Abstract
Background: Why promising health technology ventures stall between product development and real-world deployment remains insufficiently explained in entrepreneurship research. Market-centric models emphasize experimentation, customer discovery, and product-market fit, but these mechanisms are less explanatory where access to users, clinical settings, and procurement channels is institutionally mediated. Methods: This study develops a process explanation of venture progression in regulated health innovation settings. Drawing on institutional theory, innovation systems research, and process views of entrepreneurship, it uses a longitudinal comparative case design to analyze early-stage health technology ventures in Rwanda over an 18-month observation window. The empirical material comprises venture milestone plans, periodic progress reports, observational notes, and documented interactions with regulatory, clinical, and institutional actors. Results: Venture progression was not explained primarily by technical capability, entrepreneurial effort, or early market interest. Rather, outcomes varied according to whether ventures achieved coordinated validation across interdependent regulatory, clinical, and institutional domains. Three recurrent pathway configurations were identified: sequential alignment, associated with forward progression; temporally constrained alignment, associated with delayed progression despite coherent sequencing; and fragmented progression, associated with stagnation. The findings show that legitimacy in regulated health innovation settings is multi-domain, threshold-based, and time-dependent. Conclusion: The study advances the concept of coordinated validation under temporal constraint to explain how ventures move, or fail to move, from development to deployment when market entry depends on synchronized institutional approval. It contributes to entrepreneurship and innovation theory by reframing venture progression in regulated environments as a coordination problem rather than a pure capability problem. Rwanda serves as a revealing case because its comparatively coordinated health system makes the underlying synchronization problem especially visible.
Keywords
Health Technology Ventures, Venture Progression, Coordinated Validation, Institutional Theory, Digital Health Innovation,
Regulated Markets, Rwanda
1. Introduction
1.1. Background to the Study
Entrepreneurship scholarship has long explained early venture progress through opportunity recognition, iterative experimentation, and market learning. In this tradition, ventures advance by testing assumptions, revising products, and approaching product-market fit under uncertainty
| [4] | Autio, E., Kenney, M., Mustar, P., Siegel, D., & Wright, M. (2014). Entrepreneurial innovation: The importance of context. Research Policy, 43(7), 1097–1108.
https://doi.org/10.1016/j.respol.2014.01.015 |
| [6] | Blank, S. G. (2013). Why the lean start-up changes everything. Harvard Business Review, 91(5), 63–72.
https://hbr.org/2013/05/why-the-lean-start-up-changes-everything |
| [16] | McMullen, J. S., & Dimov, D. (2013). Time and the entrepreneurial journey: The problems and promise of studying entrepreneurship as a process. Journal of Management Studies, 50(8), 1481–1512. https://doi.org/10.1111/joms.12049 |
| [21] | Ries, E. (2011). The lean startup: How today's entrepreneurs use continuous innovation to create radically successful businesses. Crown Currency.
https://www.penguinrandomhouse.com/books/210088/the-lean-startup-by-eric-ries/ |
[4, 6, 16, 21]
. This analytical lens has been highly generative, but it assumes that ventures can access users, collect market feedback early, and translate internal learning into external traction. That assumption is increasingly fragile in sectors where market participation is conditioned by regulatory approval, professional gatekeeping, and institutional procurement.
Health technology is a particularly demanding case. New ventures do not simply persuade customers; they must also satisfy regulators, earn clinical trust, and fit within health system workflows and adoption channels. In low- and middle-income countries (LMICs), these demands are often compounded by limited interoperability, donor influence, fragmented service delivery, and procurement systems that reward institutional legitimacy more than entrepreneurial speed
| [3] | Aranda-Jan, C. B., Mohutsiwa-Dibe, N., & Loukanova, S. (2014). Systematic review on what works, what does not work and why of implementation of mobile health (mHealth) projects in Africa. BMC Public Health, 14, Article 188.
https://doi.org/10.1186/1471-2458-14-188 |
| [7] | Buse, K., Mays, N., & Walt, G. (2012). Making health policy (2nd ed.). Open University Press.
https://research.monash.edu/en/publications/making-health-policy-2/ |
| [10] | Greenhalgh, T., Wherton, J., Papoutsi, C., Lynch, J., Hughes, G., A'Court, C., Hinder, S., Fahy, N., Procter, R., & Shaw, S. (2017). Beyond adoption: A new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. Journal of Medical Internet Research, 19(11), e367. https://doi.org/10.2196/jmir.8775 |
| [29] | World Health Organization. (2021). Global strategy on digital health 2020–2025. https://iris.who.int/handle/10665/344249 |
[3, 7, 10, 29]
. As a result, technically promising ventures frequently become trapped between prototype development and sustained deployment. The recurring problem is visible in the digital health pilot trap, where innovations demonstrate feasibility but fail to travel into routine use at scale
. Recent systems work likewise argues that digital health produces limited value when technologies remain fragmented rather than connected across governance, service delivery, and financing structures, reinforcing the need to analyze venture progression as a coordination problem rather than a purely technical one
.
Rwanda is an especially relevant setting for this inquiry because current national health policy explicitly prioritizes research, innovation, regulation, and digitalization
, while the Ministry of Health’s digital health agenda emphasizes service accessibility, continuity of care, and evidence-based decision-making
. In such a policy environment, the key issue is not whether health innovation matters, but how promising ventures move through the institutional systems that govern authorization, clinical acceptance, and adoption. This current emphasis on innovation and digitalization also builds on Rwanda’s earlier National Digital Health Strategy, which already framed digital coordination and system integration as national priorities
.
1.2. Statement of the Problem
Existing explanations capture part of this story but not enough of it. Some studies emphasize resource scarcity, weak institutions, or infrastructural deficits
| [3] | Aranda-Jan, C. B., Mohutsiwa-Dibe, N., & Loukanova, S. (2014). Systematic review on what works, what does not work and why of implementation of mobile health (mHealth) projects in Africa. BMC Public Health, 14, Article 188.
https://doi.org/10.1186/1471-2458-14-188 |
| [8] | George, G., McGahan, A. M., & Prabhu, J. (2016). Innovation for inclusive growth: Towards a theoretical framework and a research agenda. Journal of Management Studies, 53(3), 497–512. https://doi.org/10.1111/joms.12181 |
| [27] | Webb, J. W., Khoury, T. A., & Hitt, M. A. (2020). The influence of formal and informal institutional voids on entrepreneurship. Entrepreneurship Theory and Practice, 44(3), 504–526.
https://doi.org/10.1177/1042258719830310 |
[3, 8, 27]
. Others focus on entrepreneurial agility, business model experimentation, or ecosystem interdependence
| [1] | Adner, R. (2017). Ecosystem as structure: An actionable construct for strategy. Journal of Management, 43(1), 39–58.
https://doi.org/10.1177/0149206316678451 |
| [2] | Adner, R., & Kapoor, R. (2016). Innovation ecosystems and the pace of substitution: Re-examining technology S-curves. Strategic Management Journal, 37(4), 625–648.
https://doi.org/10.1002/smj.2363 |
| [5] | Autio, E., Nambisan, S., Thomas, L. D. W., & Wright, M. (2018). Digital affordances, spatial affordances, and the genesis of entrepreneurial ecosystems. Strategic Entrepreneurship Journal, 12(1), 72–95. https://doi.org/10.1002/sej.1266 |
| [6] | Blank, S. G. (2013). Why the lean start-up changes everything. Harvard Business Review, 91(5), 63–72.
https://hbr.org/2013/05/why-the-lean-start-up-changes-everything |
| [21] | Ries, E. (2011). The lean startup: How today's entrepreneurs use continuous innovation to create radically successful businesses. Crown Currency.
https://www.penguinrandomhouse.com/books/210088/the-lean-startup-by-eric-ries/ |
[1, 2, 5, 6, 21]
. These literatures are important, yet they often treat barriers as static conditions or capabilities as portable solutions.
They say less about how ventures actually progress through regulated environments over time, especially when progress in one domain is meaningless unless another domain also moves. The central problem, therefore, is that the literature still does not adequately explain how early-stage health technology ventures move, stall, or fail when meaningful deployment depends on interdependent regulatory, clinical, and institutional validation rather than on market experimentation alone.
1.3. Research Objectives
The general objective of this study is to explain how early-stage health technology ventures in Rwanda progress toward deployment through interdependent regulatory, clinical, and institutional validation systems. Empirically, the study draws on longitudinal evidence from early-stage health technology ventures in Rwanda observed over an 18-month period. Rwanda is analytically valuable not because it is typical of all health systems, but because its comparatively coordinated governance structure makes institutional interdependencies especially visible
| [17] | Ministry of Health, Rwanda. (2024). Health Sector Strategic Plan V (2024/25–2028/29). https://www.moh.gov.rw/fileadmin/user_upload/Moh/Publications/Reports/new_annual_Report/HSSP_V_signed.pdf |
| [22] | Rudasingwa, M., Jahn, A., Uwitonze, A.-M., & Hennig, L. (2022). Increasing health system synergies in low-income settings: Lessons learned from a qualitative case study of Rwanda. Global Public Health, 17(12), 3303–3321.
https://doi.org/10.1080/17441692.2022.2129726 |
[17, 22]
.
The study’s specific objectives were:
To examine how early-stage health technology ventures progress through interdependent validation systems under institutional complexity. | [2] | Adner, R., & Kapoor, R. (2016). Innovation ecosystems and the pace of substitution: Re-examining technology S-curves. Strategic Management Journal, 37(4), 625–648.
https://doi.org/10.1002/smj.2363 |
1.4. Research Questions
RQ1. How do early-stage health technology ventures progress through interdependent validation systems under institutional complexity? RQ2. How do regulatory, clinical, and institutional actors shape the pace and direction of that progression?
1.5. Significance of the Study
This study makes three contributions. First, it reframes venture progression in regulated environments as a coordination problem rather than a pure capability problem. Second, it introduces the mechanism of coordinated validation under temporal constraint, showing that progression depends on synchronizing multiple externally governed validation processes. Third, it extends institutional and ecosystem research by showing that legitimacy in regulated innovation systems is not a single stock of approval but a multi-domain, threshold-based condition that must be achieved in aligned sequence. The paper proceeds by reviewing the relevant literature, developing the conceptual framework of institutionally mediated market formation, outlining the longitudinal case design, presenting the cross-case findings, and discussing the theoretical and practical implications.
2. Literature Review and Theoretical Background
2.1. Health Technology Innovation as Institutionally Mediated Market Formation
Health technology innovation does not unfold in a purely market setting. Unlike consumer or enterprise software ventures that can often place products directly in users’ hands, health technology ventures must engage systems of clinical governance, regulation, and institutional adoption before they can test, diffuse, and monetize their offerings. Access to users is therefore mediated, not open. The relevant market is partly constructed by ministries, hospitals, professional bodies, ethics review processes, procurement systems, and reimbursement arrangements. In such settings, the route to deployment is shaped as much by institutional permission as by market pull
| [7] | Buse, K., Mays, N., & Walt, G. (2012). Making health policy (2nd ed.). Open University Press.
https://research.monash.edu/en/publications/making-health-policy-2/ |
| [10] | Greenhalgh, T., Wherton, J., Papoutsi, C., Lynch, J., Hughes, G., A'Court, C., Hinder, S., Fahy, N., Procter, R., & Shaw, S. (2017). Beyond adoption: A new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. Journal of Medical Internet Research, 19(11), e367. https://doi.org/10.2196/jmir.8775 |
| [29] | World Health Organization. (2021). Global strategy on digital health 2020–2025. https://iris.who.int/handle/10665/344249 |
[7, 10, 29]
.
LMIC health innovation settings sharpen this point. Digital and health technology ventures often confront fragmented service platforms, uneven technical infrastructure, short funding horizons, and dependence on institutional buyers or implementation partners rather than individual consumers
| [3] | Aranda-Jan, C. B., Mohutsiwa-Dibe, N., & Loukanova, S. (2014). Systematic review on what works, what does not work and why of implementation of mobile health (mHealth) projects in Africa. BMC Public Health, 14, Article 188.
https://doi.org/10.1186/1471-2458-14-188 |
| [8] | George, G., McGahan, A. M., & Prabhu, J. (2016). Innovation for inclusive growth: Towards a theoretical framework and a research agenda. Journal of Management Studies, 53(3), 497–512. https://doi.org/10.1111/joms.12181 |
| [29] | World Health Organization. (2021). Global strategy on digital health 2020–2025. https://iris.who.int/handle/10665/344249 |
[3, 8, 29]
. Yet research still tends to describe these conditions as contextual difficulty rather than theorize how they structure venture progression itself. The result is a conceptual gap between what health systems do to ventures and how ventures move through those conditions over time.
These institutional dynamics should not be treated as background frictions that appear only after a technology is built. They are constitutive of market formation itself because they shape whether innovations can be connected to service delivery, governance, and financing structures in the first place. In that sense, the relevant market is not merely discovered by the venture; it is assembled through institutional coordination.
2.2. Limits of Market-Centric Venture Development Models
Dominant models of venture development assume that ventures can learn by direct exposure to markets. The lean start-up tradition, for example, privileges rapid experimentation, minimum viable products, customer discovery, and iterative pivoting as the route to progress
. These ideas remain influential because they identify a powerful logic of disciplined learning under uncertainty. But their explanatory reach narrows where ventures cannot interact with end users or institutional buyers without prior approval. In health technology, validation cannot begin and end with customer willingness to pay; it must also include safety, efficacy, workflow fit, and system compatibility.
Research on innovation ecosystems adds a useful corrective by emphasizing interdependence among multiple actors whose coordinated participation shapes value creation
| [1] | Adner, R. (2017). Ecosystem as structure: An actionable construct for strategy. Journal of Management, 43(1), 39–58.
https://doi.org/10.1177/0149206316678451 |
| [2] | Adner, R., & Kapoor, R. (2016). Innovation ecosystems and the pace of substitution: Re-examining technology S-curves. Strategic Management Journal, 37(4), 625–648.
https://doi.org/10.1002/smj.2363 |
| [5] | Autio, E., Nambisan, S., Thomas, L. D. W., & Wright, M. (2018). Digital affordances, spatial affordances, and the genesis of entrepreneurial ecosystems. Strategic Entrepreneurship Journal, 12(1), 72–95. https://doi.org/10.1002/sej.1266 |
| [13] | Jacobides, M. G., Cennamo, C., & Gawer, A. (2018). Towards a theory of ecosystems. Strategic Management Journal, 39(8), 2255–2276. https://doi.org/10.1002/smj.2904 |
[1, 2, 5, 13]
. Even so, much of this literature still leaves underdeveloped the problem of ventures that face delayed or conditional access to the very relationships through which ecosystem coordination would normally unfold. Interdependence is acknowledged, but the process through which ventures secure permission to participate in the ecosystem is not fully explained.
2.3. Institutional Complexity and Asynchronous Validation Systems
Institutional theory offers a more suitable starting point because it treats organizational action as shaped by formal rules, normative expectations, and culturally supported conceptions of appropriateness
. In health technology settings, however, the issue is not simply institutional constraint in the abstract. Ventures confront multiple validation domains, each with its own logic, evidence requirements, and timing. These domains are also shaped by distinct institutional logics, meaning that endorsement from one class of actors can enable innovation while still leaving other forms of legitimacy unresolved
| [20] | Pahnke, E. C., Katila, R., & Eisenhardt, K. M. (2015). Who takes you to the dance? How partners’ institutional logics influence innovation in young firms. Administrative Science Quarterly, 60(4), 596–633.
https://doi.org/10.1177/0001839215592913 |
[20]
. Regulatory actors prioritize compliance and safety. Clinical actors privilege efficacy, professional judgment, and workflow fit. Institutional adopters, including hospitals and public agencies, are concerned with procurement feasibility, integration, and operational sustainability. Progress in one domain does not automatically unlock the others.
This produces asynchronous validation systems. Ventures may have a technically mature prototype but lack regulatory clearance. They may secure regulatory recognition but still fail to persuade clinicians. Or they may obtain clinical interest without a procurement pathway capable of supporting deployment. The challenge is therefore not a single legitimacy deficit but a problem of cross-domain alignment. This insight also refines work on institutional voids in emerging markets. In the present context, the decisive problem is often not missing institutions but overlapping institutions whose criteria and rhythms are not naturally synchronized
| [24] | Scott, W. R. (2014). Institutions and organizations: Ideas, interests, and identities (4th ed.). SAGE Publications.
https://collegepublishing.sagepub.com/products/institutions-and-organizations-4-237665 |
| [27] | Webb, J. W., Khoury, T. A., & Hitt, M. A. (2020). The influence of formal and informal institutional voids on entrepreneurship. Entrepreneurship Theory and Practice, 44(3), 504–526.
https://doi.org/10.1177/1042258719830310 |
[24, 27]
.
2.4. Business Model Formation Under Institutional Mediation
These dynamics also shape business model formation. Health technology ventures seldom monetize through simple direct exchange between founder and end user. Revenue often depends on hospitals, governments, insurers, donors, or hybrid partnerships. Consequently, business models are not merely commercial choices made after a product exists; they are co-produced by the same validation processes that determine whether the venture can enter the field at all. Claims about value proposition, customer, payer, and route to scale are inseparable from regulatory clearance, clinical acceptance, and institutional onboarding
| [3] | Aranda-Jan, C. B., Mohutsiwa-Dibe, N., & Loukanova, S. (2014). Systematic review on what works, what does not work and why of implementation of mobile health (mHealth) projects in Africa. BMC Public Health, 14, Article 188.
https://doi.org/10.1186/1471-2458-14-188 |
| [12] | Hwang, J., & Christensen, C. M. (2008). Disruptive innovation in health care delivery: A framework for business-model innovation. Health Affairs, 27(5), 1329–1335.
https://doi.org/10.1377/hlthaff.27.5.1329 |
[3, 12]
.
That point matters theoretically because it means business model uncertainty is downstream from validation uncertainty. Ventures do not simply ask who will pay. They first confront the prior question of who is permitted to use, recommend, authorize, and purchase the solution. That ordering problem is under-theorized in standard venture development models.
2.5. From the Pilot Trap to the Deployment Problem
The digital health literature has extensively described the distance between innovation and scale, often under the rubric of failed pilots, weak sustainability, or poor integration
| [10] | Greenhalgh, T., Wherton, J., Papoutsi, C., Lynch, J., Hughes, G., A'Court, C., Hinder, S., Fahy, N., Procter, R., & Shaw, S. (2017). Beyond adoption: A new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. Journal of Medical Internet Research, 19(11), e367. https://doi.org/10.2196/jmir.8775 |
| [14] | Labrique, A., Vasudevan, L., Chang, L. W., & Mehl, G. (2013). H_pe for mHealth: More “y” or “o” on the horizon? International Journal of Medical Informatics, 82(5), 467–469.
https://doi.org/10.1016/j.ijmedinf.2012.11.016 |
| [29] | World Health Organization. (2021). Global strategy on digital health 2020–2025. https://iris.who.int/handle/10665/344249 |
[10, 14, 29]
. Yet most of that literature is stronger at explaining why deployed initiatives do not scale than at explaining why ventures struggle to reach meaningful deployment in the first place. The distinction is analytically important. The mechanisms that shape pre-deployment progression are not identical to those that shape post-deployment diffusion. A venture may fail before scale becomes relevant.
This study therefore shifts attention upstream. It asks how ventures construct a pathway to initial deployment in contexts where market access is institutionally mediated and where validation occurs across multiple, interdependent domains.
2.6. Research Gap and Positioning
Taken together, the literature suggests three unresolved issues. First, much work remains factor-based, cataloguing obstacles without tracing how ventures move through them over time
| [3] | Aranda-Jan, C. B., Mohutsiwa-Dibe, N., & Loukanova, S. (2014). Systematic review on what works, what does not work and why of implementation of mobile health (mHealth) projects in Africa. BMC Public Health, 14, Article 188.
https://doi.org/10.1186/1471-2458-14-188 |
| [8] | George, G., McGahan, A. M., & Prabhu, J. (2016). Innovation for inclusive growth: Towards a theoretical framework and a research agenda. Journal of Management Studies, 53(3), 497–512. https://doi.org/10.1111/joms.12181 |
| [27] | Webb, J. W., Khoury, T. A., & Hitt, M. A. (2020). The influence of formal and informal institutional voids on entrepreneurship. Entrepreneurship Theory and Practice, 44(3), 504–526.
https://doi.org/10.1177/1042258719830310 |
[3, 8, 27]
. Second, dominant entrepreneurship models remain market-centric and therefore travel imperfectly to sectors where market entry follows, rather than precedes, institutional validation
| [6] | Blank, S. G. (2013). Why the lean start-up changes everything. Harvard Business Review, 91(5), 63–72.
https://hbr.org/2013/05/why-the-lean-start-up-changes-everything |
| [21] | Ries, E. (2011). The lean startup: How today's entrepreneurs use continuous innovation to create radically successful businesses. Crown Currency.
https://www.penguinrandomhouse.com/books/210088/the-lean-startup-by-eric-ries/ |
| [10] | Greenhalgh, T., Wherton, J., Papoutsi, C., Lynch, J., Hughes, G., A'Court, C., Hinder, S., Fahy, N., Procter, R., & Shaw, S. (2017). Beyond adoption: A new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. Journal of Medical Internet Research, 19(11), e367. https://doi.org/10.2196/jmir.8775 |
[6, 21, 10]
. Third, the connections between entrepreneurship, institutional theory, and health systems research remain thinner than the phenomenon demands
. To address these gaps, the paper develops a process framework of institutionally mediated market formation and uses it to explain cross-case variation in venture progression. The move from factor-based explanation to process explanation matters because the barriers identified in prior research do not act as isolated obstacles; they acquire causal force through temporal sequence, interdependence, and threshold effects across validation domains.
2.7. Conceptual Framework: Institutionally Mediated Market Formation
2.7.1. Conceptual Foundation
The core proposition of the framework is straightforward: in regulated health innovation settings, ventures do not enter markets directly; they construct a pathway to conditional market entry through the sequencing and alignment of multiple validation processes. Market formation is therefore institutionally mediated. It depends on the accumulation of legitimacy across domains that are analytically distinct but operationally interdependent.
From this perspective, market entry is not the opposite of institutional mediation. It is its outcome. Ventures become market participants only after they have secured sufficient legitimacy to move through regulatory, clinical, and institutional gates. This shifts analytical attention from demand discovery alone to the problem of coordinated validation.
2.7.2. Framework Components
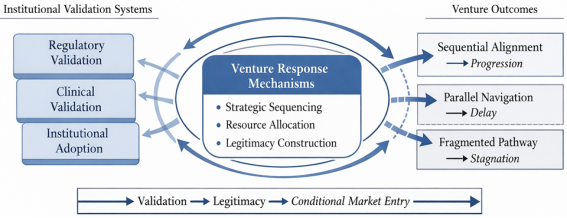
The first component of the framework is the set of institutional validation systems that shape deployment. Three domains are central. Regulatory validation concerns formal approval, compliance, and safety authorization. Clinical validation concerns professional acceptance, evidence of efficacy, usability, and fit with clinical practice. Institutional adoption concerns onboarding into service delivery and procurement structures, including hospitals, pharmacies, public programs, and other delivery intermediaries. These domains are mutually dependent but not automatically coordinated. A venture may satisfy one and still be unable to progress.
The second component concerns venture response mechanisms. Ventures are not passive recipients of institutional demands. They respond through strategic sequencing, resource allocation under constraint, and legitimacy construction. Strategic sequencing captures the order in which ventures engage validation domains. Resource allocation under constraint captures how scarce time, capital, and technical effort are distributed across product development, compliance, trials, and partnership-building. Legitimacy construction captures how ventures build credibility with regulators, clinicians, and adopters whose judgments are not identical. These mechanisms are analytically distinct but practically intertwined.
The third component concerns progression pathways. When validation activities are staged in mutually reinforcing order, ventures exhibit sequential alignment. When activities are pursued with some logic but are slowed by the timing of external decision processes, ventures experience temporally constrained alignment. When engagements are dispersed, opportunistic, or weakly connected across domains, ventures exhibit fragmented progression. These pathways are not simply descriptive categories; they represent different ways of organizing action under institutional complexity.
The framework therefore identifies a central mechanism: coordinated validation under temporal constraint. Progress depends on whether ventures can synchronize their own actions with institutional processes that they do not control. This has three implications. First, legitimacy is cumulative but not infinitely fungible. Regulatory gains can strengthen clinical or institutional credibility, but they cannot replace the need to cross domain-specific thresholds. Second, coordination is temporal as well as structural. Validation activities must not only connect; they must connect at the right time. Third, venture outcomes are shaped by the interplay between internal strategy and external pacing.
This framework contributes to entrepreneurship research by specifying a boundary condition to market-centric accounts of venture development. It contributes to ecosystem research by showing that interdependence is partly constituted by permission structures that condition entry into the ecosystem. It contributes to institutional theory by specifying how multi-domain legitimacy operates in regulated innovation systems.
Figure 1 presents the conceptual framework of institutionally mediated market formation.
Figure 1. Institutionally mediated market formation framework.
Note. Developed by the authors. The figure shows how institutional validation systems, venture response mechanisms, and outcome pathways interact to shape conditional market entry in regulated health innovation settings.
3. Materials and Methods
3.1. Research Design
The study uses a longitudinal, comparative case design to examine how early-stage health technology ventures progressed toward deployment over time. A process approach is appropriate because the objective is not to estimate static relationships between variables but to explain sequences, dependencies, turning points, and divergent pathways of progression
| [15] | Langley, A., Smallman, C., Tsoukas, H., & Van de Ven, A. H. (2013). Process studies of change in organization and management: Unveiling temporality, activity, and flow. Academy of Management Journal, 56(1), 1–13.
https://doi.org/10.5465/amj.2013.4001 |
| [26] | Van de Ven, A. H., Polley, D. E., Garud, R., & Venkataraman, S. (1999). The innovation journey. Oxford University Press.
https://openlibrary.org/books/OL16948965M/The_innovation_journey |
[15, 26]
. Comparative case analysis also allows analytically meaningful variation to be examined while preserving sensitivity to institutional context
.
3.2. Empirical Setting and Case Logic
Rwanda provides a revealing empirical setting. Health technology ventures in Rwanda engage a health system where public institutions play a central role in regulation, authorization, and adoption
| [17] | Ministry of Health, Rwanda. (2024). Health Sector Strategic Plan V (2024/25–2028/29). https://www.moh.gov.rw/fileadmin/user_upload/Moh/Publications/Reports/new_annual_Report/HSSP_V_signed.pdf |
| [22] | Rudasingwa, M., Jahn, A., Uwitonze, A.-M., & Hennig, L. (2022). Increasing health system synergies in low-income settings: Lessons learned from a qualitative case study of Rwanda. Global Public Health, 17(12), 3303–3321.
https://doi.org/10.1080/17441692.2022.2129726 |
[17, 22]
. This makes the institutional mediation of venture progression unusually visible. The case is not presented as representative of all African or LMIC health systems. Rather, it is analytically valuable because relatively coordinated governance structures make the alignment problem easier to observe and theorize.
3.3. Sample and Data Sources
The sample was purposively constructed around early-stage ventures developing technology-enabled health solutions and actively engaging at least one formal validation process. Selection followed three criteria: the venture had to be developing a technology-enabled health solution; it had to remain at an early stage of product development or initial deployment effort; and it had to be actively engaging at least one formal validation process such as regulatory review, clinical testing, or institutional integration. The empirical material spans an 18-month observation window and combines four sources: venture milestone plans and planning documents, periodic progress reports and internal tracking records, observational notes generated through engagement with venture teams, and documented interactions with regulatory, clinical, and institutional actors. Together, these materials provide a longitudinal view of how ventures set priorities, revised milestones, distributed resources, and negotiated institutional demands.
To protect confidentiality, ventures are anonymized and sensitive operational details are abstracted. This choice constrains the level of firm-identifying narrative detail that can be reported, but it strengthens candor in the analysis of progression dynamics. The goal is mechanism-based explanation rather than firm profiling.
3.4. Analytical Strategy
The analysis proceeded in four steps. First, the empirical material was organized into venture-period observations, creating a temporal matrix for each case. This structure allowed the analysis to capture not only activities performed in each period, but also critical transition points at which progress in one validation domain either unlocked or blocked movement in the next. Second, within-case process narratives were reconstructed to identify critical events, bottlenecks, and shifts in strategic emphasis. Third, the cases were coded comparatively around three theoretically informed dimensions: validation sequencing, resource allocation under constraint, and legitimacy construction across domains. Fourth, recurring configurations were grouped into pathway types and compared across cases to identify the mechanism linking validation dynamics to progression outcomes.
Analytically, the study seeks pattern-based causal explanation rather than frequency-based inference. The logic of generalization is therefore analytic. The question is whether the identified mechanism clarifies how venture progression operates in institutionally mediated environments, not whether the observed distribution of cases is statistically representative
.
Table 1 summarizes the research design and analytical structure.
Table 1. Research design and analytical structure.
Element | Description |
Research strategy | Longitudinal comparative case study with process tracing. |
Setting | Early-stage health technology ventures operating in Rwanda within a health system where public institutions strongly mediate authorization and adoption. |
Observation window | 18 months. |
Selection logic | Purposive inclusion of early-stage ventures developing technology-enabled health solutions and engaging at least one formal validation process. |
Data sources | Milestone plans, progress reports, observational notes, and records of interaction with regulatory, clinical, and institutional actors. |
Analytical unit | Venture-period observation. |
Primary coding dimensions | Validation sequencing, resource allocation under constraint, and legitimacy construction across domains. |
Logic of generalization | Analytic rather than statistical generalization. |
3.5. Rigor and Ethics
Several steps were taken to strengthen rigor. Triangulation across multiple documentary and observational sources reduced dependence on any single account
. The longitudinal design allowed sequences and reversals to be observed rather than inferred retrospectively
| [15] | Langley, A., Smallman, C., Tsoukas, H., & Van de Ven, A. H. (2013). Process studies of change in organization and management: Unveiling temporality, activity, and flow. Academy of Management Journal, 56(1), 1–13.
https://doi.org/10.5465/amj.2013.4001 |
[15]
. Cross-case comparison disciplined interpretation by forcing claims to account for both common patterns and meaningful contrasts
. Ethical care centered on confidentiality, case anonymization, and the avoidance of commercially sensitive disclosure.
4. Findings
4.1. Venture Progression Depends on Coordinated Validation
The cross-case analysis shows that venture progression was not explained primarily by differences in technical sophistication, commitment, or entrepreneurial activity. Across the cases, ventures displayed substantial effort, active product development, and, in some instances, early signs of demand or partnership interest. Yet these strengths did not reliably produce forward movement toward deployment. The decisive variation lay in whether validation activities across regulatory, clinical, and institutional domains became aligned.
Market entry therefore emerged as an institutionally mediated process. Ventures did not progress because they had discovered demand alone. They progressed when they built a sequence in which one validation stage supported the next, and when that sequence remained synchronized with the timing of external actors. Where such coordination failed, progress stalled even when the venture itself remained active and capable.
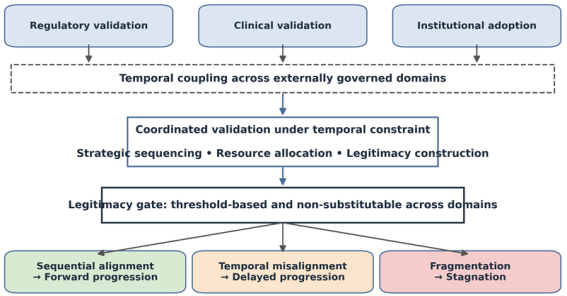
Three recurrent pathway configurations were observed. The first was sequential alignment associated with forward progression. The second was temporally constrained alignment associated with delay despite otherwise appropriate sequencing. The third was fragmented progression associated with stagnation.
Figure 2 presents the mechanism of coordinated validation under temporal constraint and its three pathway outcomes.
Figure 2. Coordinated validation under temporal constraint. Note. Developed by the authors. The figure synthesizes how regulatory, clinical, and institutional validation interact through temporal coupling to produce forward progression, delayed progression, or stagnation.
4.2. Sequential Alignment and Forward Progression
In the forward-progression configuration, ventures did not approach validation domains randomly. They engaged them in a strategically ordered way. Regulatory work was addressed early enough to reduce downstream uncertainty. Clinical validation followed from, rather than competed with, that regulatory footing. Institutional adoption discussions were then pursued from a position of growing legitimacy rather than speculative promise alone. In practical terms, ventures in this pathway first clarified compliance expectations, then used that clarity to structure pilot or clinician-facing activities before approaching institutional adopters.
This sequencing mattered because each successful validation step altered the venture’s position in the next domain. Regulatory credibility strengthened the plausibility of clinical trials or pilot use. Clinical endorsement, in turn, improved the venture’s standing with hospitals or public agencies that would ultimately determine deployment. Legitimacy was therefore cumulative and partly transferable across domains, but only when the sequence was coherent.
Importantly, the process was iterative without becoming directionless. Ventures revisited earlier assumptions, modified plans, and responded to feedback, but these adjustments occurred within an aligned pathway rather than through disconnected experimentation. In effect, iteration improved the fit of the sequence instead of replacing it. The result was forward progression toward conditional market entry.
4.3. Temporally Constrained Alignment and Delayed Progression
A second pattern revealed that correct sequencing was necessary but not sufficient. In these cases, ventures followed a logic of staged validation, often prioritizing regulatory or ethical clearance before more visible market engagement. Internally, they appeared ready to advance. Externally, however, the relevant institutions moved more slowly. Approval cycles, review processes, and decision bottlenecks produced delay even though the venture’s own sequencing remained coherent. In several cases, teams continued refining products and cultivating relationships while awaiting decisions they could not accelerate.
This pattern exposes a key feature of regulated innovation systems: coordination is governed not only by interdependence but by timing. Even when ventures do the right things in the right order, progression depends on externally controlled rhythms. The issue is not strategic failure but temporal coupling. Internal readiness cannot be converted into deployment until institutional actors cross their own thresholds.
The implication is important. Delay should not automatically be read as evidence of weak entrepreneurial capability. In institutionally mediated settings, delay can also be the outcome of dependency on external validation schedules. Ventures in this configuration continued building technical capability and partnerships, but progression remained suspended until authorization caught up with readiness.
4.4. Fragmented Progression and Stagnation
The third pathway was marked by high activity but weak coordination. Ventures in this configuration pursued product development, partnership exploration, and market conversations in parallel, yet without a coherent sequence linking these efforts across validation domains. Regulatory engagement was partial or late. Clinical validation remained thin or episodic. Institutional conversations occurred before the underlying evidence base or authorization pathway was sufficiently established. Typical examples included opening partnership discussions before compliance requirements were settled or exploring pilots without a clear route to procurement and integration.
Such ventures often appeared dynamic on the surface. They pivoted, explored opportunities, and kept multiple conversations alive. But because progress in one domain was not converted into credibility in the next, effort was dispersed rather than compounded. Product development could not substitute for regulatory clearance. Partnership interest could not substitute for clinical endorsement. Market exploration could not substitute for adoption readiness.
The central empirical insight here is that legitimacy is non-substitutable across critical domains. A venture cannot make up for missing regulatory or clinical validation through entrepreneurial energy alone. Where coordination remained fragmented, no single domain reached the threshold necessary to unlock broader deployment, and stagnation followed.
4.5. Cross-case Synthesis
Across the three pathways, the decisive variable was the structure of validation, not the quantity of activity. Comparable levels of technical sophistication, entrepreneurial effort, and partnership activity yielded different outcomes because internal capability could not be converted into deployment unless validation advanced in synchronized cross-domain sequence. Forward progression emerged when validation domains were engaged in mutually reinforcing order. Delay emerged when that order existed but was slowed by the externally governed timing of institutional processes. Stagnation emerged when validation work was dispersed across domains without alignment.
This pattern supports the paper’s core claim: venture progression in regulated health technology settings is best explained as coordinated validation under temporal constraint. The relevant entrepreneurial challenge is not only to build a good solution, but to synchronize validation across institutional systems that impose different evidence standards, authority relations, and pacing rhythms.
Table 2 summarizes the key contrasts among the three pathway configurations.
Table 2. Pathways of venture progression across validation systems.
Pathway | Sequencing pattern | Coordination problem | Result |
Sequential alignment | Validation activities are staged in a mutually reinforcing order across regulatory, clinical, and adoption domains. | Dependencies are managed through an explicit sequence that allows legitimacy to build cumulatively. | Forward progression toward deployment. |
Temporally constrained alignment | The venture follows a coherent sequence, but external approvals and institutional reviews move more slowly than venture readiness. | Temporal coupling across externally governed domains delays conversion of readiness into deployment. | Delayed progression. |
Fragmented progression | Activities are pursued opportunistically or in parallel without cross-domain synchronization. | Resources and attention are dispersed, so no domain reaches the threshold required to unlock the next. | Stagnation. |
5. Discussion
5.1. Reframing Venture Progression in Regulated Settings
The findings reframe how early-stage venture progression should be understood in regulated environments. Market-centric models remain valuable for explaining experimentation and learning once ventures can access users and buyers. But they are incomplete where access itself is conditioned by prior institutional approval. In such settings, the primary problem is not simply whether a venture can discover demand; it is whether the venture can organize a credible pathway through multiple validation gates. Product-market fit may still matter, but it does not arrive first
.
This argument defines a boundary condition for lean venture development logics. Rapid iteration and customer discovery are not universally wrong; they are conditionally available. Their usefulness depends on whether the venture has enough institutional standing to engage the relevant users, sites, or buyers in the first place. In health technology, that standing must often be constructed before meaningful market learning can occur
| [10] | Greenhalgh, T., Wherton, J., Papoutsi, C., Lynch, J., Hughes, G., A'Court, C., Hinder, S., Fahy, N., Procter, R., & Shaw, S. (2017). Beyond adoption: A new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. Journal of Medical Internet Research, 19(11), e367. https://doi.org/10.2196/jmir.8775 |
| [29] | World Health Organization. (2021). Global strategy on digital health 2020–2025. https://iris.who.int/handle/10665/344249 |
[10, 29]
.
5.2. Extending Ecosystem and Institutional Theory
The study also extends ecosystem research. Existing work rightly emphasizes that value creation depends on coordinated action among interdependent actors
| [1] | Adner, R. (2017). Ecosystem as structure: An actionable construct for strategy. Journal of Management, 43(1), 39–58.
https://doi.org/10.1177/0149206316678451 |
| [13] | Jacobides, M. G., Cennamo, C., & Gawer, A. (2018). Towards a theory of ecosystems. Strategic Management Journal, 39(8), 2255–2276. https://doi.org/10.1002/smj.2904 |
[1, 13]
. The present findings add that coordination is temporal as well as structural. Ventures do not coordinate only with other actors; they coordinate with the timing of other actors. Where institutional rhythms are slow, asynchronous, or opaque, even well-structured strategies can become delayed. Ecosystem participation is therefore partly a question of synchronization. This also resonates with ecosystem research showing that ventures in nascent ecosystems must continually navigate interdependence under uncertainty rather than merely coordinate with a stable set of complementary actors
| [11] | Hannah, D. P., & Eisenhardt, K. M. (2018). How firms navigate cooperation and competition in nascent ecosystems. Strategic Management Journal, 39(12), 3163–3192.
https://doi.org/10.1002/smj.2750 |
[11]
.
For institutional theory, the paper refines the concept of legitimacy. Legitimacy did not operate here as a single generalized perception of appropriateness. It operated as a multi-domain, threshold-based condition. Regulatory, clinical, and institutional legitimacy were related, but not interchangeable. Gains in one domain could strengthen prospects in another, yet each domain retained its own gatekeeping authority. This makes legitimacy both cumulative and bounded.
More precisely, legitimacy functioned as a threshold-based gating mechanism. Gains in product development, partnership formation, or entrepreneurial momentum could improve prospects, but they could not substitute for missing regulatory or clinical legitimacy once those thresholds became binding. The content and timing of those thresholds were also defined largely by external actors rather than by the venture itself.
5.3. Practical Implications
The practical implications are direct. Founders and venture teams in health technology should treat validation architecture as a core strategic problem, not as an afterthought to product development. This means mapping the sequence of necessary approvals and endorsements, identifying the dependencies between them, and allocating scarce resources accordingly. Incubators and investors should likewise evaluate ventures not only on technological promise, but on the quality of their validation strategy. A venture with a weak coordination plan may look innovative while remaining structurally unprepared for deployment.
Policy implications are equally important. If governments and health system actors want more promising ventures to reach deployment, reducing misalignment across validation systems matters as much as, and often more than, increasing entrepreneurial capability in the abstract. Clearer approval pathways, better coordination between ethics, regulatory, and adoption actors, and more transparent institutional expectations could materially change the progression prospects of early-stage ventures. Recent work on AI-driven healthcare entrepreneurship in LMICs likewise shows that interoperability, governance, trust, and reimbursement pathways remain decisive for moving entrepreneurial health technologies beyond pilot activity and into routine service delivery
| [23] | Sangwa, S., & Mutabazi, P. (2025). AI-driven healthcare entrepreneurship: Transforming clinical practice through innovation, access, and affordability [Version 1; peer review: 1 approved with reservations]. F1000 Research, 14, Article 921.
https://doi.org/10.12688/f1000research.169681.1 |
[23]
.
This also implies a governance agenda. Health innovation systems require not only supportive entrepreneurship programs but also operational coordination across regulation, ethics review, clinical validation, interoperability standards, procurement, and implementation support. Recent digital-health governance research likewise shows that leadership, data governance, and cross-institutional coordination are foundational conditions of successful transformation rather than secondary administrative matters
| [9] | Gotsadze, G., Zoidze, A., Gabunia, T., & Chin, B. (2024). Advancing governance for digital transformation in health: Insights from Georgia’s experience. BMJ Global Health, 9(10), e015589. https://doi.org/10.1136/bmjgh-2024-015589 |
[9]
.
5.4. Boundary Conditions
The argument is not that capability is irrelevant. Technical quality, persistence, and strategic judgment still matter. The point is narrower and more precise: in regulated health innovation settings, capability becomes consequential through coordination. Rwanda makes this especially visible because institutional interdependencies are relatively concentrated. In more fragmented systems, the same mechanism may operate through different actors and with more dispersed sites of authority, but the need for coordinated validation is unlikely to disappear. The mechanism should therefore travel beyond Rwanda to other settings where deployment depends on linked approvals, institutional gatekeeping, and phased adoption; what varies across contexts is the number of gatekeepers, the degree of fragmentation, and the speed with which legitimacy can be assembled.
6. Conclusion and Future Research
This study set out to explain why early-stage health technology ventures often struggle to move from development to deployment in regulated environments. Drawing on longitudinal comparative evidence from Rwanda, it showed that the key explanatory issue is not capability alone but the alignment of validation across regulatory, clinical, and institutional systems. Ventures progressed when validation activities became mutually reinforcing. They were delayed when sequencing was sound but external pacing slowed conversion to deployment. They stagnated when efforts were fragmented across domains.
The study’s central contribution is the concept of coordinated validation under temporal constraint. This concept reorients analysis from firm capability in isolation to system-embedded synchronization across domains that ventures do not fully control. It also helps explain why promising health innovations so often stall before scale becomes relevant.
The study has clear limits. The case material is small-N and confidentiality requirements constrain the degree of firm-specific exposition that can be provided. The analysis focuses on progression toward deployment rather than long-run scale, sustainability, or commercial performance. It also does not fully capture the political micro-dynamics through which powerful institutional actors shape validation standards and timing.
Those standards and timelines are not neutral. They are enacted through professional judgments, administrative routines, organizational risk tolerances, and positional authority that can accelerate some ventures while holding others in suspension. A fuller account of progression in regulated environments therefore requires closer attention to the politics of gatekeeping, not only to the architecture of coordination.
Future research should compare these dynamics across differently structured health systems, follow ventures beyond initial deployment, and examine how entrepreneurs actively negotiate and reshape validation environments. A particularly important comparison would be between relatively coordinated systems, where interdependencies are concentrated and more visible, and more fragmented systems, where the same mechanism may be distributed across a larger number of gatekeepers and transaction points. Even with these limits, the evidence supports a clear conclusion: in regulated health innovation systems, ventures fail less because they lack ideas than because validation systems remain insufficiently aligned with the pathways through which those ideas must travel.
Abbreviations
LMICs | Low- and Middle-Income Countries |
DDG | Digitization Directorate General |
ORCID | Open Researcher and Contributor ID |
Author Contributions
Stanley Mukasa: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Supervision, Visualization, Writing – original draft, Writing – review & editing
Sixbert Sangwa: Data curation, Formal Analysis, Investigation, Methodology, Validation, Visualization, Writing – review & editing
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Adner, R. (2017). Ecosystem as structure: An actionable construct for strategy. Journal of Management, 43(1), 39–58.
https://doi.org/10.1177/0149206316678451
|
| [2] |
Adner, R., & Kapoor, R. (2016). Innovation ecosystems and the pace of substitution: Re-examining technology S-curves. Strategic Management Journal, 37(4), 625–648.
https://doi.org/10.1002/smj.2363
|
| [3] |
Aranda-Jan, C. B., Mohutsiwa-Dibe, N., & Loukanova, S. (2014). Systematic review on what works, what does not work and why of implementation of mobile health (mHealth) projects in Africa. BMC Public Health, 14, Article 188.
https://doi.org/10.1186/1471-2458-14-188
|
| [4] |
Autio, E., Kenney, M., Mustar, P., Siegel, D., & Wright, M. (2014). Entrepreneurial innovation: The importance of context. Research Policy, 43(7), 1097–1108.
https://doi.org/10.1016/j.respol.2014.01.015
|
| [5] |
Autio, E., Nambisan, S., Thomas, L. D. W., & Wright, M. (2018). Digital affordances, spatial affordances, and the genesis of entrepreneurial ecosystems. Strategic Entrepreneurship Journal, 12(1), 72–95.
https://doi.org/10.1002/sej.1266
|
| [6] |
Blank, S. G. (2013). Why the lean start-up changes everything. Harvard Business Review, 91(5), 63–72.
https://hbr.org/2013/05/why-the-lean-start-up-changes-everything
|
| [7] |
Buse, K., Mays, N., & Walt, G. (2012). Making health policy (2nd ed.). Open University Press.
https://research.monash.edu/en/publications/making-health-policy-2/
|
| [8] |
George, G., McGahan, A. M., & Prabhu, J. (2016). Innovation for inclusive growth: Towards a theoretical framework and a research agenda. Journal of Management Studies, 53(3), 497–512.
https://doi.org/10.1111/joms.12181
|
| [9] |
Gotsadze, G., Zoidze, A., Gabunia, T., & Chin, B. (2024). Advancing governance for digital transformation in health: Insights from Georgia’s experience. BMJ Global Health, 9(10), e015589.
https://doi.org/10.1136/bmjgh-2024-015589
|
| [10] |
Greenhalgh, T., Wherton, J., Papoutsi, C., Lynch, J., Hughes, G., A'Court, C., Hinder, S., Fahy, N., Procter, R., & Shaw, S. (2017). Beyond adoption: A new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies. Journal of Medical Internet Research, 19(11), e367.
https://doi.org/10.2196/jmir.8775
|
| [11] |
Hannah, D. P., & Eisenhardt, K. M. (2018). How firms navigate cooperation and competition in nascent ecosystems. Strategic Management Journal, 39(12), 3163–3192.
https://doi.org/10.1002/smj.2750
|
| [12] |
Hwang, J., & Christensen, C. M. (2008). Disruptive innovation in health care delivery: A framework for business-model innovation. Health Affairs, 27(5), 1329–1335.
https://doi.org/10.1377/hlthaff.27.5.1329
|
| [13] |
Jacobides, M. G., Cennamo, C., & Gawer, A. (2018). Towards a theory of ecosystems. Strategic Management Journal, 39(8), 2255–2276.
https://doi.org/10.1002/smj.2904
|
| [14] |
Labrique, A., Vasudevan, L., Chang, L. W., & Mehl, G. (2013). H_pe for mHealth: More “y” or “o” on the horizon? International Journal of Medical Informatics, 82(5), 467–469.
https://doi.org/10.1016/j.ijmedinf.2012.11.016
|
| [15] |
Langley, A., Smallman, C., Tsoukas, H., & Van de Ven, A. H. (2013). Process studies of change in organization and management: Unveiling temporality, activity, and flow. Academy of Management Journal, 56(1), 1–13.
https://doi.org/10.5465/amj.2013.4001
|
| [16] |
McMullen, J. S., & Dimov, D. (2013). Time and the entrepreneurial journey: The problems and promise of studying entrepreneurship as a process. Journal of Management Studies, 50(8), 1481–1512.
https://doi.org/10.1111/joms.12049
|
| [17] |
Ministry of Health, Rwanda. (2024). Health Sector Strategic Plan V (2024/25–2028/29).
https://www.moh.gov.rw/fileadmin/user_upload/Moh/Publications/Reports/new_annual_Report/HSSP_V_signed.pdf
|
| [18] |
Ministry of Health, Rwanda. (2018). National Digital Health Strategy 2018–2023.
https://extranet.who.int/countryplanningcycles/planning-cycle-files/national-digital-health-strategy-2018-2023
|
| [19] |
Ministry of Health, Rwanda. (n.d.). Digitization Directorate General (DDG).
https://www.moh.gov.rw/digitization-directorate-general-ddg
|
| [20] |
Pahnke, E. C., Katila, R., & Eisenhardt, K. M. (2015). Who takes you to the dance? How partners’ institutional logics influence innovation in young firms. Administrative Science Quarterly, 60(4), 596–633.
https://doi.org/10.1177/0001839215592913
|
| [21] |
Ries, E. (2011). The lean startup: How today's entrepreneurs use continuous innovation to create radically successful businesses. Crown Currency.
https://www.penguinrandomhouse.com/books/210088/the-lean-startup-by-eric-ries/
|
| [22] |
Rudasingwa, M., Jahn, A., Uwitonze, A.-M., & Hennig, L. (2022). Increasing health system synergies in low-income settings: Lessons learned from a qualitative case study of Rwanda. Global Public Health, 17(12), 3303–3321.
https://doi.org/10.1080/17441692.2022.2129726
|
| [23] |
Sangwa, S., & Mutabazi, P. (2025). AI-driven healthcare entrepreneurship: Transforming clinical practice through innovation, access, and affordability [Version 1; peer review: 1 approved with reservations]. F1000 Research, 14, Article 921.
https://doi.org/10.12688/f1000research.169681.1
|
| [24] |
Scott, W. R. (2014). Institutions and organizations: Ideas, interests, and identities (4th ed.). SAGE Publications.
https://collegepublishing.sagepub.com/products/institutions-and-organizations-4-237665
|
| [25] |
Suchman, M. C. (1995). Managing legitimacy: Strategic and institutional approaches. Academy of Management Review, 20(3), 571–610.
https://doi.org/10.5465/amr.1995.9508080331
|
| [26] |
Van de Ven, A. H., Polley, D. E., Garud, R., & Venkataraman, S. (1999). The innovation journey. Oxford University Press.
https://openlibrary.org/books/OL16948965M/The_innovation_journey
|
| [27] |
Webb, J. W., Khoury, T. A., & Hitt, M. A. (2020). The influence of formal and informal institutional voids on entrepreneurship. Entrepreneurship Theory and Practice, 44(3), 504–526.
https://doi.org/10.1177/1042258719830310
|
| [28] |
World Bank. (2023). Digital-in-health: Unlocking the value for everyone. World Bank.
http://hdl.handle.net/10986/40212
|
| [29] |
World Health Organization. (2021). Global strategy on digital health 2020–2025.
https://iris.who.int/handle/10665/344249
|
| [30] |
Yin, R. K. (2014). Case study research: Design and methods (5th ed.). SAGE Publications.
https://collegepublishing.sagepub.com/products/case-study-research-5-237921
|
Cite This Article
-
APA Style
Mukasa, S., Sangwa, S. (2026). Coordinated Validation Under Temporal Constraint: Explaining Early-Stage Health Technology Venture Progression in Rwanda. American Journal of Engineering and Technology Management, 11(2), 20-30. https://doi.org/10.11648/j.ajetm.20261102.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Mukasa, S.; Sangwa, S. Coordinated Validation Under Temporal Constraint: Explaining Early-Stage Health Technology Venture Progression in Rwanda. Am. J. Eng. Technol. Manag. 2026, 11(2), 20-30. doi: 10.11648/j.ajetm.20261102.12
Copy
|
Download
AMA Style
Mukasa S, Sangwa S. Coordinated Validation Under Temporal Constraint: Explaining Early-Stage Health Technology Venture Progression in Rwanda. Am J Eng Technol Manag. 2026;11(2):20-30. doi: 10.11648/j.ajetm.20261102.12
Copy
|
Download
-
@article{10.11648/j.ajetm.20261102.12,
author = {Stanley Mukasa and Sixbert Sangwa},
title = {Coordinated Validation Under Temporal Constraint: Explaining Early-Stage Health Technology Venture Progression in Rwanda},
journal = {American Journal of Engineering and Technology Management},
volume = {11},
number = {2},
pages = {20-30},
doi = {10.11648/j.ajetm.20261102.12},
url = {https://doi.org/10.11648/j.ajetm.20261102.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajetm.20261102.12},
abstract = {Background: Why promising health technology ventures stall between product development and real-world deployment remains insufficiently explained in entrepreneurship research. Market-centric models emphasize experimentation, customer discovery, and product-market fit, but these mechanisms are less explanatory where access to users, clinical settings, and procurement channels is institutionally mediated. Methods: This study develops a process explanation of venture progression in regulated health innovation settings. Drawing on institutional theory, innovation systems research, and process views of entrepreneurship, it uses a longitudinal comparative case design to analyze early-stage health technology ventures in Rwanda over an 18-month observation window. The empirical material comprises venture milestone plans, periodic progress reports, observational notes, and documented interactions with regulatory, clinical, and institutional actors. Results: Venture progression was not explained primarily by technical capability, entrepreneurial effort, or early market interest. Rather, outcomes varied according to whether ventures achieved coordinated validation across interdependent regulatory, clinical, and institutional domains. Three recurrent pathway configurations were identified: sequential alignment, associated with forward progression; temporally constrained alignment, associated with delayed progression despite coherent sequencing; and fragmented progression, associated with stagnation. The findings show that legitimacy in regulated health innovation settings is multi-domain, threshold-based, and time-dependent. Conclusion: The study advances the concept of coordinated validation under temporal constraint to explain how ventures move, or fail to move, from development to deployment when market entry depends on synchronized institutional approval. It contributes to entrepreneurship and innovation theory by reframing venture progression in regulated environments as a coordination problem rather than a pure capability problem. Rwanda serves as a revealing case because its comparatively coordinated health system makes the underlying synchronization problem especially visible.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Coordinated Validation Under Temporal Constraint: Explaining Early-Stage Health Technology Venture Progression in Rwanda
AU - Stanley Mukasa
AU - Sixbert Sangwa
Y1 - 2026/04/24
PY - 2026
N1 - https://doi.org/10.11648/j.ajetm.20261102.12
DO - 10.11648/j.ajetm.20261102.12
T2 - American Journal of Engineering and Technology Management
JF - American Journal of Engineering and Technology Management
JO - American Journal of Engineering and Technology Management
SP - 20
EP - 30
PB - Science Publishing Group
SN - 2575-1441
UR - https://doi.org/10.11648/j.ajetm.20261102.12
AB - Background: Why promising health technology ventures stall between product development and real-world deployment remains insufficiently explained in entrepreneurship research. Market-centric models emphasize experimentation, customer discovery, and product-market fit, but these mechanisms are less explanatory where access to users, clinical settings, and procurement channels is institutionally mediated. Methods: This study develops a process explanation of venture progression in regulated health innovation settings. Drawing on institutional theory, innovation systems research, and process views of entrepreneurship, it uses a longitudinal comparative case design to analyze early-stage health technology ventures in Rwanda over an 18-month observation window. The empirical material comprises venture milestone plans, periodic progress reports, observational notes, and documented interactions with regulatory, clinical, and institutional actors. Results: Venture progression was not explained primarily by technical capability, entrepreneurial effort, or early market interest. Rather, outcomes varied according to whether ventures achieved coordinated validation across interdependent regulatory, clinical, and institutional domains. Three recurrent pathway configurations were identified: sequential alignment, associated with forward progression; temporally constrained alignment, associated with delayed progression despite coherent sequencing; and fragmented progression, associated with stagnation. The findings show that legitimacy in regulated health innovation settings is multi-domain, threshold-based, and time-dependent. Conclusion: The study advances the concept of coordinated validation under temporal constraint to explain how ventures move, or fail to move, from development to deployment when market entry depends on synchronized institutional approval. It contributes to entrepreneurship and innovation theory by reframing venture progression in regulated environments as a coordination problem rather than a pure capability problem. Rwanda serves as a revealing case because its comparatively coordinated health system makes the underlying synchronization problem especially visible.
VL - 11
IS - 2
ER -
Copy
|
Download