Society: The International Classification of Headache Disorders 3ed.
|
| [12] |
Mamikoglu B, Algın O, Mengü G, Erdoğan-Küçükdağlı F, Kessler A. Transverse sinus pathologies, vestibular migraine and intracranial hypertension without papilledema. Am J Otolaryngol. 2023 Sep-Oct; 44(5): 103931.
https://doi.org/10.1016/j.amjoto.2023.103931
|
| [13] |
Belinchon A, Perez-Garrigues H, Tenias JM, Lopez A. Hearing assessment in Menière's disease. Laryngoscope. 2011 Mar; 121(3): 622-6.
https://doi.org/10.1002/lary.21335
|
| [14] |
Scarpa A, Gioacchini FM, Cassandro E, Tulli M, Ralli M, Re M, Cassandro C. Clinical application of cVEMPs and oVEMPs in patients affected by Ménière's disease, vestibular neuritis and benign paroxysmal positional vertigo: a systematic review. Acta Otorhinolaryngol Ital. 2019 Oct; 39(5): 298-307.
https://doi.org/10.14639/0392-100X-2104
|
| [15] |
Gazioglu S, Boz C. Ocular and cervical vestibular evoked myogenic potentials in multiple sclerosis patients. Clin Neurophysiol 2012; 123: 1872-9.
https://doi.org/10.1016/j.clinph.2012.01.022
|
| [16] |
Rosengren SM, Welgampola MS, Colebatch JG. Vestibular evoked myogenic potentials: past, present and future. Clin Neurophysiol 2010; 121: 636-51.
https://doi.org/10.1016/j.clinph.2009.10.016
|
| [17] |
Dorbeau C, Bourget K, Renard L, Calais C, Bakhos D. Vestibular evoked myogenic potentials. Eur Ann Otorhinolaryngol Head Neck Dis. 2021 Dec; 138(6): 483-488.
https://doi.org/10.1016/j.anorl.2021.01.001
Epub 2021 Jan 19.
|
| [18] |
Marcelli, Vincenzo. “VESTIBOLOGIA CLINICA.” 72. Cap. 15. NEMS-MNAMON Editor., 2021, ISBN 979-12-80296-10-8.
|
| [19] |
Van Esch BF, Abolhosseini K, Masius-Olthof S, van der Zaag-Loonen HJ, van Benthem PPG, Bruintjes TD. Video-head impulse test results in patients with Menière's disease related to duration and stage of disease. J Vestib Res. 2018; 28(5-6): 401-407.
https://doi.org/10.3233/VES-190654
|
| [20] |
Georges Dumas, Ian S Curthoys, Alexis Lion, Philippe Perrin, Sebastien Schmerber. The Skull vibration- induced Nystagmus Test of vestibular Function-A Review. Frontiers in Neurology, 2017, 8, pp. 41.
https://doi.org/10.3389/fneur.2017.00041
|
| [21] |
DUMAS Georges DUMAS, Christol FABRE, Flavio PEROTTINO, Haoyue TAN, Patrick PROY, Sébastien SCHMERBER Skull vibration induced nystagmus test in Menière’s disease Otorinolaringologia 2020 December; 70(4): 121-7
https://doi.org/10.23736/S0392-6621.20.02320-6
|
| [22] |
Han K, Chao AC, Chang FC, Hsu HY, Chung CP, Sheng WY, Chan L, Wu J, Hu HH. Diagnosis of Transverse Sinus Hypoplasia in Magnetic Resonance Venography: New Insights Based on Magnetic Resonance Imaging in Combined Dataset of Venous Outflow Impairment Case-Control Studies: Post Hoc Case-Control Study. Medicine (Baltimore). 2016 Mar; 95(10): e2862.
https://doi.org/10.1097/MD.0000000000002862
|
| [23] |
Purkayastha S, Sorond F. Transcranial Doppler ultrasound: technique and application. Semin Neurol. 2012 Sep; 32(4): 411-20.
https://doi.org/10.1055/s-0032-1331812
|
| [24] |
Kim SY, Lee CH, Yoo DM, et al. Association Between Meniere Disease and Migraine. JAMA Otolaryngol Head Neck Surg. 2022; 148(5): 457–464.
https://doi.org/10.1001/jamaoto.2022.0331
|
| [25] |
Attanasio G, Califano L, Bruno A, Giugliano V, Ralli M, Martellucci S, Milella C, de Vincentiis M, Russo FY, Greco A. Chronic cerebrospinal venous insufficiency and menière's disease: Interventional versus medical therapy. Laryngoscope. 2020 Aug; 130(8): 2040-2046.
https://doi.org/10.1002/lary.28389
|
| [26] |
Filipo R, Ciciarello F, Attanasio G, Mancini P, Covelli E, Agati L, Fedele F, Viccaro M. Chronic cerebrospinal venous insufficiency in patients with Ménière's disease. Eur Arch Otorhinolaryngol. 2015 Jan; 272(1): 77-82.
https://doi.org/10.1007/s00405-013-2841-1
Epub 2013 Dec 7.
|
| [27] |
Di Berardino F, Alpini DC, Bavera PM, Cecconi P, Farabola M, Mattei V, Ambrosetti U, Cesarani A. Chronic cerebrospinal venous insufficiency in Ménière disease. Phlebology. 2015 May; 30(4): 274-9.
https://doi.org/10.1177/0268355514526871
|
| [28] |
Friis M, Qvortrup K. A potential portal flow in the inner ear. Laryngoscope. 2007 Feb; 117(2): 194-8.
https://doi.org/10.1097/mlg.0b013e31802c028d
.
|
| [29] |
Beggs CB, Magnano C, Shepherd SJ, Marr K, Valnarov V, Hojnacki D, Bergsland N, Belov P, Grisafi S, Dwyer MG, Carl E, Weinstock-Guttman B, Zivadinov R. Aqueductal cerebrospinal fluid pulsatility in healthy individuals is affected by impaired cerebral venous outflow. J Magn Reson Imaging. 2014 Nov; 40(5): 1215-22.
https://doi.org/10.1002/jmri.24468
|
| [30] |
Marinoni M, Ginanneschi A, Forleo P, Amaducci L. Technical limits in transcranial Doppler recording: inadequate acoustic windows. Ultrasound Med Biol. 1997; 23(8): 1275-7.
https://doi.org/10.1016/s0301-5629(97)00077-x
|
| [31] |
Giuliano D. A., Gallina S., Speciale R., Cupido G., Restivo S. Analisi dei potenziali evocati miogeni nelle turbe dell'equilibrio.” Otorinolaringoiatria, 2002. September; 52(3): 101-6.
|
| [32] |
Di Stadio A, Ricci G, Ralli M, Paolo T, Agostini G, Faralli M. Head-Shaking Nystagmus in the Early Stage of Unilateral Meniere's Disease. J Int Adv Otol. 2019 Dec; 15(3): 425-430.
https://doi.org/10.5152/iao.2019.7338
|
| [33] |
Teggi R, Gatti O, Familiari M, Cangiano I, Bussi M. Skull Vibration-Induced Nystagmus Test (SVINT) in Vestibular Migraine and Menière's Disease. Audiol Res. 2021 Nov 8; 11(4): 603-608.
https://doi.org/10.3390/audiolres11040054
|
| [34] |
Oberman BS, Patel VA, Cureoglu S, Isildak H. The aetiopathologies of Ménière's disease: a contemporary review. Acta Otorhinolaryngol Ital. 2017 Aug; 37(4): 250-263.
https://doi.org/10.14639/0392-100X-793
|
Cite This Article
-
APA Style
Neri, G., Neri, L., Sanese, G., Xhepa, K., Mazzatenta, A., et al. (2025). Asymmetries of Transverse Sinuses in Patients with Menière Disease and Non-Migrainous Headache. American Journal of Internal Medicine, 13(3), 32-42. https://doi.org/10.11648/j.ajim.20251303.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Neri, G.; Neri, L.; Sanese, G.; Xhepa, K.; Mazzatenta, A., et al. Asymmetries of Transverse Sinuses in Patients with Menière Disease and Non-Migrainous Headache. Am. J. Intern. Med. 2025, 13(3), 32-42. doi: 10.11648/j.ajim.20251303.11
Copy
|
Download
AMA Style
Neri G, Neri L, Sanese G, Xhepa K, Mazzatenta A, et al. Asymmetries of Transverse Sinuses in Patients with Menière Disease and Non-Migrainous Headache. Am J Intern Med. 2025;13(3):32-42. doi: 10.11648/j.ajim.20251303.11
Copy
|
Download
-
@article{10.11648/j.ajim.20251303.11,
author = {Giampiero Neri and Letizia Neri and Giovanni Sanese and Klajdi Xhepa and Andrea Mazzatenta and Anna Rita Fetoni and Giuseppe Chiarella},
title = {Asymmetries of Transverse Sinuses in Patients with Menière Disease and Non-Migrainous Headache},
journal = {American Journal of Internal Medicine},
volume = {13},
number = {3},
pages = {32-42},
doi = {10.11648/j.ajim.20251303.11},
url = {https://doi.org/10.11648/j.ajim.20251303.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajim.20251303.11},
abstract = {Menière's disease (MD) is a chronic inner ear disorder characterised by vertigo, fluctuating hearing loss, and fullness, frequently associated with migraine. The aetiology of MD is multifactorial but unclear. Endolymphatic hydrops (EH) is the histopathological marker. The correlation between venous disorders and MD is described in the literature. Our study aims to evaluate the incidence of Transverse Sinus Asymmetries (TSA) in patients with Menière Disease (MD) and non-migrainous headaches to test a physiopathological hypothesis. Materials and Methods: We conducted a retrospective study of 32 patients with symptoms of MD and non-migrainous headaches who presented to TSA on Magnetic Resonance Imaging (MR). Each patient underwent clinical evaluation, Audiometry, impedanceometry, VHIT, VEMPS, RM Angiography (RMA), transcranial colour doppler ultrasound (TCD) to study the intracranial venous system and vascular flow. Results: All patients were diagnosed as probable in 41% and certain in 59%. On RMA results, 91% showed TSA. We propose four TSA stages. RMA showed 83% left TS hypoplasia and 17% right TS hypoplasia. All patients with TSA showed MD. Patients with left TSA showed right MD; patients with right TSA showed left or bilateral MD. We used TCD in 15 patients: 10 patients showed alteration or flow reversal. In 5 subjects was not possible due to mastoid ossification. Conclusions: Ultimately, a clear association exists between TS absence or hypoplasia in many Menière’s patients with non-migrainous headaches. Moreover, there is a correspondence between the side of MD and TSA, which is contralateral. Our study suggests to follow-up patients with TSA to prevent the onset of EH.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Asymmetries of Transverse Sinuses in Patients with Menière Disease and Non-Migrainous Headache
AU - Giampiero Neri
AU - Letizia Neri
AU - Giovanni Sanese
AU - Klajdi Xhepa
AU - Andrea Mazzatenta
AU - Anna Rita Fetoni
AU - Giuseppe Chiarella
Y1 - 2025/06/26
PY - 2025
N1 - https://doi.org/10.11648/j.ajim.20251303.11
DO - 10.11648/j.ajim.20251303.11
T2 - American Journal of Internal Medicine
JF - American Journal of Internal Medicine
JO - American Journal of Internal Medicine
SP - 32
EP - 42
PB - Science Publishing Group
SN - 2330-4324
UR - https://doi.org/10.11648/j.ajim.20251303.11
AB - Menière's disease (MD) is a chronic inner ear disorder characterised by vertigo, fluctuating hearing loss, and fullness, frequently associated with migraine. The aetiology of MD is multifactorial but unclear. Endolymphatic hydrops (EH) is the histopathological marker. The correlation between venous disorders and MD is described in the literature. Our study aims to evaluate the incidence of Transverse Sinus Asymmetries (TSA) in patients with Menière Disease (MD) and non-migrainous headaches to test a physiopathological hypothesis. Materials and Methods: We conducted a retrospective study of 32 patients with symptoms of MD and non-migrainous headaches who presented to TSA on Magnetic Resonance Imaging (MR). Each patient underwent clinical evaluation, Audiometry, impedanceometry, VHIT, VEMPS, RM Angiography (RMA), transcranial colour doppler ultrasound (TCD) to study the intracranial venous system and vascular flow. Results: All patients were diagnosed as probable in 41% and certain in 59%. On RMA results, 91% showed TSA. We propose four TSA stages. RMA showed 83% left TS hypoplasia and 17% right TS hypoplasia. All patients with TSA showed MD. Patients with left TSA showed right MD; patients with right TSA showed left or bilateral MD. We used TCD in 15 patients: 10 patients showed alteration or flow reversal. In 5 subjects was not possible due to mastoid ossification. Conclusions: Ultimately, a clear association exists between TS absence or hypoplasia in many Menière’s patients with non-migrainous headaches. Moreover, there is a correspondence between the side of MD and TSA, which is contralateral. Our study suggests to follow-up patients with TSA to prevent the onset of EH.
VL - 13
IS - 3
ER -
Copy
|
Download